

Abstract
Coronary artery aneurysms (CAAs) occur when an artery dilates 1.5 times the reference vessel. They occur most commonly because of atherosclerosis. CAAs are a rare phenomenon, and it is even rarer to find a giant CAA, which is roughly defined as a size 400% above the reference vessel. Giant CAAs are commonly found in the right coronary artery. The sinoatrial nodal artery (SNA) is among the least common sites for CAA involvement. Sometimes, communication exists between the aneurysm and a chamber of the heart or a great vessel. The consequences of the fistula depend on its size. Because of the rarity of the condition, guidelines are not well developed. However, small CAAs can be managed conservatively, whereas giant CAAs require resection, ligation, and bypass grafting. CAAs have a predilection for males and the elderly. We describe a 40-year-old South Asian woman presenting with mild dyspnea on exertion of 1 year’s duration. Echocardiography showed a 60×60 mm cystic sac, subsequently confirmed by computerized tomography, which showed 3 large aneurysms (70×61 mm) and 3 small aneurysms in the SNA. Coronary angiography illustrated that the SNA branched off the left main coronary artery, and the aneurysm communicated with the right coronary artery. The aneurysm was partially resected and plicated.
Keywords: Aneurysm, false; Coronary aneurysm; Right atrium; Coronary angiography
Introduction
Coronary artery anomalies constitute a class of disorders that can be life-threatening regardless of the presence or absence of other cardiovascular risk factors. Coronary artery aneurysms (CAAs) comprise a category of such anomalies. Coronary artery dilations of over 50% of the diameter of the normal adjacent artery are conventionally termed “CAAs”. It is an uncommon condition found in up to 0.3% to 5% of individuals during coronary angiography.1 Because of the rising trend in interventional techniques, the incidence of CAAs is rising.2 CAAs usually involve a single vessel, whereas rarely do they involve more than 1 vessel.3 The right coronary artery (RCA) is the most commonly involved vessel in CAAs.4 Atherosclerosis is the known cause in half of CAAs.5 Sinoatrial nodal artery (SNA) aneurysms are extremely rare.6, 7 There is no strict cutoff, but CAAs 4 times greater than the reference vessel are termed “giant CAAs” and seen in fewer than 0.2% of CAAs. The incidence rate of giant CAAs above 50 mm is only 0.02%.1 Sometimes, the aneurysm may form a fistula between the heart chambers or the major cardiac vessels.7
We describe a 40-year-old woman presenting with dyspnea. Cardiac computerized tomography (CT) showed findings suggestive of a giant aneurysmal sac arising from the SNA with a fistula into the right atrium. We successfully treated the aneurysm with surgery. This is the first reported case in Pakistan regarding a giant SNA aneurysm and should assist healthcare professionals in the management of similar cases.
Case Report
A 46-year-old woman with no history of trauma presented with shortness of breath and chest pain on mild exertion of 1 year’s duration. The pain was mild in intensity, with no associated symptoms. The patient had no known comorbidity. Her transthoracic echocardiography revealed a large round cystic space visualized anterior to the right atrium measuring 60×60 mm with continuous flow, suggestive of a coronary artery fistula with an aneurysm. No obstruction existed in the superior or inferior vena cava flow. Cardiac CT showed an SNA originating from the left main coronary artery (LMCA) via a separate ostium with a retro-aortic course. The SNA had 3 small pseudoaneurysms (9.6 mm, 8.5 mm, and 6.0 mm) and 1 large pseudoaneurysm (70.4 mm craniocaudally and 61.7 mm axially) with a small feeding vessel of 3.0 mm compressing the right atrium, and no thrombus was noted (Figure 1). Coronary angiography and left ventriculography illustrated normal coronary arteries and an aberrant SNA originating from the LMCA with a distal aneurysmal sac near the right atrium (Figure 2).
Figure 1.
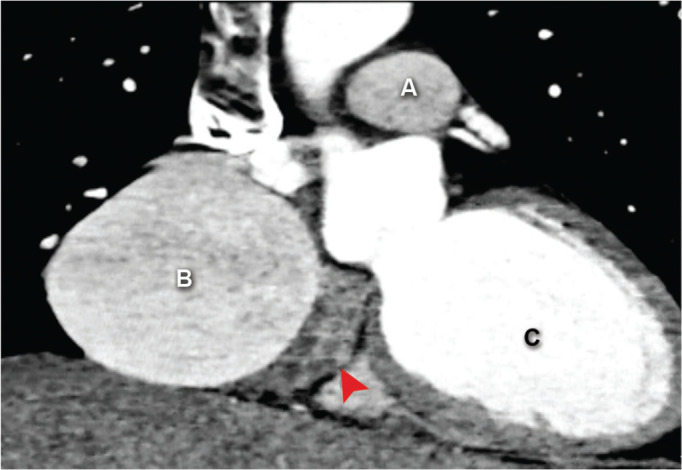
The computerized tomography of the chest with contrast in a patient with a giant sinoatrial artery aneurysm shows (arrow red), A) the descending aorta, B) a giant sinoatrial artery aneurysm compressing the right atrium, and C) the left ventricle.
Figure 2.
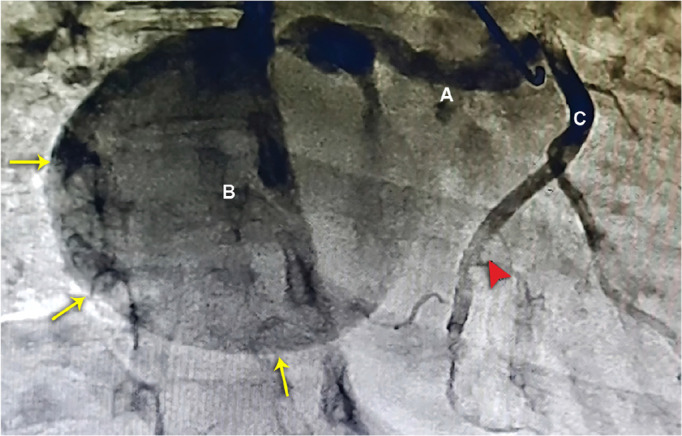
The coronary angiography in the left anterior oblique cranial view shows A) an aberrant vessel arising from the left main coronary artery, B) a giant sinoatrial aneurysm (arrows yellow), and C) the right coronary artery (arrow red).
An open-heart surgical operation was planned. The patient provided informed consent and was prepared for surgery. After all antiseptic measures were taken, a median sternotomy incision was made. A pericardiotomy visualized an aneurysmal sac, 70×70 mm in size, compressing the right atrium (Figure 3). Next, aortic and venous cannulation was done, a hypothermia of 32 ℃ was achieved, and a cardiopulmonary bypass (CPB) machine was used. Afterward, the aneurysmal sac was opened; it contained the incoming ostium of the aberrant SNA with a high-velocity flow into the sac and a second communication with the right atrium. The 2 communications were then sutured and closed with pledgeted PROLENE suture 4.0, and the other communication and the fistula between the sac and the right atrium were closed. Subsequently, the course of the feeding vessel into the aneurysmal sac was traced: it had a retro-aortic course. The vessel was tied and clipped behind the aorta. The aneurysmal sac was excised partially and then plicated. The patient was rewarmed and decannulated with a weaning-off bypass. She was extubated on the same day and had an event-free postoperative hospital course. On a 1-week follow-up, she was symptom-free and exhibited no complications. The patient was discharged home after 5 days of hospital stay.
Figure 3.
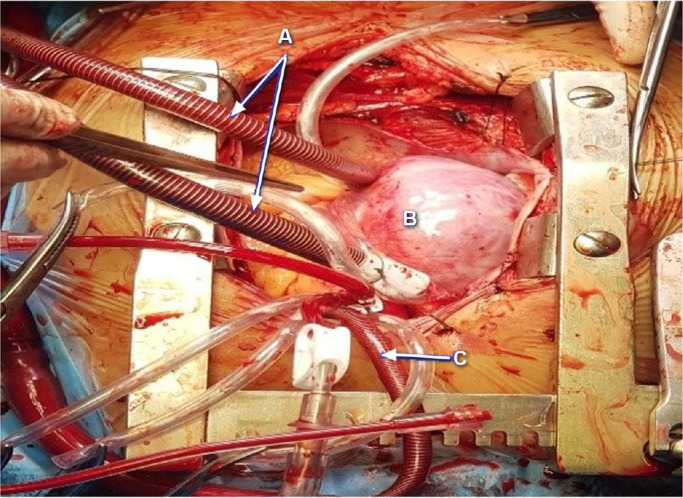
Exposure by a median sternotomy shows A) bicaval cannulation, B) a giant sinoatrial artery aneurysm, and C) aortic cannulation.
Discussion
Giant CAAs are a rare entity predominantly found in adults over the age of 60 years and are slightly more common in males than in females.2, 4 Small CAAs are often asymptomatic and may not require resection, whereas giant CAAs produce symptoms.8 Dyspnea, chest pain, and palpitations are the common symptoms of giant CAAs.4 The chances of rupture increase if the size of the aneurysm exceeds 30 mm.4, 9 In addition, the female gender, a saccular shape, and Asian ethnicity are risk factors for aneurysm rupture.9
In this case, a 46-year-old woman with no history of trauma presented with chest pain and dyspnea on exertion. Her transthoracic echocardiography revealed a round mass anterior to the right atrium, later confirmed by cardiac CT and coronary angiography as a giant CAA arising from the SNA branching off the LMCA. Open-heart surgery was done, and the aneurysm was partially resected with the plication of the arterial edges.
Giant SNA aneurysms with fistulae have been reported rarely. Hiraoka et al6 2012 reported an atherosclerotic giant SNA aneurysm with a fistulous opening into the left atrium. Huang et al7 2018 presented a case of a giant SNA aneurysm with a fistulous tract opening into the right atrium, which on histological examination of the biopsy specimen was revealed as fibrous hyperplasia. Our case of a congenital giant aneurysm of the SNA with a fistula into the right atrium is unique and is the first reported case of this nature. Indeed, we described a patient with a unique and solitary congenital SNA aneurysm branching off the LMCA who experienced symptoms of angina.
Most CAAs reported were treated surgically by placing the patient on CPB, resecting the aneurysm, and installing a bypass graft using a saphenous vein or the internal mammary artery.8 This approach hinges on achieving a stable heart rhythm and other hemodynamic parameters while occluding the coronary artery proximal to the aneurysm during the procedure. In our case, the resection of the aneurysm and the plication of the arterial margins were successfully undertaken using CPB. More favorable standardized management strategies are required to deal with CAAs.
Conclusion
The case presented herein highlights the rare occurrence of a giant SNA aneurysm with a fistula into the right atrium. Despite the high mortality rate associated with such aneurysms, our prompt intervention and successful surgical management conferred a favorable outcome. This case report serves to raise awareness among clinicians of this rare condition and highlights the significance of prompt diagnosis and surgical intervention in similar cases. Further research may provide insights into the underlying pathophysiology of such aneurysms and help optimize treatment strategies for better outcomes in affected patients.
Notes:
This paper should be cited as: Kumari U, Rahman M, Jan MU, Ullah SR, Abbas F, Shirazi Z, et al. Giant Sinoatrial Nodal Artery Aneurysm with Fistula into the Right Atrium Treated by Partial Resection and Plication: A Case Report. J Teh Univ Heart Ctr 2023;18(2):142-145.
References
- 1.Crawley PD, Mahlow WJ, Huntsinger DR, Afiniwala S, Wortham DC. Giant coronary artery aneurysms: review and update. Tex Heart Inst J 2014;41:603–608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Afzal A, Mobin S, Sharbatji M, Nawaz H, Siddiqui M. Rare Case of Giant Asymptomatic Left Coronary Artery Aneurysm of 10 cm Associated with Coronary Cameral Fistula. Cureus 2018;10:e3566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Khouzam MS, Khouzam N. Giant coronary artery aneurysms involving more than one coronary artery: case report. J Cardiothorac Surg 2021;16:177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wang L, Wang J, Cheng TO, Xie M, Wang X, Song Y, Liu J, Wei F. Giant left coronary artery aneurysms: Review of the literature and report of a rare case diagnosed by transthoracic echocardiography. Int J Cardiol 2015;189:267–271. [DOI] [PubMed] [Google Scholar]
- 5.Zelis JM, Andriessen FPJ, Elenbaas TWD, Peels KH. Giant coronary aneurysm exposed on routine echocardiogram. Eur Heart J 2017;38:3240. [DOI] [PubMed] [Google Scholar]
- 6.Hiraoka A, Kuinose M, Totsugawa T, Yoshitaka H. Giant coronary artery aneurysm arising from the sinus node artery with a fistula into the left atrium. Eur J Cardiothorac Surg 2013;43:646–648. [DOI] [PubMed] [Google Scholar]
- 7.Huang J, Zeng K, Yang Y, Zhang Y, Wang J. Sinus node artery aneurysm arising from the left main coronary artery with a fistula into the right atrium. J Card Surg 2019;34:37–40. [DOI] [PubMed] [Google Scholar]
- 8.Raut MS, Hanjoora VM, Srivastava AR, Khangarot SS, Jyoti A, Mahajan V, Rawal N. Congenital giant right coronary artery. Ann Card Anaesth 2020;23:230–231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pongbangli N, Jai-Aue S, Ketwong M, Doikean S, Wongcharoen W, Phrommintikul A. Large Aneurysmal Rupture of Coronary-Pulmonary Artery Fistula After Buffalo Goring. Am J Case Rep 2019;20:1892–1895. [DOI] [PMC free article] [PubMed] [Google Scholar]