

Abstract
Background
While research has led to significant advancements in the health and life expectancy of children with Down Syndrome (DS), there remains a significant burden of disease and health inequity. Further research, focused on areas of greatest need, is imperative to address this. An understanding of what research has been undertaken, and any existing gaps, helps to guide future academic efforts.
Methods
We utilised an epistemological approach to summarise two decades of paediatric DS literature. Publications were categorised according to the country of origin, methodology, primary health themes and subcategory research themes.
Results
Across 5,800 paediatric DS publications we demonstrate a general increase in the number of publications in this field between 2000 and 2014, with a trending decline thereafter. The majority of publications were affiliated with Institutions based in Western countries. The majority of studies utilised a cross-sectional methodology (33.3%), while relatively few were interventional (5.6%), qualitative (2.7%) or mixed-method studies (1.6%). Most publications focused on development & cognition (13.1%), neurology (9.9%) and oncology (9.8%), with fewer focusing on genitourinary health (0.9%), growth (0.9%), mortality (0.9%) and child protection (0.2%).
Conclusion
These findings highlight areas of relative paucity within the paediatric DS literature which may warrant increased academic attention.
Introduction
Research has informed significant advancements in the treatment and care of individuals with DS, and contributed to a significant increase in life expectancy over recent decades 1,2. However, individuals with DS continue to have a greater mortality and morbidity compared with both the general population, and also compared with individuals who have other forms of intellectual disability3. This demonstrates a need for ongoing research, to improve the quality of health, and duration of life for those with DS.
Existing studies have suggested a general decline in the proportion of all academic publications focusing on DS, and a shift in focus away from childhood and towards prenatal diagnostic studies.4 However, there are no existing studies which provide an overview of the existing paediatric DS literature.
Mapping of academic literature according to themes can be described as an ‘epistemological approach’. As with traditional systematic reviews, it employs a standardised, repeatable approach to select, review and synthesise the literature; however, its applications and outcomes differ. While traditional systematic reviews may address a more specific research question, a mapping exercise provides a broader overview.
A broader overview of the existing DS literature assists in identifying ‘gaps’ and areas of relative research paucity in this field. Such an understanding will help guide future DS related research, and funding allocation, in order to direct resources to the areas which are potentially most in need of academic investment.
The aims of this literature mapping exercise were to determine (i) the annual number of publications which have focused on children with DS, per year, since 2000; (ii) the geographical distribution of those publications; (iii) the current distribution of research methodologies used in the paediatric DS literature; (iv) the current distribution of ‘primary health themes’ in the paediatric DS literature; (v) the current distribution of ‘subcategory research themes’ in the paediatric DS literature; and (vi) to identify gaps in the evidence base, and thus guide future research.
Methods
Search strategy
Literature searches were performed using the online databases Pubmed, Embase.com, CINAHL-Plus and the Cochrane Library. The search terms for each database are available in Supplementary information 1. Duplicate titles were removed using Endnote X7 duplication recognition software. The resultant titles were independently screened by two authors to assess eligibility ,and only those with a unanimous decision to exclude were removed at this stage. The abstracts of the remaining titles were obtained, and independently assessed by two authors according to the inclusion / exclusion criteria (Figure 1). Discrepancies were resolved by consultation between the two reviewers and, if necessary, reviewing the full text of the papers and/ or discussing with a third reviewer from the research team. If a consensus was not reached the wider research team was consulted.
Figure 1:
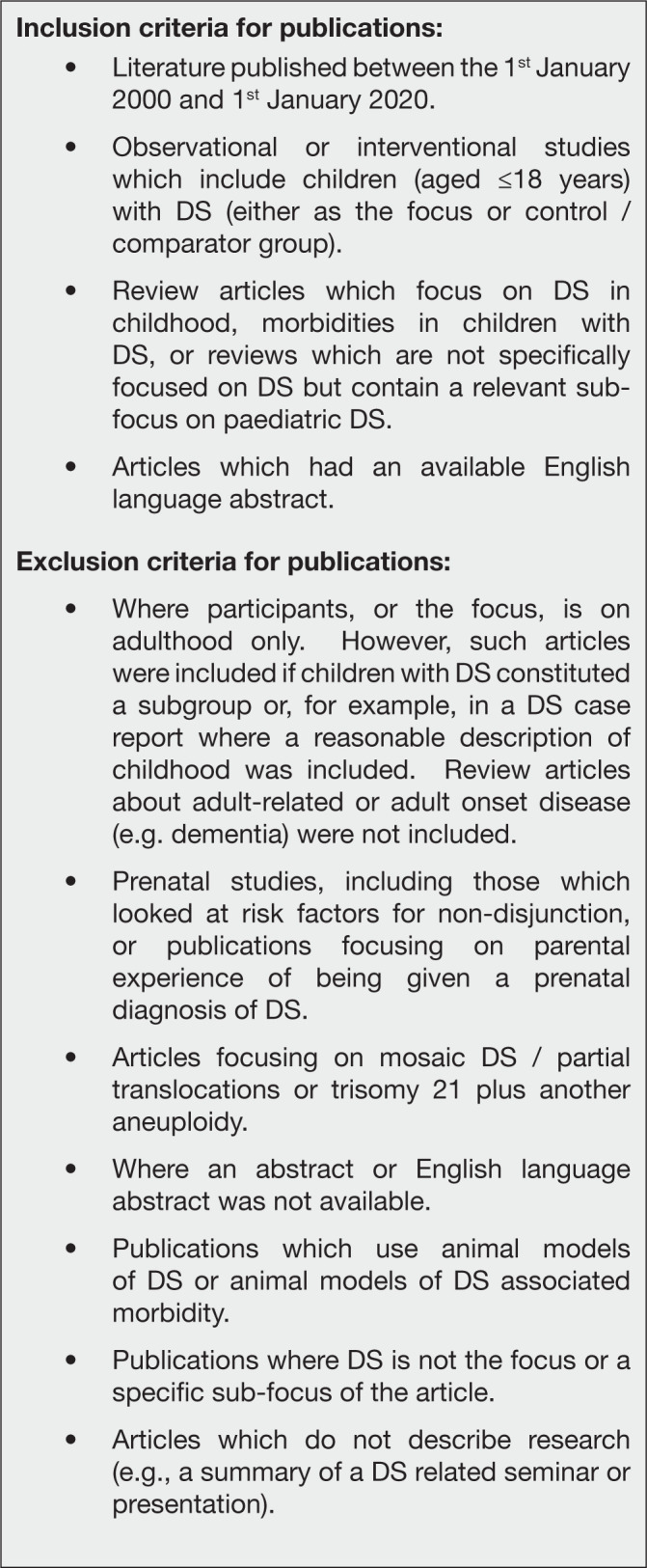
Abstract inclusion/ exclusion criteria
Each abstract was categorised according to year of publication, country of first author Institution, methodology, ‘primary health theme’ and ‘subcategory research theme’. The categories for methodology and subcategory research theme are presented in.. The ‘primary health themes’ correspond to key areas of medical research, which in turn largely correspond to clinical specialties and body/ disease systems: Behaviour/ Mental Health, Cardiac/ Circulatory, Child Protection, Dental, Dermatological, DS Prevalence Study, Development & Cognition, Endocrine, Nutrition & Metabolic, Ear, Nose and Throat (ENT), Gastrointestinal, Growth, Haematological, Infection and Immunology, Mortality, Musculoskeletal, Neurology, Non-specific/ General, Oncology, Other, Renal/ Genitourinary, Respiratory, and Surgical/ Anaesthetics.
Governance
Research Design approval was sought and obtained from the Joint Research and Development Office at the Great Ormond Street Institute of Child Health, UCL (R&D number 17PP09)
Results
Publications included/excluded
A total of 11,066 titles were downloaded from the literature databases, of which 5,800 were included in the final analysis (Figure 2).
Figure 2.
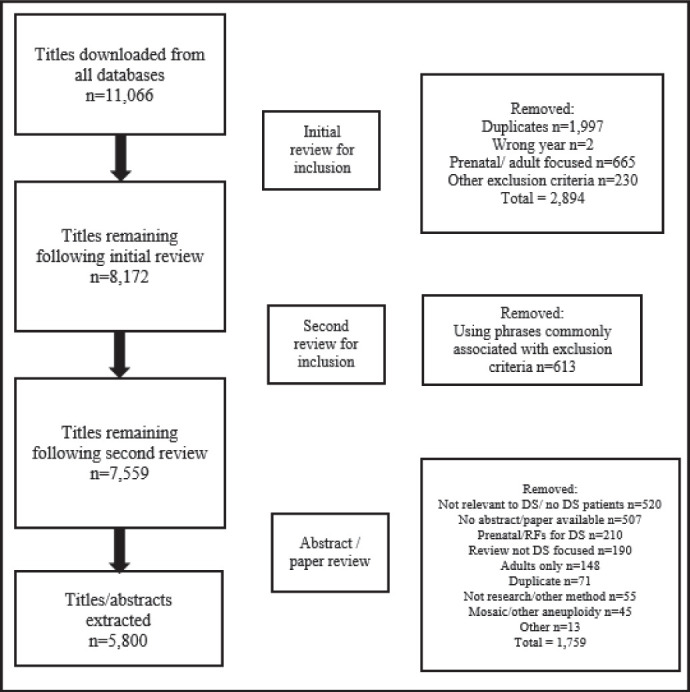
Flow chart illustrating the number of titles identified through literature searches (N=11,066) and the final number of publications which were included in the mapping exercise (n=5,800).
Number of Publications Per Year
Figure 3 summarises the number of publications per year, which were included in the final analysis. There was a general trend of an increase in the number of publications per year until 2014, and then a general trend of decline thereafter.
Figure 3:

The number of paediatric DS publications per year, Jan 1st 2000-Jan 1st 2020 (n=5,800).
Country of First Author Publication
Publications originated from institutions in 101 different countries. For 5.2% (n=304) of publications it was not possible to identify the country of first author institution. The largest proportionate contributions were from the USA and UK.
Research Methodologies
Cross-sectional studies made up the largest portion of methodologies used (33.3%, n=1,933), followed by cohort studies (15.7%, n=913) and case reports (13.7%, n=792). There were relatively few interventional studies (5.6%, n=322), basic science studies (5.5%, n=321), qualitative studies (2.7%, n=158) and those utilising mixed methods (1.6%, n=94).
Primary Health Themes
Publications focusing on development & cognition (13.1%, n=757), neurology (9.9%, n=576) and oncology (9.8%, n=569) made up the largest proportions. Relatively few publications focused on renal and genitourinary (n=53), growth (n=50), mortality (n=50) and child protection (n=10).
Subcategory Research Themes
Publications focusing on prognosis and the natural history of individuals with DS made up the largest proportion (24.9%, n= 1,445), followed by those that focused on treatments and prevention of disease (20.5%, n=1,191) and full or ‘general picture’ (e.g. case reports and case series describing a patient’s history, treatment and outcomes) (14.3%, n=831). There were relatively few publications focusing on the postnatal diagnosis of DS (n=45), economic analysis (n=15) and ethics (n=6).
Discussion
This unique systematic literature mapping exercise of 5,800 paediatric DS publications, over two decades, provides a broad overview of the existing literature.
The findings demonstrate a general increase in the number of publications focusing on paediatric DS between 2000 and 2014, with a trending decline thereafter. The majority of publications were affiliated with Institutions based in the USA and UK. The majority of studies utilised a crosssectional methodology, while relatively few studies were interventional, qualitative or mixed method. The distribution of ‘primary health themes’ in the paediatric DS literature was more spread. Overall, most publications focused on development & cognition, oncology and neurology, with fewer focusing on genitourinary health, growth, mortality and child protection. With regard to ‘subcategory research themes’, the majority of paediatric DS publications focused on prognosis and/or the natural history of individuals with DS, and treatments.
The literature mapping exercise was performed using a systematic approach. Relevant titles were extracted from multiple medical literature databases and the search terms were highly inclusive. The definitions used for methodologies and ‘themes’ were based on those frequently utilised in research. These definitions were refined to optimise applicability to the paediatric DS literature and trialled by multiple researchers, reaching a high degree of consensus. The assessment for inclusion and exclusion of all titles, and subsequent data extraction for those publications, was performed by two independent reviewers and discrepancies were resolved by discussion with a third reviewer, or the wider research team where appropriate.
While this systematic approach reflects a high degree of academic rigor, it is possible that some titles may still have been misclassified. However, given the large number of publications included in the mapping exercise infrequent misclassifications would not be expected to significantly impact the overall findings.
It should be noted that for the majority of publications, categorisation was based on the contents of the abstract only, as opposed to review of the full text publication. However, where the methodology or ‘themes’ were unclear, and in the case of reviewer discrepancy, the full-text was consulted. It is possible that in some cases the content of the abstract was a poor reflection of the study, thus leading to misclassification. However, extracting data largely from abstracts had the advantage of making it possible to include a larger number of publications, over a longer time period, than would have been practical if the full text article was consulted for every paper.
This is the first study which attempts to map paediatric DS literature.5 Venekamp et al. employed a similar ‘epistemological approach’ to map 5 years of literature focusing on obstructive sleep apnoea in childhood (non-DS). In this field they too found a predominance of publications focusing on treatment and prognosis, and few publications focusing on service delivery and health economics. Also reflecting the findings of this mapping exercise, the majority of the studies utilised an observational methodology, with very few interventional or qualitative studies.5
The general trend of an increased number of publications focusing on paediatric DS per year, over the majority of the study period (2000-2014), is somewhat promising (146 per year, to 450 per year). However, the number of publications should be considered in the context of all research articles published over the same time period. As has previously been illustrated,4 while there may have been an increase in the number of DS research publications over time (not limited to paediatric DS), there has been a proportionate decline, relative to all academic publications. This suggests that DS is receiving relatively less academic focus and attention.
Table 1:
Methodological categories and definitions
The definitions of the research methodologies are based upon those presented in the A Dictionary of Epidemiology(Porta, 2014), the (National Institute for Health Research) NIHR Glossary, Evaluation, Trials and Studies(NIHR, 2016) and research group consensus.
| Aetiology / risk factors for DS associated morbidities | The study aims to identify factors which may be associated with the development of DS associated morbidity. This also includes studies where DS is a risk factor for a disease or a specific outcome. |
| Prevalence/ incidence of DS associated morbidities | The study aims to determine the number of individuals with a DS associated morbidity, or health event, in a defined population, within a specified period of time. Also includes studies where the prevalence of DS is described in a disease subgroup. |
| Prevalence/ incidence of DS | The study aims to determine the prevalence/ incidence of DS within a defined population (e.g. geographical). If the study determines the prevalence of DS in a disease subgroup this should be defined as Prevalence/ incidence of DS associated morbidities. |
| Diagnosis / health surveillance for DS associated morbidities | The study focuses on the diagnosis of/health surveillance for DS associated morbidities. |
| Diagnosis of DS (postnatal) | The study aims to determine the accuracy of diagnosis of DS in a post-natal population (e.g. comparing clinical diagnosis with molecular diagnosis). |
| Treatment (including Rx outcomes)/ prevention | The study focuses on a treatment/intervention that aims to improve the health or well-being of a patient(s) with DS, or to prevent associated morbidities. It includes studies which look at outcomes of treatments/interventions. This definition does not include studies which look at the outcomes of health service interventions, i.e. interventions which target the way in which health care is organised or functions (see Service delivery). |
| Prognosis / Natural history of DS | The study aims to describe/inform/further the knowledge base on the natural course of DS, or a morbidity in the context of DS. This includes studies which aim to define ‘normality’ or normative values within the DS phenotype. This definition also includes studies which further the knowledge base on the development of the DS phenotype, but does not include studies which focus on the aetiology or risk factors for DS associated morbidities (see Aetiology / risk factors for DS associated morbidities). Where the focus is on prevalence (proportion, rate, count) of an associated morbidity, these should be classified as Prevalence/ incidence of DS associated morbidities). (Note these are usually crosssectional studies). This definition does not include studies which focus on the outcomes of treatments/interventions (see Treatment (incl Rx outcomes)/prevention). |
| Economic analysis | The study focuses on the economic evaluation (e.g. cost-benefit) of services, interventions or treatments. |
| Family impact | The study focuses on the impact of DS on any aspect of family life, including familial experiences and perceptions. However, those studies with a prenatal focus should not be included (see Inclusion/ Exclusion criteria). |
| Service delivery | The study focuses on the organisation, functioning, and performance of health services relevant to those with DS. Such research is usually concerned with relationships between needs, demand, supply, use, and outcomes of health services. |
| Ethical issues | The study primarily focus on ethics or ‘moral principles’. This does not include publications which focus on the ethics of prenatal diagnosis or terminations, these studies should be excluded. |
| Outcome research | The study assesses the validity / reliability of specific outcome measures such as (generic or disease specific) quality of life instruments and the inter-reliability of diagnostic tests. |
| Full/ general picture | Typically case reports, case series or review articles which include multiple health and ‘subcategory research themes’. |
| Other | Those studies not clearly covered by other definitions. |
Table 3:
Paediatric DS publications according to country of first author institution, limited to those countries contributing ≥1% of the total (N=4,923).
| Country of 1st author institution | n= | % |
|---|---|---|
| USA | 1,535 | 26.5 |
| UK | 450 | 7.8 |
| Italy | 322 | 5.6 |
| Unknown | 304 | 5.2 |
| Japan | 295 | 5.1 |
| Brazil | 259 | 4.5 |
| Spain | 204 | 3.5 |
| India | 195 | 3.4 |
| Canada | 184 | 3.2 |
| The Netherlands | 169 | 2.9 |
| Turkey | 167 | 2.9 |
| Australia | 160 | 2.8 |
| Germany | 133 | 2.3 |
| France | 117 | 2.0 |
| Israel | 86 | 1.5 |
| Saudi Arabia | 77 | 1.3 |
| Poland | 75 | 1.3 |
| Sweden | 68 | 1.2 |
| China | 65 | 1.1 |
| Ireland | 58 | 1.0 |
| Total (N=5,800) | 4,923 | 84.9 |
The trend of decline in the number of publications focusing on paediatric DS from 2014-2020 noted in this study may represent a shift in focus away from childhood studies and towards the prenatal period. This follows significant advancements in the prenatal diagnosis of DS via non-invasive techniques over recent years.4,6 Research focusing on the prenatal diagnosis of DS does not inform improvements in the health and care of live-born children with DS. The findings of this study provide support for a “rebalancing” of focus in DS research, by increasing investment in studies which aim to improve the health and well-being of children, and adults, with DS.
Table 4:
Paediatric DS publications according to methodology (%) (N=5,800).
| Methodology | n= | % |
|---|---|---|
| Cross-sectional study | 1,933 | 33.3 |
| Cohort study | 913 | 15.7 |
| Case report | 792 | 13.7 |
| Review (combined)* | 512 | 8.8 |
| Case control study | 363 | 6.3 |
| Case series | 328 | 5.7 |
| Interventional study / Trial | 322 | 5.6 |
| Basic science/ underpinning | 321 | 5.5 |
| Qualitative study | 158 | 2.7 |
| Mixed methods | 94 | 1.6 |
| Other* | 64 | 1.1 |
| Total= | 5800 | 100 |
Publications categorised as guidelines, opinion pieces and letters to the editor were combined as “Other”. Systematic and ‘unspecified’ review articles were combined into one category (Review (combined)).
Academic institutions in the UK, and particularly the USA, appear to dominate paediatric DS publications. This may be a recurrent pattern in the wider field of research and academia. However, the over-representation of research from certain regions, where the population is predominantly White and ‘high income’, may limit the generalisability of findings in paediatric DS research. Therefore, these findings provide some support for investment in research which includes patient groups which are likely under-represented in the paediatric DS literature (e.g. low resource settings, non-white ethnicity).
The mapping exercise also demonstrates a predominance of observational studies (cross-sectional, cohort and case control studies, case reports and case series). In particular, there were a large number of case reports (13.7% of publications). While case reports make a valuable contribution to research literature they are considered further down the ‘hierarchy of evidence’. Robust, large-scale interventional studies will be required to advance the evidence-based healthcare of children with DS. These findings support increased investment in interventional studies aimed at children with DS.
The study findings also highlight a relative paucity of qualitative and/or mixed method studies. Improving healthcare for children with DS requires, not only a quantitative approach, but also an understanding of the experience of the child and family. Qualitative research is ideal to identify areas of health priority for patients and carers, and also to identify opportunities to optimise their interactions with the healthcare system.
Looking at ‘primary health themes’, the distribution of categories was more evenly spread than that observed for the other outcomes. The ‘primary health themes’ which appeared to receive the greatest attention are not surprising and reflect important, well established areas of DS child health (i.e. development & cognition, neurology and oncology). However, it is notable that relatively few publications focus on respiratory health, infections and immunological disease, as these are recognised as significant causes of mortality and morbidity in children with DS.1,7 The findings of this study support investment in these areas of DS child health, as well growth, mortality and child protection, as these health themes appear to have received the least attention in the existing paediatric DS literature.
Table 5:
Paediatric DS publications according to ‘primary health themes’ (%) (N=5,800).
| Primary health theme | n= | % |
|---|---|---|
| Development & Cognition | 757 | 13.1 |
| Neurology | 576 | 9.9 |
| Oncology | 569 | 9.8 |
| Other | 518 | 8.9 |
| Cardiac/ Circulatory | 468 | 8.1 |
| Endocrine, nutrition, metabolic | 383 | 6.6 |
| Musculoskeletal | 366 | 6.3 |
| Behaviour / Mental health | 351 | 6.1 |
| Ear, Nose & Throat (ENT) | 303 | 5.2 |
| Gastrointestinal | 247 | 4.3 |
| Dental | 228 | 3.9 |
| Infection & Immunology | 204 | 3.5 |
| Surgical/ anaesthetics | 194 | 3.3 |
| Respiratory | 118 | 2.0 |
| DS prevalence study | 106 | 1.8 |
| Dermatological | 88 | 1.5 |
| Haematological | 82 | 1.4 |
| Non-specific, general | 79 | 1.4 |
| Renal, genitourinary | 53 | 0.9 |
| Growth | 50 | 0.9 |
| Mortality | 50 | 0.9 |
| Child protection | 10 | 0.2 |
| Total = | 5,800 | 100 |
Finally, with regard to ‘subcategory research themes’, the majority of publications described the natural history of children with DS (i.e. they aimed to define normality or normative values within the DS phenotype, or to further the knowledge base on the development of the DS phenotype over time). For example, studies determining the average lipid profiles among individuals with DS, the typical trajectory of speech and language development in children with DS, or average activity levels among teenagers with DS. While it is valuable to understand normative health characteristics in the DS population the findings suggest that, more than 150 years since the condition was first described, the natural history of individuals with DS is relatively well documented. The findings of this study support investment in other areas of DS research which appear relatively under-represented e.g. the diagnosis of and screening for DS associated morbidities, service delivery and economic analyses.
Table 6:
Respondent Demographics
| Subcategory research theme | n= | % |
|---|---|---|
| Prognosis / natural history of DS | 1,445 | 24.9 |
| Treatment (including outcomes) / prevention | 1,191 | 20.5 |
| Full / general picture | 831 | 14.3 |
| Prevalence/ incidence of DS associated morbidities | 592 | 10.2 |
| Aetiology / risk factors for DS associated morbidities | 561 | 9.7 |
| Diagnosis / health surveillance for DS associated morbidities | 301 | 5.2 |
| Family impact / parent experience | 228 | 3.9 |
| Other | 202 | 3.5 |
| Service delivery | 138 | 2.4 |
| Outcome research | 125 | 2.2 |
| Prevalence/incidence of DS | 120 | 2.1 |
| Diagnosis of DS (postnatal) | 45 | 0.8 |
| Economic analysis | 15 | 0.3 |
| Ethical issues | 6 | 0.1 |
| Total= | 5,800 | 100.0 |
Footnotes
UMJ is an open access publication of the Ulster Medical Society (http://www.ums.ac.uk).
REFERENCES
- 1.Bittles AH, Bower C, Hussain R, Glasson EJ. The four ages of Down syndrome. Eur J Public Health. 2007;2007;17(2):221–5. doi: 10.1093/eurpub/ckl103. [DOI] [PubMed] [Google Scholar]
- 2.Penrose LS. The incidence of mongolism in the general population. J Ment Sci. 1949;95(400):685–8. doi: 10.1192/bjp.95.400.685. [DOI] [PubMed] [Google Scholar]
- 3.Coppus AM. People with intellectual disability: What do we know about adulthood and life expectancy? Dev Disabil Res Rev. 2013;18(1 Special Issue):6–16. doi: 10.1002/ddrr.1123. [DOI] [PubMed] [Google Scholar]
- 4.Manikam L., et al. “G366 Mapping research on the management of children and adults with down’s syndrome: A systematic review of UK and ROI research and published outputs 1990-2015.”. (2016):A214–A215. [Google Scholar]
- 5.Venekamp RP, Chandrasekharan D, Abel F, Blackshaw H, Kreis IA, Evans HE, et al. Research into childhood obstructive sleep-disordered breathing: a systematic review. Chest. 2017;152(1):51–7. doi: 10.1016/j.chest.2016.12.001. [DOI] [PubMed] [Google Scholar]
- 6.Palomaki GE, Kloza EM, Lambert-Messerlian GM, Haddow JE, Neveux LM, Ehrich M, et al. DNA sequencing of maternal plasma to detect Down syndrome: an international clinical validation study. Genet Med. 2011;13(11):913–20. doi: 10.1097/GIM.0b013e3182368a0e. [DOI] [PubMed] [Google Scholar]
- 7.Day SM, Strauss DJ, Shavelle RM, Reynolds RJ. Mortality and causes of death in persons with Down syndrome in California. Dev Med Child Neurol. 2005;47(3):171–6. doi: 10.1017/s0012162205000319. [DOI] [PubMed] [Google Scholar]