

Abstract
This study examines how population aging will shape a crucial aspect of mental health and social well-being – loneliness. Drawing on theories of demographic metabolism, United Nations’ population estimates and projections, and survey data covering approximately 50% of the world’s population aged 50 and above living in 27 countries, we estimate the role of population aging in shaping cross-national differences in loneliness from 1990 to 2050. We use survey data to estimate the prevalence of late middle age and older adult loneliness by age and sex, and then apply these rates to the evolving age and sex distributions of the populations. Our results highlight massive increases in loneliness at ages 50 and above with a tripling of the number of lonely adults in these age groups in our sample countries from 104.9 million in 1990 to 333.5 million in 2050, increasing variability across countries in the share of their populations composed of lonely adults 50 and above, and the feminization of global later life loneliness with an increasing share of lonely adults in these age ranges being women. These results illustrate the power of demographic modeling to advance understandings of national profiles of mental health and social well-being.
Introduction
Population aging is reshaping societies around the world. As a diverse and growing set of countries age rapidly, demographers have highlighted population aging’s influence on economic trajectories (Bongaarts, 2004; Lee & Mason, 2010, 2011) and caregiving pressures (Agree & Glaser, 2009). Population aging can also reshape national health profiles around the world, leading to increasing numbers of late middle age and older adults, adults over the age of 50, in poor physical health (De Meijer et al., 2013). However, an overlooked aspect of the relationship between population aging and health is what population aging implies for mental health and social well-being at the population level, and how it might create new social pressures in these domains. Like physical health, mental health is included in the World Health Organization’s encompassing definition of health, “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” (World Health Organization, 2021). Additionally, mental health is a critical determinant of other, better-studied ramifications of population aging like economic productivity, caregiving capacities, and physical health (Bloom et al., 2012; Prince et al., 2007; World Health Organization, 2013).
Loneliness is a crucial component of mental health and social well-being that has sparked abundant policy attention in recent years. Loneliness occurs when individuals assess that their social networks are lacking or deficient in some manner, whether in size or quality of connections (De Jong Gierveld, 1989; Perlman & Peplau, 1981; Weiss, 1973). Loneliness is a strong predictor of mental health problems such as depression (Cacioppo et al., 2006; Domènech-Abella et al., 2019; Heikkinen & Kauppinen, 2004), anxiety (Domènech-Abella et al., 2019), and psychological distress (Hawkley et al., 2003; Stickley et al., 2013). Loneliness also leads to unhealthy behaviors such as smoking and alcohol consumption (Stickley et al., 2013), chronic conditions such as hypertension (Hawkley et al., 2006), stroke (Valtorta et al., 2016), metabolic syndrome (Whisman, 2010), cognitive conditions such as Alzheimer’s disease (Wilson et al., 2007), and even increased mortality risk (Holt-Lunstad et al., 2010; Lara et al., 2020; Stokes et al., 2021; Takagi & Saito, 2020).
Research on what predicts loneliness tends to focus on the individual level, finding it is associated with small social networks (Ayalon et al., 2013), poor physical health (Aartsen & Jylhä, 2011), and living alone (De Jong Gierveld et al., 2012). Two core demographic variables, being female (Aartsen & Jylhä, 2011; Dykstra et al., 2005; Nicolaisen & Thorsen, 2014) and older age (Dykstra, 2009; Nicolaisen & Thorsen, 2014; Victor & Yang, 2012), are also critical predictors of loneliness. Cross-national differences in mental health are a prominent area of research (Kessler et al., 2009; Vigo et al., 2016; Whiteford et al., 2015), but, to date, few studies have considered cross-national differences in loneliness (an exception is Newmyer et al., 2021), and those that have focus on variation within Europe (Fokkema et al., 2012; Nyqvist et al., 2019; Rico-Uribe et al., 2016; Stickley et al., 2013; Sundström et al., 2009; Yang & Victor, 2011). Most research relegates demographic drivers of mental health to control variables, and no studies of which we are aware consider whether demographic changes could be driving changes in the prevalence of poor mental health symptoms.
Demographers are well-positioned to revolutionize understandings of cross-national differences at the intersections of mental, social, and physical well-being because most research on these topics focuses on non-demographic explanations of variation, such as institutional, economic, and cultural differences (Fokkema et al., 2012; Höllinger & Haller, 1990), or even measurement errors (Newmyer et al., 2021). A demographic understanding of national loneliness profiles would begin with the theory of demographic metabolism (Lutz, 2013; Lutz & KC, 2011; Lutz & Muttarak, 2017), which posits that “societies change as a consequence of the changing composition of their members with respect to certain relevant and measurable characteristics… This is a theory predicting aggregate-level change rather than individual behavior” (Lutz, 2013, p. 283). The approach “is not primarily intended to explain and forecast demographic variables (such as population size, birth and death rates, and the like); rather, the goal is to predict socioeconomic change in a broader sense (e.g., values, religions, skills, and productivity of the workforce) using a demographic paradigm” (Lutz, 2013: pp.283–284). However, in contrast to demographic determinism, demographic metabolism theory does not assume that populations cannot adapt to environmental and social changes and innovations (such as those that made deterministic predictions in the 1960s inaccurate; see Lam, 2011). Nor does it infer that cohorts are completely determined where individuals have no flexibility, thus resulting in a “stagnant pond” of individuals in a population (Ryder, 1980). The idea is to assess the implications of demographic change given a series of assumptions, which scholars can use to draw boundaries around possible futures and reframe questions about future change: for instance, how much would remarriage rates have to change to meaningfully shrink the rapidly growing pool of divorced older adults (Verdery et al., 2019). Applications of demographic metabolism have ranged from studying aggregate changes in education and the stock of human capital (Lutz, 2013; Lutz & KC, 2011), Europeans with pan-European identities (Lutz, 2013; Striessnig & Lutz, 2016), attitudes toward same-sex relationships (Lutz & Striessnig, 2016), adaptive capacities to climate change (Lutz, 2013; Lutz & Muttarak, 2017), older adult family composition (Verdery & Margolis, 2017; Verdery, 2019), “super diversity” in terms of language and religious composition (Bélanger et al., 2019), and immigrant workforce dynamics in terms of literacy (Vézina & Bélanger, 2019; Vézina et al., 2019). To date, the theory of demographic metabolism has not made substantial inroads into the study of health, particularly as it relates to mental health.
For late middle age and older adult loneliness, a demographic understanding of national loneliness profiles would examine how loneliness varies according to age and sex structures and whether changes in these demographic factors can explain changes in loneliness prevalence at the aggregate level. What is particularly exciting about a demographic consideration of cross-national differences in mental health is that it can offer grounded projections of how national mental health profiles will change in the coming decades under certain assumptions. Specifically, to the extent that the same age and sex structures (absent cohort distinctions) for which we have numerous high-quality projections determine mental health prevalence, if we can assume that such determination continues, we can develop an understanding of the demographic metabolism of mental health. Armed with these, we can explore relaxing the assumption of stability in the age- and sex- patterns to see how much they would need to change to override the demographically implied trends. These contributions are important because they contextualize present cross-national differences in standardized terms, offer a baseline against which to judge future developments, and highlight the need for policy planning in different contexts. Put simply, if population aging will drastically alter national loneliness profiles in the coming decades, and big changes in possible associations between loneliness and demographic variables do not override such implied trends, these findings should compound concerns about population aging’s antecedent health, social, and economic impacts.
The Current Study
We focus on late adulthood because late middle age and older adults have unique circumstances that elevate loneliness risks (B. Cornwell et al., 2008; Dykstra et al., 2005; Nicolaisen & Thorsen, 2017; Ong et al., 2016; Rico-Uribe et al., 2016) and are a core policy concern in many countries (Gerst-Emerson & Jayawardhana, 2015; Prohaska et al., 2020; Yeginsu, 2018), and can be studied with high-quality, harmonized cross-national survey data (https://g2aging.org/). We ask how population aging has influenced both the prevalence of late middle age and older adult loneliness and the number of lonely adults in these age ranges in a wide range of countries in recent decades, and how it will reshape this landscape in coming decades. To accomplish these goals, we use harmonized, cross-national data from countries in the Americas, Europe, and Asia that contain about half of the world’s population of people over the age of 50. We first assess the prevalence of late middle age and older adult loneliness and its associations with age and sex in each country, including whether age differences owe to cohort variation. These analyses highlight the extent to which late middle age and older adult loneliness is determined by age and sex, with limited cohort variation, and thus that population prevalence of late middle age and older adult loneliness is amenable to modeling as a function of demographic metabolism. Building on these analyses, we then combine each studied country’s age- and sex- profiles of loneliness with United Nations historical and projected estimates of national age and sex profiles (United Nations, 2019) to examine the potential for demographically-induced changes in loneliness prevalence. Our analyses demonstrate how national profiles of loneliness in late middle age and older adulthood have changed and could change in different countries due to population aging, drawing attention to the potential for demographic metabolism modeling to contribute to understandings of cross-national mental health changes.
Demographic Predictors of Loneliness
The core demographic variables, age and sex, do not cause loneliness, but they are strong predictors of the factors that do, especially for late middle age and older adults. This situation is not that different from other topics familiar to demographers, like fertility, which is associated with age but is instead shaped by social roles (e.g., marriage) and biological factors (e.g., fecundity) that are so age-graded that fertility can be amenably modeled as a function of age.
Research on the age pattern of loneliness highlights a U-shaped curve over the life course, where adults age 18–29 have high levels of loneliness, which then decrease into middle age, before increasing again in later life starting around age 65 (Nicolaisen & Thorsen, 2014). Young adults generally have high levels of loneliness because of low satisfaction with the size of their social networks, but late middle age and older adults are often lonely due to the loss of friends, colleagues, and family members (Nicolaisen & Thorsen, 2014, 2017; Victor & Yang, 2012). Some argue that loneliness is relatively stable throughout old age (Victor & Bowling, 2012), but a larger body of scholarship suggests that it tends to increase among the oldest old (Dahlberg et al., 2015; Dykstra et al., 2005; Heikkinen & Kauppinen, 2004). These studies all focus on one European country such as Great Britain (Victor & Bowling, 2012), Sweden (Dahlberg et al., 2015), the Netherlands (Dykstra et al., 2005) or Finland (Heikkinen & Kauppinen, 2004).
Other age-related factors that predict late middle age and older adult loneliness include partnership status (Aartsen & Jylhä, 2011; Dahlberg et al., 2018; Dykstra et al., 2005; Morgan & Burholt, 2020; Nicolaisen & Thorsen, 2014) and major life transitions like retirement (Suanet & Huxhold, 2020). Adults over the age of 50 whose networks extend beyond family tend to report fewer feelings of loneliness than their counterparts with smaller networks (Dykstra et al., 2005; Mair, 2010, 2019). However, as adults in their 50s and older age, their networks become primarily composed of family members rather than acquaintances or friends (Ajrouch et al., 2005; Antonucci & Akiyama, 1987; B. Cornwell et al., 2008; Fredrickson & Carstensen, 1990). Dense family-structured networks may provide adequate resources and care to those with close relationships, but such networks can be detrimental for those who do not have close relationships with their family members (Takagi & Saito, 2020) or those with family members occupied with their own lives (Ajrouch et al., 2005). Additionally, as individuals age, the odds of key family members dying rise (Nicolaisen & Thorsen, 2017). Limited mobility and social participation, often hallmarks of the disabilities and chronic conditions that beset many late middle age and older adults, are also strong predictors of loneliness (Dahlberg et al., 2015; Macdonald et al., 2018; Paul et al., 2006).
Research finds strong associations between loneliness and sex. Although research shows this link between sex and loneliness, many of these differences are likely a function of gender as determinants of loneliness are generally social in contrast to biological.1 Women tend to report being lonelier than their male counterparts (Aartsen & Jylhä, 2011; Dykstra et al., 2005; Nicolaisen & Thorsen, 2014), part of a long-recognized tendency for women to report higher rates of depressive symptoms in all manner of contexts (Weissman et al., 1993). This sex disparity may owe to men being less likely to admit feelings of loneliness in surveys than women (Nicolaisen & Thorsen, 2014). Another contributor to these patterns is different dimensions of loneliness and how they vary across the sexes. Men may be more socially lonely than women meaning they have fewer social contacts, which evidence suggests is true for people of comparable ages (Cornwell et al., 2008); in contrast, women may be more emotionally lonely than men, meaning they are more likely to identify feelings of loneliness (Nicolaisen & Thorsen, 2014). Even if men have fewer contacts than women at a given age, however, compositional differences in the population over the age of 50 may make women lonelier overall. For instance, women may also be at a greater risk of loneliness than men due to living longer and their greater likelihoods of being widowed (Dahlberg et al., 2015; Nicolaisen & Thorsen, 2014) and living alone (Reher & Requena, 2018).
Sex differences in the structure of social networks may also contribute to sex differences in late middle age and older adult loneliness. Women may experience more structural changes to their social networks over the life course than men. Older women tend to have smaller social networks than middle-aged women (Ajrouch et al., 2005), which could induce a sense of loss that leads to loneliness. In contrast, men’s network structures vary less across the life course (Ajrouch et al., 2005). Women’s roles as “kin keepers” and the normative centrality of children in women’s lives (Hagestad, 1986) may contribute to these associations. Retirement, a life transition that late middle age and older adult men are more likely than women to experience (owing to higher employment among men than women), may temporarily increase a retiree’s number of social connections (Suanet & Huxhold, 2020) and retirees are increasingly retaining work-related relationships into retirement (Cozijnsen et al., 2010). These differences in network structure may offer men more protection against loneliness in late middle age and older adulthood than they do for women.
Although most research on loneliness focuses on individual-level predictors of loneliness, a small number of studies examine its cross-national variation. Countries may have different relationships between loneliness and demographic variables such as age and sex, as national differences in factors such as retirement ages (Saure & Zoabi, 2011), health conditions (Verdery et al., 2021), and the size and shape of social networks (Mair, 2019). Additionally, considerations such as built environments (e.g., reliance on driving), social norms (e.g., expectations of family solidarity), and other geographic factors may also feed into differences in loneliness. Prior cross-national studies of loneliness primarily focus on the differences in prevalence levels between contemporary European countries (Fokkema et al., 2012; Nyqvist et al., 2019; Rico-Uribe et al., 2016; Stickley et al., 2013; Yang & Victor, 2011). Within Europe, loneliness is geographically patterned, with higher levels in Eastern than Western Europe (De Jong Gierveld et al., 2012) or Northern Europe (Nyqvist et al., 2019; Yang & Victor, 2011). Loneliness is also more prevalent in Southern Europe than Northern Europe (Dykstra, 2009; Fokkema et al., 2012). Most ascribe these differences to social policies (Nyqvist et al., 2019) and the tension between familistic norms and reality (Dykstra, 2009). Late middle age and older adults in Northern European countries, often characterized as highly individualistic places (Reher, 1998), may be less lonely than those in Southern Europe because it is more common to live alone there (Dykstra, 2009). However, it is unclear how levels of loneliness in contexts such as East Asia might compare to those in Europe. For instance, East Asian countries like the Republic of Korea have rapidly aging populations and familistic values that might place them at an increased risk of experiencing high levels of loneliness in their populations, but, conversely, late middle age and older adults in the Republic of Korea tend to be in good health and thus less mobility-restricted (Verdery et al., 2021), which may predict low levels of loneliness.
Population Aging and Changes in Loneliness
It remains an open question whether population aging will influence the population prevalence of late middle age and older adult loneliness, and it is not entirely predictable how such influences might play out across countries. There are two relevant factors: the country-specific pace of population aging – including dynamics in the distribution of the age-sex structure among those over 50 years old, not just the mean age – and each country’s age-sex pattern of adult loneliness in these age ranges. These factors contribute to prevalence levels by shaping important aspects such as the number of lonely late middle age and older adults, as well as sex differences in loneliness.
Over the next several decades, there will be uneven rates of aging across countries (United Nations, 2019). According to the UN World Population Prospects, in 2020, the two countries with the largest share of the population over age 65 were Japan (28.4%) and Italy (23.3%); in 2050, the Republic of Korea (38.1%) and Japan (37.7%) will be the world’s oldest populations, but 28 other countries will have populations with a greater percentage of the population above 65 than Japan does today. Even countries with comparatively small shares of late middle age and older adults today, like Saudi Arabia (3.5% to 17.2%) or Indonesia (6.3% to 15.9%), are expected to see rapid aging in the coming decades. Both the rate of population aging and the age pattern of loneliness will uniquely continue to shape the population level prevalence of loneliness of countries. For example, Greece and Italy both have rapidly aging populations whose aging patterns are comparable, with Greece going from 22.3% to 36.2% and Italy going from 23.3% to 36.0% of their populations older than age 65 between 2020 and 2050 (United Nations, 2019), but they have very different levels of late middle age and older adult loneliness today (Newmyer et al., 2021).
How population aging will interact with country-specific age-sex patterns of loneliness is challenging to predict. To illustrate a few scenarios, Table 1 presents a highly stylized example that focuses on three hypothetical countries: A, B, and C (the bottom row offers notation we refer to here). We show trends in aging in each of these countries at two time points (columns with notation and ). In the first period () there are stark differences in the share of each population’s late middle age and older adults that is in the oldest old category: B has twice as many oldest old individuals as A, and C has three times as many. By the second period (), these differences have waned, but the rank order remains. We also show a hypothetical categorical age difference in loneliness prevalence (columns with notation and ), which here is assumed to be constant over time. In all three countries, loneliness prevalence is twice as high among the oldest old individuals () as it is among the younger set (), but the baseline rates differ by country such that A has the highest loneliness levels at each age, followed by C, then B.2 What does this example reveal? Even though it is quite simple to calculate the expected loneliness in each time period (the bottom row gives the resultant calculations), which we present in the table’s rightmost columns, this example highlights the need to consider the complexities of population aging to better understand how societies’ prevalence of loneliness might change in response to population aging in the coming decades. In the remainder of this article, we pursue such computations.
Table 1.
Hypothetical Example of Population Loneliness and Population Aging
| Trends in aging (% oldest old) | Age curve of loneliness (% lonely by age) | Expected loneliness (% lonely by time) | ||||
|---|---|---|---|---|---|---|
| Time 1 | Time 2 | Younger older adults | Oldest old adults | Time 1 | Time 2 | |
| Country A | 20% | 50% | 30% | 60% | 36% | 45% |
| Country B | 40% | 60% | 10% | 20% | 14% | 16% |
| Country C | 60% | 70% | 25% | 50% | 40% | 43% |
| Notation/Calculation | ||||||
Materials and Methods
Data
We study population aging’s influence on late middle age and older adult loneliness using multiple international studies, which allows us to evaluate and compare various countries from diverse regions (https://g2aging.org/). We draw on nine surveys collectively covering 27 countries around the world that contain an estimated 48.5% of the current global population over 50. These studies are the Chinese Health and Retirement Longitudinal Survey (CHARLS), the English Longitudinal Study of Aging (ELSA), the Health, Aging, and Retirement in Thailand (HART) study, the U.S. Health and Retirement Study (HRS), the Indonesia Family Life Survey (IFLS), the Korean Longitudinal Survey of Aging (KLoSA), the Mexican Health and Aging Study (MHAS), and the Survey of Health, Aging and Retirement in Europe (SHARE),3 and the Irish Longitudinal Study on Aging (TILDA). We select these surveys because they are “International Sister Studies” of the Health and Retirement Study (HRS; https://hrs.isr.umich.edu/about/international-sister-studies).4 These data sets cover the following countries: Austria, Belgium, China, Croatia, the Czech Republic, Denmark, England, Estonia, France, Germany, Greece, Ireland, Indonesia, Israel, Italy, Luxembourg, Mexico, the Netherlands, Poland, Portugal, the Republic of Korea, Slovenia, Spain, Sweden, Switzerland, Thailand, and the United States. With weights, these data are nationally representative of each corresponding country, but in two of them (Ireland and Thailand) we do not have access to the weights.5 All the surveys cover late middle age and older adults, but the minimum age of inclusion varies somewhat between studies. To arrive at a consistent age cutoff, we restrict our analyses to respondents age 50 and above in each survey.
Table 2 presents detailed information about the sample surveys we analyze: numbers of respondents, survey waves/years, country codes, and income levels. As can be seen, most of these studies are quite large with thousands or tens of thousands of respondents, typically observed several times. The studies also provide substantial coverage of both late middle age and older adults, with a large number of observations among those age 65 and above. For reference, we include the International Organization for Standardization three-digit (ISO3) codes for each country, which we use in several figures later in the manuscript. Unfortunately, these data primarily cover upper middle and high income countries, reflecting the dearth of global aging data collected in low and middle income countries; nonetheless, these 27 countries contain substantial numbers of the world’s late middle age and older adults (48.5% of the global age 50+ population in 2020).
Table 2.
Data Sets and Countries Used to Examine Population Loneliness
| Survey | Countries Covered (ISO3 Codes) | Years Used | # of Observations | # of Unique Respondents | # of Observations age 65+ | Income Levela | % of 2020 Global Age 50+ Population |
|---|---|---|---|---|---|---|---|
| CHARLS | China (CHN) | 2011, 2013, & 2018 | 37,021 | 15,864 | 14,279 | UM | 25.1% |
| ELSA | England (ENGb) | 2003–2015 | 65,487 | 16,747 | 34,613 | Hc | 1.4%c |
| HART | Thailand (THA) | 2015 & 2016 | 8,400 | 5,057 | 5,176 | UM | 1.3% |
| HRS | United States (USA) | 1992–2016 | 203,850 | 36,827 | 110,457 | H | 6.3% |
| IFLS | Indonesia (IDN) | 2000–2015 | 7,817 | 5,897 | 3,652 | UM | 3.0% |
| KLoSA | Republic of Korea (KOR) | 2006–2016 | 41,297 | 9,372 | 25,045 | H | 1.1% |
| MHAS | Mexico (MEX) | 2001–2012 | 36,308 | 18,168 | 15,840 | UM | 1.4% |
| SHARE | Austria (AUS), Belgium (BEL), Czechia (CZE), Denmark (DNK), Estonia (EST), France (FRA), Germany (DEU), Israel (ISR), Italy (ITA), Luxembourg (LUZ), Netherlands (NLD), Slovenia (SVN), Spain (ESP), Sweden (SWE), Switzerland (CHE), Croatia (HRV), Greece (GRC), Poland (POL), & Portugal (POR) | 2013*, 2015, & 2017 | 141,331 | 83,540 | 83,964 | H | 9.0% |
| TILDA | Ireland (IRE) | 2010–2015 | 20,234 | 8,172 | 9,671 | H | 0.1% |
|
| |||||||
| Total | 561,745 | 199,644 | 302,697 | 48.5% | |||
SHARE includes Croatia, Greece, Poland, and Portugal in the sample beginning in 2016 (Wave 6).
World Bank, 2020–2021 Income Level Categories: Low Income (L: < $1,036), Lower-Middle Income (LM: $1,036-$4,045), Upper-Middle Income (UM: $4,046-$12,535), and High Income (H: > $12,535).
Covers only England. Not an official ISO3 code.
Statistics are for United Kingdom.
In addition to survey data that provide us with data on loneliness and demographic information on representative samples of respondents, we also use data from the UN World Population Prospects to model historical and projected changes in countries’ age-sex composition and size (United Nations, 2019). The UN data cover the period 1950–2100, but we focus on the years between 1990 and 2050. This period looks backward and forward 30 years from the present and stays within a future period whereby all of the late middle age and older adults of 2050 are currently alive, making the timeframe within the bounds of reasonable projections. It is important to recognize that our focus on age groups 50+ and the timeframe of our study (1990 to 2050) means that our results do not vary substantially by whether we use the UN high, medium, or low estimates, which only vary fertility levels and, thus, do not yield variation in population composition within our focal age groups during our study period: e.g., the first year in which the UN projects within-country variation in the age 50–55 category is 2075 (reflecting uncertain estimates of those born in 2025, who would enter the 50–55 year old age group in that year). To test for other sources variability, we conducted several sensitivity analyses that we discuss in a dedicated Sensitivity Analyses section below; one of these tests includes using entirely different demographic projections derived from the Shared Socioeconomic Pathways (SSP) projections.6
Table 3 shows the past and projected future number of late middle age and older adults across our surveyed countries using estimates from the UN data. Even though the number of late middle age and older adults varies, the size of the population over age 50 is expected to increase in all countries from 1990–2050. The pace of aging combined with population size increases leads to quite staggering estimates of growth in the numbers of adults over age 50 worldwide: from 887.4 million in the world in 1990 to 1.883 billion today all the way to 3.179 billion in 2050. Our sample countries reflect this growth, with 431.6 million late middle age and older adults living in sample countries in 1990 to 914.2 million today to 1.3 billion in 2050.
Table 3.
Key Population Aging Indicators for the Sample Countries.
| Number of adults aged 50+ (millions) | Adults aged 50+ as percent of country’s total population | |||||
|---|---|---|---|---|---|---|
| 1990 | 2020 | 2050 | 1990 | 2020 | 2050 | |
| Austria | 2.4 | 3.7 | 4.5 | 31.4% | 41.3% | 49.2% |
| Belgium | 3.2 | 4.6 | 5.5 | 32.1% | 39.4% | 44.8% |
| China | 187.7 | 472.0 | 662.5 | 15.9% | 32.8% | 47.2% |
| Croatia | 1.5 | 1.7 | 1.7 | 30.7% | 42.5% | 51.1% |
| Czechia | 2.9 | 4.2 | 4.9 | 27.9% | 38.8% | 46.8% |
| Denmark | 1.6 | 2.3 | 2.7 | 30.9% | 40.1% | 42.9% |
| England | 17.9 | 25.7 | 32.4 | 31.4% | 37.9% | 43.8% |
| Estonia | 0.5 | 0.5 | 0.6 | 29.5% | 39.3% | 48.3% |
| France | 16.8 | 26.2 | 30.5 | 29.6% | 40.1% | 45.1% |
| Germany | 26.7 | 37.5 | 39.3 | 33.7% | 44.7% | 49.0% |
| Greece | 3.3 | 4.5 | 4.9 | 31.9% | 43.2% | 54.0% |
| Indonesia | 23.1 | 56.7 | 109.7 | 12.7% | 20.7% | 33.2% |
| Ireland | 0.8 | 1.6 | 2.4 | 22.6% | 31.8% | 42.9% |
| Israel | 0.9 | 2.2 | 3.9 | 19.6% | 25.6% | 30.6% |
| Italy | 18.8 | 27.6 | 29.5 | 32.9% | 45.7% | 54.2% |
| Luxembourg | 0.1 | 0.2 | 0.3 | 30.7% | 34.4% | 43.5% |
| Mexico | 9.8 | 27.2 | 55.0 | 11.7% | 21.1% | 35.5% |
| Netherlands | 4.1 | 7.1 | 8.0 | 27.5% | 41.3% | 46.7% |
| Poland | 9.5 | 14.4 | 17.1 | 25.1% | 38.0% | 51.3% |
| Portugal | 3.0 | 4.5 | 4.8 | 30.3% | 43.9% | 52.7% |
| Rep. of Korea | 7.0 | 20.3 | 27.6 | 16.2% | 39.7% | 59.0% |
| Slovenia | 0.6 | 0.9 | 1.0 | 27.4% | 42.3% | 49.6% |
| Spain | 11.6 | 19.3 | 23.3 | 29.6% | 41.3% | 53.5% |
| Sweden | 2.8 | 3.9 | 4.9 | 33.1% | 38.8% | 42.9% |
| Switzerland | 2.0 | 3.5 | 4.6 | 30.7% | 40.5% | 47.2% |
| Thailand | 8.3 | 24.1 | 32.7 | 14.7% | 34.5% | 49.6% |
| USA | 64.7 | 117.8 | 154.6 | 25.6% | 35.6% | 40.8% |
|
| ||||||
| Study countries total | 431.6 | 914.2 | 1,268.9 | |||
| Rest of world | 456.0 | 969.1 | 1,909.7 | 14.7% | 19.3% | 27.8% |
| World | 887.4 | 1,883.4 | 3,178.7 | 16.7% | 24.2% | 32.7% |
The pace of aging in each country is also rapid, though there is substantial variation between places as illustrated in the table’s estimates of the percent of each country’s entire population that are late middle age and older adults. In 1990, the percent of each national population over the age of 50 ranged from a low of 12%−16% (Mexico, Thailand, China, and Republic of Korea) to a high of 33% or more (Italy, Sweden, and Germany). In 2050, all but one country (Israel) will have more than a third of their populations over the age of 50, as high as 59% in the Republic of Korea. The growth in the share of the population over 50 is in general much higher in the Asian countries (the Republic of Korea, Thailand, and China) than elsewhere. These data reveal that population aging is a global concern and affects countries of varied income levels and in diverse geographic regions.
Measuring Loneliness in Surveys
To assess loneliness prevalence in each country, we use a single-item measure that is harmonized across surveys, which prior work suggests works well for measuring cross-national differences in late middle age and older adult loneliness and performs similarly as multi-item scales (Newmyer et al., 2021). The question about loneliness in most surveys comes from the Center for Epidemiological Studies-Depression (CES-D) scale, which evaluates respondents’ depressive symptoms (Radloff, 1977). This question inquires whether a respondent felt lonely in the past week. In surveys that do not include the CES-D scale, there is a comparable question, “How often do you feel lonely?” We harmonize respondents’ answers across surveys into a dichotomous measure, coding respondents who answer they “never” or “rarely” feel lonely as not being lonely and those answering they feel lonely more frequently than that as being lonely. Appendix A includes details about the specific questions and answers for each survey.
We assess the extent to which loneliness varies across ten-year birth cohorts (<1920, 1920–9, 1930–9, 1940–9, 1950–9, and 1960–9), age groups (50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80+), and sex (male and female). Using uniform 10-year birth cohorts allows for measurement comparability across countries. Our sample includes more cohorts in some countries than others, depending on when surveys were administered. For example, we observe more cohorts and more observations across cohorts in the United States (HRS) than Spain (SHARE) because the HRS had earlier and more frequent data collections than SHARE. This means that the cohort born before 1924 in the HRS (Aging and Health Dynamics cohort – AHEAD), a theoretically defined “generation” (Sonnega et al., 2014), cannot be compared to the same cohort in other surveys, which motivates us to focus on fixed 10-year birth cohorts.
Analytic Plan
Our central aim in this article is to understand how population aging influences national late middle age and older adult loneliness levels, in service of a broader effort to showcase the potential for demographic analyses to shed light on changing national and global mental health burdens. To achieve this aim, we proceed in multiple stages.
We first attempt to estimate reliable age-sex patterns of late middle age and older adult loneliness in each country, which we will later use to model changing loneliness prevalence in these age ranges as a function of changes in the age-sex structure among those over age 50 (i.e., demographic metabolism). However, the validity of these subsequent analyses hinges on the critical assumption that the age-sex pattern of loneliness is time-invariant across the period of analysis (1990–2050). If there are cohort differences in the age pattern of loneliness, then this assumption of a time-invariant age-sex pattern of loneliness is invalid. We first test its applicability to the recent past using empirical data, as described here. Then, as described in the Sensitivity Analyses section, we test how our results might change were assumed time-invariance to wane in the future.
Figure 1 presents the age pattern of loneliness for multiple cohorts in a select group of three countries (i.e., Greece, China, and Denmark; ignoring sex differences for now). This figure highlights the types of data we use and illustrates what the cohort-invariance assumption implies. Each point is the average for a given birth cohort’s responses to the loneliness questions of interest when they are the ages indicated on the x-axis, which we derive from the survey measures over multiple years so that we can see members of a cohort at different ages and multiple cohorts at any given age. Three key features stand out. First, the figure shows the generally strong regularity in the age patterns of age 50 and older loneliness in each country. It is age, rather than birth cohorts, that is important for late middle age and older adult loneliness prevalence in these countries. As an example, consider the clear continuity between the average loneliness levels of 75–79-year-old residents of each of the countries born ten years apart, in the 1930–39 and 1940–49 birth cohorts. Second, there is substantial heterogeneities in late middle age and older adult loneliness levels by country (e.g., high in Greece, low in Denmark). Third, it highlights that different countries have different age patterns of late middle age and older adult loneliness: Greece has a dip in loneliness around traditional retirement ages then an increase; China has an approximately uniform increase across ages; and Denmark has stability prior to traditional retirement ages then a slow increase thereafter. Appendix B shows similar figures for each country we examine, again leveraging multiple survey years to examine each birth cohort at multiple ages and multiple cohorts at any given age. Among the countries we examine, age differences in loneliness are far greater than cohort differences, with few deviations (e.g., Chinese ages 50–54, Greeks ages 65–69 and 80+).
Figure 1.
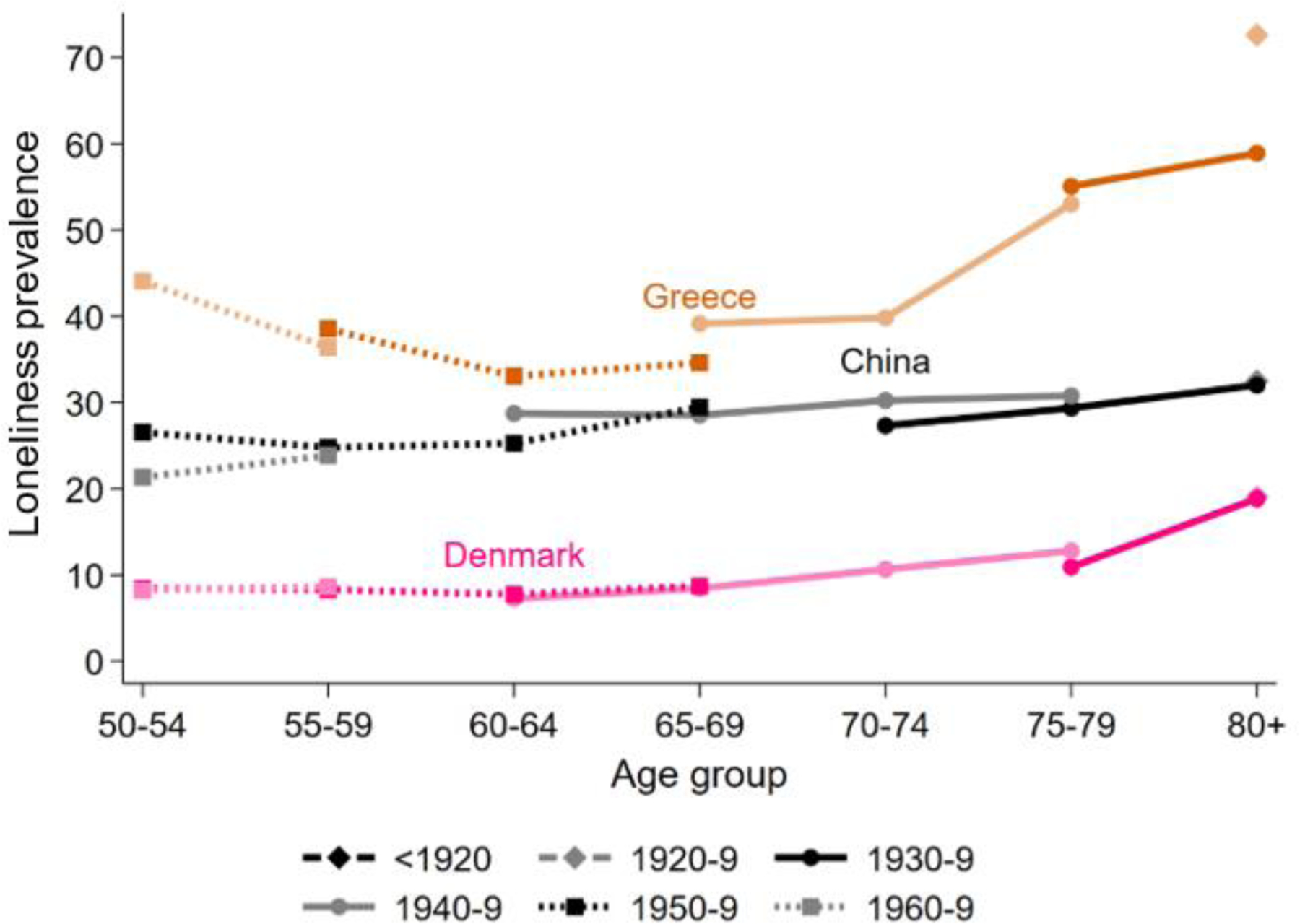
Loneliness by Age and Cohort in Select Countries
Note. See Appendix B for results for all countries.
We also statistically assess whether the age pattern of loneliness varies by cohort in each of the countries. To do this, we regress loneliness on age group, sex, and birth cohort, with an interaction between age group and birth cohort, in each country. This procedure produces between 0 and 17 age-by-cohort interactions, depending on how frequently we observe cross-classified age-by-cohort cases in each country. The magnitude and statistical significance of these interaction terms allow us to ascertain whether there is meaningful cohort variation that would preclude assuming that the age-sex pattern of late middle age and older adult loneliness in each country is approximately time-invariant. We detail the results of these analyses in Appendix C, which summarizes the number of interactions we test in each country and how many are statistically significant. We also examine joint tests of significance for the overall set of interactions to gauge whether cohort, overall, has a statistically significant multiplicative relationship with age.
Our results in Figure 1, Appendix B, and Appendix C show that age rather than birth cohort is the clear delineator of loneliness levels among adults over age 50 in our sample countries. Countries that have a substantial fraction of significant interactions, for instance, do not display evidence of overall cohort variation on the joint test of significance, or else their Figures in Appendix B clearly highlight a general age pattern of late middle age and older adult loneliness. There is room for debate about this conclusion, but we do not believe that the bulk of evidence suggests substantial violations of approximately cohort-robust age patterns of late middle age and older adult loneliness in each of the countries.
Because we found little evidence of cohort variation in the age patterns of late middle age and older adult loneliness in our focal countries, we proceed to the second step in our analytic plan. Our second step is to model recent past and near future period changes in loneliness as a function of changes in each country’s age and sex distribution and country-specific age-sex loneliness curves. We do this by first calculating country-specific predicted probabilities of loneliness prevalence in each age-sex group. Predicted probabilities are calculated using postestimation from logistic regression models predicting odds of loneliness that also control for cohort, age group, and sex. We then apply each country’s predicted age-sex pattern of loneliness prevalence to the UN’s estimates of that country’s age and sex structure, from 1990 to 2050. These procedures allow us to examine how national aging trends might contribute to changes in late middle age and older adult loneliness prevalence, given a data-grounded assumption of time-invariant age-sex patterns of loneliness in these age ranges (see Sensitivity Analyses section for discussion of how we relax this assumption).
To assess whether our modeling strategy replicates the observed late middle age and older adult loneliness prevalence levels in each of the countries, in Figure 2 we graph the observed values in each survey year against the modeled values for that year, the former estimated directly from the data in applicable years and the latter created using our measure of the age-sex pattern described above and the United Nations’ data on changing age-sex structures over the relevant period. We include a line of equality in red (where the observed proportion equals the modeled proportion) and the country ISO3 codes and survey years in the markers to help identify major outliers. In general, the modeled results closely match the survey results. The correlation between the two series is 0.95, and there is neither a major deviation from the line of equality nor is there substantial heteroscedasticity (i.e., the modeling appears to work about as well for countries with low levels of late middle age and older adult loneliness prevalence as for countries with high levels). There are some outlier cases, such as Israel in 2015 where our modeled loneliness is about 11% lower than the observed loneliness, but overall, the model does quite well. In the case of Israel, for instance, the observed 2015 value represents a substantial shift from the observation two years earlier, from 28% lonely in the 2013 SHARE wave to 44% in the 2015 wave. Our model misses these big year-to-year shifts in a few places, as would be expected modeling loneliness as a function of demographic changes. Additional contributions to these discrepancies arise from measurement error, coverage error, sampling error, and non-alignment between our assumptions of cohort invariance and reality. In the case of Israel, for instance, we note that we have fewer observations within age groups across cohorts than in most other countries (see Appendix B).
Figure 2.
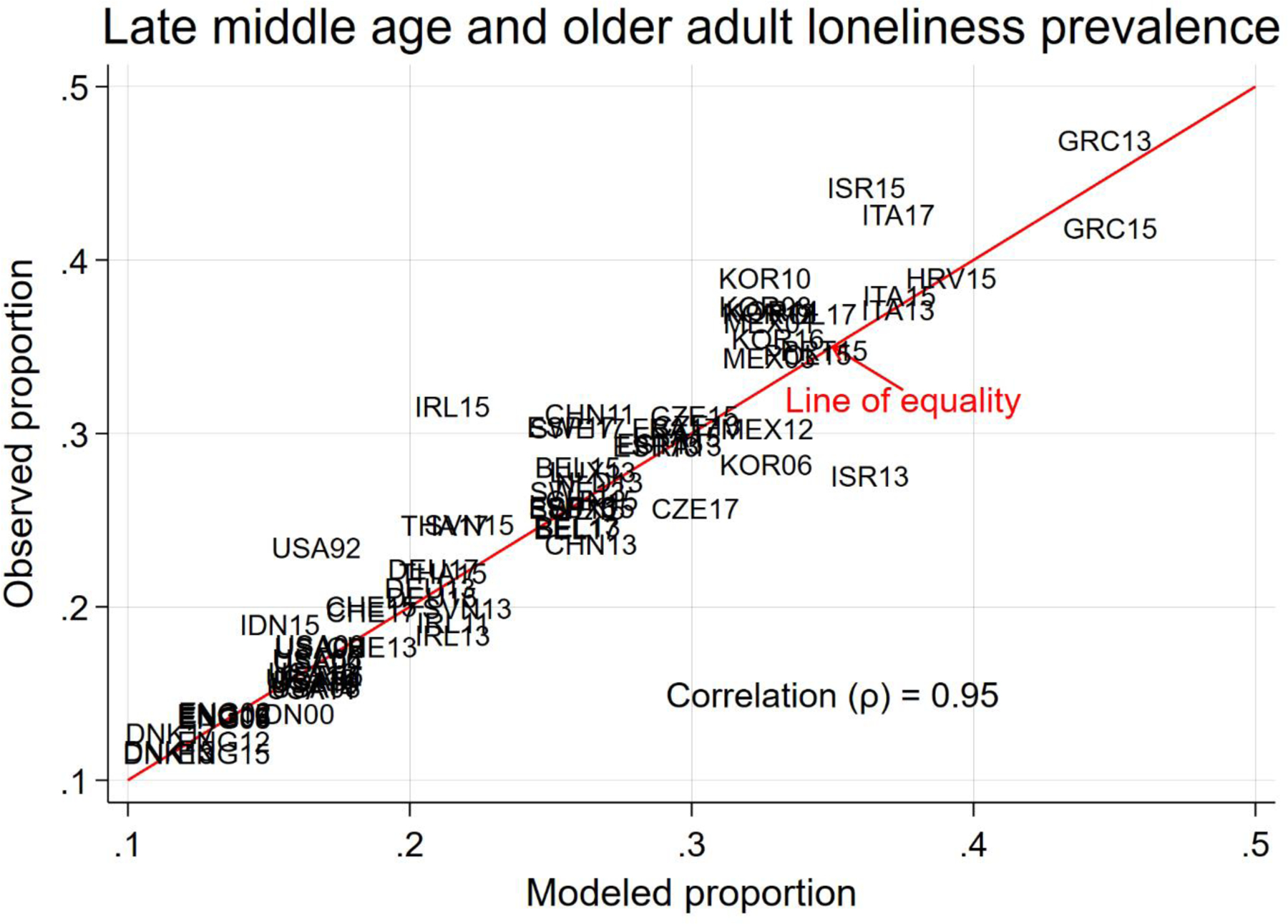
Comparing Observed and Modeled Late Middle Age and Older Adult Loneliness Prevalence in Focal Countries in Different Sample Years
Note. See column 2 in Table 2 for country codes.
Sensitivity Analyses
Our modeling strategy relies on a key assumption of time-invariance in the age-sex patterns of loneliness in each country, which we believe is empirically justified on the basis of the analyses in Figure 1, Appendix B, and Appendix C. However, although these results convince us that a time-invariance assumption is likely justified in the short term, the future remains uncertain. Technological change, health and mobility improvements (or deterioration), or other factors may make it such that patterns of loneliness by age and sex observed in the recent past do not apply in the future. As such, we conduct a first sensitivity test wherein we varied our assumptions about the time-invariance of the age-sex loneliness curves. We do this by projecting increasing uncertainty in the modeled age-sex loneliness curves in each country as time progresses. Specifically, we create two scenarios; in the first, we increase the loneliness curves at each point by 0.175% per year starting in 2020 (i.e., where L is the probability of being lonely and c, a, s, and t index country, age, sex, and time respectively from 2021 to 2050); in the second, we do the same but decrease it by that amount. This procedure yields a total variation around our loneliness assumptions of about 5.9% (2×1.001^29) by the end of the period, which is slightly more than one half a standard deviation in the distribution of loneliness prevalence observed between country-years in the empirical survey data graphed in Figure 2 (10.7%). We assess how such changes might alter our results. We also conduct a second sensitivity test wherein we vary the underlying demographic projection models. To do this, we substitute the Wittgenstein Center’s SSP projections in place of the United Nations’ projections. The SSP projections, unlike the United Nations ones, make assumptions about differential mortality and migration rates, and thus there is more variation in demographic trajectories among the 50 population in these models. The SSP models contain five scenarios, which are described in Appendix D, which all begin from 2010. We re-ran our models using all five scenarios, then took the highest and lowest values for outcomes of interest in each year. Because our aim is to contextualize potential future change by considering how it might differ from what we think has recently occurred, we privilege the results from the United Nations models in the main text owing to those models allowing us to examine the 1990–2020 period in addition to future change. We discuss the results of these sensitivity analyses below.
Outcomes of Interest
We examine what our model results imply for how population aging will change the mental health profiles of different countries in terms of late middle age and older adult loneliness. We examine four outcomes of interest: (1) Modeled country-specific percentage changes in the prevalence of late middle age and older adult loneliness from 1990 to 2050, to characterize how aging has and will influence loneliness levels and how it may differ by sex (Figure 3), (2) Modeled changes in the percent and number of late middle age and older adults who are lonely in each country, to illustrate the magnitude of these changes (Table 4), (3) A growing sex gap in the number of lonely late middle age and older adults across all sample countries, to feature the increasing feminization of loneliness (Figure 4), and (4) The modeled percentage of each country’s overall population that are lonely late middle age and older adults, to highlight how disparities in the pace of aging interacts with the aging-induced adult loneliness dynamics in each country (Figures 5 and 6). These analyses allow us to explore how the prevalence of late middle age and older adult loneliness in countries responds, and is projected to react, to population aging, prevalence of loneliness, and population growth. Figure 7 examines variation under the first sensitivity analysis, where we relax the time-invariance assumption, and Figure 8 and Appendix D examine the sensitivity of the results owing to the demographic projection models we use.
Figure 3.
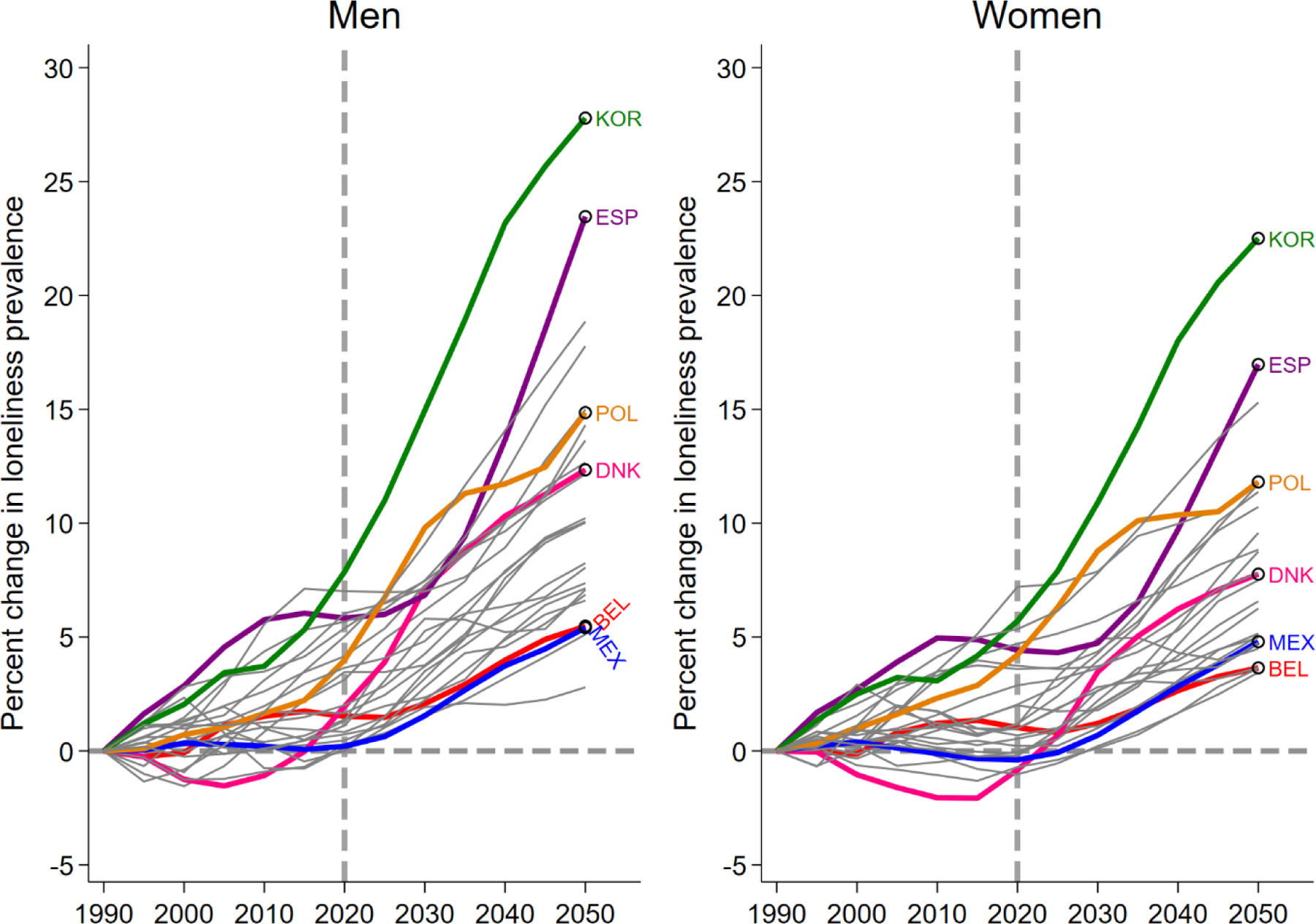
Modeled Percent Changes from 1990 Late Middle Age and Older Adult Loneliness Prevalence by Country and Sex
Note. See column 2 in Table 2 for country codes.
Table 4.
Modeled Results for Loneliness Prevalence and Number of Adults 50+ by Country.
| Modeled loneliness prevalence among older adults aged 50+ (%) | Modeled number of lonely older adults aged 50+ (Millions) | |||||
|---|---|---|---|---|---|---|
| 1990 | 2020 | 2050 | 1990 | 2020 | 2050 | |
| Austria | 18.2 | 18.1 | 19.7 | 0.4 | 0.7 | 0.9 |
| Belgium | 25.8 | 25.8 | 26.5 | 0.8 | 1.2 | 1.5 |
| China | 26.4 | 26.5 | 28.2 | 49.5 | 125.2 | 187.0 |
| Croatia | 37.8 | 39.4 | 41.0 | 0.6 | 0.7 | 0.7 |
| Czechia | 30.3 | 30.2 | 31.2 | 0.9 | 1.3 | 1.5 |
| Denmark | 11.7 | 11.6 | 12.7 | 0.2 | 0.3 | 0.3 |
| England | 13.4 | 13.4 | 14.3 | 2.4 | 3.5 | 4.6 |
| Estonia | 27.6 | 29.4 | 30.6 | 0.1 | 0.2 | 0.2 |
| France | 29.3 | 29.4 | 30.8 | 4.9 | 7.7 | 9.4 |
| Germany | 20.7 | 20.9 | 22.0 | 5.5 | 7.8 | 8.7 |
| Greece | 42.6 | 44.7 | 46.9 | 1.4 | 2.0 | 2.3 |
| Indonesia | 15.4 | 15.5 | 17.1 | 3.6 | 8.8 | 18.8 |
| Ireland | 21.9 | 21.7 | 22.6 | 0.2 | 0.3 | 0.6 |
| Israel | 36.1 | 36.3 | 37.3 | 0.3 | 0.8 | 1.5 |
| Italy | 36.0 | 37.3 | 40.4 | 6.8 | 10.3 | 11.9 |
| Luxembourg | 26.9 | 26.3 | 27.8 | 0.0 | 0.1 | 0.1 |
| Mexico | 32.7 | 32.7 | 34.5 | 3.2 | 8.9 | 19 |
| Netherlands | 27.0 | 26.7 | 27.9 | 1.1 | 1.9 | 2.2 |
| Poland | 33.4 | 34.6 | 37.2 | 3.2 | 5.0 | 6.4 |
| Portugal | 33.9 | 34.9 | 36.6 | 1.0 | 1.6 | 1.8 |
| Rep. of Korea | 31.8 | 33.5 | 39.1 | 2.2 | 6.8 | 10.8 |
| Slovenia | 21.5 | 22.3 | 24.6 | 0.1 | 0.2 | 0.2 |
| Spain | 24.7 | 25.6 | 29.0 | 2.9 | 5.0 | 6.8 |
| Sweden | 26.1 | 26.0 | 27.4 | 0.7 | 1.0 | 1.3 |
| Switzerland | 18.7 | 18.7 | 19.6 | 0.4 | 0.7 | 0.9 |
| Thailand | 20.8 | 21.3 | 23.1 | 1.7 | 5.1 | 7.5 |
| USA | 16.6 | 16.4 | 17.2 | 10.8 | 19.4 | 26.6 |
| All sample countries | 104.9 | 226.5 | 333.5 | |||
Figure 4.
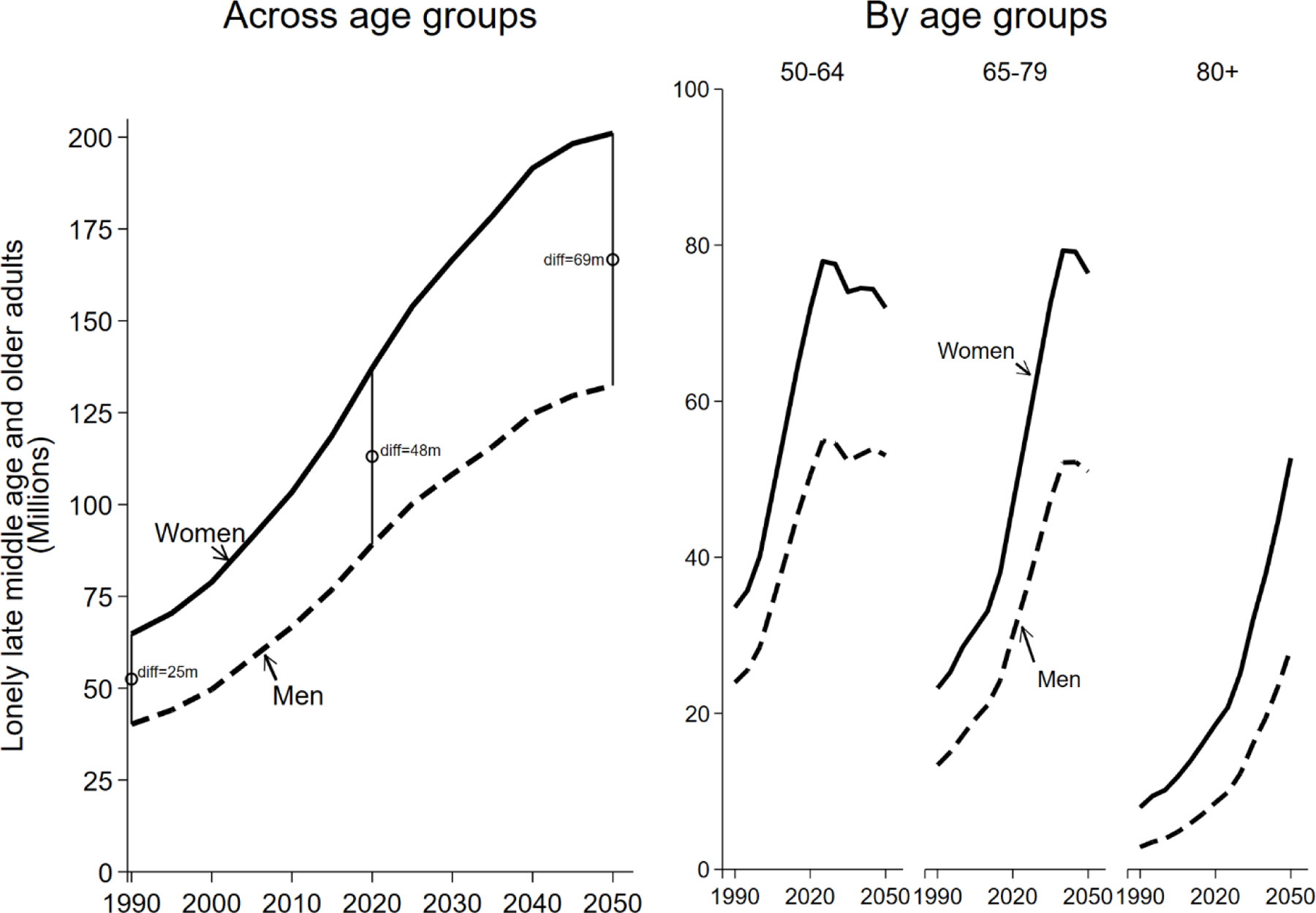
Modeled Results for Number of Lonely Late Middle Age and Older Adults in All Sample Countries, by Sex and Broken Down by Age Group
Figure 5.
Modeled Changes in the Percent of Each Country Composed of Lonely Late Middle Age and Older Adults.
Note. See column 2 in Table 2 for country codes.
Figure 6.
Modeled Changes in the Percent of Each Country Composed of Lonely Late Middle Age and Older Adults.
Notes: Data are sorted by percent lonely late middle age and older adults in 2020. See column 2 in Table 2 for country codes.
Figure 7.
Sensitivity Analysis: Modeled Percent Changes from 1990 Late Middle Age and Older Adult Loneliness Prevalence by Country under Uncertainty Scenarios (Compare to Figure 3).
Note. See column 2 in Table 2 for country codes.
Figure 8.
Sensitivity Analysis: Modeled Percent Changes from 1990 Late Middle Age and Older Adult Loneliness Prevalence by Country under SSP Demographic Models (Compare to Figure 3).
Note. See column 2 in Table 2 for country codes. See Appendix B for greater detail.
Results
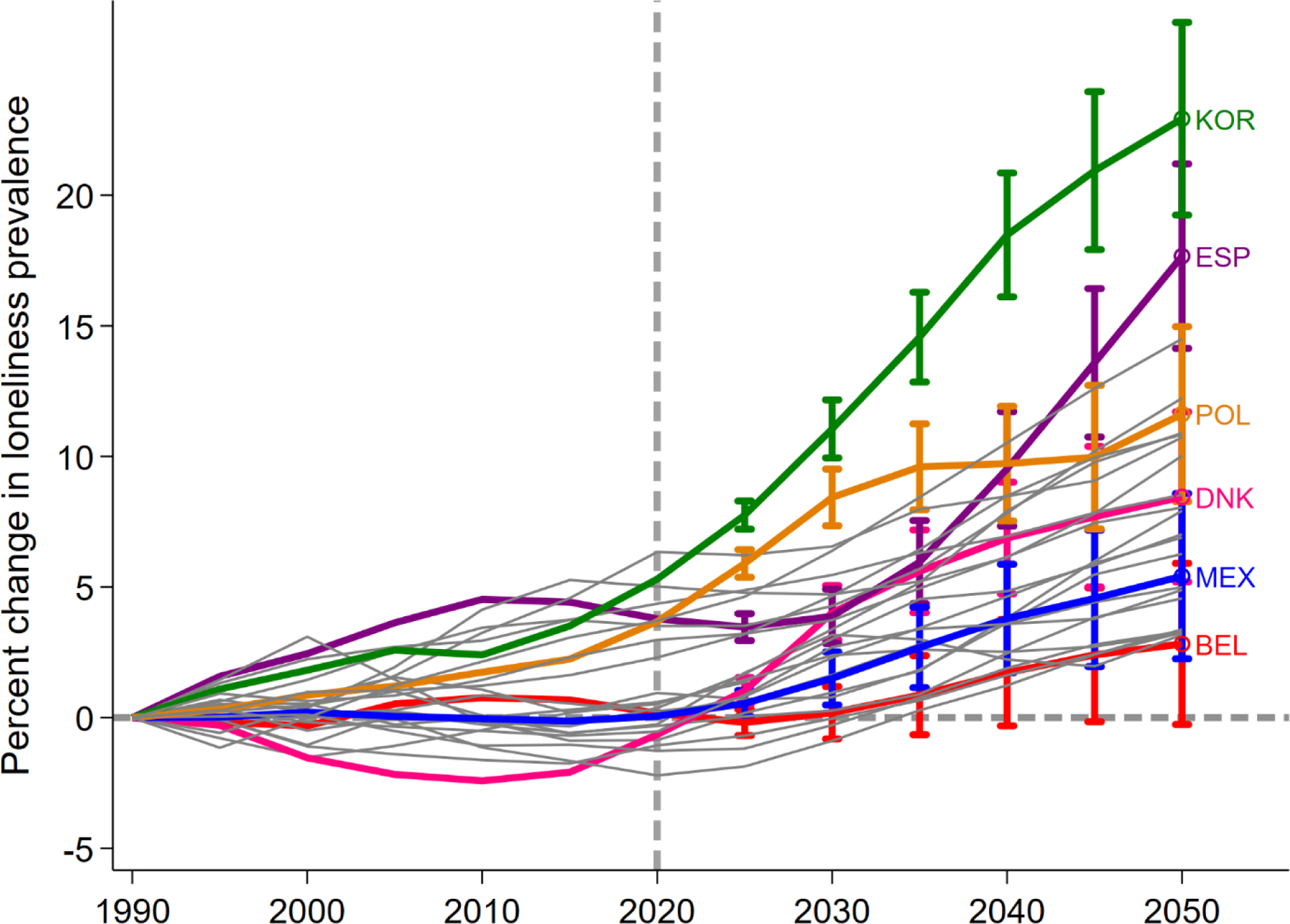
First, we examine how population aging is shaping late middle age and older adult loneliness in our sample of countries. Figure 3 plots the percent change in late middle age and older adult loneliness prevalence for each country from 1990 to 2050, using 1990 levels as the baseline (0% change), with separate panels by sex. We label select countries and include a reference line at 2020 to facilitate comparison of changes over the past and next 30 years. The broad contours of the figure are comparable for men and women. Our model suggests population aging had minimal effects on percent change in loneliness prevalence in most countries between 1990–2020; all changes were within ±5%. The model implies some countries like Denmark had small decreases in late middle age and older adult loneliness, with others like Mexico barely changing, and others like Poland, Spain and the Republic of Korea rising slightly by about 5% in the past 30 years. However, the story is different when looking into the future. Late middle age and older adult loneliness prevalence is projected to rise from 2020 to 2050 in all countries, some quite steeply in percentage terms, with widening disparities across countries. The Republic of Korea (KOR) and Spain (ESP) have the greatest increases in percent change of loneliness prevalence over the projected time points. In contrast, our model projects that several countries, such as Denmark (DNK) and Poland (POL), will have strong discontinuities in their loneliness prevalence growth, while other countries such as the Mexico (MEX) and Belgium (BEL) might undergo more incremental and delayed increases in the prevalence of late middle age and older adult loneliness over time. Considering differences by sex, these results suggest greater prevalence increases for men in most but not all countries.
Table 4 shows late middle age and older adult loneliness prevalence and numbers of lonely adults over age 50 in each country in our sample for 1990, 2020 and 2050. These numbers allow examining unstandardized percentage point changes, showcasing the variation across countries in levels of late middle age and older adult loneliness. Although loneliness prevalence grows overall in all the countries we examine (left of Table 4), there is substantial variation across countries. Greece has the highest percentage of lonely adults over age 50, and its loneliness prevalence increases from 42.6% in 1990 to 44.7% in 2020, and to 46.9% in 2050. The Republic of Korea is projected to experience the highest percent change in loneliness due to population aging (as shown in Figure 3), but other Asian countries with substantial levels of population aging, like China and Thailand, show more moderate increases in levels of late middle age and older adult loneliness. The United States has the lowest projected percentage point increase, from 16.6% to 17.2% between 1990 and 2050 (Belgium has the lowest increase, as shown in Figure 3).
Table 4 (right) also presents estimates of the number of lonely late middle age and older adults in each country. These results underscore the projected massive growth in the global population of lonely late middle age and older adults that our analyses imply. These results are driven by both aging dynamics within the late middle age and older adult population and the growing numbers of late middle age and older adults in each country. More populous countries have more lonely adults over age 50, with China having the most in 1990 (49.5 million) and in 2050 (187.0 million). In contrast, Luxembourg has the fewest in 1990 (31 thousand), which is expected to grow substantially to 97 thousand in 2050.
Results presented so far have aggregated men and women. However, late middle age and older women’s higher rates of loneliness, as well as the fact that women make up a greater share of the population over age 50 due to their greater longevity, mean that loneliness may be disproportionately affecting late middle age and older women. Building on the total numbers available in Table 3, Figure 4 shows the number (in millions) of lonely late middle age and older adults by sex for all the countries in our sample (left panel) and broken down into three relevant age groups 50–64, 65–79, and 80+ (right panel). These results show a large and widening gap in the number of lonely late middle age and older adults by sex. Our model suggests in 1990, there were 24.6 million more late middle age and older adult women than late middle age and older adult men in our sample countries; this widens to 48.0 million in 2020, and 68.7 million in 2050. These results highlight the increasing feminization of late middle age and older adult loneliness. The gap is evident across all age groups, but the age-group specific results highlight that future growth in it is driven by widening gaps in the older age groups.
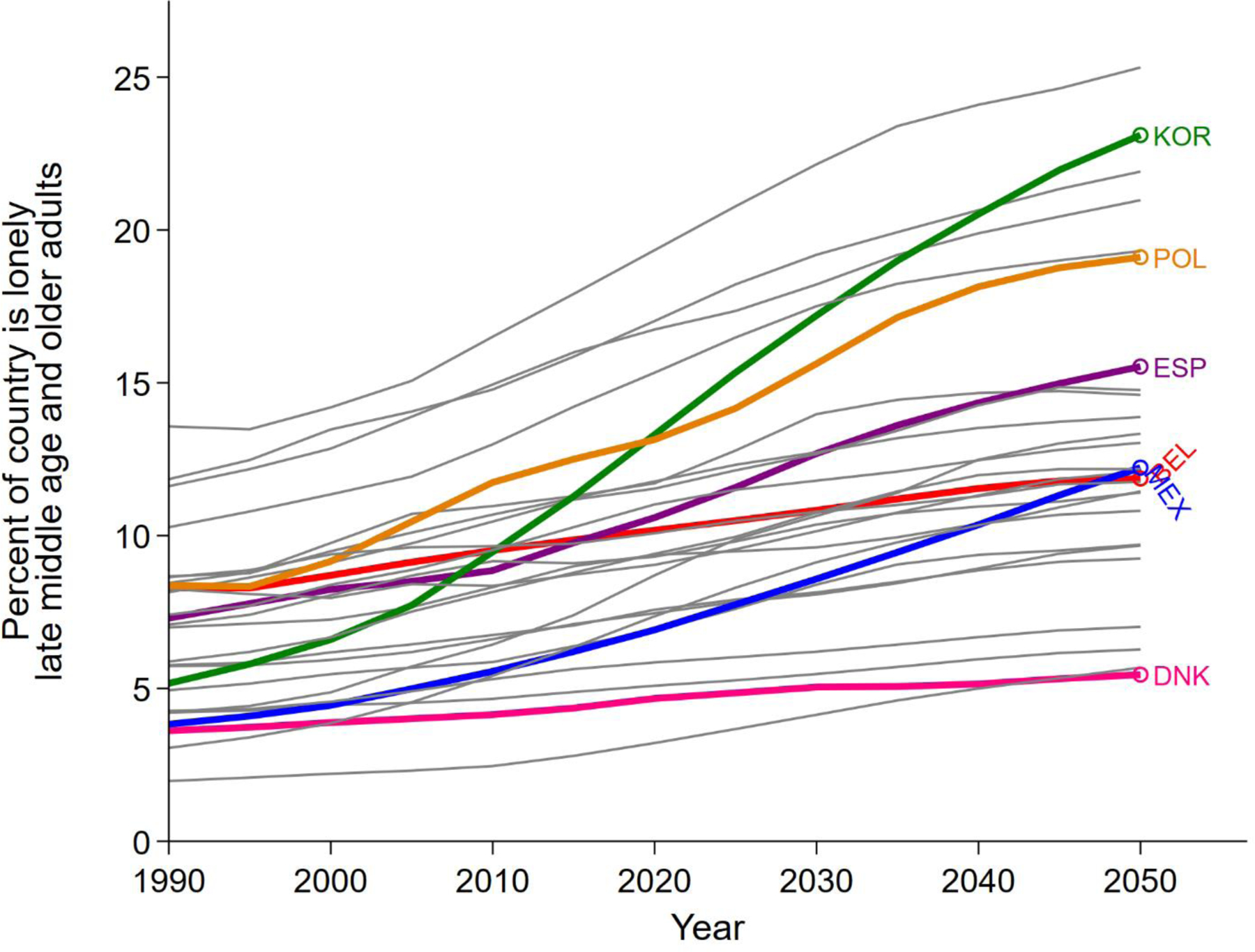
The last part of our analysis (Figures 5 and 6) presents the percentage of each country’s population that are lonely late middle age and older adults between 1990 and 2050. We estimate these numbers by taking the number of lonely late middle age and older adults in each country and time period (shown for specific years in Table 4, right) by the total population of the country. This measure presents the scale of the challenge that late middle age and older adult loneliness might constitute in each country when considered against its overall population. Figure 5 shows that our models suggest that all countries will see an increase in the percentage of their population that are lonely late middle age and older adults, with a small increase from 8.3% to 11.9% in Belgium (1990 to 2050), and very large increases in the Republic of Korea (5.2% to 23.1% from 1990 to 2050), Poland (8.4% to 19.1% from 1990 to 2050), and Spain (7.3% to 15.5% from 1990 to 2050). The models also point to increasing variability over the period of analysis. In 1990, our modeled results suggest that most countries had less than 10% lonely late middle age and older adults (excepting, in order, Portugal [10.3%], Croatia [11.6%], Italy [11.8%], and Greece [13.6%]), while in 2050, the range is much greater (from 5.5% in Denmark to 25.3% in Greece). In the majority of countries we studied, the model results imply that 10% or more of the residents will be lonely late middle age and older adults in 2050 (excepting, in order, Denmark [5.5%], Indonesia [5.7%], England [6.3%], The United States [7.0%], Switzerland [9.2%], Austria [9.7%], and Ireland [9.7%]).
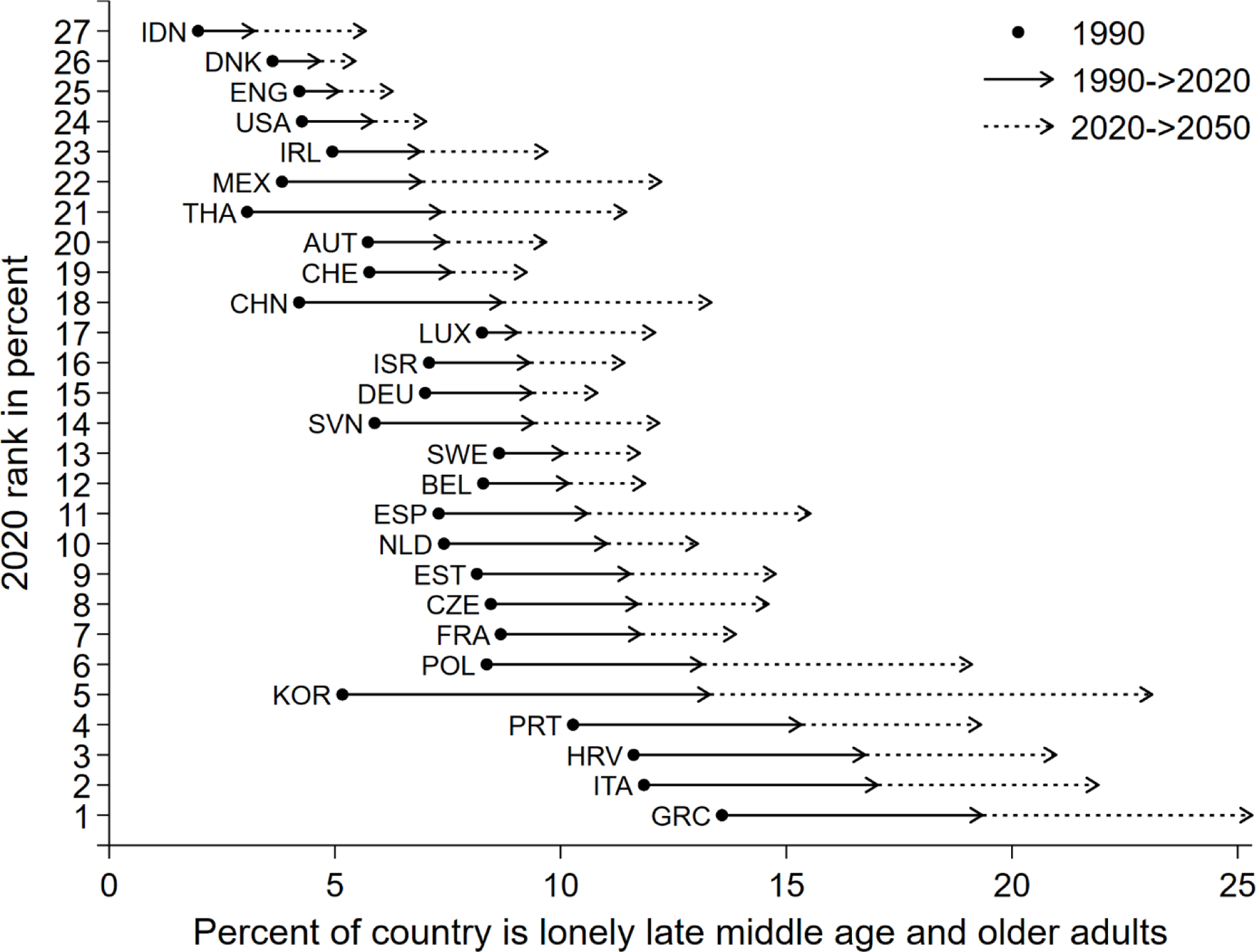
Another way to visualize the increases in the percent of countries comprised of late middle age and older adults is the summary in Figure 6, modeling changes from 1990 to 2020 and 2050. This figure ranks countries in order of the percent of the country that is lonely late middle age and older adults in 2020, with Denmark at the low end and Greece at the high end. The black circle notes the 1990 percent of lonely late middle age and older adults in the country, with the black arrow noting the change in the next 30 years, and the dotted arrow noting the change between 2020 and 2050. As shown, all countries are expected to have increasing percentages of lonely late middle age and older adults, with the largest increase in Greece and Italy, and the lowest increases in Denmark, England, and the USA.
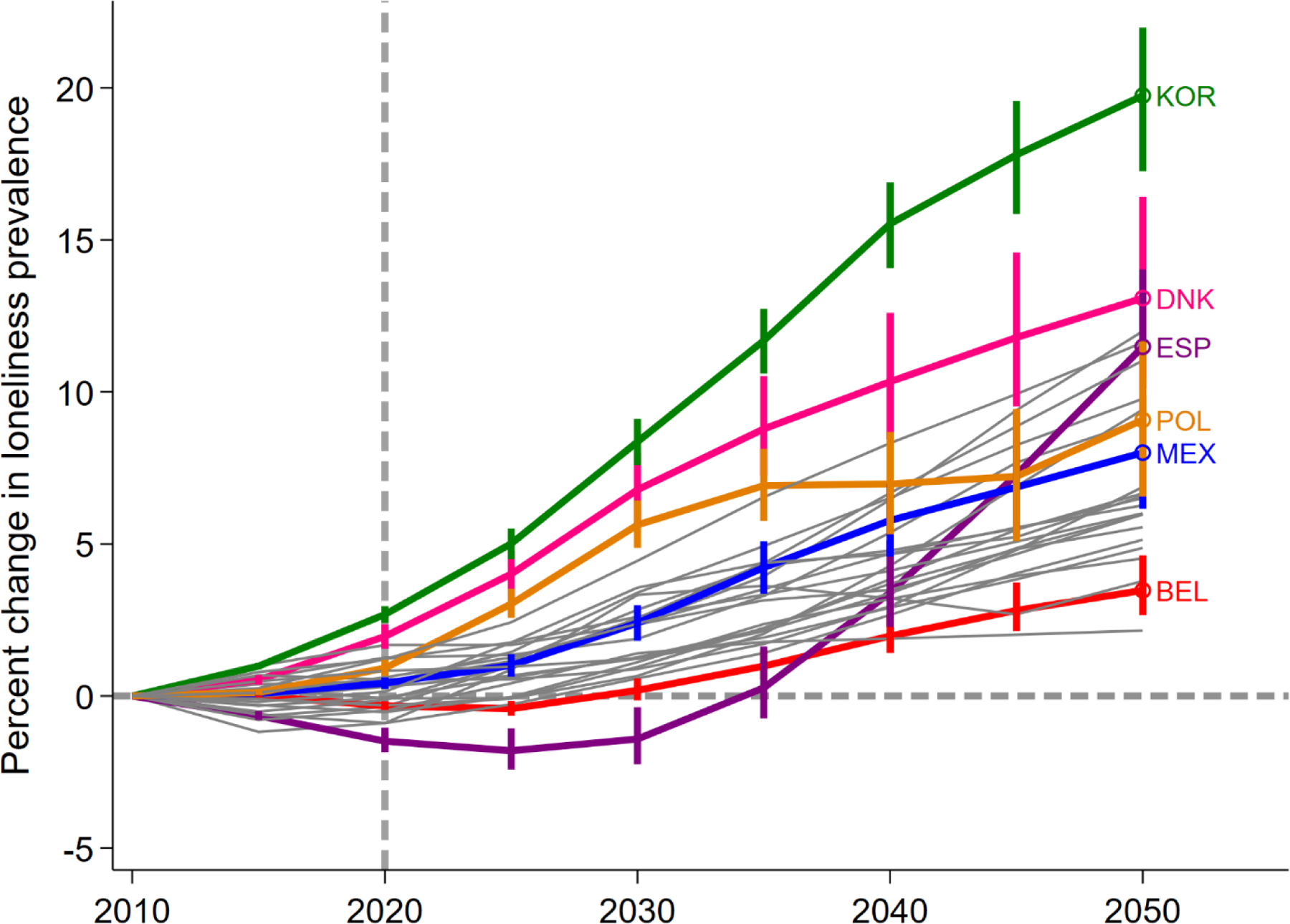
Last, we assess the sensitivity of our results to different assumptions about the future stability of age-sex loneliness patterns in each country (Figure 7) and about the demographic changes that are likely to occur in the next thirty years (Figure 8; Appendix D). Figure 7 highlights that even assuming a drift in each country’s loneliness curve equal to one half a standard deviation of the distribution of loneliness prevalence between countries, the results still suggest meaningful increases in loneliness in nearly all of the countries we examine. Figure 8 and Appendix D highlight that differences in the underlying demographic projections we use also do not fundamentally alter these conclusions. Late middle age and older adult loneliness is likely to increase in the near future, sometimes quite dramatically, in all countries owing to population aging.
Discussion
Population aging is an enormously important factor in the rising tide of loneliness around the world. Adopting a demographic metabolism approach, as we have here, can greatly improve our understanding of population health, and how we can prepare for future changes. Although loneliness prevalence levels vary by country, we find increases among adults over age 50 in all countries. Our models indicate that some of these country differences are due to population dynamics such as age and sex structures. Our estimates of late middle age and older adult loneliness levels in 2020 ranged from about 12% in Denmark to about 45% in Greece (a 33% point difference). However, our demographic metabolism models suggested that some countries might expect increases of three percentage points or more over the next 30 years solely owing to changing age and sex structures: Italy (3.1), Spain (3.4), and the Republic of Korea (5.6). We assessed whether these results were malleable to other future demographic scenarios and our sensitivity analyses yielded substantively similar results as those that used U.N. estimates, although with some variation. Changes in sex structure might also exacerbate other disparities as our results also highlight that loneliness will continue to be an issue that disproportionately affects late middle age and older women. Our results indicate that globally, there are more lonely late middle age and older adult women than men, and this gap is projected to expand in the future, particularly for adults age 65 and above.
The substantial increases in late middle age and older adult loneliness have important implications for physical health (Valtorta et al., 2016; Whisman, 2010; Wilson et al., 2007), mental health (Cacioppo et al., 2006; Domènech-Abella et al., 2019; Hawkley et al., 2003) and social well-being. We present the demography of late middle age and older adult loneliness among almost half of the world’s current population of people over age 50. Our findings document that loneliness is very common among late middle age and older adults around the world; in the majority of the countries in our sample, over 10% of late middle age and older adults report being lonely, and in 17 of the 27 countries it was more than 25%. Moreover, loneliness has a common but not universal age pattern, generally increasing across age groups, especially after traditional retirement ages. These results align with past research that found a similar U-shaped pattern in age and loneliness over the life course (Nicolaisen & Thorsen, 2014). There are country-specific nuances to these age-sex curves, though, none more important than what is in effect an intercept difference (i.e., differences in the prevalence of loneliness regardless of age).
We tested for differences by birth cohorts, as some previous research suggests there are cohort differences in social integration and social capital (Putnam, 2001; Rainie & Wellman, 2012; Stevens & van Tilburg, 2011). However, we did not find compelling evidence of cohort variations in age-sex patterns of late middle age and older adult loneliness in the countries we studied. Of course, that does not mean that such changes might not emerge in the future. For example, the COVID-19 pandemic might change or exacerbate loneliness (van Tilburg, 2021); though emerging evidence suggests that it had limited effect or even lowered the prevalence of mental health challenges among late middle age and older adults (Vahia et al., 2020; Van Winkle et al., 2021).
In country after country, there is substantial attention to perceived increases in loneliness among late middle age and older adults (Fasano, 2019; Park, 2019; Rivers & Lee, 2019; Troya, 2019; Yeginsu, 2018), with only limited consideration of how the challenges associated with late middle age and older adult loneliness might change in the future or why it seems to be rising more quickly in some places than others. The results we present in this article show that the default expectation should be that late middle age and older adult loneliness will grow substantially soon in some places but not others – not because of changing social mores and culture, but because of population aging, demographic metabolism, and country-specific age patterns of loneliness. In some countries, like Greece, Croatia, Italy, and the Republic of Korea, our models predict that lonely adults over age 50 will soon comprise a fifth to a quarter of the total population. In others, such as Denmark, England, and Indonesia we predict the share of the population that are lonely adults over age 50 is set to remain quite low. These divergent dynamics will pose different challenges in different places. For some, the next thirty years will be a continuation of the past, with slow increases in late middle age and older adult loneliness, or a small reversal from no meaningful change to moderate increases, but in others these shifts will be quite rapid. Our study focuses on cross-national projections of loneliness in late middle age and older adulthood in 27 countries. In this effort, we are unable to also give attention to other important contributors that might produce meaningful sub-national variations in loneliness such as living in an urban or rural location or socioeconomic status. This remains an important avenue for future research.
Our analysis focuses on the effects of population aging on loneliness levels. To put these findings into perspective, we can think about other important predictors of loneliness that may compound or mitigate the effects of population aging. The first two important factors to watch are the prevalence of living alone and the proportion of late middle age and older adults divorced or widowed – as both factors are strongly associated with loneliness in late middle and older age groups (De Jong Gierveld et al., 2012; Stickley et al., 2013). Both the number of late middle age and older adults living alone (Esteve et al., 2020; Reher & Requena, 2018) and the proportion of divorced and unpartnered late middle age and older adults have increased (Brown & Lin, 2012; Cooney & Dunne, 2001; Sassler, 2010), and if these trends persist globally, they might further increase future prevalence levels of late middle age and older adult loneliness. These changes might also exacerbate the sex disparities in loneliness in late middle age and older adulthood as women are often more likely to live alone or experience widowhood due, in part, to more favorable life expectancies (Dahlberg et al., 2015; Nicolaisen & Thorsen, 2014; Reher & Requena, 2018; Victor & Yang, 2012). Another factor that could also affect trends in loneliness of adults ages 50 and above is that of health and disability, particularly those in the oldest age groups as they have a high likelihood of being lonely as well as have other health complications. Health limitations are a key factor that limit the social engagement and activities of late middle age and older adults, and in many contexts, mobility problems, chronic conditions, and disability are increasing among middle-aged adults, foreshadowing an increase in poor health in future cohorts of late middle age and older adults (Freedman, 2018; Zimmer et al., 2012). On the other hand, there are social trends which could work in the opposite direction, working to decrease loneliness. Increased political attention to the issue has led to numerous policy interventions that target community and family supports (Fakoya et al., 2020; Masi et al., 2011). For example, improved social support or providing opportunities for social interaction are effective interventions at decreasing loneliness of late middle age and older adults (Masi et al., 2011).
Our study highlights the necessity to consider how population aging is reshaping mental health profiles of populations globally. Though our results conclude that loneliness levels are generally increasing with population aging around the world these projections are not absolute. Factors such as changes in social interaction or public policies might be able to reduce these rates. As the world changes due to population aging, it is increasingly important for demographers to understand the consequences of these population dynamics. Although we focus on these consequences for loneliness, future research could use a similar approach to understand how other dimensions of health such as prevalence of chronic physical health conditions, family dynamics such as caregiving, or other social dynamics might be reshaped by population aging.
Supplementary Material
Funding statement:
This work was supported by the Government of Canada—Canadian Institutes of Health Research (MYB-150262), Social Sciences and Humanities Research Council (435–2017-0618 and 890–2016-9000), National Institute on Aging (1R01AG060949), Pennsylvania State University Population Research Institute (supported by an infrastructure grant by the Eunice Kennedy Shriver National Institute of Child Health and Human Development P2C-HD041025), and an institutional NICHD predoctoral traineeship grant (T-32HD007514). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or other funding sources.
Footnotes
Conflict of interest disclosure: Authors declare no conflict of interests.
Because the survey data we use rely on measures of respondent sex rather than gender, we focus on our discussion on sex differences.
Note that these examples are highly stylized, and real data contain further complexities, where the entire age-sex distribution of the over age 50 adult population and loneliness patterns therein matter.
Within SHARE, we do not include Bulgaria, Cyprus, Finland, Hungary, Latvia, Lithuania, Malta, Romania, and Slovakia because they only have one wave of data where loneliness was measured.
We exclude HRS Sister studies that do not currently have publicly available data (the Malaysia Ageing and Retirement Survey and the Healthy Aging in Scotland study), require a full proposal to access (the Northern Ireland Cohort for the Longitudinal Study of Aging), do not measure loneliness (the Costa Rican Longevity and Healthy Aging Study), have limited waves of data (the Brazilian Longitudinal Study of Aging, the Longitudinal Aging Study in India, and the Health and Aging in Africa study) or age ranges (Japanese Study of Aging and Retirement), or include countries covered in other surveys (the World Health Organization Study on Global Ageing and Adult Health).
The HART study does not generate sample weights, nor do they have guidelines on how to do so. TILDA only provides sample weights for the first wave of data.
The SSP database is hosted by the IIASA Energy Program at https://tntcat.iiasa.ac.at/SspDb.
Data availability statement:
This study uses data from and United Nations World Population Prospects (https://population.un.org/wpp/) and Gateway to Global Aging (https://g2aging.org/). Registered users can access and download the data.
References
- Aartsen M, & Jylhä M (2011). Onset of loneliness in older adults: Results of a 28 year prospective study. European Journal of Ageing, 8, 31–38. 10.1007/s10433-011-0175-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agree EM, & Glaser K (2009). Demography of informal caregiving. In Uhlenberg P (Ed.), International Handbook of Population Aging (pp. 647–668). 10.1007/978-1-4020-835 [DOI]
- Ajrouch KJ, Blandon AY, & Antonucci TC (2005). Social networks among men and women: The effects of age and socioeconomic status. Journal of Gerontology: Social Sciences, 60B(6), S311–S317. [DOI] [PubMed] [Google Scholar]
- Antonucci TC, & Akiyama H (1987). Social networks in adult life and a preliminary examination of the convoy model. Journal of Gerontology, 42(5), 519–527. [DOI] [PubMed] [Google Scholar]
- Ayalon L, Shiovitz-Ezra S, & Palgi Y (2013). Associations of loneliness in older married men and women. Aging and Mental Health, 17(1), 33–39. 10.1080/13607863.2012.702725 [DOI] [PubMed] [Google Scholar]
- Bélanger A, Sabourin P, Marois G, Van Hook J, & Vézina S (2019). A framework for the prospective analysis of ethno-cultural super-diversity. Demographic Research, 41, 293–330. 10.4054/DEMRES.2019.41.11 [DOI] [Google Scholar]
- Bloom DE, Cafiero E, Jané-Llopis E, Abrahams-Gessel S, Bloom LR, Fathima S, ... & Weiss J. (2012). The global economic burden of noncommunicable diseases (No. 8712). Program on the Global Demography of Aging
- Bongaarts J (2004). Population aging and the rising cost of public pensions. Population and Development Review, 30(1), 1–23. [Google Scholar]
- Brown SL, & Lin I-F (2012). The gray divorce revolution: Rising divorce among middle-aged and older adults, 1990–2010. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 67(6), 731–741. 10.1093/geronb/gbs089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cacioppo JT, Hughes ME, Waite LJ, Hawkley LC, & Thisted RA (2006). Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses. Psychology and Aging, 21(1), 140–151. 10.1037/0882-7974.21.1.140 [DOI] [PubMed] [Google Scholar]
- Cooney TM, & Dunne K (2001). Intimate relationships in later life: Current realities, future prospects. Journal of Family Issues, 22(7), 838–858. [Google Scholar]
- Cornwell B, Laumann EO, & Schumm LP (2008). The social connectedness of older adults: A national profile. American Sociological Review, 73(April), 185–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cozijnsen R, Stevens NL, & Van Tilburg T (2010). Maintaining work-related personal ties following retirement. Personal Relationships, 17, 345–356. 10.1111/j.1475-6811.2010.01283.x [DOI] [Google Scholar]
- Dahlberg L, Agahi N, & Lennartsson C (2018). Lonelier than ever? Loneliness of older people over two decades. Archives of Gerontology and Geriatrics, 75, 96–103. 10.1016/j.archger.2017.11.004 [DOI] [PubMed] [Google Scholar]
- Dahlberg L, Andersson L, McKee KJ, & Lennartsson C (2015). Predictors of loneliness among older women and men in Sweden: A national longitudinal study. Aging and Mental Health, 19(5), 409–417. 10.1080/13607863.2014.944091 [DOI] [PubMed] [Google Scholar]
- De Jong Gierveld J (1989). Personal relationships, social support, and loneliness. Journal of Social and Personal Relationships, 6, 197–221. [Google Scholar]
- De Jong Gierveld J, Dykstra PA, & Schenk N (2012). Living arrangements, intergenerational support types and older adult loneliness in Eastern and Western Europe. Demographic Research, 27, 167–200. 10.4054/DemRes.2012.27.7 [DOI] [Google Scholar]
- De Meijer C, Wouterse B, Polder J, & Koopmanschap M (2013). The effect of population aging on health expenditure growth: A critical review. European Journal of Ageing, 10, 353–361. 10.1007/s10433-013-0280-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Domènech-Abella J, Mundó J, Haro JM, & Rubio-Valera M (2019). Anxiety, depression, loneliness and social network in the elderly: Longitudinal associations from The Irish Longitudinal Study on Ageing (TILDA). Journal of Affective Disorders, 246, 82–88. 10.1016/j.jad.2018.12.043 [DOI] [PubMed] [Google Scholar]
- Dykstra PA (2009). Older adult loneliness: Myths and realities. European Journal of Ageing, 6, 91–100. 10.1007/s10433-009-0110-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dykstra PA, Van Tilburg TG, & Gierveld JDJ (2005). Changes in older adult loneliness: Results from a seven-year longitudinal study. Research on Aging, 27(6), 725–747. 10.1177/0164027505279712 [DOI] [Google Scholar]
- Esteve A, Reher DS, Treviño R, Zueras P, & Turu A (2020). Living alone over the life course: Cross-national variations on an emerging issue. Population and Development Review, 6. 10.1111/padr.12311 [DOI] [Google Scholar]
- Fakoya OA, McCorry NK, & Donnelly M (2020). Loneliness and social isolation interventions for older adults: A scoping review of reviews. BMC Public Health, 20(129), 1–14. 10.1186/s12889-020-8251-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fasano G (2019, September 20). L’isolamento, la malattia, le difficoltà: Essere anziano in Italia. Corriere Della Sera Retrieved from https://www.corriere.it/cronache/19_settembre_19/isolamento-malattia-difficolta-essere-anziano-italia-7a3d4cd4-db24-11e9-94b9-f72cb5920b7e.shtml?refresh_ce-cp
- Fokkema T, De Jong Gierveld J, & Dykstra PA (2012). Cross-national differences in older adult loneliness. Journal of Psychology, 146(1–2), 201–228. 10.1080/00223980.2011.631612 [DOI] [PubMed] [Google Scholar]
- Fredrickson BL, & Carstensen LL (1990). Choosing social partners: How old age and anticipated endings make people more selective. Psychology and Aging, 5(3), 335–347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freedman VA (2018). The demography of late-life disability. Future Directions for the Demography of Aging, 269–305. 10.17226/25064 [DOI]
- Gerst-Emerson K, & Jayawardhana J (2015). Loneliness as a public health issue: The impact of loneliness on health care utilization among older adults. American Journal of Public Health, 105(5), 1013–1019. 10.2105/AJPH.2014.302427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagestad GO (1986). The family: Women and grandparents as kin-keepers. In Pifer AJ & Bronte L (Eds.), Our aging society: Paradox and promise (pp. 141–160). W.W. Norton & Co Inc. [Google Scholar]
- Hawkley LC, Burleson MH, Berntson GG, & Cacioppo JT (2003). Loneliness in everyday life: Cardiovascular activity, psychosocial context, and health behaviors. Journal of Personality and Social Psychology, 85(1), 105–120. 10.1037/0022-3514.85.1.105 [DOI] [PubMed] [Google Scholar]
- Hawkley LC, Masi CM, Berry JD, & Cacioppo JT (2006). Loneliness is a unique predictor of age-related differences in systolic blood pressure. Psychology and Aging, 21(1), 152–164. 10.1037/0882-7974.21.1.152 [DOI] [PubMed] [Google Scholar]
- Heikkinen R-L, & Kauppinen M (2004). Depressive symptoms in late life: A 10-year follow-up. Archives of Gerontology and Geriatrics, 38, 239–250. 10.1016/j.archger.2003.10.004 [DOI] [PubMed] [Google Scholar]
- Höllinger F, & Haller M (1990). Kinship and social networks in modern societies: A cross-cultural comparison among seven nations. European Sociological Review, 6(2), 103–124. 10.1093/oxfordjournals.esr.a036553 [DOI] [Google Scholar]
- Holt-Lunstad J, Smith TB, & Layton JB (2010). Social relationships and mortality risk: A meta-analytic review. PLoS Medicine, 7(7), e1000316. 10.1371/journal.pmed.1000316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, Aguilar-Gaxiola S, Alonso J, Chatterji S, Lee S, Ormel J, … Wang PS (2009). The global burden of mental disorders: An update from the WHO World Mental Health (WMH) Surveys. Epidemiologia e Psichiatria Sociale, 18(1), 23–33. 10.1016/j.jvs.2011.06.062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lam D (2011). How the World Survived the Population Bomb: Lessons From 50 Years of Extraordinary Demographic History. Demography, 48, 1231–1262. 10.1007/s13524-011-0070-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lara E, Moreno-Agostino D, Martín-María N, Miret M, Rico-Uribe LA, Olaya B, … Ayuso-Mateos JL (2020). Exploring the effect of loneliness on all-cause mortality: Are there differences between older adults and younger and middle-aged adults? Social Science & Medicine, 258, 113087. 10.1016/j.socscimed.2020.113087 [DOI] [PubMed] [Google Scholar]
- Lee R, & Mason A (Eds.). (2011). Population aging and the generational economy: A global perspective Edward Elgar Publishing. [Google Scholar]
- Lee R, & Mason A (2010). Some macroeconomic aspects of global population aging. Demography, 47, S151–S172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lutz W (2013). Demographic metabolism: A predictive theory of socioeconomic change. Population and Development Review, 38, 283–301. 10.1111/j.1728-4457.2013.00564.x [DOI] [Google Scholar]
- Lutz W, & KC S (2011). Global human capital: Integrating education and population. Science, 333(6042), 587–592. [DOI] [PubMed] [Google Scholar]
- Lutz W, & Muttarak R (2017). Forecasting societies’ adaptive capacities through a demographic metabolism model. Nature Climate Change, 7(3), 177–184. 10.1038/nclimate3222 [DOI] [Google Scholar]
- Lutz W, & Striessnig E (2016, March 31-April 2) Attitudes toward homosexuality change through the demographic metabolism: An international comparison [Conference presentation]. PAA 2016, Washington, D.C., United States. [Google Scholar]
- Macdonald SJ, Deacon L, Nixon J, Akintola A, Gillingham A, Kent J, … Highmore L (2018). ‘The invisible enemy’: Disability, loneliness and isolation. Disability & Society, 33(7), 1138–1159. 10.1080/09687599.2018.1476224 [DOI] [Google Scholar]
- Mair CA (2010). Social ties and depression: An intersectional examination of black and white community-dwelling older adults. Journal of Applied Gerontology, 29(6), 667–696. 10.1177/0733464809350167 [DOI] [Google Scholar]
- Mair CA (2019). Alternatives to Aging Alone?: “Kinlessness” and the importance of friends across European contexts. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 74(8), 1416–1428. 10.1093/geronb/gbz029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masi CM, Chen HY, Hawkley LC, & Cacioppo JT (2011). A meta-analysis of interventions to reduce loneliness. Personality and Social Psychology Review, 15(3), 219–266. 10.1177/1088868310377394 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morgan DJ, & Burholt V (2020). Loneliness as a biographical disruption - Theoretical implications for understanding changes in loneliness. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences [DOI] [PMC free article] [PubMed]
- Newmyer L, Verdery AM, Margolis R, & Pessin L (2021). Measuring older adult loneliness across countries. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 76(7), 1408–1414. 10.1093/geronb/gbaa109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nicolaisen M, & Thorsen K (2014). Who are lonely? Loneliness in different age groups (18–81 years old), using two measures of loneliness. International Journal of Aging and Human Development, 78(3), 229–257. 10.2190/AG.78.3.b [DOI] [PubMed] [Google Scholar]
- Nicolaisen M, & Thorsen K (2017). What are friends for? Friendships and loneliness over the lifespan - from 18 to 79 years. International Journal of Aging and Human Development, 84(2), 126–158. 10.1177/0091415016655166 [DOI] [PubMed] [Google Scholar]
- Nyqvist F, Nygård M, & Scharf T (2019). Loneliness amongst older people in Europe: A comparative study of welfare regimes. European Journal of Ageing, 16, 133–143. 10.1007/s10433-018-0487-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ong AD, Uchino BN, & Wethington E (2016). Loneliness and health in older adults: A mini-review and synthesis. Gerontology, 62, 443–449. 10.1159/000441651 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park J (2019). Lonely in Korea? You’re not alone. The Korea Herald Retrieved from http://www.koreaherald.com/view.php?ud=20190403000445
- Paul C, Ayis S, & Ebrahim S (2006). Psychological distress, loneliness and disability in old age. Psychology, Health and Medicine, 11(2), 221–232. 10.1080/13548500500262945 [DOI] [PubMed] [Google Scholar]
- Perlman D, & Peplau LA (1981). Toward a social psychology of loneliness. In Duck M & Gilmour R (Eds.), Personal relationships in disorder (pp. 31–56). Academic Press. [Google Scholar]
- Prince M, Patel V, Saxena S, Maj M, Maselko J, Phillips MR, & Rahman A (2007). No health without mental health. Lancet, 370, 859–877. 10.1016/S0140-6736(07)61238-0 [DOI] [PubMed] [Google Scholar]
- Prohaska T, Burholt V, Burns A, Golden J, Hawkley L, Lawlor B, … Fried L (2020). Consensus statement: Loneliness in older adults, the 21st century social determinant of health? BMJ Open, 10, e034967. 10.1136/bmjopen-2019-034967 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Putnam RD (2001). Bowling alone: The collapse and revival of American community. Simon and Schuster
- Radloff LS (1977). The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. 10.1177/014662167700100306 [DOI] [Google Scholar]
- Rainie L, & Wellman B (2012). Networked: The new social operating system MIT Press. [Google Scholar]
- Reher DS (1998). Family ties in Western Europe: Persistent contrasts. Population and Development Review, 24(2), 203–234. [Google Scholar]
- Reher DS, & Requena M (2018). Living alone in later life: A global perspective. Population and Development Review, 44(3), 427–454. 10.1111/padr.12149 [DOI] [Google Scholar]
- Rico-Uribe LA, Caballero FF, Olaya B, Tobiasz-Adamczyk B, Koskinen S, Leonardi M, … Miret M (2016). Loneliness, social networks, and health: A cross-sectional study in three countries. PLoS ONE, 11(1), e0145264. 10.1371/journal.pone.0145264 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rivers M, & Lee L (2019, February 8). Isolated and abandoned: The heartbreaking reality of old age in rural China. CNN Retrieved from https://www.cnn.com/2019/02/07/asia/china-elderly-people-new-year-intl/index.html
- Ryder N (1980). The Cohort Approach: Essays in the Measurement of Temporal Variation in Demographic Behavior Ayer Publishing. [Google Scholar]
- Sassler S (2010). Partnering across the life course: Sex, relationships, and mate selection. Journal of Marriage and Family, 72(3), 557–575. 10.1111/j.l741-3737.2010.00718.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saure PU, & Zoabi H (2011). Retirement age across countries: The role of occupations. Available at SSRN 1940452
- Sonnega A, Faul JD, Ofstedal MB, Langa KM, Phillips JWR, & Weir DR (2014). Cohort profile: The Health and Retirement Study (HRS). International Journal of Epidemiology, 43(2), 576–585. 10.1093/ije/dyu067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stevens NL, & van Tilburg TG (2011). Cohort differences in having and retaining friends in personal networks in later life. Journal of Social and Personal Relationships, 28(1), 24–43. 10.1177/0265407510386191 [DOI] [Google Scholar]
- Stickley A, Koyanagi A, Roberts B, Richardson E, Abbott P, Tumanov S, & Mckee M (2013). Loneliness: Its correlates and association with health behaviours and outcomes in nine countries of the former Soviet Union. PLoS ONE, 8(7), e67978. 10.1371/journal.pone.0067978 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stokes AC, Xie W, Lundberg DJ, Glei DA, & Weinstein MA (2021). Loneliness, social isolation, and all-cause mortality in the United States. SSM - Mental Health, 1, 100014. 10.1016/j.ssmmh.2021.100014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Striessnig E, & Lutz W (2016). Demographic strengthening of European identity. Population and Development Review, 42(2), 305–311. 10.1111/j.1728-4457.2016.00133.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suanet B, & Huxhold O (2020). Cohort difference in age-related trajectories in network size in old age: Are networks expanding? The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 75(1), 137–147. 10.1093/geronb/gbx166 [DOI] [PubMed] [Google Scholar]
- Sundström G, Fransson E, Malmberg B, & Davey A (2009). Loneliness among older Europeans. European Journal of Ageing, 6, 267–275. 10.1007/s10433-009-0134-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Takagi E, & Saito Y (2020). Japanese older adults’ loneliness, family relationships and mortality: Does one’s living arrangement make a difference? Geriatrics and Gerontology International, 20, 156–160. 10.1111/ggi.13837 [DOI] [PubMed] [Google Scholar]
- Troya MS (2019, April). Más de 850.000 personas mayores de 80 años viven solas en España. El País
- United Nations. (2019). World population prospects 2019 https://population.un.org/wpp/
- Vahia IV, Jeste DV, & Reynolds CF (2020). Older adults and the mental health effects of COVID-19. JAMA, 324(22), 2253–2254. 10.1093/geronb/gbaa120 [DOI] [PubMed] [Google Scholar]
- Valtorta NK, Kanaan M, Gilbody S, Ronzi S, & Hanratty B (2016). Loneliness and social isolation as risk factors for coronary heart disease and stroke: Systematic review and meta-analysis of longitudinal observational studies. Heart, 102, 1009–1016. 10.1136/heartjnl-2015-308790 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Tilburg TG (2021). Emotional, social, and existential loneliness before and during the COVID-19 pandemic: Prevalence and risk factors among Dutch older adults. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 1–6. 10.1093/geronb/gbab101 [DOI] [PMC free article] [PubMed]
- Van Winkle Z, Ferragina E, & Recchi E (2021). The unexpected decline in feelings of depression among adults ages 50 and older in 11 European countries amid the COVID-19 pandemic. Socius, 7, 1–11. 10.1177/23780231211032741 [DOI] [Google Scholar]
- Verdery AM (2019). Modeling the future of China’s changing family structure to 2100. In Eberstadt N (Ed.), China’s next big demographic problems: Urbanization and family structure (pp. 23–78). The American Enterprise Institute. [Google Scholar]
- Verdery AM, & Margolis R (2017). Projections of white and black older adults without living kin in the United States, 2015 to 2060. Proceedings of the National Academy of Sciences of the United States of America, 114(42), 11109–11114. 10.1073/pnas.1710341114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verdery AM, Newmyer L, Wagner B, & Margolis R (2021). National profiles of coronavirus disease 2019 mortality risks by age structure and preexisting health conditions. The Gerontologist, 61(1), 71–77. 10.1093/geront/gnaa152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vézina S, & Bélanger A (2019). Impacts of education and immigration on the size and skills of the future workforce. Demographic Research, 41, 331–366. 10.4054/demres.2019.41.12 [DOI] [Google Scholar]
- Vézina S, Bélanger A, Sabourin P, & Marois G (2019). Literacy skills of the future Canadian working-age population: Assessing the skill gap between the foreign- and Canadian-born. Canadian Studies in Population 46, 46(1), 5–25. [Google Scholar]
- Victor CR, & Bowling A (2012). A longitudinal analysis of loneliness among older people in Great Britain. Journal of Psychology, 146(3), 313–331. 10.1080/00223980.2011.609572 [DOI] [PubMed] [Google Scholar]
- Victor CR, & Yang K (2012). The prevalence of loneliness among adults: A case study of the United Kingdom. The Journal of Psychology, 146(1–2), 85–104. 10.1080/00223980.2011.613875 [DOI] [PubMed] [Google Scholar]
- Vigo D, Thornicroft G, & Atun R (2016). Estimating the true global burden of mental illness. The Lancet Psychiatry, 3(2), 171–178. 10.1016/S2215-0366(15)00505-2 [DOI] [PubMed] [Google Scholar]
- Weiss RS (1973). Loneliness: The experience of emotional and social isolation MIT Press. [Google Scholar]
- Weissman MM, Bland R, Joyce PR, Newman S, Wells JE, & Wittchen H-U (1993). Sex differences in rates of depression: Cross-national perspectives. Journal of Affective Disorders, 29, 77–84. 10.1016/0165-0327(93)90025-F [DOI] [PubMed] [Google Scholar]
- Whisman MA (2010). Loneliness and the metabolic syndrome in a population-based sample of middle-aged and older adults. Health Psychology, 29(5), 550–554. 10.1037/a0020760 [DOI] [PubMed] [Google Scholar]
- Whiteford HA, Ferrari AJ, Degenhardt L, Feigin V, & Vos T (2015). The global burden of mental, neurological and substance use disorders: An analysis from the global burden of disease study 2010. PLoS ONE, 10(2), e0116820. 10.1371/journal.pone.0116820 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson RS, Krueger KR, Arnold SE, Schneider JA, Kelly JF, Barnes LL, … Bennett DA (2007). Loneliness and risk of alzheimer disease. Archives of General Psychiatry, 64, 234–240. [DOI] [PubMed] [Google Scholar]
- World Health Organization (WHO). (2021). Constitution https://www.who.int/about/who-we-are/constitution
- World Health Organization (WHO). (2013). Investing in mental health: Evidence for action https://www.who.int/mental_health/publications/financing/investing_in_mh_2013/en/
- Yang K, & Victor C (2011). Age and loneliness in 25 European nations. Ageing and Society, 31, 1368–1388. 10.1017/S0144686X1000139X [DOI] [Google Scholar]
- Yeginsu C (2018, January 17). UK appoints minister for loneliness. The New York Times Retrieved from https://www.nytimes.com/2018/01/17/world/europe/uk-britain-loneliness.html
- Zimmer Z, Martin LG, Nagin DS, & Jones BL (2012). Modeling disability trajectories and mortality of the oldest-old in China. Demography, 49(1), 291–314. 10.1007/s [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
This study uses data from and United Nations World Population Prospects (https://population.un.org/wpp/) and Gateway to Global Aging (https://g2aging.org/). Registered users can access and download the data.