

Abstract
Background
Higher ambient temperature and air pollution may contribute to increased risk of behaviors harmful to oneself or to others; however, quantitative evidence is limited. We examined the relationship of deaths due to suicide and homicide with temperature and air pollution in California—a state prone to high levels of both exposures.
Method
California death certificates from 2014 to 2019 were used to identify deaths due to suicide and homicide. Residential data for decedents were used to assign exposure to daily temperature (maximum[Tmax], minimum[Tmin]) and daily average air pollution concentrations (particulate matter <10 μm[PM10] and <2.5 μm[PM2.5], nitrogen dioxide[NO2], ozone[O3]). Tmin served as a surrogate for nighttime temperature. A time-stratified case-crossover study design using conditional logistic regression was used to assess the effects of daily exposure to temperature and air pollutants on suicide and homicide mortality, adjusting for relative humidity. Effect modification by sex and age was assessed.
Results
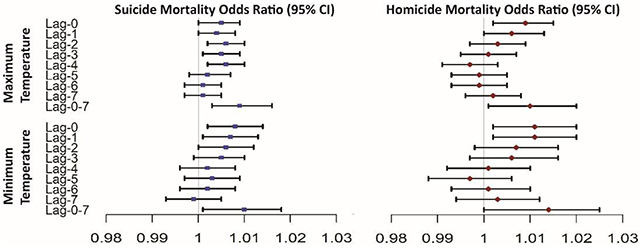
We observed 24,387 deaths due to suicide and 10,767 deaths due to homicide. We found a monotonic temperature association for both outcomes. A 5°C increase in Tmax at lag-2 and Tmin at lag-0 was associated with 3.1% (95% confidence interval [CI]: 1.1%–5.2%) and 3.8% (95%CI: 0.9%–6.8%) increased odds of death due to suicide, respectively. The increased odds of homicide mortality per 5°C increase in Tmax at lag-0 and Tmin at lag-1 were 4.9% (95%CI: 1.6%–8.1%) and 6.2% (95%CI: 1.6%–11.0%), respectively. No air pollutant associations were statistically significant. Temperature associations were robust after adjustment for PM2.5. Some temperature effects were larger among women for suicide and men for homicide mortality, and among those over age 65 years for both outcomes.
Conclusion
Risk of suicide and homicide mortality increases with increasing daily ambient temperatures. Findings have public health relevance given anticipated increases in temperatures due to global climate change.
Keywords: Temperature, Air pollution, Suicide, Homicide, Mortality
Graphical Abstrcat
INTRODUCTION
Violent behavior is a major public health problem in the United States (US) and worldwide. Deaths due to suicide and homicide (commonly referred to as violent deaths) are a major cause of premature death for young adults in the United States (CDC, 2019). For persons aged 10-24 in 2017, suicide and homicide followed closely behind unintentional injuries, with suicide ranking second and homicide ranking as the third leading cause of death (Heron, 2019).
Climate change affects a wide range of human health outcomes. Recent evidence has elucidated the impacts of climatic conditions, such as changes to high temperature, excessive precipitation and drought, on behavioral and mental health related outcomes (Burke et al., 2018; To et al., 2021). The rise of air pollution and temperature due to climate change is highly relevant for many areas around the world, including the western United States (McClure and Jaffe, 2018; Xie et al., 2022). California in particular is prone to elevated temperatures and associated increased frequency and severity of wildfires (Williams et al., 2019), which affects air quality by increasing concentrations of particulate matter.
Unlike other health outcomes, there is limited quantitative evidence on the associations between climatic conditions (and their impacts) and mental health related outcomes. Several studies have observed associations between temperature and air pollution with violent deaths (Burkhardt et al., 2020; Gates et al., 2019; Helama et al., 2013; Kim et al., 2011; Liu et al., 2021; Thompson et al., 2018), and recent work suggests that these associations vary by location. (Xu et al., 2020). Xu et al. (2020) recently examined the effect of increased temperature on death due to homicide in nine US cities and found associations only in Chicago and New York. A California study reported an increase in emergency department visits for mental health related outcomes, including depression, self-harm/suicide, and homicide/inflicted injury associated with daily mean levels of PM2.5 and O3 (Nguyen et al., 2021). Regional-scale studies are needed to characterize the associations between environmental factors and violent deaths. California is a climate vulnerable area: since the 1970s, the state has experienced a progressive increase in average summertime temperature of approximately 1.4 °C (Williams et al., 2019). Wildfire is one of the major drivers of increased air pollution concentration in the Western United States (McClure and Jaffe, 2018). Yet, studies that have evaluated associations between temperature and air pollution with violent deaths lacked fine temporal resolution. An ecological study reported an association between monthly average temperature and suicide rate in five California counties; however, monthly average data limits the ability to examine acute effects (Cheng et al., 2021). Notably, no previous study has comprehensively studied the effect of both daily temperature and air pollution on the risk of suicide and homicide mortality across the state of California.
In this study, we examined the associations between acute temperature and air pollution exposure with deaths due to suicide and homicide, and potential effect modification by sex and age. We leveraged six years of mortality data in California and used decedent’s residential address information to estimate exposure to temperature and air pollution on the day of death, as well as on each of the seven preceding days.
METHODS
Study Design
A time-stratified case-crossover study design was used to assess the relationship between temperature (Tmax and Tmin) and air pollution (particulate matter <10 μm [PM10] and <2.5 μm [PM2.5], nitrogen dioxide [NO2], ozone [O3]) with suicide and homicide mortality. This study design allows individuals to serve as their own control, thus allowing for control of all time-independent (within the same month) factors such as age, race/ethnicity, education level, pre-existing chronic disease, and socioeconomic status. Rather than recording case individuals, case days are used. Case days are the day of an individual’s death, and control days are days in the weeks prior to or following the individual’s death within the same month and falling on the same day of the week. For example, if an individual’s death occurred on the third Tuesday of March 2017, the first, second, and fourth Tuesdays of March 2017 were used as control days.
Definition of Outcome
The California Department of Public Health’s vital statistics provided death certificate data for deaths due to all causes occurring in California from 1 January 2014 to 31 December 2019, supplying demographical data related to the decedent. Using the 10th revision of the International Classification of Diseases (ICD-10), these data were subset to specific immediate causes of death listed on the decedent’s death certificate: deaths due to suicide and homicide. Suicide was defined as intentional self-harm through various methods (ICD-10 codes X60 -X84, Y87.0), while homicide was characterized as assault through several means, including sequelae of assault (ICD-10 codes X85-Y09, Y87.1). Management and analysis of these data were approved by the Committee for the Protection of Human Subjects for the state of California.
Exposure Assessment
Data for temperature, defined as continuous daily temperature measured in degrees Celsius (°C), were assessed using daily gridMET, a gridded re-analysis dataset estimating daily meteorological conditions for the continental United States with 4 km resolution (Abatzoglou, 2013). Using nearest grid points, census tracts were assigned daily maximum (Tmax) and minimum (Tmin, a surrogate for nighttime) temperatures, and corresponding relative humidity (RHmax and RHmin also from gridMET) during the years 2014 to 2019. Air pollutants examined include daily (24-hour) mean concentrations of PM2.5, PM10, and NO2 and daily maximum 8-hour average O3. Ambient pollutant concentrations were based on data from the ambient air quality monitoring system obtained from the US Environmental Protection Agency’s Air Quality System for 2014 to 2019. Estimates of pollutant concentration for census tract population weighted centroids were based on inverse distance squared weighting of observations from up to four nearby (<50 km) monitoring locations (Wong et al., 2004). Prior work by our group has validated this approach for estimating exposure at census tract resolution (Eckel et al., 2016). Decedents’ residential census tracts obtained from the death certificates were used for linkage with exposure data. We examined same day (lag 0) through up to seven days prior (lag 7) exposure, with each lag examined in a separate model.
Statistical Analysis
Conditional logistic regression models were fit to assess the effects of temperature (Tmax and Tmin) and air pollution (PM10, PM2.5, NO2, and O3) on suicide and homicide. Specifically, conditional logistic regression models were used to evaluate the association between deaths due to suicides and homicides with temperature and air pollution for each exposure-outcome pairing separately. Single exposure models of temperature and each pollutant across all lag days were evaluated. Potential nonlinearity was examined by plotting exposure–response (E–R) curves using a natural cubic spline with 3 degrees of freedom (df). Additionally, potential nonlinearity was tested by including a polynomial terms (i.e., quadratic, cubic) for exposure in the models. We performed a single-day lag model (i.e., a linear parameterization for each of the individual lags) for temperatures and air pollutants. Further, a distributed non-linear lag model (DLNM) was also applied to estimate the cumulative effects of lag exposures days (Gasparrini, 2011; Gasparrini et al., 2010). With DLNM, we modeled the nonlinear exposure-outcome associations using natural spline functions. The df for the natural spline was chosen based on lowest Akaike information criterion (AIC) value. Based on AIC, the linear model provided the best fit. The general form of the case-crossover conditional logistic model is logit( where πm is either suicide or homicide mortality, XE is one of the exposures (either temperature or a pollutant), XRH is relative humidity, ns(XRH) denotes a natural cubic spline with 3 degrees of freedom, and XS is any additional covariates included for sensitivity analyses as mentioned below.
Effect modification by sex and age was also evaluated. Studies report that the elderly are more susceptible to high temperatures (Gronlund et al., 2016; Hopp et al., 2018; Kim et al., 2011; Son et al., 2011; Wang et al., 2016); however, a growing recent literature suggests that the largest temperature effects might be found among younger adults and middle aged populations (Kingsley et al., 2016; Sun et al., 2021; Zhao et al., 2017). To examine the temperature effects on suicide or homicide mortality among young adults, middle aged, and older adults we conducted an age interaction model by categorizing age into the following groups: ≤24 years, 24–65 years, and ≥65 years. Wald chi-squared tests were performed to assess the interaction. All models were adjusted for same lag day relative humidity using a natural cubic spline with 3 df to control for potential confounding (Kim et al., 2010; Lin et al., 2016; Xu et al., 2020). For air pollution models, we adjusted for same lag day temperature (with natural cubic spline of 3 df) in addition to relative humidity of same lag day. Temperature effects may be confounded by air pollution, particularly PM2.5 (Rahman et al., 2022; Tian et al., 2019), thus in a sensitivity analysis, both Tmax and Tmin models were adjusted for PM2.5 to evaluate the robustness of association. O3 may be on the causal pathway between temperature and health (Massazza et al., 2022; Reid et al., 2012), thus we did not adjust for O3 in models for temperature effects.
Odds ratios (OR) of suicide or homicide mortality (separately) associated with a 1°C increase in temperature and an inter-quartile range increase in air pollutant concentrations are reported. All analyses were performed using R Statistical Software (v3.5.2; R Core Team 2021). R packages “survival”, “splines”, and “dlnm” were used for data analysis.
RESULTS
From 1 January 2014 to 31 December 2019 we identified 1,514,292 deaths in the state of California. Of these, 24,387 were due to suicide and 10,767 were due to homicide (Table 1). The mean (standard deviation) age at death due to suicide was 48.9 (19.3) years and at death due to homicide was 35.3 (16.0) years. For both outcomes, more decedents were men than women.
Table 1.
Distribution of demographic and exposure characteristics among decedents with death due to suicide or homicide. Mean (standard deviations) presented unless otherwise noted.
| Decedents’ characteristic | Suicide | Homicide |
|---|---|---|
| N | 24,387 | 10,767 |
| Age, years | 48.9 (19.3) | 35.3 (16.5) |
| Sex, n (%) | ||
| Men | 18,813 (77.1) | 8,909 (82.7) |
| Women | 5,574 (22.9) | 1,858 (17.3) |
| Environmental exposure on case days | ||
| Maximum Temperature, °C | 24.27 (7.10) | 24.56 (7.11) |
| Minimum Temperature, °C | 11.81 (5.27) | 12.14 (5.31) |
| PM10, μg/m3 | 25.90 (18.61) | 28.29 (18.31) |
| PM2.5, μg/m3 | 10.08 (8.02) | 10.82 (8.16) |
| NO2, ppb | 10.40 (7.40) | 11.49 (7.70) |
| O3, ppb | 43.45 (14.33) | 43.49 (15.05) |
| Maximum Relative Humidity, % | 80.04 (18.24) | 79.40 (17.90) |
| Minimum Relative Humidity, % | 37.00 (18.41) | 36.51 (18.24) |
| Environmental exposure on control days | ||
| Maximum Temperature, °C | 24.21 (7.11) | 24.40 (7.09) |
| Minimum Temperature, °C | 11.79 (5.27) | 12.09 (5.27) |
| PM10, μg/m3 | 25.83 (17.02) | 28.00 (17.63) |
| PM2.5, μg/m3 | 10.10 (8.10) | 10.75 (8.31) |
| NO2, ppb | 10.36 (7.37) | 11.40 (7.68) |
| O3, ppb | 43.38 (14.33) | 43.40 (15.04) |
| Maximum Relative Humidity, % | 80.26 (18.03) | 79.82 (17.75) |
| Minimum Relative Humidity, % | 37.19 (18.39) | 36.93 (18.24) |
Descriptive statistics for temperature, relative humidity, and air pollutants on both case and control days for each outcome are presented in Table 1. The mean Tmax on days when suicide and homicide deaths occurred was 24.3°C and 24.6°C, respectively. For suicide mortality, the mean concentrations of PM10, PM2.5, NO2, and O3 on case days were 25.9 μg/m3, 10.1 μg/m3, 10.4 ppb, and 43.5 ppb, respectively. For homicide mortality, the mean concentrations of PM10, PM2.5, NO2, and O3 on case days were 28.3 μg/m3, 10.8 μg/m3, 11.5 ppb, and 43.5 ppb, respectively.
We observed a monotonic association between daily temperature and increased odds of death due to suicide and homicide, with no clear evidence of a threshold (Figure 1). Evaluation of polynomial terms for exposure revealed no evidence of non-linearity in the association between temperature and either mortality outcome (data not shown). Tmax was statistically significantly associated with deaths due to suicide across several lag-days exposures (lag-0 to lag-4), with largest association at lag-2 (Table 2). A 1°C increase in Tmax at lag-2 was associated with higher odds of death due to suicide by 0.6 % (OR = 1.006; 95% CI: 1.002, 1.010). The cumulative effect of Tmax over 0-7 lag days was 0.9% (OR = 1.009; 95% CI: 1.003, 1.106). Similarly, Tmin at lag-0 to lag-1 was statistically significantly associated with death due to suicide, with the largest association at lag-0. A 1°C increase in same day (i.e., lag-0) Tmin was associated with 0.9% (OR = 1.009; 95% CI: 1.002, 1.015) higher odds of death due to suicide. The cumulative effect of Tmin over 0-7 lag days was slightly higher than from the single lag day effect (OR = 1.010; 95% CI: 1.001, 1.020). A statistically significant association was found between same-day Tmax and death due to homicide. For every 1°C increase in Tmax, the odds of homicide mortality was 0.8% higher (OR = 1.008; 95% CI: 1.002, 1.014). Similar results were observed for Tmin with both lag-0 and lag-1 exposures. For every 1°C increase in one day prior Tmin (i.e., lag-1), the odds of homicide mortality was 1.1% higher (OR=1.002; 95% CI: 1.020, 1.110). The cumulative effects of Tmin on suicide and homicide mortality were slightly higher from single lag day effect. The association of Tmax and Tmin with suicide and homicide mortality were not markedly different in a sensitivity analysis adjusting for PM2.5 (Supplementary Table 1).
Figure 1.

Exposure-response curves for associations between daily maximum ambient temperature and suicide (lag-2) and homicide (lag-0) mortality. Solid lines represent mean odds ratios and dashed lines represent 95% confidence intervals.
Table 2.
Associations of maximum and minimum temperature with deaths due to suicide and deaths due to homicide. Results are shown for same day exposure (Lag-0) to 7 days prior exposure (Lag-7), per 1°C increase in temperature.
| Lag | Suicide OR (95% CI) | Homicide OR (95% CI) | |
|---|---|---|---|
| Maximum Temperature | 0 | 1.005 (1.000, 1.009) | 1.009 (1.002, 1.015) |
| 1 | 1.004 (1.000, 1.008) | 1.006 (1.000, 1.013) | |
| 2 | 1.006 (1.002, 1.010) | 1.003 (0.997, 1.009) | |
| 3 | 1.005 (1.001, 1.009) | 1.001 (0.995, 1.007) | |
| 4 | 1.006 (1.002, 1.010) | 0.997 (0.991, 1.003) | |
| 5 | 1.002 (0.998, 1.007) | 0.999 (0.993, 1.005) | |
| 6 | 1.001 (0.997, 1.005) | 0.999 (0.993, 1.005) | |
| 7 | 1.001 (0.997, 1.005) | 1.002 (0.996, 1.008) | |
| 0-7 | 1.009 (1.003, 1.016) | 1.010 (1.001, 1.020) | |
| Minimum Temperature | 0 | 1.008 (1.002, 1.014) | 1.011 (1.002, 1.020) |
| 1 | 1.007 (1.001, 1.013) | 1.011 (1.002, 1.020) | |
| 2 | 1.006 (1.000, 1.012) | 1.007 (0.998, 1.016) | |
| 3 | 1.005 (0.999, 1.010) | 1.006 (0.997, 1.016) | |
| 4 | 1.002 (0.996, 1.008) | 1.001 (0.992, 1.010) | |
| 5 | 1.003 (0.997, 1.009) | 0.997 (0.988, 1.006) | |
| 6 | 1.002 (0.996, 1.008) | 1.001 (0.993, 1.010) | |
| 7 | 0.999 (0.993, 1.005) | 1.003 (0.994, 1.012) | |
| 0-7 | 1.010 (1.001, 1.018) | 1.014 (1.000, 1.025) |
Models were adjusted for same lag day relative humidity.
Air pollutants associations with suicide mortality were largely positive although they did not reach statistical significance. In contrast, air pollutants associations with homicide mortality were largely null (Table 3). The cumulative effects of air pollutants on both suicide and homicide mortality were larger than single day lag effects but these results are not statistically significant either. Since_no significant increase in death due to suicide or homicide was observed for any air pollutant, analyses for effect modification by sex or age were restricted to the temperature exposures.
Table 3.
Associations of PM10, PM2.5, NO2, and O3 with deaths due to suicide and deaths due to homicide. Results are shown for same day exposure (Lag-0) to 7 days prior exposure (Lag-7), per inter-quartile range (IQR) increase in air pollutants concentrations.
| Pollutants | Lag | Suicide OR (95% CI) | Homicide OR (95% CI) |
|---|---|---|---|
| PM10 | 0 | 1.012 (0.990, 1.032) | 1.016 (0.982, 1.051) |
| 1 | 1.007 (0.983, 1.030) | 0.982 (0.945, 1.019) | |
| 2 | 1.008 (0.990, 1.027) | 0.991 (0.954, 1.028) | |
| 3 | 1.017 (0.993, 1.040) | 0.988 (0.950, 1.027) | |
| 4 | 1.017 (0.992, 1.040) | 0.972 (0.934, 1.011) | |
| 5 | 1.007 (0.982, 1.030) | 0.965 (0.926, 1.004) | |
| 6 | 1.018 (0.995, 1.042) | 0.975 (0.936, 1.012) | |
| 7 | 0.973 (0.950, 0.998) | 0.988 (0.952, 1.023) | |
| 0-7 | 1.022 (0.979, 1.066) | 0.961 (0.897, 1.030) | |
| PM2.5 | 0 | 1.000 (0.987, 1.013) | 1.002 (0.945, 1.060) |
| 1 | 1.003 (0.990, 1.016) | 0.966 (0.906, 1.025) | |
| 2 | 1.010 (0.996, 1.022) | 0.979 (0.920, 1.035) | |
| 3 | 1.005 (0.992, 1.019) | 0.995 (0.938, 1.051) | |
| 4 | 1.003 (0.990, 1.016) | 0.961 (0.904, 1.018) | |
| 5 | 1.006 (0.993, 1.019) | 0.973 (0.917, 1.028) | |
| 6 | 0.998 (0.985, 1.011) | 0.979 (0.922, 1.034) | |
| 7 | 0.998 (0.985, 1.011) | 0.979 (0.922, 1.037) | |
| 0-7 | 1.011 (0.991, 1.031) | 0.981 (0.950, 1.012) | |
| NO2 | 0 | 0.993 (0.958, 1.027) | 0.986 (0.888, 1.085) |
| 1 | 0.993 (0.958, 1.028) | 1.023 (0.926, 1.122) | |
| 2 | 0.988 (0.954, 1.023) | 0.970 (0.872, 1.067) | |
| 3 | 1.018 (0.983, 1.053) | 0.926 (0.830, 1.023) | |
| 4 | 1.012 (0.978, 1.047) | 0.970 (0.872, 1.067) | |
| 5 | 1.026 (0.991, 1.061) | 0.975 (0.881, 1.071) | |
| 6 | 1.014 (0.980, 1.048) | 0.975 (0.879, 1.073) | |
| 7 | 0.988 (0.954, 1.021) | 0.926 (0.830, 1.023) | |
| 0-7 | 1.020 (0.962, 1.082) | 0.953 (0.870, 1.044) | |
| O3 | 0 | 0.996 (0.961, 1.032) | 0.954 (0.901, 1.005) |
| 1 | 1.004 (0.968, 1.039) | 0.938 (0.885, 0.989) | |
| 2 | 1.014 (0.979, 1.050) | 0.972 (0.918, 1.025) | |
| 3 | 1.002 (0.966, 1.037) | 0.993 (0.942, 1.046) | |
| 4 | 1.025 (0.989, 1.060) | 0.996 (0.943, 1.048) | |
| 5 | 1.009 (0.973, 1.044) | 0.996 (0.943, 1.050) | |
| 6 | 1.030 (0.995, 1.066) | 0.956 (0.903, 1.007) | |
| 7 | 1.025 (0.989, 1.060) | 1.007 (0.954, 1.060) | |
| 0-7 | 1.047 (0.983, 1.115) | 0.922 (0.839, 1.011) |
Models were adjusted for same lag day temperature and relative humidity. IQR for PM10, PM2.5, NO2, and O3 were 16.8 μg/m3, 6.0 μg/m3, 8.9 ppb, and 17.7 ppb, respectively.
In the sex-specific analysis, we found some evidence that the effects of temperature on suicide mortality were larger among women [ORmen = 1.004 (95% CI: 0.997, 1.010) vs. ORwomen = 1.019 (95% CI: 1.007, 1.032, interaction P-value=0.03) for 1°C increase in Tmin at lag-1], whereas for the homicide mortality the temperature effect estimates were larger among men [ORmen = 1.012 (95% CI: 1.005, 1.018) vs. ORwomen = 0.995 (95% CI: 0.982, 1.008), P-int=0.02) for 1°C increase in Tmax at lag-0] (Table 4). Our age-specific model provided some evidence that the effects of temperature on both suicide and homicide mortality were larger among the elderly (decedents aged over 65 years) (Table 5 & 6). For example, the odds ratio of suicide mortality for a 1°C increase in same-day (e.g., lag-0) Tmax were 0.994 (95% CI: 0.984, 1.005) for ≤ 24 years old age group, 1.003 (95% CI: 0.998, 1.008) for between 24 and 65 years old age group, and 1.016 (95% CI: 1.007, 1.024) for ≥ 65 years old age group (global interaction P-value = <0.01).
Table 4.
Sex-specific effect estimates (odd ratios) of suicide and homicide mortality for exposure to maximum and minimum temperature. Results are shown for same-day exposure (Lag-0) to 7 days prior exposure (Lag-7), per 1°C increase in temperature.
| Suicide |
Homicide |
||||||
|---|---|---|---|---|---|---|---|
| Lag | Men (N=18,813) | Women (N=5,574) | P | Men (N=8,909) | Women (N=1,858) | P | |
| Maximum Temperature | 0 | 1.005 (1.000, 1.009) | 1.004 (0.996, 1.012) | 0.8 7 | 1.012 (1.005, 1.018) | 0.995 (0.982, 1.008) | 0.02 |
| 1 | 1.004 (0.999, 1.008) | 1.007 (0.999, 1.014) | 0.4 9 | 1.009 (1.002, 1.016) | 0.993 (0.980, 1.007) | 0.03 | |
| 2 | 1.005 (1.000, 1.009) | 1.012 (1.004, 1.020) | 0.1 1 | 1.003 (0.996, 1.010) | 1.004 (0.991, 1.017) | 0.8 8 | |
| 3 | 1.003 (0.999, 1.008) | 1.010 (1.002, 1.018) | 0.1 2 | 1.001 (0.994, 1.008) | 1.001 (0.988, 1.014) | 0.9 9 | |
| 4 | 1.005 (1.001, 1.010) | 1.008 (1.000, 1.016) | 0.5 5 | 0.996 (0.990, 1.003) | 1.000 (0.987, 1.014) | 0.5 8 | |
| 5 | 1.002 (0.998, 1.007) | 1.002 (0.994, 1.010) | 0.9 3 | 0.997 (0.991, 1.004) | 1.008 (0.994, 1.021) | 0.1 6 | |
| 6 | 1.002 (0.998, 1.007) | 0.997 (0.989, 1.005) | 0.2 3 | 0.998 (0.991, 1.004) | 1.004 (0.991, 1.018) | 0.3 4 | |
| 7 | 1.002 (0.997, 1.006) | 0.999 (0.991, 1.007) | 0.5 6 | 1.002 (0.995, 1.008) | 1.003 (0.990, 1.016) | 0.8 8 | |
| Minimum Temperature | 0 | 1.007 (1.000, 1.014) | 1.010 (0.998, 1.023) | 0.6 5 | 1.012 (1.002, 1.022) | 1.008 (0.987, 1.029) | 0.7 5 |
| 1 | 1.004 (0.997, 1.010) | 1.019 (1.007, 1.032) | 0.0 3 | 1.011 (1.001, 1.021) | 1.010 (0.990, 1.032) | 0.9 4 | |
| 2 | 1.004 (0.997, 1.010) | 1.014 (1.002, 1.027) | 0.1 4 | 1.006 (0.996, 1.016) | 1.009 (0.989, 1.030) | 0.7 9 | |
| 3 | 1.004 (0.997, 1.010) | 1.008 (0.996, 1.021) | 0.4 9 | 1.003 (0.994, 1.013) | 1.020 (1.000, 1.042) | 0.1 5 | |
| 4 | 1.001 (0.994, 1.008) | 1.005 (0.993, 1.017) | 0.5 6 | 1.001 (0.991, 1.011) | 1.004 (0.983, 1.024) | 0.8 1 | |
| 5 | 1.003 (0.996, 1.009) | 1.005 (0.993, 1.017) | 0.7 5 | 0.995 (0.986, 1.005) | 1.006 (0.986, 1.027) | 0.3 3 | |
| 6 | 1.003 (0.996, 1.009) | 0.999 (0.987, 1.011) | 0.6 2 | 1.001 (0.991, 1.011) | 1.003 (0.983, 1.023) | 0.8 8 | |
| 7 | 0.999 (0.993, 1.005) | 0.999 (0.987, 1.011) | 0.9 7 | 1.004 (0.994, 1.014) | 0.998 (0.979, 1.018) | 0.6 2 | |
N represents number of deaths. Models were adjusted for same lag day relative humidity. Wald chi-squared test was performed to test heterogeneity between 2 groups.
Table 5.
Age-specific effect estimates (odd ratios) of deaths due to suicide for exposure maximum and minimum temperature. Results are shown for same-day exposure (Lag-0) to 7 days prior exposure (Lag-7), per 1°C increase in temperature.
| Lag | Age <= 24 (N=2,875) |
Age > 24 & < 65 (N=16,224) |
Age >= 65 (N=5,284) |
P | |
|---|---|---|---|---|---|
| Maximum Temperature | 0 | 0.994 (0.984, 1.005) | 1.003 (0.998, 1.008) | 1.016 (1.007, 1.024) | <0.01 |
| 1 | 0.997 (0.986, 1.008) | 1.002 (0.997, 1.007) | 1.014 (1.006, 1.023) | <0.01 | |
| 2 | 1.004 (0.994, 1.015) | 1.005 (1.000, 1.010) | 1.011 (1.003, 1.020) | 0.34 | |
| 3 | 1.004 (0.994, 1.015) | 1.004 (0.999, 1.009) | 1.007 (0.999, 1.015) | 0.82 | |
| 4 | 1.005 (0.995, 1.016) | 1.005 (1.000, 1.010) | 1.009 (1.001, 1.017) | 0.74 | |
| 5 | 0.998 (0.988, 1.009) | 1.002 (0.997, 1.006) | 1.007 (0.999, 1.015) | 0.36 | |
| 6 | 1.000 (0.990, 1.011) | 1.001 (0.996, 1.006) | 1.004 (0.996, 1.012) | 0.81 | |
| 7 | 1.004 (0.993, 1.014) | 1.000 (0.995, 1.004) | 1.003 (0.996, 1.011) | 0.61 | |
| Minimum Temperature | 0 | 0.997 (0.981, 1.014) | 1.006 (0.999, 1.013) | 1.018 (1.005, 1.030) | 0.13 |
| 1 | 1.005 (0.988, 1.022) | 1.005 (0.998, 1.012) | 1.014 (1.002, 1.027) | 0.44 | |
| 2 | 1.001 (0.985, 1.018) | 1.005 (0.998, 1.012) | 1.012 (1.000, 1.025) | 0.54 | |
| 3 | 0.998 (0.981, 1.015) | 1.003 (0.996, 1.010) | 1.013 (1.000, 1.026) | 0.28 | |
| 4 | 0.994 (0.978, 1.011) | 1.002 (0.995, 1.009) | 1.006 (0.994, 1.018) | 0.53 | |
| 5 | 0.995 (0.979, 1.011) | 1.005 (0.998, 1.012) | 1.002 (0.990, 1.015) | 0.55 | |
| 6 | 0.998 (0.982, 1.015) | 1.003 (0.996, 1.010) | 1.000 (0.988, 1.012) | 0.84 | |
| 7 | 0.997 (0.981, 1.014) | 1.000 (0.993, 1.007) | 0.996 (0.984, 1.008) | 0.80 |
N represents number of suicide deaths. Models were adjusted for same lag day relative humidity. Wald chi-squared test was performed to test heterogeneity across 3 groups.
Table 6.
Age-stratified effect estimates (odd ratios) of deaths due to homicide for exposure maximum and minimum temperature. Results are shown for same-day exposure (Lag-0) to 7 days prior exposure (Lag-7), per 1°C increase in temperature.
| Lag | Age <= 24 (N=3,174) |
Age > 24 & < 65 (N=6,967) |
Age >= 65 (N=623) |
P | |
|---|---|---|---|---|---|
| Maximum Temperature | 0 | 1.008 (0.997, 1.018) | 1.008 (1.001, 1.016) | 1.019 (0.996, 1.043) | 0.64 |
| 1 | 1.008 (0.997, 1.019) | 1.005 (0.997, 1.012) | 1.014 (0.992, 1.038) | 0.68 | |
| 2 | 1.007 (0.997, 1.018) | 1.000 (0.993, 1.008) | 1.010 (0.988, 1.034) | 0.43 | |
| 3 | 1.005 (0.995, 1.016) | 1.000 (0.992, 1.007) | 0.995 (0.972, 1.019) | 0.56 | |
| 4 | 0.999 (0.989, 1.010) | 0.997 (0.989, 1.004) | 0.992 (0.969, 1.015) | 0.82 | |
| 5 | 1.000 (0.989, 1.010) | 0.999 (0.992, 1.007) | 0.992 (0.969, 1.015) | 0.80 | |
| 6 | 0.999 (0.988, 1.009) | 1.000 (0.993, 1.007) | 0.982 (0.960, 1.005) | 0.33 | |
| 7 | 0.998 (0.988, 1.008) | 1.004 (0.997, 1.012) | 0.993 (0.970, 1.016) | 0.41 | |
| Minimum Temperature | 0 | 1.014 (0.998, 1.031) | 1.006 (0.995, 1.017) | 1.051 (1.015, 1.089) | 0.06 |
| 1 | 1.019 (1.002, 1.036) | 1.006 (0.994, 1.017) | 1.034 (0.999, 1.071) | 0.18 | |
| 2 | 1.011 (0.995, 1.028) | 1.003 (0.992, 1.014) | 1.023 (0.987, 1.06) | 0.46 | |
| 3 | 1.001 (0.985, 1.017) | 1.009 (0.998, 1.020) | 1.005 (0.969, 1.042) | 0.70 | |
| 4 | 0.994 (0.978, 1.010) | 1.005 (0.994, 1.016) | 0.995 (0.960, 1.031) | 0.51 | |
| 5 | 0.987 (0.971, 1.003) | 1.002 (0.992, 1.013) | 0.991 (0.957, 1.026) | 0.26 | |
| 6 | 0.989 (0.974, 1.005) | 1.008 (0.997, 1.019) | 0.991 (0.957, 1.026) | 0.14 | |
| 7 | 0.991 (0.975, 1.007) | 1.009 (0.999, 1.020) | 0.990 (0.956, 1.026) | 0.12 |
N represents number of homicide deaths. Models were adjusted for same lag day relative humidity. Wald chi-squared test was performed to test heterogeneity across 3 groups.
DISCUSSION
In this study of 24,387 deaths due to suicide and 10,767 deaths due to homicide from 2014 to 2019 in California, we observed that exposure to higher daily temperature, both minimum and maximum, was monotonically associated with increased odds of suicide and homicide mortality, without an evidence of threshold value. Results are consistent with a prior study reporting a monotonic association of temperature with hospital admissions and emergency department visits for multiple disease outcomes, including mental disorders (Qiu et al., 2022; Sun et al., 2021). The temperature associations with suicide and homicide mortality observed in this study were robust to adjustment for PM2.5. We observed some evidence of temperature-mortality effect heterogeneity by sex and age group. Some temperature-suicide mortality associations were larger among women and some temperature-homicide mortality associations were larger among men. The odds ratios for suicide and homicide deaths associated with some lags of higher daily temperature, particularly the most recent lag days, were larger among decedents aged 65 years and older. No associations were observed between air pollutants and either of the two mortality outcomes.
With progressing climate change, there is a pressing need to understand health effects associated with increased temperature. Exposure to higher daily temperature is associated with a range of health outcomes, including cardiovascular and respiratory mortality (Ban et al., 2017; Chen et al., 2018; Gasparrini et al., 2012), with a growing literature on the associations between temperature and mental health outcomes (Liu et al., 2021; Palinkas and Wong, 2020). Most studies have evaluated these relations with populations outside of the US, including in Western Europe, South Africa and Western/Southeast Asia (Gao et al., 2019; Gates et al., 2019; Helama et al., 2013; Kim et al., 2011; Lehmann et al., 2022; Liu et al., 2021; Thompson et al., 2018). Xu et al., recently examined temperature association with daily homicide mortality in nine US cities (Xu et al., 2020), and a California study examined the air pollution effects on mental health related emergency room visits (Nguyen et al., 2021). To our best knowledge, this is the first study to assess the associations of acute heat and pollution exposure with suicide and homicide mortality across the state of California. Elucidating these relations is an important area of research given the expected continued increase in heat and pollution exposure with the changing climate (McClure and Jaffe, 2018), and our study adds to the limited research in this area.
The magnitude of the associations between temperature and suicide mortality in our study was smaller than reported in a recent meta-analysis (Liu et al., 2021) of nine studies examining suicide mortality associations with daily temperature. The overall pooled results estimated that a 1°C increase in temperature was associated with a 1.2% increase in suicide mortality (RR = 1.012; 95% CI: 1.003–1.021). However, the magnitude of the association varied greatly among studies (I2=79.9%, p < 0.001). Only a few studies have examined the association between homicide and temperature. Most temperature-homicide mortality studies have been cross-sectional in design or were based on monthly or annual homicide mortality data (Mares, 2013; Rotton and Cohn, 2003; Takahashi, 2017; Tiihonen et al., 2017), making it difficult to evaluate the acute effects of temperature on homicide. To the best of our knowledge, few studies have considered daily level temperature and homicide exposure and used a case-crossover study design as we did in the current study (Gates et al., 2019; Xu et al., 2020). Both studies reported increased homicides with short-term increases in temperature with reported effect estimates that were somewhat larger compared with those in this current study. Gates et al. reported that a 1°C increase in same-day maximum temperature was associated with a 1.5% (95% CI: 1.3%–1.8%) increase in homicide mortality in South Africa (Gates et al., 2019). Xu et al. found statistically significant association in two US cities (New York and Chicago) among nine cities examined; the association was an 8.8% (95% CI: 1.5%–16.6%) increase per 5°C increase in daily mean temperature in New York and a 9.5% (95% CI: 4.3%–15.0%) increase in Chicago (Xu et al., 2020). It is worth mentioning that Los Angeles, the largest city in California comprising ~10% of the state’s population, was included in the Xu et al. study, but no association was observed (−7.7% [95% CI: −19.7%, 6.1%]). This may be due to a smaller number of homicide deaths in that study (N=3,256) compared to this current study (N=10,767). In addition, this current study included a broader geographical area (compared to a single city) with increased heterogeneity in temperature exposures and socio-demographic structures.
Several hypotheses have been proposed to explain the link between increased ambient temperature and the risk of violent deaths. Temperature increase is associated with aggressive behavior and with exacerbation of depressive disorders due to lack of social activities and interaction on a very hot day, and depression and aggression are both associated with suicide and homicide (Lehmann et al., 2022). In addition, hot temperature increases an individual’s discomfort resulting in disrupted sleep (Obradovich et al., 2022; Rifkin et al., 2018), and poor sleep is associated with aggression and violence (Kamphuis et al., 2012). It is important to note that our observed suicide and homicide mortality associations were for higher temperature across a range of temperatures, not only on hot days. The specific mechanisms underlying these relations maybe different depending on the specific temperature changes (e.g., cool to warm day, warm to warmer, hot to hotter, etc.). The underlying biological mechanism linking temperature with suicide and homicide remains unclear. Temperature increase may inhibit 5-hydroxytryptamine (5-HT) function in human beings, resulting in decrease in serotonin level with increase in temperature (Tiihonen et al., 2017; Xu et al., 2020). Serotonin level was found to be lower in people who committed suicide compared to those who died from other causes (Maes et al., 1995). Dysfunction in the serotonergic system is linked with depression and aggressive behavior (Carballo et al., 2009; Lehmann et al., 2022).
We did not find any statistically significant associations between short-term increases in air pollution and suicide or homicide mortality in this study, but there is growing literature suggesting that increased air pollution exposure is associated with suicide mortality (Davoudi et al., 2021). We found no study on air pollution and homicide mortality but two studies have reported associations between air pollution (PM2.5 and O3) and violent crime (Berman et al., 2019; Bondy et al., 2018). The physiological pathway of suicide and homicide mortality risk associated with air pollution is hypothesized to be neuroinflammatory, proposing that air particulates and gaseous pollutants act as irritants generating systemic and local inflammatory responses, leading to the exacerbation of mental disorders including depression and self-harm behaviors (Costa et al., 2014; Gładka et al., 2018).
We found some evidence of a possible larger temperature-suicide association among women. While this result is largely inconsistent with prior studies, it is consistent with studies of the general population which have found that women are at higher risk of attempting suicide, while men are more likely to complete it (Miranda-Mendizabal et al., 2019). A recent meta-analysis reported that the association between temperature and suicide did not vary by sex [men= 1.020 (95% CI: 1.002–1.038); women= 1.022 (95% CI: 0.998–1.046)] (Liu et al., 2021). Among two studies that examined temperature-homicide mortality association using daily level data (Gates et al., 2019; Xu et al., 2020), only one assessed sex-specific association (Gates et al., 2019). Gates et al. (2019) reported that temperature-homicide association did not vary by the sex of the victims, whereas we found the strongest associations among men. More research is needed to better understand this possible sex difference in the effect of temperature and homicide mortality.
Consistent with prior literature (Kim et al., 2011; Liu et al., 2021), we found that temperature associations with both suicide and homicide mortality were largest among the elderly. Elderly people may be more vulnerable to the temperature effects on suicide deaths possibly contributed by higher rates of depression due to having co-morbid disease conditions, disability, isolation, and relocation (Alexopoulos, 2005; Conwell et al., 2010; Kim et al., 2011). Depression is shown to be associated with aggression, violence, suicide, and homicide (Bénézech and Bourgeois, 1992; Hynan and Grush, 1986; Judd et al., 2013; Krakowski and Czobor, 2014; Mamdani et al., 2022). In addition, temperature effects on sleep disturbance, which could lead to decreased duration of sleep and is thus in turn related to deaths due to violence (Rod et al., 2011), may be more pronounced among the elderly compared with young adults (Okamoto-Mizuno and Mizuno, 2012; Okamoto et al., 1998). Because aging impairs thermoregulation (Meade et al., 2020), which is a critical determinant of both falling asleep and staying asleep (Kräuchi, 2007; Obradovich et al., 2022).
This study has several strengths. First, we focused on two understudied temperature-mortality outcomes — suicide and homicide — compared with more well-studied effects on all-cause, cardiovascular, and respiratory mortality. It is important to note that these outcomes impact, on average, younger people, as demonstrated by our distribution of age at death. Second, the case-crossover design controlled for time-invariant potential confounding factors such as socioeconomic status and history of mental illness, which may be difficult to control in other study designs. Third, we included six years of data on all deaths in California, and because outcomes were identified based on cause of death listed on death certificates using ICD-10 codes, we expect outcome misclassification to be low and likely to be non-differential with respect to our exposures. Fourth, we included both minimum and maximum daily temperatures—approximating nighttime minimums and daytime maximums, respectively—which may have different mechanisms and thus impacts. Indeed, slightly differing effect estimates were observed, with strongest effects from daily minimum temperature increase. One possible explanation of strongest effects of high nighttime temperature could be that it interferes with physiological processes that regulate the sleep–wake cycle and thermoregulation (Murage et al., 2017; Obradovich et al., 2022).
This study has some limitations. First, residential census tracts were used to assign exposure to both temperature and air pollution, which could lead to some exposure misclassification. Exposure assessment was not available for the exact geocoded residential address, which would have been preferred. Regardless, the census tract-based approach was used for all study subjects, so we expect any misclassification to be non-differential with respect to outcome, and would not have resulted in falsely positive associations. Second, given the focus on mortality, we were only able to examine homicide deaths (and characteristics of the decedent) and not the perpetrators of homicide, whose characteristics may be more relevant when considering effect heterogeneity. Future studies might try to expand on this area to better differentiate the possible differing effects of temperature in these subpopulations. We did not have on information time-varying acute disease conditions, so we were not able to adjust these potential confounders.
In conclusion, increase in ambient temperature was linearly associated with higher odds of death due to suicide and homicide. There is limited previous quantitative evidence of acute effects of temperature on violent deaths. This study adds to the growing literature from a climate change vulnerable region, which has experienced, and will continue to experience, progressively increasing temperatures—both gradual long-term and acute short-term shifts, the latter being most relevant to this study—over several decades under climate change (Williams et al., 2019). Our findings suggest that violent deaths might increase with the progression of the climate crisis. While further study is needed on this important topic, our study provide evidence in support of the development of targeted prevention policies and guidelines to prevent heat-related mental health mortality.
Supplementary Material
HIGHLIGHTS.
Increased ambient temperature was associated with increased odds of suicide deaths
Increased ambient temperature was associated with increased odds of homicide deaths
The temperature-mortality associations were larger among older individuals
No associations with suicide or homicide deaths were observed for air pollutants
ACKNOWLEDGEMENT
FUNDING
This work was supported by the National Institute of Environmental Health Sciences grant P30ES007048, Office of Research and Southern California Environmental Health Sciences Climate Change and Health Pilot Project Program, University of Southern California Office of Research Strategic Development of Research Award, and National Science Foundation (NSF) grant CBET-1752522.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
ETHICAL APPROVAL
This study was approved by the Committee for the Protection of Human Subjects of the state of California.
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
CONFLIT OF INTERESTS
The authors declare they have no actual or potential competing interests. Frederick Lurmann is employed by Sonoma Technology, Inc., Petaluma, CA
REFERENCES
- Abatzoglou JT, 2013. Development of gridded surface meteorological data for ecological applications and modelling. Int. J. Climatol 33, 121–131. https://doi.org/ 10.1002/joc.3413 [DOI] [Google Scholar]
- Alexopoulos GS, 2005. Depression in the elderly. Lancet 365, 1961–1970. 10.1016/S0140-6736(05)66665-2 [DOI] [PubMed] [Google Scholar]
- Ban J, Xu D, He MZ, Sun Q, Chen C, Wang W, Zhu P, Li T, 2017. The effect of high temperature on cause-specific mortality: A multi-county analysis in China. Environ. Int 106, 19–26. 10.1016/j.envint.2017.05.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bénézech M, Bourgeois M, 1992. [Homicide is strongly correlated to depression and not to mania]. Encephale. 18 Spec No, 89–90. [PubMed] [Google Scholar]
- Berman JD, Burkhardt J, Bayham J, Carter E, Wilson A, 2019. Acute Air Pollution Exposure and the Risk of Violent Behavior in the United States. Epidemiology 30, 799–806. 10.1097/EDE.0000000000001085 [DOI] [PubMed] [Google Scholar]
- Bondy M, Roth S, Sager L, 2018. Crime is in the Air : The Contemporaneous Relationship between Air Pollution and Crime. [Google Scholar]
- Burke M, González F, Baylis P, Heft-Neal S, Baysan C, Basu S, Hsiang S, 2018. Higher temperatures increase suicide rates in the United States and Mexico. Nat. Clim. Chang 8, 723–729. 10.1038/s41558-018-0222-x [DOI] [Google Scholar]
- Burkhardt J, Bayham J, Wilson A, Berman JD, O’Dell K, Ford B, Fischer EV, Pierce JR, 2020. The relationship between monthly air pollution and violent crime across the United States. J. Environ. Econ. Policy 9, 188–205. 10.1080/21606544.2019.1630014 [DOI] [Google Scholar]
- Carballo JJ, Currier D, Figueroa AE, Giner L, Kelly SA, Sublette ME, Oquendo MA, 2009. Neurobiological underpinnings of suicidal behavior : Integrating data from clinical and biological studies. Eur. J. Psychiatry 23, 243–259. [Google Scholar]
- CDC, 2019. Death Rates Due to Suicide and Homicide Among Persons Aged 10–24: United States, 2000–2017 [WWW Document]. URL https://www.cdc.gov/nchs/products/databriefs/db352.htm#ref4 [PubMed]
- Chen R, Yin P, Wang L, Liu C, Niu Y, Wang W, Jiang Y, Liu Y, Liu J, Qi J, You J, Kan H, Zhou M, 2018. Association between ambient temperature and mortality risk and burden: time series study in 272 main Chinese cities. BMJ 363, k4306. 10.1136/bmj.k4306 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheng S, Plouffe R, Nanos SM, Qamar M, Fisman DN, Soucy J-PR, 2021. The effect of average temperature on suicide rates in five urban California counties, 1999– 2019: an ecological time series analysis. BMC Public Health 21, 974. 10.1186/s12889-021-11001-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conwell Y, Duberstein PR, Hirsch JK, Conner KR, Eberly S, Caine ED, 2010. Health status and suicide in the second half of life. Int. J. Geriatr. Psychiatry 25, 371–379. https://doi.org/ 10.1002/gps.2348 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costa LG, Cole TB, Coburn J, Chang Y-C, Dao K, Roque P, 2014. Neurotoxicants are in the air: convergence of human, animal, and in vitro studies on the effects of air pollution on the brain. Biomed Res. Int 2014, 736385. 10.1155/2014/736385 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davoudi M, Barjasteh-Askari F, Amini H, Lester D, Mahvi AH, Ghavami V, Rezvani Ghalhari M, 2021. Association of suicide with short-term exposure to air pollution at different lag times: A systematic review and meta-analysis. Sci. Total Environ 771, 144882. https://doi.org/ 10.1016/j.scitotenv.2020.144882 [DOI] [PubMed] [Google Scholar]
- dos Santos Oliveira SJG, dos Reis CL, Cipolotti R, Gurgel RQ, Santos VS, Martins-Filho PRS, 2017. Anxiety, depression, and quality of life in mothers of newborns with microcephaly and presumed congenital Zika virus infection: a follow-up study during the first year after birth. Arch. Womens. Ment. Health 20, 473–475. 10.1007/s00737-017-0724-y [DOI] [PubMed] [Google Scholar]
- Eckel SP, Cockburn M, Shu Y-H, Deng H, Lurmann FW, Liu L, Gilliland FD, 2016. Air pollution affects lung cancer survival. Thorax 71, 891–898. 10.1136/thoraxjnl-2015-207927 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gao J, Cheng Q, Duan J, Xu Z, Bai L, Zhang Y, Zhang H, Wang S, Zhang Z, Su H, 2019. Ambient temperature, sunlight duration, and suicide: A systematic review and meta-analysis. Sci. Total Environ 646, 1021–1029. 10.1016/j.scitotenv.2018.07.098 [DOI] [PubMed] [Google Scholar]
- Gasparrini A, 2011. Distributed Lag Linear and Non-Linear Models in R: The Package dlnm. J. Stat. Softw 43, 1–20. [PMC free article] [PubMed] [Google Scholar]
- Gasparrini A, Armstrong B, Kenward MG, 2010. Distributed lag non-linear models. Stat. Med 29, 2224–2234. 10.1002/sim.3940 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gasparrini A, Armstrong B, Kovats S, Wilkinson P, 2012. The effect of high temperatures on cause-specific mortality in England and Wales. Occup. Environ. Med 69, 56 LP – 61. 10.1136/oem.2010.059782 [DOI] [PubMed] [Google Scholar]
- Gates A, Klein M, Acquaotta F, Garland RM, Scovronick N, 2019. Short-term association between ambient temperature and homicide in South Africa: a case-crossover study. Environ. Heal 18, 109. 10.1186/s12940-019-0549-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gładka A, Rymaszewska J, Zatoński T, 2018. Impact of air pollution on depression and suicide. Int. J. Occup. Med. Environ. Health 31, 711–721. 10.13075/ijomeh.1896.01277 [DOI] [PubMed] [Google Scholar]
- Gronlund CJ, Zanobetti A, Wellenius GA, Schwartz JD, O’Neill MS, 2016. Vulnerability to Renal, Heat and Respiratory Hospitalizations During Extreme Heat Among U.S. Elderly. Clim. Change 136, 631–645. 10.1007/s10584-016-1638-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Helama S, Holopainen J, Partonen T, 2013. Temperature-associated suicide mortality: contrasting roles of climatic warming and the suicide prevention program in Finland. Environ. Health Prev. Med 18, 349–355. 10.1007/s12199-013-0329-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heron M, 2019. Deaths: Leading causes for 2017. Natl. Vital Stat. Reports 68. [PubMed] [Google Scholar]
- Hopp S, Dominici F, Bobb JF, 2018. Medical diagnoses of heat wave-related hospital admissions in older adults. Prev. Med. (Baltim) 110, 81–85. 10.1016/j.ypmed.2018.02.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hynan DJ, Grush JE, 1986. Effects of impuisivity, depression, provocation, and time on aggressive behavior. J. Res. Pers 20, 158–171. https://doi.org/ 10.1016/0092-6566(86)90115-7 [DOI] [Google Scholar]
- Judd LL, Schettler PJ, Coryell W, Akiskal HS, Fiedorowicz JG, 2013. Overt irritability/anger in unipolar major depressive episodes: past and current characteristics and implications for long-term course. JAMA psychiatry 70, 1171–1180. 10.1001/jamapsychiatry.2013.1957 [DOI] [PubMed] [Google Scholar]
- Kamphuis J, Meerlo P, Koolhaas JM, Lancel M, 2012. Poor sleep as a potential causal factor in aggression and violence. Sleep Med. 13, 327–334. 10.1016/j.sleep.2011.12.006 [DOI] [PubMed] [Google Scholar]
- Kim C, Jung SH, Kang DR, Kim HC, Moon KT, Hur NW, Shin DC, Suh I, 2010. Ambient Particulate Matter as a Risk Factor for Suicide. Am. J. Psychiatry 167, 1100–1107. 10.1176/appi.ajp.2010.09050706 [DOI] [PubMed] [Google Scholar]
- Kim Y, Kim H, Kim DS, 2011. Association between daily environmental temperature and suicide mortality in Korea (2001-2005). Psychiatry Res. 186, 390–396. 10.1016/j.psychres.2010.08.006 [DOI] [PubMed] [Google Scholar]
- Kingsley SL, Eliot MN, Gold J, Vanderslice RR, Wellenius GA, 2016. Current and Projected Heat-Related Morbidity and Mortality in Rhode Island. Environ. Health Perspect 124, 460–467. 10.1289/ehp.1408826 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krakowski MI, Czobor P, 2014. Depression and impulsivity as pathways to violence: implications for antiaggressive treatment. Schizophr. Bull 40, 886–894. 10.1093/schbul/sbt117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kräuchi K, 2007. The thermophysiological cascade leading to sleep initiation in relation to phase of entrainment. Sleep Med. Rev 11, 439–451. 10.1016/j.smrv.2007.07.001 [DOI] [PubMed] [Google Scholar]
- Lawrence T, Zubatsky M, Meyer D, 2020. The association between mental health diagnoses and influenza vaccine receipt among older primary care patients. Psychol. Health Med 25, 1083–1093. 10.1080/13548506.2020.1717557 [DOI] [PubMed] [Google Scholar]
- Lehmann F, Alary P-E, Rey G, Slama R, 2022. Association of Daily Temperature With Suicide Mortality: A Comparison With Other Causes of Death and Characterization of Possible Attenuation Across 5 Decades. Am. J. Epidemiol. 10.1093/aje/kwac150 [DOI] [PubMed] [Google Scholar]
- Lin G-Z, Li L, Song Y-F, Zhou Y-X, Shen S-Q, Ou C-Q, 2016. The impact of ambient air pollution on suicide mortality: a case-crossover study in Guangzhou, China. Environ. Health 15, 90. 10.1186/s12940-016-0177-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu J, Varghese BM, Hansen A, Xiang J, Zhang Y, Dear K, Gourley M, Driscoll T, Morgan G, Capon A, Bi P, 2021. Is there an association between hot weather and poor mental health outcomes? A systematic review and meta-analysis. Environ. Int 153, 106533. https://doi.org/ 10.1016/j.envint.2021.106533 [DOI] [PubMed] [Google Scholar]
- Maes M, Scharpé S, Verkerk R, D’Hondt P, Peeters D, Cosyns P, Thompson P, De Meyer F, Wauters A, Neels H, 1995. Seasonal variation in plasma L-tryptophan availability in healthy volunteers. Relationships to violent suicide occurrence. Arch. Gen. Psychiatry 52, 937–946. 10.1001/archpsyc.1995.03950230051008 [DOI] [PubMed] [Google Scholar]
- Mamdani F, Weber MD, Bunney B, Burke K, Cartagena P, Walsh D, Lee FS, Barchas J, Schatzberg AF, Myers RM, Watson SJ, Akil H, Vawter MP, Bunney WE, Sequeira A, 2022. Identification of potential blood biomarkers associated with suicide in major depressive disorder. Transl. Psychiatry 12, 159. 10.1038/s41398-022-01918-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mares D, 2013. Climate change and crime: monthly temperature and precipitation anomalies and crime rates in St. Louis, MO 1990–2009. Crime, Law Soc. Chang 59, 185–208. 10.1007/s10611-013-9411-8 [DOI] [Google Scholar]
- Massazza A, Teyton A, Charlson F, Benmarhnia T, Augustinavicius JL, 2022. Quantitative methods for climate change and mental health research: current trends and future directions. Lancet Planet. Heal 6, e613–e627. https://doi.org/ 10.1016/S2542-5196(22)00120-6 [DOI] [PubMed] [Google Scholar]
- McClure CD, Jaffe DA, 2018. US particulate matter air quality improves except in wildfire-prone areas. Proc. Natl. Acad. Sci 115, 7901–7906. 10.1073/pnas.1804353115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meade RD, Akerman AP, Notley SR, McGinn R, Poirier P, Gosselin P, Kenny GP, 2020. Physiological factors characterizing heat-vulnerable older adults: A narrative review. Environ. Int 144, 105909. 10.1016/j.envint.2020.105909 [DOI] [PubMed] [Google Scholar]
- Miranda-Mendizabal A, Castellví P, Parés-Badell O, Alayo I, Almenara J, Alonso I, Blasco MJ, Cebrià A, Gabilondo A, Gili M, Lagares C, Piqueras JA, Rodríguez-Jiménez T, Rodríguez-Marín J, Roca M, Soto-Sanz V, Vilagut G, Alonso J, 2019. Gender differences in suicidal behavior in adolescents and young adults: systematic review and meta-analysis of longitudinal studies. Int. J. Public Health 64, 265–283. 10.1007/s00038-018-1196-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murage P, Hajat S, Kovats RS, 2017. Effect of night-time temperatures on cause and age-specific mortality in London. Environ. Epidemiol. (Philadelphia, Pa.) 1, e005–e005. 10.1097/EE9.0000000000000005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nguyen A-M, Malig BJ, Basu R, 2021. The association between ozone and fine particles and mental health-related emergency department visits in California, 2005–2013. PLoS One 16, e0249675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Obradovich N, Migliorini R, Mednick SC, Fowler JH, 2022. Nighttime temperature and human sleep loss in a changing climate. Sci. Adv 3, e1601555. 10.1126/sciadv.1601555 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okamoto-Mizuno K, Mizuno K, 2012. Effects of thermal environment on sleep and circadian rhythm. J. Physiol. Anthropol 31, 14. 10.1186/1880-6805-31-14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okamoto K, Nagai Y, Iizuka S, 1998. Age Effects on Physiological Responses and Bed Climate during Sleep after Heating the Lower Extremities. J. Home Econ. Japan 49, 1307–1312. [Google Scholar]
- Palinkas LA, Wong M, 2020. Global climate change and mental health. Curr. Opin. Psychol 32, 12–16. 10.1016/j.copsyc.2019.06.023 [DOI] [PubMed] [Google Scholar]
- Qiu X, Wei Y, Weisskopf M, Spiro A, Shi L, Castro E, Coull B, Koutrakis P, Schwartz J, 2022. Air pollution, climate conditions and risk of hospital admissions for psychotic disorders in U.S. residents. Environ. Res. 114636. https://doi.org/ 10.1016/j.envres.2022.114636 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rahman MM, Garcia E, Lim CC, Ghazipura M, Alam N, Palinkas LA, McConnell R, Thurston G, 2022. Temperature variability associations with cardiovascular and respiratory emergency department visits in Dhaka, Bangladesh. Environ. Int 164, 107267. https://doi.org/ 10.1016/j.envint.2022.107267 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reid CE, Snowden JM, Kontgis C, Tager IB, 2012. The role of ambient ozone in epidemiologic studies of heat-related mortality. Environ. Health Perspect 120, 1627–1630. 10.1289/ehp.1205251 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rifkin DI, Long MW, Perry MJ, 2018. Climate change and sleep: A systematic review of the literature and conceptual framework. Sleep Med. Rev 42, 3–9. 10.1016/j.smrv.2018.07.007 [DOI] [PubMed] [Google Scholar]
- Rod NH, Vahtera J, Westerlund H, Kivimaki M, Zins M, Goldberg M, Lange T, 2011. Sleep disturbances and cause-specific mortality: Results from the GAZEL cohort study. Am. J. Epidemiol 173, 300–309. 10.1093/aje/kwq371 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rotton J, Cohn EG, 2003. Global Warming and U.S. Crime Rates: An Application of Routine Activity Theory. Environ. Behav 35, 802–825. 10.1177/0013916503255565 [DOI] [Google Scholar]
- Son J-Y, Lee J-T, Anderson GB, Bell ML, 2011. Vulnerability to temperature-related mortality in Seoul, Korea. Environ. Res. Lett 6. 10.1088/1748-9326/6/3/034027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sun S, Weinberger KR, Nori-Sarma A, Spangler KR, Sun Y, Dominici F, Wellenius GA, 2021. Ambient heat and risks of emergency department visits among adults in the United States: time stratified case crossover study. BMJ 375, e065653. 10.1136/bmj-2021-065653 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Takahashi R, 2017. Climate, Crime, and Suicide: Empirical Evidence from Japan. Clim. Chang. Econ 08, 1750003. 10.1142/S2010007817500038 [DOI] [Google Scholar]
- Thompson R, Hornigold R, Page L, Waite T, 2018. Associations between high ambient temperatures and heat waves with mental health outcomes: a systematic review. Public Health 161, 171–191. https://doi.org/ 10.1016/j.puhe.2018.06.008 [DOI] [PubMed] [Google Scholar]
- Tian Y, Liu H, Id YS, Id YC, Song J, Li M, Wu Y, Wang X, Xiang X, Juan J, Chen L, Wei C, Id PG, Id YH, 2019. Association between temperature variability and daily hospital admissions for cause- specific cardiovascular disease in urban China : A national time-series study. PLOS Med. 16, 1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tiihonen J, Halonen P, Tiihonen L, Kautiainen H, Storvik M, Callaway J, 2017. The Association of Ambient Temperature and Violent Crime. Sci. Rep 7, 6543. 10.1038/s41598-017-06720-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- To P, Eboreime E, Agyapong VIO, 2021. The Impact of Wildfires on Mental Health: A Scoping Review. Behav. Sci. (Basel, Switzerland) 11. 10.3390/bs11090126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang Yan, Bobb JF, Papi B, Wang Yun, Kosheleva A, Di Q, Schwartz JD, Dominici F, 2016. Heat stroke admissions during heat waves in 1,916 US counties for the period from 1999 to 2010 and their effect modifiers. Environ. Health 15, 83. 10.1186/s12940-016-0167-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams AP, Abatzoglou JT, Gershunov A, Guzman-Morales J, Bishop DA, Balch JK, Lettenmaier DP, 2019. Observed Impacts of Anthropogenic Climate Change on Wildfire in California. Earth’s Futur. 7, 892–910. 10.1029/2019EF001210 [DOI] [Google Scholar]
- Wong DW, Yuan L, Perlin SA, 2004. Comparison of spatial interpolation methods for the estimation of air quality data. J. Expo. Sci. Environ. Epidemiol 14, 404–415. 10.1038/sj.jea.7500338 [DOI] [PubMed] [Google Scholar]
- Xie Y, Lin M, Decharme B, Delire C, Horowitz LW, Lawrence DM, Li F, Séférian R, 2022. Tripling of western US particulate pollution from wildfires in a warming climate. Proc. Natl. Acad. Sci 119, e2111372119. 10.1073/pnas.2111372119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xu R, Xiong X, Abramson MJ, Li S, Guo Y, 2020. Ambient temperature and intentional homicide: A multi-city case-crossover study in the US. Environ. Int 143, 105992. 10.1016/j.envint.2020.105992 [DOI] [PubMed] [Google Scholar]
- Yang J, Jit M, Zheng Y, Feng L, Liu X, Wu JT, Yu H, 2017. The impact of influenza on the health related quality of life in China: An EQ-5D survey. BMC Infect. Dis 17, 1–12. 10.1186/s12879-017-2801-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhao Q, Zhang Y, Zhang W, Li S, Chen G, Wu Y, Qiu C, Ying K, Tang H, Huang J-A, Williams G, Huxley R, Guo Y, 2017. Ambient temperature and emergency department visits: Time-series analysis in 12 Chinese cities. Environ. Pollut 224, 310–316. 10.1016/j.envpol.2017.02.010 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.