

Abstract
The transition to electric vehicles is projected to have considerable public health co-benefits, but most evidence regarding air quality and health impacts comes from projections rather than real-world data. We evaluated whether population-level respiratory health and air quality co-benefits were already detectable at the relatively low levels of zero-emissions vehicles (ZEV): battery electric, plug-in hybrid, hydrogen fuel cell vehicle) adoption in California, and evaluated the ZEV adoption gap in underserved communities. We conducted a zip code-level ecologic study relating changes in annual number of ZEVs (nZEV) per 1000 population from 2013–2019 to: (i) annual average monitored nitrogen dioxide (NO2) concentrations and (ii) annual age-adjusted asthma-related emergency department (ED) visit rates, while considering educational attainment. The average nZEV increased from 1.4 per 1,000 population in 2013 (standard deviation [SD]: 2.1) to 14.7 per 1,000 in 2019 (SD: 14.7). ZEV adoption was considerably slower in zip codes with lower educational attainment (p<0.0001). A within-zip code increase of 20 ZEVs per 1,000 was associated with a −0.41 ppb change in annual average NO2 (95% confidence interval [CI]:−1.12, 0.29) in an adjusted model. A within-zip code increase of 20 ZEVs per 1,000 population was associated with a 3.2% decrease in annual age-adjusted rate of asthma-related ED visits (95% CI:−5.4, −0.9). Findings were supported by a variety of sensitivity analyses. Observational data on the early phase ZEV transition in California provided a natural experiment, enabling us to document the first real-world associations between increasing nZEV and changes in air quality and health. Results suggest co-benefits of the early-phase transition to ZEV but with an adoption gap among less affluent populations which threatens the equitable distribution of possible co-benefits.
Keywords: asthma, air pollution, climate change, respiratory health, traffic-related pollution
Graphical Abstract
1. INTRODUCTION
The transition to electric vehicles (EV) is not only an important climate change mitigation strategy but is also projected to have considerable co-benefits for public health.1,2 On-road vehicles are major contributors to harmful ambient air pollution through tailpipe-related emissions, including carbon monoxide, particulate matter <2.5μm (PM2.5), and oxides of nitrogen (NOX) including nitrogen dioxide (NO2). Exposure to traffic-related air pollution (TRAP) is associated with a range of adverse health outcomes, including respiratory symptoms, development of asthma, asthma exacerbations, reduced lung function, cardiovascular disease, and premature death.3–8
Projected impacts of the EV transition on air quality and health (“co-benefits”) have been calculated for hypothetical scenarios for several locations around the world, with results depending on local features such as the electrical power generation mix used for EV charging. Air quality co-benefit projections anticipate reductions in NOX, PM2.5, carbon monoxide, volatile organic compounds, and ground-level ozone (O3)—although some predict some occasional increases in O3 due to lower NOX emissions.2,9–17 Health co-benefits of EV adoption have been estimated for Turin, Italy,14 Paris, France,18 Rotterdam, Netherlands,19 Toronto/Hamilton area, Canada,17 Houston, Texas,9 Seattle, Washington,20 and for the entire US1,2 with projections anticipating reductions in premature mortality, asthma exacerbations, and respiratory and cardiovascular hospitalizations. Indeed, in the United States (U.S.), a complete shift to EVs is projected to produce more than $1.2 trillion in cumulative health benefits by 2050, including: over 2.7 million avoided pediatric asthma exacerbations; 57,200 fewer asthma-related emergency department (ED) visits; and 110,000 lives saved.2
The transition to EVs has already begun, but there is little real-world data on observed co-benefits of the early transition. There is also serious concern that EV adoption is not equitably distributed across the population. Underserved communities potentially have most to gain from the transition because they are overburdened with TRAP21–23 and TRAP-related diseases;5,7,24 however, these communities tend to lag in the EV transition due to multiple barriers, such as access to charging infrastructure, concerns about charge time, range, and real/perceived expense related to purchase, maintenance, and charging, as well as limited knowledge of financial incentives.25,26
Asthma is a leading chronic health conditions with documented increased exacerbations (leading to emergency department [ED] visits) in response to tailpipe emission pollutants,5,27–30 thus a compelling outcome to examine as early markers of respiratory health response to increased EV adoption. The annual cost of asthma in the US is approximately $56 billion, including $50 billion in direct healthcare costs.31 Persons of lower socioeconomic status and from historically marginalized communities and the uninsured comprise a disproportionate amount of asthma-related ED visits,32–35 highlighting a health equity issue.
We conducted an ecologic study across California to evaluate the associations between adoption of zero-emissions vehicles (ZEV: battery electric, plug-in hybrid, hydrogen fuel cell vehicle) and air quality and asthma outcomes. Specifically, in this study we relate within-zip code number of ZEVs to: (a) annual averages of monitored NO2 concentrations and (b) asthma-related ED visits, from 2013 through 2019 (prior to the COVID-19 pandemic), while considering zip code-level educational attainment which serves as a proxy for socioeconomic status. We aimed to evaluate whether population-level air quality and respiratory health and co-benefits were already detectable at the still relatively low levels of ZEV adoption and evaluate the ZEV adoption gap in underserved communities. California is a socio-economically diverse state heavily impacted by TRAP and is a pioneer in the early adoption of ZEVs36 making it an ideal setting for this analysis. Observational data on the early phase ZEV transition in California provided a natural experiment, enabling us to quantify some of the first evidence of real-world co-benefits of the transition to a zero-tailpipe-emissions transportation sector.
2. METHODS
2.1. Data
2.1.1. Number of zero-emissions vehicles
Annual counts of light-duty vehicles registered in California, by fuel type, have been publicly released by the California Energy Commission through a partnership with the California Department of Motor Vehicles.37 We tabulated the total number of ZEV vehicles (battery electric, plug-in hybrid, hydrogen fuel cell) for each zip code and year starting in 2013, to coincide with the availability of asthma ED visit data (described below in section 2.1.3.). Years with no records of ZEV vehicles occurred most frequently in the earliest years of the study period and were assigned counts of 0. The number of ZEV (nZEV) per 1,000 population was calculated using the American Community Survey (ACS) estimates of population size (described below in section 2.1.4.).
2.1.2. Ambient NO2 air pollution
We selected NO2 as the air pollutant of interest due to on-road vehicles being its largest source of emissions38 and the greater availability of monitoring sites measuring NO2 compared with other traffic-related air pollutants (e.g., PM2.5). We obtained annual average NO2 measurements from the U.S. Environmental Protection Agency’s (EPA) AirData website as pre-generated data files, dated 2022-11-14, from all available air monitoring stations operating in California39 from 2013–2019 to coincide with the availability of asthma ED visit data (described below in section 2.1.3.). Secondary analyses considered additional data from 2020–2021. State and local monitoring plans guide placement of air monitoring stations, which might include areas with larger populations or thought to have higher pollution concentrations.40 We used annual data calculated according to the NO2 Annual 1971 pollutant standard, with all monitoring sites reporting 1 hour sample duration.41 We processed these data to ensure only one NO2 annual average estimate per site per year. In the few cases where multiple records existed for a given site-year (22 out of 843 [2.6%] site-years), we selected a single record using the following criteria. First, if there were records from multiple instruments, we selected the instrument with the longest duration of records at that site during the study period. Second, if there were records from two versions of the annual average including or excluding exceptional events as defined by the EPA (i.e., events that affect air quality but which the local agency has no control over, such as wildfires),41 we selected the record excluding exceptional events since exceptional events are unlikely to be related to local number of ZEV. Finally, if multiple records remained, we selected the record with the largest number of days contributing to the annual average. In primary analyses, we used annual average NO2 records based on at least 50% complete data and in secondary analyses we used records with ≥75% complete (i.e., satisfying the regulatory completeness criteria by the monitor for the year).41
2.1.3. Asthma emergency department visits
Data on zip code-level annual age-adjusted rate (per 10,000) of asthma-related emergency department (ED) visits from 2013–2019 were obtained from the California Health and Human Services (CHHS) Open Data Portal. These data are produced by the California Department of Public Health, California Breathing Asthma Program, based on a database of ED visits from all licensed hospitals in California maintained by the California Department of Health Care Access and Information.42 These data reflect the number of ED visits related to asthma during each calendar year for a given zip code, including ED visits that results in hospitalization, normalized for zip code population.42 Age-adjusted rates of asthma ED visits were calculated by the California Breathing Asthma Program using yearly population estimates from the California Department of Finance which are then age-adjusted to the 2000 U.S. standard population from the U.S. Census Bureau using weights for the 24 age groups from Centers for Disease Control and Prevention43 (L. Avendaño, California Breathing, personal communication, December 19–20, 2022). The use of age-adjusted rates controls for possible confounding by differences in population age distribution across zip codes. Asthma-related ED visits were identified based on the International Classification of Diseases (ICD) primary discharge codes: ICD-9 493.xx or ICD-10 J45.42 Rates are approximate since they are based on total number of visits rather than the number of unique individuals and CHHS suppressed rates calculated from small counts (e.g., <12) due to statistical instability and/or de-identification purposes.
2.1.4. Population characteristics
Zip code-level population size and educational attainment, defined as percent of the population over age 25 years with at least a bachelor’s degree, were obtained from the 2015–2019 American Community Survey (ACS) 5-Year Estimates.44 Educational attainment serves as a proxy for socioeconomic status, representing the structural and financial barriers driving disparities rather than the lack of education itself. In secondary analyses we considered alternative measures of socioeconomic status, including: percentage of the population over age 25 with at least a high school degree, median household income, and percentage poverty defined as the percentage of the population whose income in past 12 months was below the poverty level.
2.1.5. Final analysis datasets
There were 629 records of annual average NO2 from 107 air monitoring stations in 95 zip codes available from 2013–2019, after excluding one site located in a zip code with no asthma ED visit data (Miramar, ≤1 ZEV during study period) and dropping 30 site-year records where the annual averages had used <50% complete data. There were 8,170 observations of non-missing annual age-adjusted rates of asthma ED visits in 1,240 zip codes from 2013–2019. In our analyses, we considered only zip codes with non-missing population size greater than 0, which reduced the final asthma ED visit dataset to 8,163 observations in 1,238 zip codes. ZEV data were available for all years/zip codes in the NO2 and asthma ED visit datasets. All datasets used in this study were not collected for the purpose of our study and none of our study team had access to any subject identifiers (only publicly available de-identified, aggregated data were used). According to the Office for Human Research Protection of U.S. Department of Health and Human Services, these analyses do not constitute human subjects research requiring Institutional Review Board approval or consent.
2.2. Statistical Methods
2.2.1. Descriptive statistics
Data distributions were summarized using means and standard deviations (SD). Differences in characteristics between zip codes with and without NO2 monitor data were compared using t-tests. Longitudinal trends in the: nZEV per 1,000 population, annual average NO2, and age-adjusted rate of asthma-related ED visits were visualized using spaghetti plots color coded by zip-code level educational attainment (% bachelor’s degree). Differences in the baseline level (in 2013) and annual rate of change of each of these variables by educational attainment were assessed using linear mixed effects models with a linear function of year (centered on 2013) and educational attainment, along with their interaction, and a zip code (or monitoring site) level random intercept and slope on year.
2.2.2. Analyses relating nZEV and NO2
The crude association between nZEV and NO2 was evaluated using predicted 7-year change from 2013 to 2019 estimated from separate simple linear regression models. For example, to obtain predicted 7-year change in nZEV a separate simple linear regression model was fit relating nZEV per 1,000 to calendar year for each zip code to predict the 7-year change in nZEV per 1,000 for that zip code. To obtain predicted 7-year change in NO2, a separate simple linear regression model was fit relating annual average NO2 to calendar year for each monitoring site to predict the 7-year change in NO2 for that site. For the 102 sites in 91 zip codes with >1 year of NO2 data, we plotted the monitoring site predicted 7-year change in NO2 versus the zip code (for that site) predicted 7-year change in nZEV, and calculated Pearson’s correlation coefficient.
The adjusted association between annual average NO2 (Yijk) at monitoring site k in zip code i at year j and nZEVs per 1,000 population (Xij) in zip code i at year j was estimated using the linear mixed effects model:
where β1 quantifies the association of within-zip code changes in nZEV with within-monitoring site changes in annual average NO2, adjusting for educational attainment (Zi) and calendar year (tij, centered at 2013; linear and quadratic effects included) to account for secular trends. Random intercepts for zip code (U0i) and site within zip code (U0ik) account for correlation in the longitudinal, multilevel data and the zip code-level random slope on the linear effect of year (U1i) allowed for variation in secular trends by zip code. No random slope was specified for year squared due to convergence issues, likely due to the smaller number of zip codes in this analysis (N=95) and the complexity of random intercepts for monitoring sites nested in zip codes. All random effects were assumed to be normally distributed and zip-code level random effects (U0i, U1i) were allowed to be correlated.
2.2.3. Analyses relating nZEV and asthma ED visits
The adjusted association between log transformed annual age-adjusted rate of asthma ED visits (Yij) in zip code i at year j and nZEVs per 1,000 population (Xij) in zip code i at year j was estimated using the linear mixed model:
where β1 quantifies the association of within-zip code changes in nZEV with within-zip code changes in log annual age-adjusted rate of asthma-related ED visits, adjusting for educational attainment (Zi) and calendar year (tij, centered at 2013; linear and quadratic effects included) to account for secular trends. Zip code level random intercepts (U0i) and random slopes on both terms for year (U1i, U2i) allowed for variation across zip codes in baseline age-adjusted rate of asthma ED visits and in secular trends. All random effects were assumed to be normally distributed and zip-code level random effects (U0i, U1i, U2i) were allowed to be correlated. Age-adjusted rate of asthma ED visits was natural log transformed to better satisfy modeling assumptions. Secondary analyses included investigating a nonlinear association with nZEV, using a generalized additive mixed model (GAMM)45 analogous to the linear mixed model above but that replaces the term β1Xij with the smooth function, s(Xij), estimated using a thin plate regression spline basis with automated selection of effective degrees of freedom.
When developing the primary models presented above, a variety of models were evaluated to identify key model features, and to assess the sensitivity of the results to various model specification and data inclusion choices. Results of sensitivity analyses are presented. Models were estimated using lme() and gamm() in the nlme46,47 and mgcv45 packages of R version 4.2.1.48
3. RESULTS
3.1. Descriptive statistics
Distributions of selected zip code demographic and socioeconomic characteristics are presented in Table 1. Among the 1,238 zip codes in the asthma ED visit analysis, the mean population size was 31,296 (min: 702 and max: 111,165) and the total population size across all 1,238 zip codes was 38,743,804. Zip code level educational attainment ranged from 1.1% to 87.1% of adults over age 25 years with at least a bachelor’s degree, with a mean (SD) of 33.4% (20.1%). The zip code level nZEV per 1,000 population had a mean (SD) of 1.4 (2.0) in 2013 and 14.7 (14.7) in 2019 (Supplemental Table 1). Zip code level number of ZEV per 1,000 in 2019 was highly correlated with measures of socioeconomic status, with Pearson’s correlation of: 0.84 for % bachelor’s degree, 0.83 for median household income, 0.55 for % high school degree, and −0.51 for % poverty. Zip code level annual age-adjusted asthma ED visit rates had a mean (SD) of 49.5 (30.5) per 10,000 in 2013 and 43.0 (27.5) per 10,000 in 2019 (Supplemental Table 1).
Table 1.
Distribution of selected demographic and socioeconomic characteristics among zip codes included in the asthma ED visit rate and nitrogen dioxide (NO2) analysis. Mean (standard deviation) presented, unless otherwise indicated.
| Characteristic | Zip codes in asthma ED visit analysis | Zip codes in NO2 analysis | P-value a |
|---|---|---|---|
| N | 1,238 | 95 | |
| Population size | 31,295.5 (21,311.5) (min: 702; max: 111,165) |
44,704.5 (19,253.9) (min: 1771; max: 88,979) |
<0.001 |
| Educational attainment b | |||
| % Bachelor’s degree or higher | 33.4 (20.1) | 29.2 (17.8) | 0.019 |
| % High school degree or higher | 83.8 (13.1) | 80.7 (12.2) | 0.013 |
| Income | |||
| Median household income | $79,385 ($34,477) | $71,248 ($28,645) | 0.005 |
| % Poverty c | 13.7 (8.6) | 16.3 (8.6) | 0.003 |
P-value from t-tests comparing differences in characteristics between zip codes with and without NO2 monitor data.
Among adults over age 25 years.
Percentage of the population whose income in past 12 months was below the poverty level.
Annual NO2 data were available from 107 monitoring locations, which were located in a subset of 95 of the 1,238 zip codes. The 95 zip codes covered a total of 4,246,931 people, representing 11.0% of the population included in the asthma ED visit analysis. Compared to zip codes without NO2 monitors, the 95 zip codes with NO2 monitors had higher average population size (p<0.001), lower educational attainment (p=0.01–0.02), lower household income (p=0.005), higher level of poverty (p=0.003), fewer ZEV per 1,000 in 2019 (p<0.001), and higher age-adjusted rates of asthma ED visits in 2019 (p=0.006; Table 1 and Supplemental Table 1). Extensive longitudinal data were available over the 7-year study period, from 2013–2019, with 100% of zip codes having nZEV data for all 7 years, 80.4% of included monitoring sites having 5 or more years of NO2 data, and 93.0% of included zip codes having 5 or more years of asthma ED visit data.
3.2. Longitudinal trends in nZEV, annual average NO2, and asthma-related ED visits
There was considerable growth in nZEV from 2013–2019 in California (Figure 1a), and growth in nZEV was slower for zip codes with lower educational attainment (p<0.0001). For example, we estimated that a typical zip code at the 25th percentile of educational attainment (17.1% bachelor’s degree) had an annual increase in nZEV per 1,000 of 0.70 (95% Confidence Interval [CI]: 0.61, 0.78) while a typical zip code at the 75th percentile of educational attainment (47.2% bachelor’s degree) had an annual increase in nZEV per 1,000 of 3.55 (95% CI: 3.47, 3.63). Declines in annual average NO2 and in age-adjusted rates of asthma-related ED visits were more modest over the study period (Figure 1b–c). The 2013 level of annual average NO2 was negatively associated with educational attainment (p<0.001), but the annual rate of change was not (p=0.48). Similarly, the 2013 level of age-adjusted asthma-related ED visits was negatively associated with educational attainment (p<0.001), but the annual rate of change was not (p=0.30).
Figure 1.
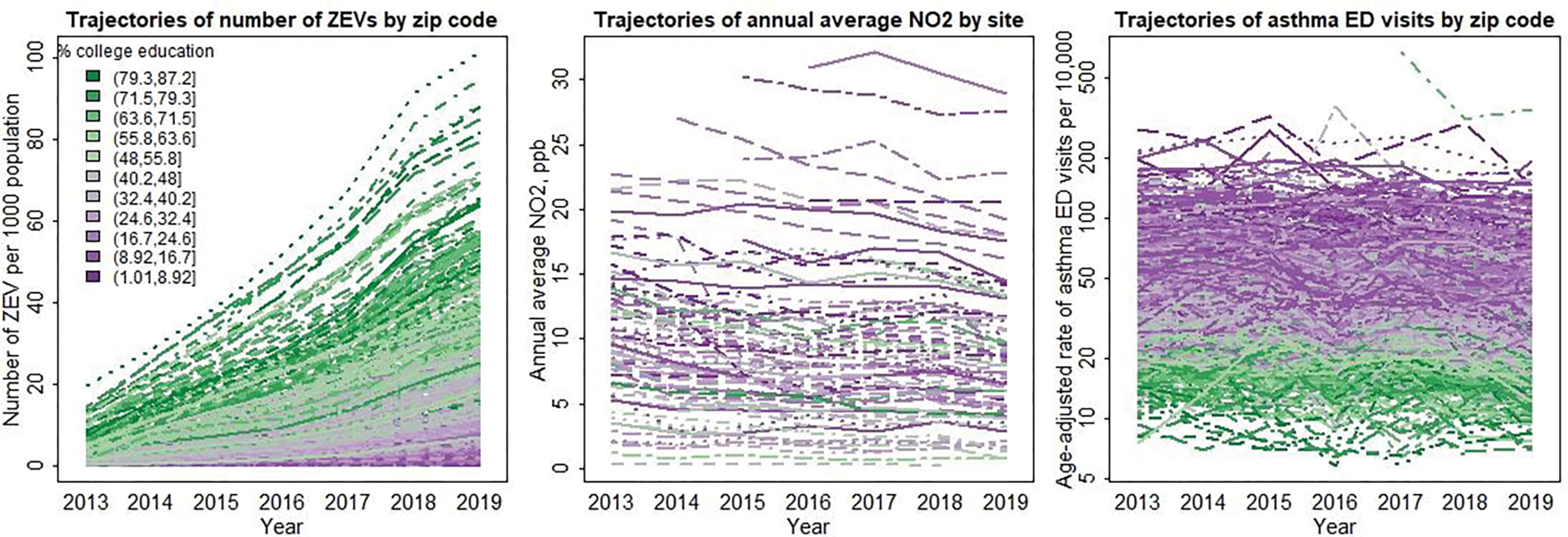
Longitudinal trends, from 2013–2019 in: (a) number of zero-emissions vehicles (ZEVs) per 1,000 population in 1,238 California zip codes, (b) annual average nitrogen dioxide (NO2) concentrations observed at 107 California monitoring stations, and (c) annual age-adjusted rate of asthma-related emergency department (ED) visits per 10,000 in 1,238 California zip codes. Color indicates educational attainment (% of adults age 25+ with at least a bachelor’s degree) at the zip code level, from lower (purple) to higher (green).
3.3. Associations of nZEV with monitored annual average NO2 concentrations
Higher nZEV was associated with lower annual NO2 concentrations measured at monitoring sites, though not statistically significant in the primary model. Results were consistent both in a crude analysis (Figure 2) and in a linear mixed model adjusting for confounders (Table 2) where we estimated that a within-zip code increase of 20 ZEVs per 1,000 population was associated with a −0.41 ppb change in annual average NO2 concentration (95% CI: −1.12, 0.29; p-value=0.25). The estimated association remained negative in a variety of sensitivity analyses (Supplemental Table 2) and had even greater magnitude of associations, some statistically significant, when: adjusting for alternative measures of socioeconomic status, adjusting for a fixed effect of monitoring site, or excluding the random slope on year. Inclusion of additional data from 2020–2021 or only 2021 (to avoid 2020, which was heavily impacted by the COVID-19 pandemic) resulted in greater magnitude negative associations that were statistically significant, even when restricting to the subset of observations that satisfied regulatory requirements for completeness (≥75%; Supplemental Table 2).
Figure 2.

Crude association between predicted 7-year change in nitrogen dioxide (NO2) versus 7-year change in number of zero-emissions vehicles (ZEVs) based on data from 102 air monitoring sites in 91 zip codes in California, with color indicating zip code level educational attainment (low: purple; high: green).
Table 2.
Adjusted model results for change in annual average nitrogen dioxide (NO2) concentration (ppb) and percent difference in age-adjusted asthma-related emergency department (ED) visits associated with a within-zip code increase of 20 zero-emissions vehicles (ZEVs) per 1,000 population.
| Model | Estimate | 95% CI | P-value |
|---|---|---|---|
| NO2 and ZEVs a | −0.41 | (−1.12, 0.29) | 0.252 |
| Asthma ED visit rate and ZEVs b | −3.2 | (−5.4, −0.9) | 0.006 |
NO2 model estimated using a linear mixed effects model adjusted for % bachelor’s degree, calendar year (linear and quadratic effect, centered at 2013), with random intercepts for zip code and site within zip cope, and a zip code-level random slope on the linear effect of year.
Asthma ED visit rate model estimated using a linear mixed effects model adjusted for % bachelor’s degree, calendar year (linear and quadratic effect, centered at 2013), with random intercepts for zip code, and a zip code-level random slope on the linear and quadratic effects of year.
3.4. Associations of nZEV with asthma-related emergency department visits
Higher nZEV was statistically significantly associated with fewer ED visits for asthma. Adjusting for zip code educational attainment and secular trends (Table 2), we estimated that a within-zip code increase of 20 ZEVs per 1,000 population was associated with a 3.2% decrease in annual age-adjusted rate of asthma-related ED visits (95% CI: −5.4, −0.9; p-value=0.006). The estimated association remained negative and statistically significant in a variety of sensitivity analyses (Supplemental Table 3). In a secondary analysis evaluating nonlinearity (Supplemental Figure 1), there was statistical evidence of the association being nonlinear (p-value = 0.002 for a test of nonlinear vs linear) with a negative association between nZEV and asthma ED visits which was stronger at higher levels of nZEV. However, much of the evidence for nonlinearity was driven by the 4 observations with nZEV greater than 82 (from zip codes 94022 and 95070 in Santa Clara County, in 2018 and 2019). Upon excluding these observations evidence for nonlinearity was more modest (p=0.03).
4. DISCUSSION
4.1. Air quality and health co-benefits of ZEV adoption
This study provides real-world evidence supporting air quality and respiratory health co-benefits from the ZEV transition, using observational data during a natural experiment of the early phase ZEV transition in California. We found statistically significant evidence that within-zip code increases in ZEV adoption were associated with decreases in rates of asthma ED visits. There was some evidence that this inverse association was nonlinear, with a suggested greater health co-benefit at higher levels of ZEV adoption—but caution must be taken not to overinterpret these nonlinear effect estimates at this early stage of the ZEV transition. As the number of ZEV increases in future years, researchers will increasingly be better positioned to evaluate evidence of nonlinear exposure-response functions. For air quality co-benefits, while the association of ZEV with annual average monitored NO2 concentrations was not statistically significant, it was in the hypothesized direction (inverse association) and relatively large in magnitude. We considered only air quality data from U.S. EPA monitoring sites, and these tended to be in zip codes that also had lower levels of ZEV adoption during the study period. We observed an adoption gap, wherein zip codes with a greater percentage of residents with lower educational attainment lagged in the ZEV transition. The strong evidence for health co-benefits and suggestive evidence for air quality co-benefits is remarkable given the still low rate of ZEV adoption in California in 2013–2019. Taken together, these results suggest that increasing ZEV adoption has the potential to improve both air quality and neighborhood-level asthma health outcomes, but the already evident adoption gap raises equity concerns.
While most studies have estimated environmental health impacts of EV adoption under hypothetical scenarios,9,14,17,18,20 our findings are consistent with the few studies that have investigated real world co-benefits of the transition to EVs or other alternative fuels.49,50 Lovasi et al. evaluated the air quality effects of the Clean Fuel Bus Program, which adopted lower-emissions buses including compressed natural gas, hybrid-electric, and ultra-low-sulfur diesel buses, in New York City, New York from 2009 to 2014.49 They reported that the shift toward clean bus service was associated with larger improvements in local NO and NO2 concentrations and areas with more bus service and higher proportional shifts towards clean buses had the largest declines in these pollutants.49 Adar et al. evaluated the air pollution and pulmonary health effects of adopting clean air technologies (e.g., diesel oxidation catalysts and crankcase ventilation systems used to reduce tailpipe and engine emissions) and fuels (e.g., ultra-low-sulfur diesel and a biodiesel mixture) on school buses in Seattle and Tahoma, Washington from 2005 to 2009.50 With these adoptions they found lower in-vehicle concentrations of fine and ultrafine particulate matter and lower pulmonary inflammation, improved lung growth, and reduced risk of school absenteeism among the schoolchildren bus riders.50 These studies provide important critical data on the environmental health impacts of vehicle technology/fuel transitions, and the present study furthers the literature by presenting the first results from a large, state-wide, population-based observational analysis of light duty vehicles.
4.2. ZEV adoption gap
Historically marginalized communities disproportionately experience higher exposure to air pollution, including TRAP,21–23 and adverse TRAP-related health outcomes such as asthma-related ED visits;33,35 thus ZEV adoption can be particularly beneficial in these communities. During this early phase of the ZEV transition, most adopters have been of higher education and income,26 aligning with the Diffusion of Innovation theory that early adopters of new technologies tend to be of higher socioeconomic status.51 This highlights a challenge for equitable transition to ZEVs and equitable distribution of related co-benefits for air quality and health. Indeed, we observed evidence for an adoption gap, with communities with lower educational attainment lagging in the ZEV transition—educational attainment here serving as a proxy for socioeconomic status and representing structural and financial barriers propelling disparities rather than the lack of education itself. While multiple potential barriers exist,25,26 increasing ZEV adoption in and around underserved and health-disparate communities could potentially help to improve local air quality and subsequently reduce adverse health impacts through a reduction in tailpipe emissions.52 Our results provide evidence to inform policy makers for the development of programs to ensure a just ZEV transition where underserved communities are able to fully realize health and air quality co-benefits.
4.3. Strengths and limitations
Our study has several strengths. First, is the use of publicly available data from the large and diverse state of California, which is at the forefront of the ZEV transition in the U.S., and contains one of the densest air quality monitoring networks in the U.S. This study setting is ideal to evaluate the environmental health co-benefits of the early ZEV transition. Second, using monitored NO2 concentration to study air quality benefits avoided potential issues with spatial-temporal ambient air pollutant models which might not yet fully account for the changing transportation fleet. Third, by studying within-zip codes trends over time, we were able to take advantage of the natural experiment afforded by the early phase ZEV transition. Finally, the study period ended in 2019, avoiding potential confounding related to the COVID-19 pandemic. Considerable growth in ZEVs has continued.
Our study also has limitations which should be taken into consideration when interpreting results. First is the use of number of ZEVs per zip code population as our measure for ZEV adoption, which does not consider ZEV miles driven or if internal combustion engine vehicles are taken off the road in response to ZEV adoption. Furthermore, the use of this metric only evaluates local, zip code level effects (based on the vehicle registration zip code); it does not consider impacts in other localities as vehicles are in operation, nor are we directly considering the air pollution from the power generation mix used to charge the vehicles or the total life cycle impacts of ZEVs which have been evaluated elsewhere.52 Second, we only evaluated the impact of light duty ZEV and did not include zero-emissions public transit or freight transport which are also key components of the ZEV transition, since these data were unavailable. Many public agencies and regulatory efforts are shifting towards low- and zero-emissions transport and continued release of temporally and spatially resolved data would allow for better evaluation of associated health co-benefits, potentially beneficial for cost-benefits analyses of such policy efforts. Third, due to the realities of relying on data from an air monitoring network—which is relatively extensive in California compared with other U.S. states—our analysis on the air pollution effects of the ZEV transition was in only 96 zip codes across the state. Although these locations do not represent the full spatial coverage across California, monitors are generally placed near population centers. Fourth, our ecologic analyses were conducted at the zip code level, which is a suboptimal geographic unit for population health studies because zip codes were designed for postal delivery. They represent varying geographic and population sizes, they can cross city/county/census boundaries, and they may change over time. This, however, was the finest spatial resolution available for the publicly available ZEV data. The challenges with zip code-level analyses are outweighed by the advantages of fine spatial resolution, especially in a state like California where a county-level analysis effectively combines a large percentage of the state’s population because some counties are so large (e.g., Los Angeles County contains ~25% of California’s population). Last, as in most observation studies, unmeasured confounding might have biased our estimated associations. We did adjust for area-level educational attainment—as a proxy for socioeconomic status—and our analyses included random intercepts for zip code which provides some control for possible unmeasured zip code-level confounding factors, and we additionally conducted various sensitivity analyses changing model specifications, adjusted covariates, and other data inclusions/exclusions; however, caution is warranted not to overinterpret results.
4.4. Future research
This study of the co-benefits of the early phase ZEV transition lays the foundation for future work. Research studying trends in the adoption of EV technology suggests that the U.S. entered the “takeoff” phase of EV adoption in 2017, marking the transition from an introductory phase to a phase of growth and mass adoption.53 With increasing numbers of ZEV, future studies can focus solely on the EV transition (excluding plug-in hybrids which are included in the present analysis) and/or with co-benefits analysis investigating a variety of health outcomes (including differences by vulnerable subgroups) and investigating a full set of ambient air pollutants (e.g., not only NO2 which has key tailpipe sources, but also PM2.5 which is impacted by brake and tire wear and might have a more complex association with EV adoptions given that EVs are on average heavier than their gasoline combustion counterparts54). Evaluation of possible nonlinear associations with co-benefits across a broader numerical range of ZEVs will be possible as their numbers increase. Additionally, the impact of electrification of other vehicle classes (e.g., such as heavy-duty on-road vehicles used in freight transport) or of transit systems (e.g., public transit, school buses) will enable new studies of observed associated public health co-benefits, including in high-traffic communities who are disproportionately exposure to TRAP.
5. CONCLUSIONS
This study leveraged a natural experiment and documents the first real-world associations between increasing nZEV and changes in air quality and health, suggesting co-benefits of the early-phase transition to ZEV in California, along with the adoption gap which threatens the equitable distribution of these co-benefits. These early results provide crucial evidence for informing future policies for a just and equitable transition to an electrified transportation sector, to both mitigate climate change and realize environmental and health co-benefits for all.
Supplementary Material
HIGHLIGHTS.
Real-world data use to quantify co-benefits of early electric vehicle transition
More zero-emissions vehicles non-significantly associated with lower pollution
Increases in zero-emissions vehicles linked with fewer asthma emergency room visits
Zero-emissions vehicles adoption gap threatens equitable co-benefits distribution
ACKNOWLEDGEMENTS
This work was supported by the University of Southern California Office of Research Strategic Directions for Research Award and the National Institute of Environmental Health Sciences [grants P30ES007048 and P2CES033433].
Abbreviations
- ACS
American Community Survey
- CHHS
California Health and Human Services
- ED
Emergency department
- EV
Electric vehicles
- ICD
International Classification of Diseases
- NO2
Nitrogen dioxide
- NOX
Oxides of nitrogen
- nZEV
Number of zero-emissions vehicles
- O3
Ozone
- PM2.5
Particulate matter <2.5μm
- SD
Standard deviations
- TRAP
Traffic-related air pollution
- ZEV
Zero-emissions vehicles
Footnotes
DECLARATION OF COMPETING INTEREST
Erika Garcia reports stock in Tesla Inc., Rivian Automotive Inc., and Ford Motor Co., all outside the submitted work, a conflict of interest (COI) managed by the USC Health Science Campus Conflict of Interest Review Committee including independent review of data collection and analyses. Sandrah Eckel reports funding from the National Institutes of Health and a spouse who works in emissions testing for a major automobile manufacturer, a COI managed by the USC Health Science Campus Conflict of Interest Review Committee including independent review of data collection and analyses. All other authors declare they have no actual or potential competing interests.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
DATA SHARING
The data that support the findings of this study are openly available in California Health and Human Services (CHHS) Open Data Portal at https://data.chhs.ca.gov/dataset/asthma-emergency-department-visit-rates; American Community Survey Data at https://www.census.gov/programs-surveys/acs/data.html; U.S. Environmental Protection Agency’s (EPA) AirData website at https://aqs.epa.gov/aqsweb/airdata/download_files.html; and California Energy Commission at http://www.energy.ca.gov/zevstats.
REFERENCES
- 1.Peters DR, Schnell JL, Kinney PL, Naik V, Horton DE. Public Health and Climate Benefits and Trade-Offs of U.S. Vehicle Electrification. GeoHealth 2020; 4: e2020GH000275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.American Lung Association. Zeroing in on Health Air; 2022.
- 3.U.S. Environmental Protection Agency. Health and Environmental Effects of Particulate Matter (PM). 2021. May 26, 2021 [cited 2022 April 10]. Available from: https://www.epa.gov/pm-pollution/health-and-environmental-effects-particulate-matter-pm. [Google Scholar]
- 4.U.S. Environmental Protection Agency. Basic Information about NO2. 2021. June 7, 2021 [cited 2022 April 10]. Available from: https://www.epa.gov/no2-pollution/basic-information-about-no2. [Google Scholar]
- 5.Guarnieri M, Balmes JR. Outdoor air pollution and asthma. Lancet 2014; 383: 1581–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Beelen R, Hoek G, van den Brandt Piet A, Goldbohm RA, Fischer P, Schouten Leo J, Jerrett M, Hughes E, Armstrong B, Brunekreef B. Long-Term Effects of Traffic-Related Air Pollution on Mortality in a Dutch Cohort (NLCS-AIR Study). Environmental Health Perspectives 2008; 116: 196–202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jerrett M, Finkelstein MM, Brook JR, Arain MA, Kanaroglou P, Stieb DM, Gilbert NL, Verma D, Finkelstein N, Chapman KR, Sears MR. A Cohort Study of Traffic-Related Air Pollution and Mortality in Toronto, Ontario, Canada. Environmental Health Perspectives 2009; 117: 772–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dastoorpoor M, Sekhavatpour Z, Masoumi K, Mohammadi MJ, Aghababaeian H, Khanjani N, Hashemzadeh B, Vahedian M. Air pollution and hospital admissions for cardiovascular diseases in Ahvaz, Iran. Sci Total Environ 2019; 652: 1318–30. [DOI] [PubMed] [Google Scholar]
- 9.Pan S, Roy A, Choi Y, Eslami E, Thomas S, Jiang X, Gao HO. Potential impacts of electric vehicles on air quality and health endpoints in the Greater Houston Area in 2040. Atmospheric Environment 2019; 207: 38–51. [Google Scholar]
- 10.Thompson T, Webber M, Allen DT. Air quality impacts of using overnight electricity generation to charge plug-in hybrid electric vehicles for daytime use. Environmental Research Letters 2009; 4: 014002. [Google Scholar]
- 11.Brinkman GL, Denholm P, Hannigan MP, Milford JB. Effects of Plug-In Hybrid Electric Vehicles on Ozone Concentrations in Colorado. Environmental Science & Technology 2010; 44: 6256–62. [DOI] [PubMed] [Google Scholar]
- 12.Li N, Chen J-P, Tsai IC, He Q, Chi S-Y, Lin Y-C, Fu T-M. Potential impacts of electric vehicles on air quality in Taiwan. Science of The Total Environment 2016; 566–567: 919–28. [DOI] [PubMed] [Google Scholar]
- 13.Nopmongcol U, Grant J, Knipping E, Alexander M, Schurhoff R, Young D, Jung J, Shah T, Yarwood G. Air Quality Impacts of Electrifying Vehicles and Equipment Across the United States. Environmental Science & Technology 2017; 51: 2830–7. [DOI] [PubMed] [Google Scholar]
- 14.Rizza V, Torre M, Tratzi P, Fazzini P, Tomassetti L, Cozza V, Naso F, Marcozzi D, Petracchini F. Effects of deployment of electric vehicles on air quality in the urban area of Turin (Italy). J Environ Manage 2021; 297: 113416. [DOI] [PubMed] [Google Scholar]
- 15.Tessum CW, Hill JD, Marshall JD. Life cycle air quality impacts of conventional and alternative light-duty transportation in the United States. Proceedings of the National Academy of Sciences 2014; 111: 18490–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Schnell JL, Naik V, Horowitz LW, Paulot F, Ginoux P, Zhao M, Horton DE. Air quality impacts from the electrification of light-duty passenger vehicles in the United States. Atmospheric Environment 2019; 208: 95–102. [Google Scholar]
- 17.Gai Y, Minet L, Posen ID, Smargiassi A, Tétreault LF, Hatzopoulou M. Health and climate benefits of Electric Vehicle Deployment in the Greater Toronto and Hamilton Area. Environ Pollut 2020; 265: 114983. [DOI] [PubMed] [Google Scholar]
- 18.Maesano CN, Morel G, Matynia A, Ratsombath N, Bonnety J, Legros G, Da Costa P, Prud’homme J, Annesi-Maesano I. Impacts on human mortality due to reductions in PM(10) concentrations through different traffic scenarios in Paris, France. Sci Total Environ 2020; 698: 134257. [DOI] [PubMed] [Google Scholar]
- 19.Tobollik M, Keuken M, Sabel C, Cowie H, Tuomisto J, Sarigiannis D, Künzli N, Perez L, Mudu P. Health impact assessment of transport policies in Rotterdam: Decrease of total traffic and increase of electric car use. Environmental Research 2016; 146: 350–8. [DOI] [PubMed] [Google Scholar]
- 20.Filigrana P, Levy JI, Gauthier J, Batterman S, Adar SD. Health benefits from cleaner vehicles and increased active transportation in Seattle, Washington. J Expo Sci Environ Epidemiol 2022: 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Miranda ML, Edwards SE, Keating MH, Paul CJ. Making the environmental justice grade: the relative burden of air pollution exposure in the United States. Int J Environ Res Public Health 2011; 8: 1755–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Loustaunau MG, Chakraborty J. Vehicular Air Pollution in Houston, Texas: An Intra-Categorical Analysis of Environmental Injustice. Int J Environ Res Public Health 2019; 16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gunier RB, Hertz A, von Behren J, Reynolds P. Traffic density in California: Socioeconomic and ethnic differences among potentially exposed children. Journal of Exposure Science & Environmental Epidemiology 2003; 13: 240–6. [DOI] [PubMed] [Google Scholar]
- 24.Boogaard H, Patton AP, Atkinson RW, Brook JR, Chang HH, Crouse DL, Fussell JC, Hoek G, Hoffmann B, Kappeler R, Kutlar Joss M, Ondras M, Sagiv SK, Samoli E, Shaikh R, Smargiassi A, Szpiro AA, Van Vliet EDS, Vienneau D, Weuve J, Lurmann FW, Forastiere F. Long-term exposure to traffic-related air pollution and selected health outcomes: A systematic review and meta-analysis. Environ Int 2022; 164: 107262. [DOI] [PubMed] [Google Scholar]
- 25.Oluwoye J. Community Attitude towards Electric Vehicle: A Pilot Study of Edmonton Heights Underserved Neighborhood in Huntsville, Alabama. East African Scholars J Eng Comput Sci 2020; 3: 98–103. [Google Scholar]
- 26.Canepa K, Hardman S, Tal G. An early look at plug-in electric vehicle adoption in disadvantaged communities in California. Transport Policy 2019; 78: 19–30. [Google Scholar]
- 27.Burnett RT, Brook JR, Yung WT, Dales RE, Krewski D. Association between ozone and hospitalization for respiratory diseases in 16 Canadian cities. Environ Res 1997; 72: 24–31. [DOI] [PubMed] [Google Scholar]
- 28.Zanobetti A, Schwartz J, Dockery DW. Airborne particles are a risk factor for hospital admissions for heart and lung disease. Environ Health Perspect 2000; 108: 1071–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Szyszkowicz M, Kousha T, Castner J, Dales R. Air pollution and emergency department visits for respiratory diseases: A multi-city case crossover study. Environ Res 2018; 163: 263–9. [DOI] [PubMed] [Google Scholar]
- 30.Halonen JI, Lanki T, Yli-Tuomi T, Kulmala M, Tiittanen P, Pekkanen J. Urban air pollution, and asthma and COPD hospital emergency room visits. Thorax 2008; 63: 635–41. [DOI] [PubMed] [Google Scholar]
- 31.Barnett SB, Nurmagambetov TA. Costs of asthma in the United States: 2002–2007. J Allergy Clin Immunol 2011; 127: 145–52. [DOI] [PubMed] [Google Scholar]
- 32.Stingone JA, Claudio L. Disparities in the use of urgent health care services among asthmatic children. Ann Allergy Asthma Immunol 2006; 97: 244–50. [DOI] [PubMed] [Google Scholar]
- 33.Jones R, Lin S, Munsie JP, Radigan M, Hwang SA. Racial/ethnic differences in asthma-related emergency department visits and hospitalizations among children with wheeze in Buffalo, New York. J Asthma 2008; 45: 916–22. [DOI] [PubMed] [Google Scholar]
- 34.Erickson SE, Iribarren C, Tolstykh IV, Blanc PD, Eisner MD. Effect of race on asthma management and outcomes in a large, integrated managed care organization. Arch Intern Med 2007; 167: 1846–52. [DOI] [PubMed] [Google Scholar]
- 35.Griswold SK, Nordstrom CR, Clark S, Gaeta TJ, Price ML, Camargo CA Jr. Asthma exacerbations in North American adults: who are the “frequent fliers” in the emergency department? Chest 2005; 127: 1579–86. [DOI] [PubMed] [Google Scholar]
- 36.California Energy Commission. New ZEV Sales in California. 2022. April 13, 2022 [cited 2022 April 20]. Available from: http://www.energy.ca.gov/zevstats. [Google Scholar]
- 37.California Energy Commission. California Energy Commission Zero Emission Vehicle and Infrastructure Statistics. 2021. April 30, 2021 [cited 2022 March 8]. Available from: http://www.energy.ca.gov/zevstats. [Google Scholar]
- 38.United States Environmental Protection Agency. Integrated Science Assessment for Oxides of Nitrogen –Health Criteria. Research Triangle Park, NC: Office of Research and Development, National Center for Environmental Assessment; 2016. No. EPA/600/R–15/068. [Google Scholar]
- 39.U.S. Environmental Protection Agency. Air Data: Air Quality Data Collected at Outdoor Monitors Across the US. 2022. November 2, 2021 [cited 2022 March 10]. Available from: https://www.epa.gov/outdoor-air-quality-data. [Google Scholar]
- 40.U.S. Environmental Protection Agency. Who decides where monitors get placed? 2022. September 14, 2022 [cited 2022 December 19]. Available from: https://www.epa.gov/outdoor-air-quality-data/who-decides-where-monitors-get-placed. [Google Scholar]
- 41.U.S. Environmental Protection Agency. AirData Download Files Documentation: 4. Annual Summary Files. December 1, 2015. [cited 2022 December 19]. Available from: https://aqs.epa.gov/aqsweb/airdata/FileFormats.html#_annual_summary_files. [Google Scholar]
- 42.California Breathing Asthma Program. Asthma Emergency Department Visit Rates. In: California Department of Public Health, editor. Emergency Department data from the California Department of Health Care Access and Information: California Health and Human Services Agency Open Data; 2022. [Google Scholar]
- 43.Klein RJ, Schoenborn CA. Age adjustment using the 2000 projected U.S. population. Healthy People 2010 Stat Notes 2001: 1–10. [PubMed] [Google Scholar]
- 44.U.S. Census Bureau. American Community Survey Data. 2021.
- 45.Wood SN. Generalized Additive Models: An Introduction with R. Chapman and Hall/CRC; 2017. [Google Scholar]
- 46.Pinheiro J, Bates D, R Core Team. nlme: Linear and Nonlinear Mixed Effects Models. R package version 3.1–159, <https://CRAN.R-project.org/package=nlme>; 2022. [Google Scholar]
- 47.Pinheiro JC, Bates DM. Mixed-Effects Models in S and S-PLUS. New York, NY: Springer; 2000. [Google Scholar]
- 48.R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2022. [Google Scholar]
- 49.Lovasi GS, Treat CA, Fry D, Shah I, Clougherty JE, Berberian A, Perera FP, Kioumourtzoglou MA. Clean fleets, different streets: evaluating the effect of New York City’s clean bus program on changes to estimated ambient air pollution. J Expo Sci Environ Epidemiol 2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Adar SD, D’Souza J, Sheppard L, Kaufman JD, Hallstrand TS, Davey ME, Sullivan JR, Jahnke J, Koenig J, Larson TV, Liu LJ. Adopting Clean Fuels and Technologies on School Buses. Pollution and Health Impacts in Children. Am J Respir Crit Care Med 2015; 191: 1413–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Rogers EM. Diffusion of innovations. New York: Free Press; 2003. [Google Scholar]
- 52.Nordelöf A, Messagie M, Tillman A-M, Ljunggren Söderman M, Van Mierlo J. Environmental impacts of hybrid, plug-in hybrid, and battery electric vehicles—what can we learn from life cycle assessment? The International Journal of Life Cycle Assessment 2014; 19: 1866–90. [Google Scholar]
- 53.Zimm C. Improving the understanding of electric vehicle technology and policy diffusion across countries. Transport Policy 2021; 105: 54–66. [Google Scholar]
- 54.Timmers VRJH Achten PAJ. Non-exhaust PM emissions from electric vehicles. Atmospheric Environment 2016; 134: 10–7. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data that support the findings of this study are openly available in California Health and Human Services (CHHS) Open Data Portal at https://data.chhs.ca.gov/dataset/asthma-emergency-department-visit-rates; American Community Survey Data at https://www.census.gov/programs-surveys/acs/data.html; U.S. Environmental Protection Agency’s (EPA) AirData website at https://aqs.epa.gov/aqsweb/airdata/download_files.html; and California Energy Commission at http://www.energy.ca.gov/zevstats.