

Abstract
Aim:
The intraoral scanners are digital devices used to digitise the oral tissues. The accuracy of the intraoral scanners has been studied under different environmental conditions, but there might be differences that occur in the actual oral environment, which is still in question. The aim of the study was to evaluate the accuracy and efficiency of Parallel Confocal Microscopy and 3D in motion video with triangulation technology-based intraoral scanners under the influence of moisture and mouth opening.
Settings and Design:
This was an Cross over clinical controlled study.
Materials and Methods:
The controlled in vivo study included healthy subjects who were in need of CBCT for the purpose of locating the position of unerupted third molars before going abroad for a job. The subjects were exposed to scans in the upper and lower jaws with two intraoral scanners based on 3D motion video technology with triangulation (Medit) and parallel confocal microscopy (Trios) under the influence of two oral conditions, which were moisture (presence and absence of moisture) and mouth opening (30 mm and 50 mm, respectively). A total of 96 scans were obtained and superimposed individually over the reference CBCT scans to find the deviations in the Geomagic Rapidform (version 2020, USA) software. The efficiency of the scanners was calculated by recording the time taken and the number of images obtained after each scan.
Statistical Analysis Used:
The significance was calculated by using the independent and paired sample t test in SPSS software (IBM, version 23).
Results:
Based on the surface analysis, the trueness of the intra-oral scanners had statistically significant differences when compared between 3D in motion video technology with Triangulation and Parallel Confocal Microscopy (P < 0.05) whereas no statistical significance was observed in precision. There was a significant difference observed in the efficiency of the intra-oral scanners (P < 0.05).
Conclusion:
There is a significant difference in the accuracy and efficiency of the intraoral scanners under the influence of oral conditions, such as different moisture levels and mouth opening conditions. 3D in motion video technology with Triangulation showed better results with the least deviation than Parallel Confocal Microscopy.
Keywords: Accuracy, digital impression, digitizers, efficiency, images captured, innovation, intraoral scanners, mouth opening, optical impression, oral fluids, precision, saliva, time taken, trueness
INTRODUCTION
Optical scanners are an integral part of digital manufacturing owing to the fact that digitization is the source of creating virtual models that can be used for the fabrication of dental prostheses by digital methods. The intraoral scanners, in particular, are preferred over conventional impressions due to their ease of use, better accuracy, elimination of several material consumptions, and increased patient comfort; the only disadvantage is the cost factor. One additional benefit of digital impressions is the ease of storage and retrieval of the data even after years, unlike stone models that can chip, break, or consume physical clinical or laboratory working space. The data capture of the intraoral scanners (IOSs) remarkably varies among different commercially available computer-aided design/computer-aided manufacturing systems. Several in vitro and in vivo studies have been carried out to test the performance of the IOSs, and they have concluded that clinically acceptable and relatively precise impressions can be made with IOSs when compared to manual impressions.[1] Any movement by the subject or error in the path of movement of the scanner by the operator while scanning will greatly affect the stitching of the images. Several factors such as illuminance,[2-5] presence of liquids,[6,7] scanning pattern,[8] scanning distance,[9] software updates,[10] preparation type and tooth geometries,[11] the distance between the abutment and the adjacent teeth[12] are said to affect the accuracy of IOSs.
Parallel confocal microscopy is used for IOS systems. This technique is used to acquire in-focus images from selected depths, a process known as optical sectioning (high-resolution optical images with depth selectivity). The parallel confocal microscopy intraoral system also works according to the principles of confocal microscopy and has a fast scanning time. A fundamental characteristic of this system is the variation of the focal plane without moving the scanner toward the subject being scanned. This system has the feature of telecentricity in the space of the subject being scanned, and it is possible to shift the focal plane while keeping telecentricity and magnification ratio.
Three dimensional (3D) in motion video technology with triangulation is able to capture moving objects. The scanner adjusts to the speed we want and is, therefore, able to follow along when the object is in motion. Meanwhile, picture-type scanning takes one picture per second. This means that the object must be held stationary to achieve the accuracy needed for good-quality images. Essentially, triangulation uses a 3-camera pattern to capture 3D imagery for this type of IOS. What makes triangulation useful is its ability to acquire high-speed data from materials we do not want to be in too much contact with, such as delicate or wet materials. In fact, triangulation principles have been widely used for centuries, but we are now beginning to really utilize them for industrial applications.
According to the present study, the trueness of the IOSs is the comparison done within the mouth opening conditions and the moisture conditions, whereas precision is the comparison between the 3D in motion video technology with triangulation and parallel confocal microscopy IOSs under different moisture and mouth opening conditions. Although we have different IOSs commercially available in the market, there is very little literature mentioning the significance of using a particular type of scanner for said intraoral or environmental conditions to avoid inaccuracies and increase the efficiency of the IOS. The study aims to compare the accuracy (trueness and precision) of two different technology-based IOSs (3D in motion video with triangulation and parallel confocal microscopy) and the efficiency, which is the time taken and the number of images obtained per scan; under different oral conditions, i.e., in the presence and absence of moisture and at two different degrees of mouth opening. The null hypothesis states that there is no difference between the two types of IOSs in terms of accuracy and efficiency.
MATERIALS AND METHODS
The clinical study was approved by the human ethics committee of the university (SRB/SDC/PROSTHO-1801/21/TH-031). All ethical guidelines specified by the WHO and the Declaration of Helsinki, 1954, were satisfied. All participants were briefed about the study, and they willingly signed informed consent forms.
Study design
A crossover clinical trial was conducted on six subjects. Each subject underwent four intraoral scans, which were full arch scans obtained from both the upper and lower arches of the subjects with two IOSs using 3D in motion video technology with triangulation (Medit i500) and parallel confocal microscopy (Trios 3) [Table 1] under 30 mm and 50 mm mouth openings and the presence and absence of saliva (total n = 96), which gave the accuracy of the scanners and the data on time taken and the number of images obtained was used to calculate the efficiency of the scanners, for which the data were extracted from the software while scanning under each condition. The sample size (n = 96) was calculated with G*Power software (Version 3.1.9.4) Mac OS X and windows XP/ vista/7/8 with a power of 95% and a high-intensity alpha error of 0.05.
Table 1.
Comparison of the different technology based intraoral scanners used in the study
| Scanner | Manufacturer | Software technology | Light source | Version |
|---|---|---|---|---|
| Trios | 3 shape | Parallel confocal microscopy | Laser | 21.2.0 |
| Medit i500 | Medit | 3D in motion video technology with triangulation | LED | V 2.4.6 |
3D: Three dimensional, LED: Light-emitting diode
Participants, eligibility criteria, and settings
Volunteers who needed a cone-beam computerized tomography (CBCT) scan to locate and determine the prognosis of their third molars without any symptoms before going abroad for a job were asked for their consent to participate in the study. They were screened for any calculus or debris and any deep caries lesions. The subjects had to have an average mouth opening of 50–55 mm. Six subjects, ranging in age from 20 to 25 years, took part in the study, and they were chosen at random from a pool of 20 other subjects. The eligibility criteria were as follows:
Inclusion criteria
Healthy controls with normal gait, stature, and build in the age group of 20–25 years of any gender with no history of systemic diseases who had a completely dentulous upper and lower arch, subjects with a complete eruption of all teeth until the second molars, mouth opening in the range of 50–55 mm, subjects with unerupted third molars without any symptoms, and subjects with normal viscosity of saliva with the normal flow were included in the study.
Exclusion criteria
Subjects with partial or complete edentulousness, restricted mouth opening, subjects who had restorations or replacements or had deep carious lesions; subjects with salivary gland disorder or with hypersalivation and xerostomia; subjects with thin or ropy saliva; subjects with noncarious lesions such as attrition, abrasion, or erosion were excluded from the study.
Intervention
The first part of the study was carried out in three steps: a CBCT scan; intraoral scanning under 30 mm and 50 mm mouth openings for the presence or absence of saliva using Medit and Trio IOSs; and the superimposition of intraoral scan data to CBCT data to evaluate the accuracy of IOS.
The second part of the study was carried out in two steps. The data entry was done after each intraoral scan, and the total number of images obtained and the scanning time were noted down from the display on the screen of the intraoral scanning software. The data were processed into an Excel sheet for statistical analysis, thereby defining the efficiency of the scanners.
Cone-beam computerized tomography scan
The subject was asked to remove any metal accessories in the head-and-neck region before proceeding with the CBCT preparation. The CBCT scan of the subject was made by making the subject stand upright with the chin resting on the chin rest. To avoid any head movements, the patient’s head is locked in position. The laser point of the CBCT machine is made to coincide with the incisors of the patient using a thumbwheel. The subject is requested to maintain a still intraoral posture by not swallowing/grinding/moving during the exposure. The CBCT data were exported in DICOM format and converted into STL format with the help of online solutions. To maintain the standardization of the study, all the scans were done at the same time by the same operator.
Intraoral scan
Scanner preparation
To obtain a gold standard scan, the IOSs were calibrated using the calibration tool kit and as suggested by the manufacturer. The scanners were connected to the desktop computer with the software open to initialize the assisted calibration process. The tip of the IOS is inserted into the calibration object, and the calibration process is started from within the software. The process takes up to 3 min, during which the scanner runs through predefined motions and calibrates itself. Once the calibration is over, the object is separated from the scanner tip, and the scanner is ready for use. The calibration process is carried out after each scan, and the tips of the scanners are disinfected and sterilized according to the manufacturer’s recommendation.
Preparing the subjects for intraoral scanning
Subjects were made to sit upright in a dental chair and asked to open their mouths to the fullest without resisting the free movement of the scanner. The scans were made with parallel confocal microscopy-based IOS followed by 3D in motion video technology with triangulation-based IOS under each condition. The whole procedure was done by a single operator and one observer at the same time for all the subjects under each condition for the standardization of the study. The observer was completely unaware of the scanner for blinding to eliminate bias.
Scanning under different degrees of mouth opening
All the subjects were made to sit in an upright position in a dental chair. They were instructed to rinse their mouths with plain water, swallow the pooled saliva, and open their mouths for scanning. The mouth opening was controlled and maintained at 50 mm with the help of the Boley’s gauge. The gauge was positioned in the right quadrant while scanning the left quadrant and in the left quadrant while scanning the right quadrant. The same was done for a 30 mm mouth opening. To follow the scanning sequence, the scanning was carried out until the gauge stopped while the gauge was being replaced in the other arch and then continued in the other arch.
Scanning under different moisture conditions
The patients were given a cup of water to rinse and asked to swallow any pooled saliva completely and open their mouths for the presence of moisture. In the absence of moisture, the subjects are asked to open their mouths, and the saliva is completely suctioned with the help of suction and wiped all around the surfaces manually with a cotton roll. The cotton rolls were also used to isolate the mucosa from the surface of the tooth, and mild air was blown with the three-way syringe. The suction was constantly placed on the floor of the mouth.
Scanning pattern
The scans were made in the upper arch, followed by the lower arch. The occlusal surface of the tooth was covered, followed by the lingual and buccal surfaces, starting from the distal most molars and passing through the incisors to the other side molar for covering the surfaces in the said pattern. The soft tissue was retracted using fingers on the buccal side and a mouth mirror on the lingual side.
Superimposition of scans
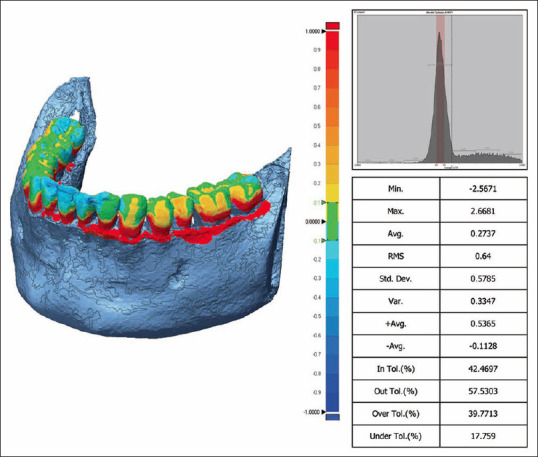
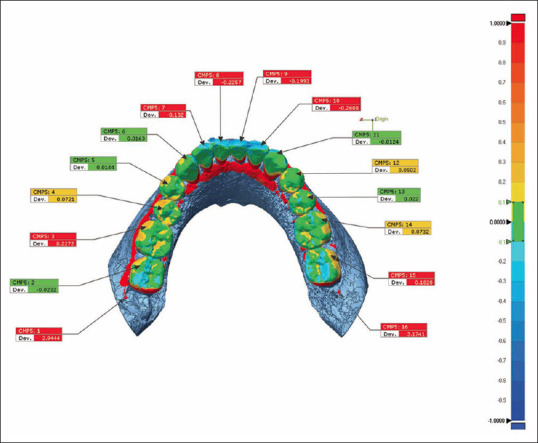
For superimposition and surface analysis, the Geomagic Rapidform (version 2020, USA) was used. The CBCT scan was considered the reference scan, and the X, Y, and Z coordinates were determined to be fixed. The intraoral scans were imported one by one into the software and made to run through an initial fit and a best-fit algorithm [Figure 1]. The values of discrepancies that arose between the reference scan and model scan were measured and displayed by the software based on the root mean square (RMS) value [Figure 2], surface maximum deviation [Figure 3], and maximum deviation in the X, Y, and Z axes [Figure 4].
Figure 1.
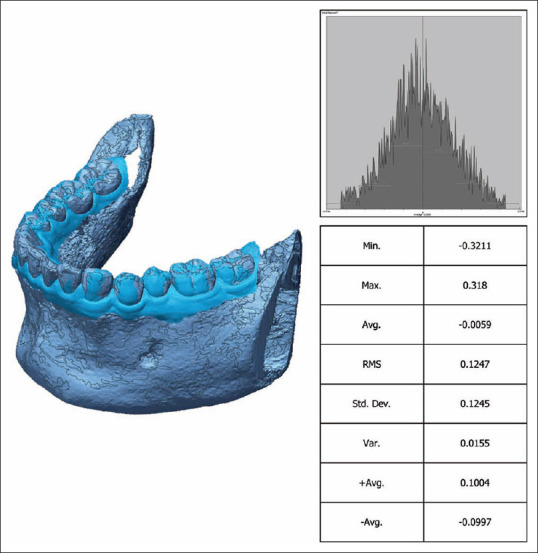
Image showing alignment of reference (CBCT) and sample data (IOS) after superimposition (best fit algorithm). CBCT: Cone-beam computerized tomography, IOS: Intraoral scan
Figure 2.
3D compare image of surface analysis with RMS values extracted by Geomagic software. 3D: Three-dimensional, RMS: Root mean square
Figure 3.
3D compare image of surface analysis with maximum deviation values extracted by Geomagic software. 3D: Three dimensional
Figure 4.
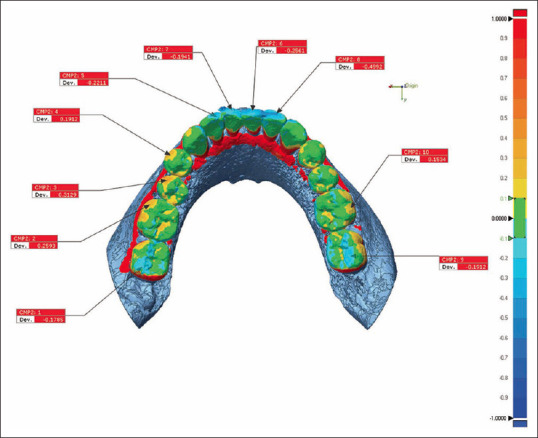
The deviations in X, Y, Z coordinate axis
Statistical analysis
Statistical analysis was performed using SPSS software (Version 23.0. Armonk, New York: IBM Corp). Data collection was done with the help of the data collection sheets. Descriptive statistics (mean, standard deviation, and standard error) were carried out for each group. An unpaired t-test was carried out to find the significance between the groups (3D in motion video technology with triangulation and parallel confocal microscopy. A paired t-test was carried out to find the significance within subgroups of moisture (between the presence and absence of moisture) and mouth opening (30 mm and 50 mm).
RESULTS
The IOSs were compared for accuracy (trueness and precision) and efficiency (time taken and number of images). The results of the samples were analyzed for accuracy based on deviations observed from the results of superimposition between the reference scan and the experimental scans in surface analysis and specific points in molars, canines, and incisors in the X, Y, and Z coordinates in coordinate analysis.
Moisture conditions
The accuracy of the IOSs did not have any statistically significant difference when compared between the presence and absence of moisture (precision) [Table 2]. The accuracy of the intraoral scanners had statistically significant differences in the RMS value when compared between two systems of scanners (trueness) for lower scans with a P < 0.05. However, there was no statistically significant difference observed with the presence of moisture in the upper arch scan. The least deviations were observed in the 3D in motion video technology with the triangulation group under the presence and absence of moisture for both the upper and lower arch [Table 3].
Table 2.
Comparison between the presence and absence of moisture based on deviations observed in surface analysis
| IOS | Arch | Moisture conditions | Mean±SD | SE | CI | t | P | |
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Lower bound | Upper bound | |||||||
| Parallel confocal microscopy | Upper | Presence of moisture | 0.55±0.14 | 0.05 | 0.40 | 0.70 | 0.46 | 0.65 |
| Absence of moisture | 0.60±0.17 | 0.07 | 0.42 | 0.78 | ||||
| Lower | Presence of moisture | 0.42±0.14 | 0.05 | 0.27 | 0.57 | 0.02 | 0.97 | |
| Absence of moisture | 0.42±0.15 | 0.06 | 0.26 | 0.58 | ||||
| 3D in motion video technology with triangulation | Upper | Presence of moisture | 0.41±0.13 | 0.05 | 0.26 | 0.55 | 0.37 | 0.71 |
| Absence of moisture | 0.37±0.15 | 0.06 | 0.21 | 0.54 | ||||
| Lower | Presence of moisture | 0.23±0.07 | 0.02 | 0.16 | 0.31 | 0.91 | 0.38 | |
| Absence of moisture | 0.20±0.04 | 0.02 | 0.15 | 0.25 | ||||
P value derived from paired sample t-test. 3D: Three dimensional, CI: Confidence interval, SE: Standard error, SD: Standard deviation, IOS: Intraoral scanner
Table 3.
Root mean square value of deviation in moisture conditions between two technology-based intraoral scanner
| Arches | Moisture conditions | IOS | Mean±SD | P |
|---|---|---|---|---|
| Lower | Presence of moisture | 3D in motion video technology with triangulation | 0.61±0.09 | 0.02* |
| Parallel confocal microscopy | 0.84±0.20 | |||
| Absence of moisture | 3D in motion video technology with triangulation | 0.62±0.12 | 0.04* | |
| Parallel confocal microscopy | 0.87±0.24 | |||
| Upper | Presence of moisture | 3D in motion video technology with triangulation | 0.94±0.20 | 0.08 |
| Parallel confocal microscopy | 1.16±0.19 | |||
| Absence of moisture | 3D in motion video technology with triangulation | 0.92±0.20 | 0.07 | |
| Parallel confocal microscopy | 1.17±0.23 |
*Level of significance P<0.05. P value derived from independent t-test. 3D: Three dimensional, SD: Standard deviation, IOS: Intraoral scanner
Mouth opening
The accuracy of the IOSs did not show any statistically significant difference when compared between 30 mm of mouth opening and 50 mm of mouth opening (precision) [Table 4]. The accuracy of the intraoral scanners showed statistically significant differences when compared between the group’s (i.e., Trueness) lower scan with 50 mm of mouth opening and the rest showing 3D in motion video technology with triangulation scan with better accuracy of the RMS value but statistically not significant [P < 0.05, Table 5].
Table 4.
Comparison of the deviations observed in surface analysis between 30 mm mouth opening and 50 mm mouth opening conditions
| Intra oral scanner | Arch | Mouth opening | P | SE | CI | t | P | |
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Lower bound | Upper bound | |||||||
| Parallel confocal microscopy | Upper | 30 mm mouth opening | 0.59±0.15 | 0.06 | 0.42 | 0.75 | 0.39 | 0.70 |
| 50 mm mouth opening | 0.55±0.14 | 0.05 | 0.40 | 0.70 | ||||
| Lower | 30 mm mouth opening | 0.36±0.08 | 0.03 | 0.27 | 0.45 | 0.91 | 0.38 | |
| 50 mm mouth opening | 0.42±0.14 | 0.05 | 0.27 | 0.57 | ||||
| 3D in motion video technology with triangulation | Upper | 30 mm mouth opening | 0.41±0.10 | 0.04 | 0.31 | 0.52 | 0.10 | 0.91 |
| 50 mm mouth opening | 0.41±0.13 | 0.05 | 0.26 | 0.55 | ||||
| Lower | 30 mm mouth opening | 0.21±0.06 | 0.02 | 0.14 | 0.28 | 0.56 | 0.58 | |
| 50 mm mouth opening | 0.23±0.07 | 0.02 | 0.16 | 0.31 | ||||
P value derived from paired sample t-test. 3D: Three dimensional, SD: Standard deviation, CI: Confidence interval, SE: Standard error
Table 5.
Root mean square value of deviation in mouth opening conditions (30 mm and 50 mm) between two technology-based intraoral scanner
| Arches | Mouth opening conditions | IOS | Mean±SD | P |
|---|---|---|---|---|
| Lower | 30 mm | 3D in motion video technology with triangulation | 0.97±0.17 | 0.14 |
| Parallel confocal microscopy | 1.15±0.21 | |||
| 50 mm | 3D in motion video technology with triangulation | 0.61±0.09 | 0.02* | |
| Parallel confocal microscopy | 0.84±0.20 | |||
| Upper | 30 mm | 3D in motion video technology with triangulation | 0.94±0.20 | 0.07 |
| Parallel confocal microscopy | 1.16±0.19 | |||
| 50 mm | 3D in motion video technology with triangulation | 0.94±0.20 | 0.08 | |
| Parallel confocal microscopy | 1.16±0.19 |
*Level of significance P<0.05. P value derived from independent sample t-test. 3D: Three dimensional, SD: Standard deviation, IOS: Intraoral scanner
Coordinate analysis
The analysis of sample results corresponding to X, Y, and Z coordinates showed no statistically significant difference in accuracy when compared between the mouth opening conditions and moisture condition. The coordinate axis analysis was done at five specific points, which were the right and left molars, the right and left canines, and one central incisor of the upper and lower arches [Tables 6 and 7].
Table 6.
Comparison of two different technology-based scanner based on the three-dimensional discrepancies observed between each intraoral scan and cone-beam computed tomography in the incisor, canine, and molar regions under the influence of the presence and absence of moisture
| IOS | Parallel confocal microscopy | 3D in motion video technology with triangulation | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|||||||||
| Arch | Coordinates and points | Mesiopalatal cusp M1 (R) | Mesiopalatal cusp M2 (L) | Cuspal tip C1 (R) | Cuspal tip C2 (L) | Incisal edge I1 (R) | Mesiopalatal cusp M1 (R) | Mesiopalatal cusp M2 (L) | Cuspal tip C1 (R) | Cuspal tip C2 (L) | Incisal edge I1 (R) |
| Upper | X coordinate | ||||||||||
| Mean±SD | −0.01±0.04 | 0.02±0.04 | −0.02±0.02 | 0.01±0.01 | −0.00±0.01 | 0.03±0.04 | −0.02±0.02 | −0.02±0.10 | 0.02±0.02 | −0.00±0.01 | |
| P | 0.30 | 0.17 | 0.05* | 0.03* | 0.68 | 0.09 | 0.10 | 0.54 | 0.14 | 0.97 | |
| Y coordinate | |||||||||||
| Mean±SD | −0.00±0.01 | 0.00±0.03 | −0.00±0.03 | −0.03±0.08 | −0.01±0.03 | 0.00±0.02 | 0.00±0.03 | −0.05±0.12 | −0.00±0.05 | −0.02±0.03 | |
| P | 0.34 | 0.67 | 0.54 | 0.38 | 0.26 | 0.53 | 0.89 | 0.31 | 0.68 | 0.19 | |
| Z coordinate | |||||||||||
| Mean±SD | 0.02±0.04 | 0.03±0.04 | −0.04±0.06 | −0.04±0.14 | −0.06±0.11 | −0.03±0.04 | −0.11±0.15 | −0.14±0.16 | 0.03±0.08 | −0.03±0.17 | |
| P | 0.33 | 0.11 | 0.15 | 0.46 | 0.22 | 0.07 | 0.14 | 0.08 | 0.40 | 0.67 | |
| Lower | X coordinate | ||||||||||
| Mean±SD | 0.00±0.03 | 0.00±0.02 | 0.00±0.00 | −0.01±0.01 | 0.00±0.00 | −0.03±0.03 | −0.01±0.02 | −0.00±0.02 | −0.00±0.01 | 0.00±0.01 | |
| P | 0.94 | 0.56 | 0.07 | 0.06 | 0.07 | 0.03* | 0.40 | 0.89 | 0.60 | 0.69 | |
| Y coordinate | |||||||||||
| Mean±SD | 0.00±0.04 | 0.00±0.02 | −0.00±0.00 | −0.01±0.01 | −0.01±0.03 | 0.28±0.01 | −0.00±0.02 | 0.01±0.02 | −0.00±0.01 | 0.00±0.01 | |
| P | 0.78 | 0.51 | 0.03* | 0.07 | 0.29 | 0.01* | 0.47 | 0.27 | 0.77 | 0.47 | |
| Z coordinate | |||||||||||
| Mean±SD | −0.00±0.03 | 0.00±0.05 | 0.01±0.01 | 0.03±0.04 | 0.04±0.08 | −0.03±0.02 | 0.00±0.05 | −0.00±0.05 | 0.00±0.03 | −0.01±0.05 | |
| P | 0.74 | 0.78 | 0.07 | 0.10 | 0.27 | 0.01* | 0.78 | 0.75 | 0.64 | 0.56 | |
*Level of significance P<0.05. P value derived from independent sample t-test. 3D: Three dimensional, SD: Standard deviation, IOS: Intraoral scanner
Table 7.
Comparison of two different technology-based scanner based on the three-dimensional discrepancies observed between each intraoral scan and cone-beam computed tomography in the incisor, canine, and molar regions under the influence of 30 mm mouth opening and 50 mm mouth opening conditions
| IOS | Parallel confocal microscopy | 3D in motion video technology with triangulation | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|||||||||
| Arch | Coordinates and points | Mesiopalatal cuspal M1 at 3 | Mesiopalatal cuspal M2 (L) 14 | Cuspal tip C1 at 6 | Cuspal tip C2 (L) 11 | Incisal edge I1 at 8 | Mesiopalatal cuspal M1 (R) | Mesiopalatal cuspal M2 (L) | Cuspal tip C1 (R) | Cuspal tip C2 (L) | Incisal edge I1 (R) |
| Upper | X coordinate | ||||||||||
| Mean±SD | −0.04±0.07 | 0.07±0.14 | −0.05±0.07 | −0.00±0.02 | 0.00±0.02 | 0.05±0.13 | −0.02±0.08 | −0.02±0.10 | 0.01±0.01 | 0.00±0.00 | |
| P | 0.24 | 0.26 | 0.12 | 0.99 | 0.83 | 0.40 | 0.50 | 0.51 | 0.11 | 0.65 | |
| Y coordinate | |||||||||||
| Mean±SD | −0.01±0.04 | 0.02±0.10 | −0.04±0.11 | −0.06±0.11 | 0.00±0.09 | −0.01±0.05 | −0.00±0.06 | −0.04±0.13 | −0.03±0.06 | −0.01±0.03 | |
| P | 0.45 | 0.52 | 0.40 | 0.20 | 0.95 | 0.49 | 0.76 | 0.46 | 0.24 | 0.24 | |
| Z coordinate | |||||||||||
| Mean±SD | 0.04±0.08 | 0.08±0.14 | −0.02±0.15 | −0.12±0.20 | −0.04±0.20 | −0.02±0.10 | −0.03±0.10 | −0.11±0.15 | 0.02±0.08 | −0.02±0.15 | |
| P | 0.29 | 0.20 | 0.76 | 0.21 | 0.63 | 0.57 | 0.40 | 0.14 | 0.52 | 0.68 | |
| Lower | X coordinate | ||||||||||
| Mean±SD | 0.01±0.08 | −0.00±0.03 | −0.00±0.04 | −0.00±0.03 | −0.00±0.01 | −0.05±0.05 | 0.01±0.04 | −0.00±0.02 | −0.00±0.03 | 0.00±0.01 | |
| P | 0.76 | 0.73 | 0.74 | 0.89 | 0.39 | 0.06 | 0.32 | 0.57 | 0.84 | 0.61 | |
| Y coordinate | |||||||||||
| Mean±SD | 0.00±0.06 | −0.00±0.03 | −0.01±0.03 | 0.00±0.03 | −0.00±0.03 | 0.04±0.04 | 0.01±0.03 | 0.01±0.05 | 0.01±0.30 | −0.01±0.02 | |
| P | 0.89 | 0.85 | 0.42 | 0.63 | 0.87 | 0.08 | 0.44 | 0.60 | 0.43 | 0.17 | |
| Z coordinate | |||||||||||
| Mean±SD | −0.00±0.06 | 0.00±0.07 | 0.01±0.10 | −0.00±0.15 | 0.02±0.09 | −0.05±0.05 | −0.06±0.07 | −0.01±0.07 | 0.02±0.12 | −0.11±0.15 | |
| P | 0.99 | 0.77 | 0.80 | 0.94 | 0.51 | 0.05* | 0.11 | 0.71 | 0.68 | 0.14 | |
*Level of significance P<0.05. P value derived from independent sample t-test. 3D: Three dimensional, SD: Standard deviation, IOS: Intraoral scanner
Efficiency of the intraoral scanners
Statistically significant differences were found in the precision of the IOSs for time taken under mouth opening conditions and the trueness of the IOSs under moisture conditions. In terms of images obtained, there was a significant difference in the trueness of the IOSs under different mouth opening and moisture conditions [Table 8].
Table 8.
Comparison of efficiency (time taken and images obtained) of two different technology-based intraoral scanners under the influence of different mouth opening (30 mm and 50 mm) and moisture (presence and absence) conditions
| Arch | Oral conditions | Intraoral scanner | Time taken | Images obtained | ||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| Mean±SD | SE | P | Mean±SD | SE | P | |||
| Upper | 30 mm mouth opening | 3D in motion video technology with triangulation | 59.16±12.02 | 4.90 | 0.28 | 1135.50±331.54 | 135.35 | 0.50 |
| Parallel confocal microscopy | 71.16±23.34 | 9.53 | 1015.33±259.63 | 105.99 | ||||
| 55 mm mouth opening | 3D in motion video technology with triangulation | 61.00±10.84 | 4.42 | 0.16 | 1338.66±257.68 | 105.19 | 0.52 | |
| Parallel confocal microscopy | 81.33±31.60 | 12.90 | 1212.33±394.13 | 160.90 | ||||
| Lower | 30 mm mouth opening | 3D in motion video technology with triangulation | 59.16±13.60 | 5.55 | 0.04* | 1213.50±357.49 | 145.94 | 0.01* |
| Parallel confocal microscopy | 43.66±9.72 | 3.97 | 733.50±136.46 | 55.71 | ||||
| 55 mm mouth opening | 3D in motion video technology with triangulation | 70.66±17.30 | 7.06 | 0.80 | 1424.33±331.90 | 135.49 | 0.04* | |
| Parallel confocal microscopy | 68.16±15.91 | 6.49 | 1036.66±237.42 | 96.92 | ||||
| Upper | Absence of moisture | 3D in motion video technology with triangulation | 55.00±11.94 | 4.87 | 0.79 | 1110.66±222.08 | 90.66 | 0.14 |
| Parallel confocal microscopy | 57.33±17.15 | 7.00 | 901.66±237.00 | 96.75 | ||||
| Presence of moisture | 3D in motion video technology with triangulation | 58.33±8.35 | 3.41 | 0.11 | 1318.33±283.34 | 115.67 | 0.60 | |
| Parallel confocal microscopy | 81.33±31.60 | 12.90 | 1212.33±394.13 | 160.90 | ||||
| Lower | Absence of moisture | 3D in motion video technology with triangulation | 52.66±10.55 | 4.31 | 0.44 | 1008.50±207.37 | 84.66 | 0.07* |
| Parallel confocal microscopy | 47.33±12.62 | 5.15 | 780.33±186.70 | 76.22 | ||||
| Presence of moisture | 3D in motion video technology with triangulation | 73.83±17.35 | 7.08 | 0.53 | 1478.00±285.33 | 116.48 | 0.03* | |
| Parallel confocal microscopy | 67.66±15.53 | 6.34 | 1088.00±246.75 | 100.73 | ||||
*Level of significance P<0.05. 3D: Three dimensional, SD: Standard deviation, SE: Standard error
DISCUSSION
The effect of saliva and oral liquids on the accuracy of the IOSs is found to be significantly similar to the in vivo study done by Camcı and Salmanpour.[13] In surface analysis, there was a significant difference in trueness but no significant difference in the precision of the IOSs under the influence of moisture conditions, which was in favor of the previous literature.[6] There was a significant difference in trueness, with the least deviations observed in 3D in motion video technology with triangulation than in parallel confocal microscopy, which was contrary to results published by Biagio Rapone,[14] where parallel confocal microscopy showed the least deviations when compared to the other two IOSs used in the study, yet 3D in motion video technology with triangulation IOS was not used in the study, making the results incomparable with the present study. 3D in motion video technology with triangulation showed the least deviations with an absence of moisture, irrespective of the arches, which may be due to 3D in motion video technology. The precision of both IOSs had lesser deviations in the lower arch and greater deviations in the upper arch, and this may be due to the fact that there is limited light exposure or direct light on the upper arch compared to the lower arch under any light conditions, the deviations in the first molars in the upper arch can be due to the parotid duct opening, and the lower arch can be due to the pooling of saliva in the posterior regions, and the tendency for inaccuracies to decrease from anterior to posterior in full arch scans. The deviations between the reference scan and the experimental scan were measured using superimposition techniques, and the analysis was carried out in two categories, namely surface analysis and coordinate axis analysis, to get the proper decision.
The coordinate axis analysis was done at five specific points, which were the right and left molars, the canine, and one central incisor of the upper and lower arches. The molars indicated the possible deviations that may arise in the posterior region; the canines indicated the possible deviations that may arise during the arch shift, and the incisors indicated the possible deviations that might arise in the anterior region. Also from the previous literature, the tooth types and geometries have shown to make a significant difference in the accuracy of the IOSs. There is a tendency for the inaccuracies to decrease from the anterior to the posterior in full arch scans.[15] In coordinate analysis, there is no significant difference in trueness but there was a significant difference in precision observed in the trios IOS in cuspal tips C1(R) and C2(L) in the X coordinate of the upper arch and in the Y coordinate of cuspal tip C1(R) in the lower arch. Increased deviations in the canine region can be because of the smoothness and regularity of the tooth surface of the canine and because deviations can occur during the arch shift.[15]
The accuracy values denoted the efficacy of the IOSs, whereas the efficiency of the IOSs was calculated based on the time taken and the number of images recorded and displayed by the software of the IOSs when the intraoral scans were taken.[16] With regard to the trueness of the time taken, there was no significant difference with the IOSs. The lowest measurements were observed in the absence of moisture, followed by the presence of moisture, irrespective of the IOS used suggesting that the absence of moisture helps in increasing the efficiency of both IOSs, supporting previous literature.[17-20]
Any movement during the scanning procedure can affect the flow of image capture. The major movements made by the patient during intraoral scanning would be mouth closure, which can be due to fatigue or restricted mouth opening. To evaluate the accuracy of the IOSs under the influence of the mouth opening conditions, two measurements were taken: 50 mm, considering the average mouth opening of Indian adults, and 30 mm, considering the average tip diameter of both IOSs used in the study. The mouth opening was controlled with the help of a Boley’s gauge. The movement of the subject’s head was controlled by resting on the headrest of the chair and was monitored by the observer. Furthermore, subjects with normal height, stature, and build were selected to avoid inconsistencies. In surface analysis, there were significant differences in the trueness of the IOSs at 30 mm mouth opening, followed by 50 mm mouth opening in the lower arch and 30 mm mouth opening in the upper arch, and close to the significant value at 50 mm mouth opening in the upper arch. There was no significant difference observed in the precision of the IOSs. 3D in motion video technology with triangulation showed better accuracy values than trios. The lower arch, irrespective of the scanners, showed better accuracy than the upper arches. This may be because of the restrictions on opening the mouth; the free movement of the scanner in the upper posterior regions might be restricted, leading to more inaccuracies. In coordinate axis analysis, there is no significant difference in trueness but there is a significant difference in precision. Trios showed more negative deviations in both upper and lower arches, with all the coordinate axes X, Y, and Z indicating superiority toward 3D in motion video with triangulation technology.
The limitations of the study are that the subjects had ideal occlusions and sound tooth structure; partial or complete edentulousness or the presence of replacements and restorations might affect the accuracy of the scanners. Standard measuring and analyzing methods have to be used for 3D analysis. The study was performed with a single right-handed operator to avoid inconsistencies in results; this might cause errors that may arise due to operator fatigue. The study rejected the null hypothesis. With continuous improvements being made in the imaging principles of the intraoral scanners and the scanning techniques, the standards of the intraoral scanners can be raised in the near future.
CONCLUSION
Within the limitations of the study, there is a significant difference in the accuracy and efficiency of the IOSs under the influence of oral conditions such as different moisture levels and mouth opening conditions. 3D in motion video technology with triangulation showed better results with the least deviation than parallel confocal microscopy. The future scope of the study would be suggestions to use more standardized measuring techniques and subject-specific scanners, which will not have a great effect on any of the clinical variables. This can lead to great success in terms of the accuracy of digital impressions and help take digital dentistry to the next level.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Aswani K, Wankhade S, Khalikar A, Deogade S. Accuracy of an intraoral digital impression: A review. J Indian Prosthodont Soc. 2020;20:27–37. doi: 10.4103/jips.jips_327_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Revilla-León M, Jiang P, Sadeghpour M, Piedra-Cascón W, Zandinejad A, Özcan M, et al. Intraoral digital scans-Part 1: Influence of ambient scanning light conditions on the accuracy (trueness and precision) of different intraoral scanners. J Prosthet Dent. 2020;124:372–8. doi: 10.1016/j.prosdent.2019.06.003. [DOI] [PubMed] [Google Scholar]
- 3.Arakida T, Kanazawa M, Iwaki M, Suzuki T, Minakuchi S. Evaluating the influence of ambient light on scanning trueness, precision, and time of intra oral scanner. J Prosthodont Res. 2018;62:324–9. doi: 10.1016/j.jpor.2017.12.005. [DOI] [PubMed] [Google Scholar]
- 4.Wesemann C, Kienbaum H, Thun M, Spies BC, Beuer F, Bumann A. Does ambient light affect the accuracy and scanning time of intraoral scans? J Prosthet Dent. 2021;125:924–31. doi: 10.1016/j.prosdent.2020.03.021. [DOI] [PubMed] [Google Scholar]
- 5.Koseoglu M, Kahramanoglu E, Akin H. Evaluating the effect of ambient and scanning lights on the trueness of the intraoral scanner. J Prosthodont. 2021;30:811–6. doi: 10.1111/jopr.13341. [DOI] [PubMed] [Google Scholar]
- 6.Chen Y, Zhai Z, Li H, Yamada S, Matsuoka T, Ono S, et al. Influence of liquid on the tooth surface on the accuracy of intraoral scanners: An in vitro study. J Prosthodont. 2022;31:59–64. doi: 10.1111/jopr.13358. [DOI] [PubMed] [Google Scholar]
- 7.Kachhara S, Nallaswamy D, Ganapathy DM, Sivaswamy V, Rajaraman V. Assessment of intraoral scanning technology for multiple implant impressions –A systematic review and meta-analysis. J Indian Prosthodont Soc. 2020;20:141–52. doi: 10.4103/jips.jips_379_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Latham J, Ludlow M, Mennito A, Kelly A, Evans Z, Renne W. Effect of scan pattern on complete-arch scans with 4 digital scanners. J Prosthet Dent. 2020;123:85–95. doi: 10.1016/j.prosdent.2019.02.008. [DOI] [PubMed] [Google Scholar]
- 9.Kim MK, Kim JM, Lee YM, Lim YJ, Lee SP. The effect of scanning distance on the accuracy of intra-oral scanners used in dentistry. Clin Anat. 2019;32:430–8. doi: 10.1002/ca.23334. [DOI] [PubMed] [Google Scholar]
- 10.Vág J, Renne W, Revell G, Ludlow M, Mennito A, Teich ST, et al. The effect of software updates on the trueness and precision of intraoral scanners. Quintessence Int. 2021;52:636–44. doi: 10.3290/j.qi.b1098315. [DOI] [PubMed] [Google Scholar]
- 11.Ashraf Y, Sabet A, Hamdy A, Ebeid K. Influence of preparation type and tooth geometry on the accuracy of different intraoral scanners. J Prosthodont. 2020;29:800–4. doi: 10.1111/jopr.13202. [DOI] [PubMed] [Google Scholar]
- 12.Huang MY, Son K, Lee KB. Effect of distance between the abutment and the adjacent teeth on intraoral scanning: An in vitro study. J Prosthet Dent. 2021;125:911–7. doi: 10.1016/j.prosdent.2020.02.034. [DOI] [PubMed] [Google Scholar]
- 13.Camcı H, Salmanpour F. Effect of saliva isolation and intraoral light levels on performance of intraoral scanners. Am J Orthod Dentofacial Orthop. 2020;158:759–66. doi: 10.1016/j.ajodo.2020.03.022. [DOI] [PubMed] [Google Scholar]
- 14.Rapone B, Palmisano C, Ferrara E, Di Venere D, Albanese G, Corsalini M. The accuracy of three intraoral scanners in the oral environment with and without saliva: A comparative study. NATO Adv Sci Inst Ser E Appl Sci. 2020;10:7762. [Google Scholar]
- 15.Son K, Lee KB. Effect of tooth types on the accuracy of dental 3D scanners: An in vitro study. Materials (Basel) 2020;13:1744. doi: 10.3390/ma13071744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ellakany P, Tantawi ME, Mahrous AA, Al-Harbi F. Evaluation of the accuracy of digital impressions obtained from intraoral and extraoral dental scanners with different CAD/CAM scanning technologies: An in vitro study. J Prosthodont. 2022;31:314–9. doi: 10.1111/jopr.13400. [DOI] [PubMed] [Google Scholar]
- 17.Oh HS, Lim YJ, Kim B, Kim MJ, Kwon HB, Baek YW. Influence of scanning-aid materials on the accuracy and time efficiency of intraoral scanners for full-arch digital scanning: An in vitro study. Materials (Basel) 2021;14:92340. doi: 10.3390/ma14092340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sallorenzo A, Gómez-Polo M. Comparative study of the accuracy of an implant intraoral scanner and that of a conventional intraoral scanner for complete-arch fixed dental prostheses. J Prosthet Dent. 2022;128:1009–16. doi: 10.1016/j.prosdent.2021.01.032. [DOI] [PubMed] [Google Scholar]
- 19.Gülsoy M, Tuna SH, Pekkan G. Evaluation of median mandibular flexure values in dentulous and edentulous subjects by using an intraoral digital scanner. J Adv Prosthodont. 2022;14:32–44. doi: 10.4047/jap.2022.14.1.32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Romalee W, Kettratad M, Trang TT, Wang DH, Chen JE, Hsu ML. Evaluation of the potential denture covering area in buccal shelf with intraoral scanner. J Dent Sci. 2022;17:1335–41. doi: 10.1016/j.jds.2022.04.010. [DOI] [PMC free article] [PubMed] [Google Scholar]