

Abstract
Background
It is known that SARS-CoV-2 antibodies from pregnant women with SARS-CoV-2 infection during pregnancy cross the placenta but the duration and the protective effect of these antibodies in infants is scarce.
Methods
This prospective study included mothers with SARS-COV-2 infection during pregnancy and their infants from April 2020 to March 2021. IgG antibodies to SARS-CoV-2 spike protein were performed on women and infants at birth and at two and six months during follow-up. Anthropometrical measures and physical and neurological examinations and a clinical history of symptoms and COVID-19 diagnosis were collected. Simple linear regression was performed to compare categorical and continuous variables. To compare the mother’s and infant’s antibody titers evolution, a mixed linear regression model was used. A predictive model of newborn antibody titers at birth has been established by means of simple stepwise linear regression.
Results
51 mother-infant couples were included. 45 (90%) of the mothers and 44 (86.3%) of the newborns had a positive serology al birth. These antibodies were progressively decreasing and were positive in 34 (66.7%) and 7 (13.7%) of infants at 2 and 6 months, respectively. IgG titers of newborns at birth were related to mothers’ titers, with a positive moderate correlation (Pearson’s correlation coefficient: 0.82, p < 0,001). Fetal/maternal antibodies placental transference rate was 1.3 (IQR: 0.7–2.2). The maternal IgG titers at delivery and the type of maternal infection (acute, recent, or past infection) was significantly related with infants’ antibody titers at birth. No other epidemiological or clinical factors were related to antibodies titers. Neurodevelopment, psychomotor development, and growth were normal in 94.2% of infants in the third follow-up visit. No infants had a COVID-19 diagnosis during the follow-up period.
Conclusions
Transplacental transfer of maternal antibodies is high in newborns from mothers with recent or past infection at delivery, but these antibodies decrease after the first months of life. Infant’s IgG titers were related to maternal IgG titers at delivery. Further studies are needed to learn about the protective role of maternal antibodies in infants.
Keywords: Gestational COVID, Neonatal SARS-COV-2 infection, Serological test, Antibodies titers, Antibodies transplacental transfer
Background
The SARS-CoV-2 pandemic has rapidly spread worldwide in the last two years, and today the numbers are as high as more than 200 million confirmed cases and 5 million deaths [1]. During this time, one of the main concerns to health care workers has been special populations such as pregnant women and their infants, due to their high susceptibility to severe infections and the possible outcomes that COVID-19 infection during pregnancy could have in infants.
It is widely known that transplacental acquired antibodies are a key element for the protection of the newborn against infections [2, 3]. It has been demonstrated that SARS-CoV-2 antibodies from pregnant women with SARS-CoV-2 infection during pregnancy cross the placenta, and have been detected in cord blood [4–7]. Nevertheless, it has been suggested that this transfer is lower if the infection occurs close to birth time, and less efficient than expected if compared with other pathogens [8–10]. The duration of these antibodies in infants is a scarcely studied issue with important consequences for newborns, as COVID-19 infection is more severe in neonates than in older children, and especially taking into account that it is unlikely that SARS-CoV-2 vaccines would be approved for young infants in the near future [11]. Small samples indicate that maternal antibodies’ titers rapidly decrease in the first weeks of life, although they may persist in a low proportion of infants at 6 months of life [12–15]. The protective effect that SARS-CoV-2 maternal antibodies could have on infant’s infection has not yet been described.
Data on perinatal outcomes of infants born to mothers with SARS-CoV-2 infection during pregnancy is rising [16]. In the first wave on COVID pandemic, poor neonatal outcomes have been shown, with high rates of cesarean sections, preterm infants, respiratory distress and NICU admission, especially in high-risk population [2, 17–24]. Over time, improved treatment of pregnant women with COVID resulted in decreased cesarean section rates and overall adverse perinatal outcomes [25].
Vertical transmission of SARS-CoV-2 has been demonstrated, usually with low rates and mild or no symptoms [21, 26–30]. Horizontal transmission in the first weeks of life seems to be also low in these infants, with scant clinical manifestations [9, 31].
The main objective of our study was to describe the maternal antibody response to SARS CoV-2 during pregnancy and the transplacental passage of the passive IgG to their newborns and the duration of these antibodies in these infants until 6 months. The secondary aim was to describe if maternal antibodies have a protective effect against neonatal infection.
Methods
We conducted a prospective study at Gregorio Marañón University Hospital, a tertiary hospital in Madrid (Spain). We included mother-infants’ dyads from the Spanish multicenter GESNEO-COVID cohort study. We included the births from April 2020 to March 2021. During the inclusion period, no mother had been vaccinated against SARS-COV-2.
GESNEO-COVID cohort recruited mothers with SARS-COV-2 infection during pregnancy and their infants. Anti SARS-COV-2 IgG antibodies were performed on women and infants at three different moments: at birth (cord or neonatal blood or plasma samples for infants), and at two and six months of the infant’s life. Only couples with all serological samples collected were included in this study.
COVID-19 infection was diagnosed in women if they had either a positive result in a reverse transcription polymerase chain reaction (RT-PCR) done on the nasopharyngeal swab (NPS) during pregnancy or a positive serology at delivery. A screening RT-PCR and SARS-CoV2 IgG antibodies were done for all women admitted to the hospital at delivery.
Data on maternal infection were collected retrospectively from electronic medical records. The date of infection was considered the day of COVID-19 related symptoms onset, or the first positive RT-PCR results in asymptomatic women. Infections in women with a serological diagnosis and who were asymptomatic could not be dated.
Pregnant women were classified according to SARS-COV-2 microbiological test at delivery into 3 groups: acute infection (positive RT-PCR, negative IgG antibodies), recent infection (positive RT-PCR, positive IgG antibodies), and past infection (negative RT-PCR at delivery, with positive RT-PCR during pregnancy and/or positive IgG antibodies at delivery).
Following the recommendations of the Spanish Society of Neonatology and the World Health Organization and according to our center’s protocol, asymptomatic newborns whose mothers had an appropriate clinical condition were rooming-in in obstetrics wards and breastfeeding was promoted [32–34]. A RT-PCR on a NPS was performed on newborns in their first 48 h of life and repeated in the next 24 h only if positive.
Three follow-up visits were performed to infants. The first one at 15 days of life, the second one at two months of life and the third one at six months of life. Anthropometrical measures and physical and neurological examinations were performed by a pediatrician. COVID-19 related symptoms, hospital admissions and RT-PCR tests were recorded. A RT-PCR was performed at the first visit. Serological tests were done in the second and third visits. Serological tests were also performed on mothers in the same study visits. Vaccination of the mothers during the follow up was recorded.
Serological tests in serum samples were performed to detect IgG antibodies against the spike protein of SARS-COV-2. These tests were carried out by using a quantitative chemiluminescent assay (SARS-CoV-2 IgG II Quant Reagent Kit) and an ARCHITECT i2000 instrument (Abbott; Chicago, USA). IgG levels were expressed in AU/mL (arbitrary units per millilitre) and were converted to BAU/mL (binding antibody units per millilitre) using the conversion coefficient provided by the manufacturer (1 BAU = 0.142 X AU) to standardize the results. The linear detection range was from 0 to 5,680 BAU/mL, being results above 7.10 BAU/mL considered positive.
RT-PCR tests on NPS samples were carried out to detect the N gene and the ORF1a1b gene (TaqPath Multiplex, Thermo Fisher®).
Statistical analysis
Continuous variables were presented with median and interquartile ranges (IQR). Categorical variables were presented as total counts and percentages (%). Due to the wide range of values, antibody titers have been expressed by logarithmic scale transformation in base 10 to normalize them.
Transplacental transfer ratio was calculated as infant IgG concentration divided by maternal IgG concentration at birth. Correlations between maternal and neonatal IgG concentrations and between transplacental transfer ratio were reported using the Pearson correlation coefficient (r).
Simple linear regression was performed to compare categorical and continuous variables. A p-value < 0.05 was considered statistically significant. To compare the mother’s and infant’s antibody titers evolution, a mixed linear regression model was used.
A predictive model of newborn antibody titers at birth has been established. The selection of the variables to be introduced in the model was made following clinical and statistical criteria by means of simple stepwise linear regression minimizing Akaike Information Criterion (AIC), Bayes Information Criterion (BIC) and R2-adjusted.
Data were analyzed using StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC and R vs. 4.1.3.
Results
Of 266 women attended with SARS-COV-2 infection during pregnancy or delivery during the study period, 51 mother-infant dyads were included. Demographic and clinical characteristics of mothers and infants are described in Tables 1 and 2 respectively.
Table 1.
Demographic and clinical characteristics of pregnant women
| Pregnant women n = 51 |
|
|---|---|
| Age (years) | 33.8 (29.5–36.4) |
| Ethnicity | |
|
- Caucasian - Latino American - Arabic |
24 (47.1%) 25 (49.0%) 2 (3.9%) |
| Diagnostic test | |
|
- RT-PCR in NF swab - Serological test |
42 (82.4) 9 (17.6%) |
| GA at diagnosis (w) | 35.2 (28.2–38.4) |
| Any comorbidity | 8 (15.7%) |
| Symptomatology | 26 (51.0%) |
| Respiratory symptoms severity* | |
|
- Mild - Moderate - Severe |
9 (64.3%) 5 (35.7%) 0 (0%) |
| Pneumonia COVID-19 | 5 (9.8%) |
| Specific treatment | 4 (7.8%) |
| COVID hospitalization | 5 (9.8%) |
| - ICU admission | 0 (0%) |
| Days of admission | 6 (6–6) |
| RT-PCR + at delivery | 17 (33.3%) |
| Infection classification at delivery | |
|
- Acute infection - Recent infection - Past infection |
5 (9.8%) 12 (23.5%) 34 (66.7%) |
Severity of respiratory infection was stratified into mild (upper respiratory tract symptoms), moderate (pneumonia confirmed by chest X-ray without signs of severity) and severe (presence of hypoxemia with partial oxygen saturation [SatO2] < 90%, acute confusional state, or arterial hypotension)
Continuous variables are described as the median and interquartile range (IQR). Categorical variables as absolute frequencies and percentages
GA: gestational age, ICU: intensive care unit
Table 2.
Demographic and clinical characteristics of infants
| Infants n = 51 |
|
|---|---|
| Sex (male) | 28 (54.9%) |
| GA (w) | 39.6 (38.4–40.3) |
| Prematurity rate | 2 (3.9%) |
| Somatometric characteristics | |
|
- Weight (g) - Length (cm) - Head circumference (cm) |
3300 (3010–3520) 50 (49–51) 34 (33.5–35) |
| Type of delivery | |
|
- Eutocic - Instrumental - Cesarean section |
39 (76.5%) 7 (13.7%) 5 (9.8%) |
| Apgar | |
|
- 1’ - 5’ |
9 (9–9) 10 (10–10) |
| Symptomatology | 5 (9.8%) |
|
- Jaundice - Perinatal asphyxia and HIE - TTNB |
4 (7.8%) 1 (2.0%) 1 (2.0%) |
| Need for NICU admission | 1 (2.0%) |
| Breastfeeding method | |
|
- Maternal - Artificial - Mixed |
32 (62.7%) 3 (5.9%) 16 (31.4%) |
Continuous variables are described as medians and interquartile ranges (IQR). Categorical variables are presented as absolute frequencies and percentages
GA: gestational age, NICU: neonatal intensive care unit, HIE: hypoxic-ischemic encephalopathy, TTNB: transient tachypnea of the newborn
SARS-CoV-2 RT-PCR was performed on 72.6% (37) of newborns in the first 48 h of life, and they were all negative. All infants completed the follow-up visits. No infants had a COVID-19 diagnosis during the follow-up period. 4.3% (2) of the infants had a cohabitant with a COVID-19 diagnosis. One (1.96%) infant needed hospital admission due to a brief resolved unexplained event (BRUE). Neurodevelopment, psychomotor development, and growth were normal in 94.2% of infants in the third follow-up visit. One infant with Down syndrome had psychomotor development retardation at 6 months follow-up, one infant had growth delay and another had mild microcephaly with normal imaging tests.
The first blood analysis was done at a median of 2.1 (IQR 2.0-2.6) months and the second one at a median of 6.1 (IQR: 6-6.5) months. Almost 90% (45) of the mothers had positive IgG antibodies at delivery. At birth, 86.3% (44) of the newborns had positive IgG antibodies in cord or neonatal blood. These results were progressively decreasing, and antibodies were positive in 66.7% (34) and 13.7% (7) of infants at 2 and 6 months, respectively. The evolution of IgG antibody titers in mothers and infants during follow-up is represented in Fig. 1.
Fig. 1.
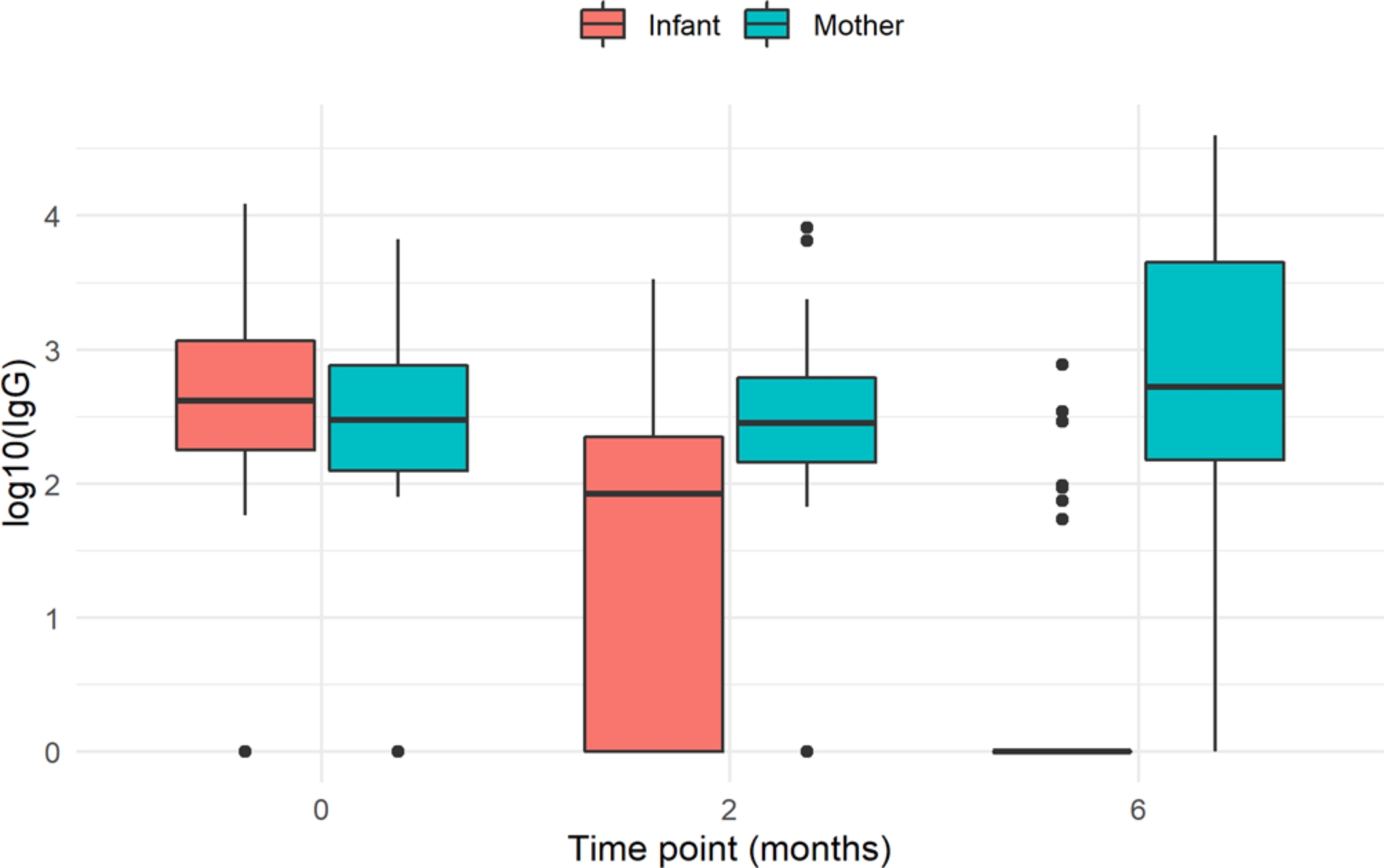
Box-and-whisker plot for log10 IgG values between mothers and newborns
29% (15) of the women received SARS-CoV-2 vaccination between the second and the third follow-up visits. Despite the difference in maternal titers, no difference in titers at 6 months was found in newborns whose mothers had been vaccinated (39.9 AU/mL vs. 19.4 AU/mL, p = 0.596).
IgG titers of newborns at birth were related to mothers’ titers at delivery, with a positive moderate correlation (Pearson’s correlation coefficient: 0.82, CI95% 0.70–0.98, p < 0,001). Fetal/maternal antibodies placental transference rate was 1.3 (IQR: 0.7–2.2). Scatter plots and correlation lines are shown in Fig. 2.
Fig. 2.

Scatter plots and correlation lines. (A) Infants IgG antibodies levels at birth according to maternal IgG antibodies levels. (B) Placental transfer ratio according to maternal IgG antibody levels
At 2 months study visit, infants experienced a 1 unit decrease in log10 IgG antibodies titers compared to their mothers (IC95% -1.4− -0.63, p < 0.001), and at 6 months, a 2.6 decrease (IC95% -2.9― -2.2, p < 0.001).
At delivery, 9.8% (5) of the women had an acute SARS-CoV-2 infection, 23.5% (12) had a recent infection, and 66.7% (34) had a past infection. All the infants born to mothers with acute infection at delivery had negative serologies at birth and during the follow up. There were another two newborns with a negative serology at birth. One of them was a newborn from a mother with recent infection and low antibodies titers at delivery (96 UA/mL), and the other one was a newborn from a mother with an asymptomatic infection at 34 weeks of pregnancy who had not developed antibodies.
The maternal IgG antibodies titers at delivery and type of maternal infection was significantly related in a univariant analysis with infants’ antibody titers at birth. No other epidemiological or clinical factors were related to antibodies titers. These results are shown in Table 3.
Table 3.
Univariate analysis by simple linear regression for log(10) IgG at birth
| Variable | Beta | 95% CI1 | p-value |
|---|---|---|---|
| Maternal age (years) | 0.11 | -0.04, 0,06 | 0.688 |
| Ethnicity | |||
|
Caucasian Latino American Arabic |
— 0.17 0.13 |
— -1.44, 1,78 -0.49, 0.76 |
0.837 0.668 |
| GA at diagnosis (weeks) | 0.00 | -0.00, 0.00 | 0.482 |
| Any comorbidity | 0.33 | -0.50, 1.16 | 0.427 |
| Symptomatology | 0.03 | -0.57, 0.64 | 0.911 |
| Specific treatment | 0.81 | -0.29, 1.92 | 0.147 |
| Hospital admission | 0.84 | -0.16, 1.83 | 0.097 |
| Infection classification at delivery | |||
|
Acute infection Recent infection Past infection |
— 2.51 2.70 |
— 1.73, 3.28 2.00, 3.40 |
< 0.001 < 0.001 |
| Maternal IgG titers at delivery (AU/mL) | 2.71 | 2.18, 3.24 | < 0.001 |
| GA at delivery (weeks) | 0.06 | -0.19, 0.30 | 0.645 |
| Sex (male) | -0.31 | -0.91, 0.30 | 0.312 |
| Type of delivery | |||
|
Eutocic Instrumental Cesarean section |
— -0.90 -0.22 |
— -0.99, 0.81 -1.26, 0.82 |
0.840 0.671 |
| Breastfeeding method | |||
|
Maternal Artificial Mixed |
— -0.74 0.32 |
— -2.03, 0.55 -0.33, 0.96 |
0.255 0.328 |
1CI = Confidence Interval
The best-established model for predicting antibody titers at birth has included the maternal IgG antibodies titers at delivery and the need for hospitalization. The IgG antibodies titers at the birth of the newborns were statistically significantly related in a multiple linear regression to the maternal IgG antibodies titers at delivery. Although maternal hospitalization is not statistically significant, it has been kept in the model because including it improves its fit. The adjusted model with its coefficients and 95%CI is shown in Table 4.
Table 4.
Multivariate linear regression for log10(IgG) of the newborn as a function of the variables selected by statistical criteria at birth
| Variable | Beta | 95% CI1 | p-value |
|---|---|---|---|
| Maternal IgG titers at delivery (AU/mL) | 2.7 | 2.13, 3.18 | < 0.001 |
| Hospital admission | 0.5 | -0.1, 1.1 | 0.09 |
1CI = Confidence Interval
AIC: 72.7, BIC: 77.9, R2 adj: 0,685
Discussion
In our sample, 86.3% of the newborns born to mothers with SARS-CoV-2 infection during pregnancy had positive anti SARS-COV-2 IgG antibodies at birth, and these antibodies progressively declined during the first 6 months of life. The timing of maternal infection was the only factor associated with antibody titers in the infants.
Previous publications analyzing the transplacental transfer of SARS-CoV-2 maternal antibodies described rates of newborns with positive antibodies at birth are similar to ours, varying from 62 to 91% [4, 5, 10]. These variations could be explained by the serological status of the mothers at delivery, which was different in the different studies depending on the inclusion criteria. In our sample, the percentage of infants with positive serologies at birth was as high as 95.6% if the mother had a positive serology at delivery. As previously described, infant’s IgG titers were related to maternal IgG titers [14, 35, 36].
In our sample, the only other factor associated with antibody titers in the newborn was the timing of maternal infection. These data are in concordance with data published by Flannery et al. In their study they analyze 83 pregnant women with positive SARS-CoV-2 serologies (IgG or IgM) and found all cord blood samples had positive IgG if the mother had the infection for more than 17 days prior to delivery [4]. On the contrary, no difference in newborns antibody titers was found if the infection was more or less than 14 days prior to delivery in the study conducted by Joseph et al. [5]. It is to notice that all women in their sample had a positive IgG at delivery, so they wouldn’t be classified as acute infection in our cohort.
We found that newborns from mothers with acute infection at delivery had negative antibodies, as described by Conti. et al. [9]. Mothers with acute infection at delivery had not yet developed an adaptative immune response with IgG antibody production, so these antibodies could not be transferred to their newborns; as these infants did not have a SARS-CoV-2 infection, they did not develop their own antibodies during the follow up. The situation of the newborn with maternal infection in the 34th week of pregnancy who did not present antibodies could be considered as a special case in which the mother did not develop antibodies, or it could also represent a false positive in the diagnostic test of the pregnant woman.
Other factors have been associated with antibody titers, such as maternal symptoms or hospitalization [5]. Nevertheless, and as seen in other cohorts, we have not found this relation [4, 10].
The duration of maternal antibodies in infants has been scarcely studied. Gao et al. described a rapid decline in the first 75 days of life of SARS-CoV-2 IgG titers in 11 infants with positive SARS-CoV-2 serologies at birth [13]. Song et al. also described a decrease in SARS-CoV-2 IgG titers in the first 28 weeks of life in 48 infants with positive SARS-CoV-2 serologies at birth [12]. Also, Capretti et al. found that SARS-CoV-2 IgG level progressively decreased in all infants in their sample, with 97% infants seronegative at 6 months of age [37]. In our sample, of 43 infants with SARS-CoV-2 IgG at delivery, 9 (20.9%) had lost these antibodies at 2 months of life and only 7 (16.2%) maintained them at 6 months of life. This makes it necessary to investigate vaccination strategies for infants above 6 months, when maternal protection is lost, and the risk of infection increases.
In contrast with other studies, in our cohort transplacental transfer of maternal antibodies was appropriate, with a 1.33 ratio [5, 10]. This is significantly higher than previously described for SARS-CoV-2, and similar to the ratio described for other infections such as Bordetella pertussis, influenza or measles, so it could confer adequate protection against SARS-CoV-2 [2, 38, 39].
In our cohort, only 72% of infants were screened with PCR at birth. According to our center’s protocol, all newborns whose mothers have had an acute or recent infection at the time of delivery were screened with PCR at birth. When the mother had had a past infection at some time during pregnancy and was not infected at the time of delivery, it was not necessary to test with PCR on the newborn, and many parents refused to have it performed.
The rate of vertical transmission of SARS-CoV-2 has been reported to be very low in previous studies, as in our cohort, where no vertical-transmitted infections were found [21, 26, 27, 30]. The rates of horizontal transmission have also been reported to be low, and we neither found horizontal SARS-CoV-2 infections during the follow-up, although 5 mothers had an acute infection at delivery and 2 cohabitants also had COVID-19 infection during the follow-up [21, 40, 41]. In addition, these 7 infants were breast-feeding, which could confer additional protection. This supports our hypothesis that maternal antibodies could prevent infection in the newborn.
Cenamo et al. found that even in cases without vertical transmission of SARS-CoV-2 infection, the cord Interferon-γ was significantly lower in cord blood of SARS-CoV-2-positive mothers, suggesting that infection can affect the fetal microenvironment even without severe maternal symptoms [42]. In our study, only SARS-COV-2 IgG antibodies were analyzed and no immunity study was performed on mothers and newborns. It would have been interesting to know the cord levels of Interferon-γ in our infants since none of them subsequently developed infection.
Serologies performed in our study (IgG anti-Spike Protein Receptor Domain antibodies) are detected not only after COVID-19 but also after SARS-CoV-2 vaccination. In Spain, vaccination for pregnant women started in May 2021, so women included in our sample were not vaccinated during pregnancy. 29.4% of women were vaccinated after delivery, between 2 and 6 months-follow-up, so this affected maternal antibody titers in the last visit, which remain high. In our sample, maternal vaccination did not affect newborn antibody titers at the end of follow-up. Maternal antibody titers at delivery and infant’s titers were not biased by vaccination. Although there is some evidence that SARS-CoV2 vaccination during pregnancy provides antibodies in cord blood to infants, if the duration and protection of these antibodies are similar than the provided in natural infection has not been studied [43]. Another important issues to be clarified soon is if infections or vaccination before pregnancy provide protection to infants and if there are differences in these antibodies depending on the SARS-CoV-2 variant.
One of our strengths is that we have included only mother-infants’ dyads with all samples taken and complete follow-up to facilitate the interpretation of the results. The clinical follow-up of infants is another of the strengths of our work, showing that the evolution is normal and that from the point of view of clinical protection we did not find moderate-severe symptomatic COVID infections in the follow-up cohort. Although we have the disadvantage of a single-center study, which affects the external validity of the study, all samples were analyzed in the same laboratory with the same microbiological technique, providing homogeneity to the sample and allowing the evolution of antibody titers over time to be correctly assessed.
One of the weaknesses of our study is that in a few mothers the diagnosis of infection was made by serological test at delivery, so we do not know the exact time of infection during pregnancy. One of the objectives was to know the protective effect of maternal antibodies on SARS-COV-2 infection in infants. Regarding this aim, other limitations are the retrospective nature of the study, the absence of active surveillance of SARS-COV-2 exposure among infants, and the absence of a control group. Although we performed RT-PCR at 15 days of life to infants and asked about COVID-19 related symptoms in the follow-up visits, it is possible that asymptomatic infections could be misdiagnosed.
Another weakness of the study is that there was no measuring of neutralizing activity antibodies. It is well known that neutralizing antibodies are essential for preventing severe disease. A recent study has demonstrated a strong neutralizing and specific maternal IgG response following SARS CoV-2 infection; however, they observed a significant reduction in neutralizing activity between maternal blood and cord blood [5].
Conclusions
In conclusion, transplacental transfer of maternal antibodies is high in newborns from mothers with recent or past infection at delivery, but these antibodies decrease quickly in the first months of life. Infant’s IgG titers were related to maternal IgG titers at delivery. Infants with antibodies may be protected against SARS-COV-2 infection.
Acknowledgements
This study has been addressed on behalf of the GESNEO COHORT WORKING GROUP from Hospital Universitario Gregorio Marañón: David Aguilera, Jesús Saavedra, María del Mar Santos, Arantxa Berzosa, Elena Zamora, Isabel Pescador, Elena Vázquez, Laura Tarancón, María Ángeles Muñoz, Pilar Catalán, Patricia Muñoz, Lara Mesones, Andrea Martínez, Santiago Lizarraga, Juan Antonio León, María Concepción Hernández, Cristina Oliver, María del Mar Muñoz, Francisco Javier Ruiz, César Sánchez. We would like to thank Pablo González Navarro for the statistical analysis supervision. We thank Unidad de Investigación Materno Infantil Fundación Familia Alonso (UDIMIFFA) for its valuable support. We would like to thank the Instituto de Salud Carlos III – Spanish Ministry of Science and Innovation for the financial support. We thank HIV Biobank and microbiology Laboratory from Hospital General Universitario Gregorio Marañón for the sample processing, midwives, and nurses from all participating hospitals for sample collection and patients and their families for their kindness.
List of abbreviations
- AIC
Akaike Information Criterion
- BIC
Bayes information criterion
- AU
Arbitrary units
- BRUE
Brief resolved unexplained event
- CI
Confidence interval
- COVID-19
Coronavirus disease 2019
- HGUGM
Gregorio Marañón University Hospital
- IgG
Immunoglobulin G
- IQR
Interquartile rate
- NICU
Neonatal intensive care unit
- NPS
Nasopharyngeal swab
- RT-PCR
Reverse transcription polymerase chain reaction
- SARS-CoV-2
Severe acute respiratory syndrome coronavirus
Authors’ contributions
SVV, AM, AHL, ICG and MLNG have contributed with the design of the study; SVV, AM, AHL, ICG, CZP, APP and MLNG have collected data; SVV and AM have contributed with the statistical analysis and prepared tables and figures, SVV, AM, AHL, ICG and MLNG interpreted the results, SVV and AM have writing the main manuscript text; AHL, ICG, CZP, APP, EMRL, BSG, MPPR, RAF, MSL and MLNG have reviewed the manuscript and MLNG has given the final approval of the manuscript.
Funding
This study was supported by the Instituto de Salud Carlos III – Spanish Ministry of Science and Innovation (Grant n° COV20/00808).
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
The study was approved by the Clinical Research Ethics Committee of Hospital General Universitario Gregorio Marañón (Code IRB 00006051). Informed consent was obtained from the mothers or legal guardians of the newborns. This study was conducted following WMA Declaration of Helsinki, a statement of ethical principles for medical research involving human subjects. The fundamental rights of the individual will be fully respected, in accordance with the essential rules of Bioethics, Health and Good Practice standards applicable to the study.
Consent for publication
Not appplicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.WHO Coronavirus (COVID-19.) Dashboard | WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. https://covid19.who.int/. Accessed 19 Dec 2021.
- 2.Albrecht M, Pagenkemper M, Wiessner C, Spohn M, Lütgehetmann M, Jacobsen H, et al. Infant immunity against viral infections is advanced by the placenta-dependent vertical transfer of maternal antibodies. Vaccine. 2021 doi: 10.1016/j.vaccine.2020.12.049. [DOI] [PubMed] [Google Scholar]
- 3.Glezen WP. Effect of maternal antibodies on the infant immune response. Vaccine. 2003;21:3389–92. doi: 10.1016/S0264-410X(03)00339-6. [DOI] [PubMed] [Google Scholar]
- 4.Flannery DD, Gouma S, Dhudasia MB, Mukhopadhyay S, Pfeifer MR, Woodford EC, et al. Assessment of maternal and neonatal cord blood SARS-CoV-2 antibodies and placental transfer ratios. JAMA Pediatr. 2021;175:594–600. doi: 10.1001/jamapediatrics.2021.0038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Joseph NT, Dude CM, Verkerke HP, Irby LS, Dunlop AL, Patel RM, et al. Maternal antibody response, neutralizing potency, and placental antibody transfer after severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection. Obstet Gynecol. 2021;138:189–97. doi: 10.1097/AOG.0000000000004440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zambrano H, Anchundia K, Aviles D, Andaluz R, Calderon N, Torres E, et al. Seroprevalence of SARS-CoV-2 immunoglobulins in pregnant women and neonatal cord blood from a highly impacted region. Placenta. 2021;115:146–50. doi: 10.1016/j.placenta.2021.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Garcia-Flores V, Romero R, Xu Y, Theis KR, Arenas-Hernandez M, Miller D et al. Maternal-fetal immune responses in pregnant women infected with SARS-CoV-2. Nat Commun. 2022;13. [DOI] [PMC free article] [PubMed]
- 8.Atyeo C, Pullen KM, Bordt EA, Fischinger S, Burke J, Michell A, et al. Compromised SARS-CoV-2-specific placental antibody transfer. Cell. 2021;184:628–642e10. doi: 10.1016/j.cell.2020.12.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Conti MG, Terreri S, Piano Mortari E, Albano C, Natale F, Boscarino G, et al. Immune response of neonates born to Mothers infected with SARS-CoV-2. JAMA Netw Open. 2021;4:1–14. doi: 10.1001/jamanetworkopen.2021.32563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Edlow AG, Li JZ, Collier ARY, Atyeo C, James KE, Boatin AA, et al. Assessment of maternal and neonatal SARS-CoV-2 viral load, transplacental antibody transfer, and placental Pathology in Pregnancies during the COVID-19 pandemic. JAMA Netw open. 2020;3:e2030455. doi: 10.1001/jamanetworkopen.2020.30455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Liguoro I, Pilotto C, Bonanni M, Ferrari ME, Pusiol A, Nocerino A, et al. SARS-COV-2 infection in children and newborns: a systematic review. Eur J Pediatr. 2020;179:1029–46. doi: 10.1007/s00431-020-03684-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Song D, Prahl M, Gaw SL, Narasimhan SR, Rai DS, Huang A et al. Passive and active immunity in infants born to mothers with SARS-CoV-2 infection during pregnancy: prospective cohort study. BMJ Open. 2021;11. [DOI] [PMC free article] [PubMed]
- 13.Gao J, Li W, Hu X, Wei Y, Wu J, Luo X, et al. Disappearance of SARS-CoV-2 antibodies in infants born to women with COVID-19, Wuhan, China. Emerg Infect Dis. 2020;26:2491–4. doi: 10.3201/eid2610.202328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wang X, Yang P, Zheng J, Liu P, Wei C, Guo J, et al. Dynamic changes of acquired maternal SARS-CoV-2 IgG in infants. Sci Rep. 2021;11:1–7. doi: 10.1038/s41598-021-87535-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rathberger K, Häusler S, Wellmann S, Weigl M, Langhammer F, Bazzano MV, et al. SARS-CoV-2 in pregnancy and possible transfer of immunity: Assessment of peripartal maternal and neonatal antibody levels and a longitudinal follow-up. J Perinat Med. 2021;49:702–8. doi: 10.1515/jpm-2021-0166. [DOI] [PubMed] [Google Scholar]
- 16.Sánchez-Luna M, Colomer BF, de Alba Romero C, Allen AA, Souto AB, Longueira FC et al. Neonates born to mothers with COVID-19: data from the spanish society of neonatology registry. Pediatrics. 2021;147. [DOI] [PubMed]
- 17.Carrasco I, Muñoz-Chapuli M, Vigil-Vázquez S, Aguilera-Alonso D, Hernández C, Sánchez-Sánchez C, et al. SARS-COV-2 infection in pregnant women and newborns in a spanish cohort (GESNEO-COVID) during the first wave. BMC Pregnancy Childbirth. 2021;21:1–10. doi: 10.1186/s12884-021-03784-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Allotey J, Stallings E, Bonet M, Yap M, Chatterjee S, Kew T et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ. 2020;370. [DOI] [PMC free article] [PubMed]
- 19.Villalaín C, Herraiz I, Luczkowiak J, Pérez-Rivilla A, Folgueira MD, Mejía I, et al. Seroprevalence analysis of SARS-CoV-2 in pregnant women along the first pandemic outbreak and perinatal outcome. PLoS ONE. 2020;15:1–12. doi: 10.1371/journal.pone.0243029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Villar J, Ariff S, Gunier RB, Thiruvengadam R, Rauch S, Kholin A, et al. Maternal and neonatal morbidity and mortality among pregnant women with and without COVID-19 infection: the INTERCOVID multinational cohort study. JAMA Pediatr. 2021;175:817–26. doi: 10.1001/jamapediatrics.2021.1050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Angelidou A, Sullivan K, Melvin PR, Shui JE, Goldfarb IT, Bartolome R, et al. Association of maternal Perinatal SARS-CoV-2 infection with neonatal outcomes during the COVID-19 pandemic in Massachusetts. JAMA Netw Open. 2021;4:1–14. doi: 10.1001/jamanetworkopen.2021.7523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zimmermann P, Curtis N. COVID-19 in children, pregnancy and neonates: a review of epidemiologic and clinical features. Pediatr Infect Dis J. 2020;39:469–77. doi: 10.1097/INF.0000000000002700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wróblewska-Seniuk K, Basiukajć A, Wojciechowska D, Telge M, Miechowicz I, Mazela J. Clinical characteristics of newborns born to mothers with covid-19. J Clin Med. 2021;10. [DOI] [PMC free article] [PubMed]
- 24.D’Antonio F, Şen C, Di Mascio D, Galindo A, Villalain C, Herraiz I. Maternal and perinatal outcomes in women with advanced maternal age affected by SARS-CoV-2 infection (Phase-2): the WAPM (World Association of Perinatal Medicine) Working Group on COVID-19. Perinat J. 2021;29:71–8. doi: 10.2399/prn.21.0291011. [DOI] [Google Scholar]
- 25.Sirico A, Carbone L, Avino L, Buonfantino C, De Angelis MC, Cresce M, Di et al. Trends in caesarean section rate according to Robson Group classification among pregnant women with SARS-CoV-2 infection: a single-center large cohort study in Italy. J Clin Med. 2022;11. [DOI] [PMC free article] [PubMed]
- 26.Bwire GM, Njiro BJ, Mwakawanga DL, Sabas D, Sunguya BF. Possible vertical transmission and antibodies against SARS-CoV-2 among infants born to mothers with COVID-19: a living systematic review. J Med Virol. 2021;93:1361–9. doi: 10.1002/jmv.26622. [DOI] [PubMed] [Google Scholar]
- 27.Walker KF, O’Donoghue K, Grace N, Dorling J, Comeau JL, Li W, et al. Maternal transmission of SARS-COV-2 to the neonate, and possible routes for such transmission: a systematic review and critical analysis. BJOG An Int J Obstet Gynaecol. 2020;127:1324–36. doi: 10.1111/1471-0528.16362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tolu LB, Ezeh A, Feyissa GT. Vertical transmission of severe acute respiratory syndrome coronavirus 2: a scoping review. PLoS ONE. 2021;16:1–12. doi: 10.1371/journal.pone.0250196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ghema K, Lehlimi M, Toumi H, Badre A, Chemsi M, Habzi A, et al. Outcomes of newborns to mothers with COVID-19. Infect Dis Now. 2021;51:435–9. doi: 10.1016/j.idnow.2021.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Vigil-Vázquez S, Carrasco-García I, Hernanz-Lobo A, Manzanares Á, Pérez-Pérez A, Toledano-Revenga J, et al. Impact of gestational COVID-19 on neonatal outcomes: is Vertical infection possible? J Bone Jt Surg. 2022;41:466–72. doi: 10.1097/INF.0000000000003518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ayed A, Embaireeg A, Benawadh A, Al-Fouzan W, Hammoud M, Al-Hathal M, et al. Maternal and perinatal characteristics and outcomes of pregnancies complicated with COVID-19 in Kuwait. BMC Pregnancy Childbirth. 2020;20:1–9. doi: 10.1186/s12884-020-03461-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Recommendations for management. of newborns for SARS-CoV-2 infection. 2020.
- 33.WHO EMRO |. Breastfeeding advice during the COVID-19 outbreak | COVID-19 | Nutrition site. http://www.emro.who.int/nutrition/covid-19/breastfeeding-advice-during-the-covid-19-outbreak.html. Accessed 22 Jun 2022.
- 34.Solís-García G, Gutiérrez-Vélez A, Pescador Chamorro I, Zamora-Flores E, Vigil-Vázquez S, Rodríguez-Corrales E, et al. Epidemiology, management and risk of SARS-CoV-2 transmission in a cohort of newborns born to mothers diagnosed with COVID-19 infection. An Pediatr. 2021;94:173–8. doi: 10.1016/j.anpedi.2020.12.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kubiak JM, Murphy EA, Yee J, Cagino KA, Friedlander RL, Glynn SM et al. Severe acute respiratory syndrome coronavirus 2 serology levels in pregnant women and their neonates. 10.1016/j.ajog.2021.01.016 [DOI] [PMC free article] [PubMed]
- 36.Poon LC, Leung BW, Ma T, Yu FNY, Kong CW, Lo TK, et al. Relationship between viral load, infection-to-delivery interval and mother-to-child transfer of anti-SARS-CoV-2 antibodies. Ultrasound Obstet Gynecol. 2021;57:974–8. doi: 10.1002/uog.23639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Capretti MG, Marsico C, Gabrielli L, Vocale C, Arcuri S, Simonazzi G et al. Infants born following SARS-CoV-2 infection in pregnancy. Pediatrics. 2022;150. [DOI] [PubMed]
- 38.Gonçalves G, Cutts FT, Hills M, Rebelo-Andrade H, Trigo FA, Barros H. Transplacental transfer of measles and total IgG. Epidemiol Infect. 1999;122:273–9. doi: 10.1017/S0950268899002046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Heininger U, Riffelmann M, Leineweber B, Wirsing Von Koenig CH. Maternally derived antibodies against bordetella pertussis antigens pertussis toxin and filamentous hemagglutinin in preterm and full term newborns. Pediatr Infect Dis J. 2009;28:443–5. doi: 10.1097/INF.0b013e318193ead7. [DOI] [PubMed] [Google Scholar]
- 40.Yu N, Li W, Kang Q, Xiong Z, Wang S, Lin X, et al. Clinical features and obstetric and neonatal outcomes of pregnant patients with COVID-19 in Wuhan, China: a retrospective, single-centre, descriptive study. Lancet Infect Dis. 2020;20:559–64. doi: 10.1016/S1473-3099(20)30176-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Dumitriu D, Emeruwa UN, Hanft E, Liao GV, Ludwig E, Walzer L, et al. Outcomes of neonates born to mothers with severe Acute Respiratory Syndrome Coronavirus 2 infection at a large Medical Center in New York City. JAMA Pediatr. 2021;175:157–67. doi: 10.1001/jamapediatrics.2020.4298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Cennamo M, La Civita E, Sarno L, Carbone G, Di Somma S, Cabaro S et al. Low Interferon-γ levels in cord and peripheral blood of pregnant women infected with SARS-CoV-2. Microorganisms. 2023;11. [DOI] [PMC free article] [PubMed]
- 43.Beharier O, Mayo RP, Raz T, Sacks KN, Schreiber L, Suissa-Cohen Y et al. Erratum: Efficient maternal to neonatal transfer of antibodies against SARS-CoV-2 and BNT162b2 mRNA COVID-19 vaccine(J Clin Invest. (2021) 131: 13 (e150319) DOI: 10.1172/JCI150319). J Clin Invest. 2021;131. [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.