

Abstract
Introduction and importance
An obturator hernia is a rare cause of bowel obstruction. Due to its narrow passage in the obturator canal, these are more susceptible to becoming incarcerated and subsequently strangulated. Due to its challenging detection, obturator hernia is often diagnosed late.
Case presentation
A 75-year-old thin-built female with COPD presented to the emergency room with symptoms of abdominal obstruction. Abdominal examination revealed distension, firmness, rigidity, and tenderness with no bowel sounds. An erect abdominal X-ray showed multiple air-fluid levels, indicating an acute abdomen due to intestinal obstruction. Emergency exploratory laparotomy revealed an obturator hernia with strangulated ileum and perforation, necessitating resection and double barrel ileostomy. Unfortunately, despite all medical interventions, the patient succumbed to hospital-acquired pneumonia following the surgery.
Discussion
Obturator hernia, known as ‘the skinny old woman hernia,’ is rarely externally visible or palpable, leading to frequent undiagnosed cases. It presents with bowel obstruction or perforation and carries the highest morbidity among abdominal hernias. Timely intervention is crucial to prevent complications like bowel strangulation.
Conclusion
This case report highlights the challenges of diagnosing and managing obturator hernia, a rare condition with significant morbidity. Early detection through imaging or operative findings is crucial to prevent complications like bowel strangulation, especially in older women at higher risk.
Keywords: Case report, Obturator hernia, Intestinal obstruction
Highlights
-
•
Obturator hernia is an uncommon cause of bowel obstruction among elderly.
-
•
Majority of the cases are detected intraoperatively.
-
•
Delayed identification/presentation of obturator hernia increases mortality.
1. Introduction
Obturator hernia (OH) is a rare type of hernia and is the rarest hernia of the pelvic floor which accounts for about 0.07–1 % among all types of abdominal hernia and 0.4 % of bowel obstruction [1]. An obturator hernia occurs when abdominal contents traverse the obturator foramen. As this is a small opening in the pelvis, there is an increased propensity for this hernia to get incarcerated and subsequently strangulated [2].
This is characterized by the protrusion of the hernial sac down from the obturator canal from where the nerve and muscle pass [1]. This hernia generally occurs in the seventh or eighth decades of life in emaciated women at about six times more than the other presenting age group [3]. In this hernia more than 80 % of patients presented with symptoms of bowel obstruction [4]. Due to the difficulty in detecting obturator hernia, it often presents with delayed diagnosis [5].
Here, we present a case of an elderly female who presented with complaints of obstructive symptoms and abdominal pain secondary to an obturator hernia. This case has been written in line with SCARE criteria [6].
2. Case presentation
A 75-year-old female with chronic obstructive pulmonary disease (COPD) and cor pulomonale under medication for several years presented to the emergency room with complaints of not passing stool and flatus, abdominal distension, abdominal pain, and vomiting for three days. She had not undergone any surgery in the past. On examination, she was lean, thin, and ill-looking with a body mass index (BMI) of 15 kg/m2. She was maintaining a saturation of 90 % with 2 l of oxygen with other vitals normal. On abdominal examination, her abdomen was distended, firm, rigid, and tender with the absence of bowel sound.
Inguinal and femoral hernias were not found on light or deep palpation. Rectal examination revealed no frank blood, fissures, or palpable masses. Complete blood count, basic metabolic panel, hepatic function panel, magnesium, phosphorus, prothrombin time, and international normalized ratio (PT-INR) were all within normal limits. An erect X-ray of the abdomen revealed multiple air-fluid levels along with distended bowel loops. With a diagnosis of acute abdomen secondary to intestinal obstruction with features suggestive of perforation peritonitis, the patient was resuscitated with intravenous fluid, and antibiotics and planned for emergency exploratory laparotomy.
Intraoperatively, an obturator hernia with strangulated ileum along with perforation was noted 20 cm away from the ileocecal junction. (Fig. 1) She underwent reduction of obturator hernia with resection of a strangulated segment of the ileum with double barrel ileostomy with the closure of the obturator canal with a round ligament. (Fig. 2, Fig. 3) On postoperative day 2, her abdomen was soft and the ileostomy was functional. However, she developed hospital-acquired pneumonia which progressed to respiratory distress and septic shock ultimately leading to the death of the patient on postoperative day 5.
Fig. 1.
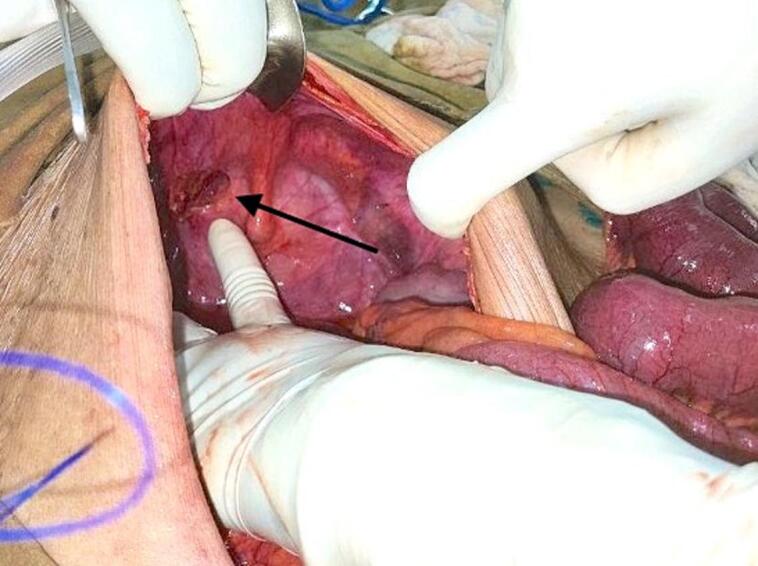
Figure shows the site of the right obturator hernia with the widening of the canal (after the reduction of the hernial contents). (arrow).
Fig. 2.

Figure showing repair of obturator hernia site with the closure of obturator canal after resection of a strangulated segment of ileum.
Fig. 3.

The gross image shown below of the postoperative ileum with a perforated wall. Perforated ileum dimensions measure about 5 mm in length and 5 mm in width.
3. Discussion
An obturator hernia is a rare pelvic hernia and is called ‘the skinny old woman hernia’. This is due to the high incidence of these hernia in women in their seventh or eighth decade, who are normally gaunt, and indeed it can almost be said to be found almost exclusively in women [7,8]. In the study by Park et al., all 11 patients were elderly women, with a mean age of 80.2 years (range, 71–87 years) and mean BMI was 17.9 kg/m2 (range: 11.9–22.2 kg/m2) [9]. The higher incidence of OH among women may be explained by the characteristic shape of the female pelvis, in which the obturator foramen is broader and more obliquely oriented than in men [10]. In addition, loss of pre-peritoneal fat with a decrease in BMI can explain the increased incidence of OH among women with lesser BMI [11]. Moreover, conditions that can increase abdominal pressure such as ascites, chronic obstructive pulmonary disease (COPD), and chronic coughs are the risk factors for developing an obturator hernia [11]. Weakened pelvic floor with multiple pregnancies, older age, and emaciation due to her chronic illness are likely contributing factors for the development of OH in our patient.
The associated clinical symptoms are mostly vague and non-specific with the pathognomonic sign for its diagnosis being the Howship–Romberg sign, which consists of ipsilateral inner thigh pain on internal rotation of the hip [11]. The most common presenting symptom is acute mechanical bowel obstruction, or/and bowel perforation at the time of diagnosis, and is associated with the highest morbidity among all abdominal hernias (13–40 %) [12]. Sometimes the obstruction may be intermittent which can cause intermittent abdominal pain if the hernia content is spontaneously reduced within the peritoneal cavity. Intermittent relief of bowel obstruction may be an important clue for its diagnosis at times [13]. Delayed diagnosis of obturator hernia often leads to strangulation of small bowel which is a typical finding in our case. Hence timely intervention is crucial to get ahead of complications [1]. A high index of suspicion is required in the elderly population, and even then, diagnosis may not be achieved without imaging or operative findings.
As accurate pre-operative diagnosis of obturator hernia is usually difficult, and most patients are operated on as intestinal obstruction of unknown cause [14]. However, CT scan of the abdomen and pelvis has been demonstrated as the most sensitive and specific imaging modality for OH detection with a reported diagnostic accuracy of up to 90 % [11,15].
The preoperative suspicion of bowel strangulation and the potential requirement for an enterectomy primarily determines the choice between an intraperitoneal or extraperitoneal approach [11]. Regardless of the operative approach chosen, the presence of strangulation necessitates resection of the affected bowel segment, the presence of which negatively affects morbidity and mortality rates [16]. Exploratory laparotomy was performed in our case to avoid major complications with resection of perforated ileum and followed by double bowel ileostomy with repair of obturator defect and drain placement.
Mortality from obturator hernias has ranged from 8 % to 47 % in the literature [17]. In a retrospective study performed at a single institution from 2001 to 2010 that reviewed 21 patients with obturator hernias, the overall mortality among patients with OH was as high as 47.6 % [18]. The morbidity of the condition relates to the late presentation and delayed identification of the problem which can lead to infective complications (such as the development of collections) and anastomotic leaks (due to bowel resections) [19]. Advanced age of the patient, perforation peritonitis, and co-existing comorbidities might have resulted in unfavorable outcomes of the patient in our patient that led to septic shock and demise.
4. Conclusion
The presence of an obstruction in thin and old women with obturator hernia is a dire emergency. Obturator hernias, although rare, require a high index of suspicion and care in surgical management as many of these patients will be elderly with a multitude of comorbid conditions.
Ethical approval
Not applicable as ethical approval is not required for writing the case report from the institutional review board in our institute.
Funding
This research work did not receive any kind of funding.
CRediT authorship contribution statement
Pratima Gautam, Prakash Mainali, Dharmesh Shah: Conceptualization, Resources, Supervision, Writing - Review & Editing, Writing - Original Draft.
Suraj Shrestha, Anurag Karki and Ashish Tiwari: Writing - Review & Editing.
The manuscript is reviewed and approved by all the authors.
Guarantor
Dr. Suraj Shrestha.
Registration of research studies
Not applicable.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Declaration of competing interest
None to declare.
Acknowledgments
None.
References
- 1.Kisaoglu A., Ozogul B., Yuce I., Bayramoglu A., Atamanalp S.S. Obturator hernia, a rare cause of small bowel obstruction: case report. Eurasian J Med. 2014;46(3):224–226. doi: 10.5152/eajm.2014.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mnari W., Hmida B., Maatouk M., Zrig A., Golli M. Strangulated obturator hernia: a case report with literature review. Pan Afr Med J. 2019;32:144. doi: 10.11604/pamj.2019.32.144.14846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Uludag M., Yetkin G., Kebudi A., Isgor A., Akgun I., Dönmez A.G. A rare cause of intestinal obstruction: incarcerated femoral hernia, strangulated obturator hernia. Hernia. 2006;10(3):288–291. doi: 10.1007/s10029-006-0074-6. [DOI] [PubMed] [Google Scholar]
- 4.Sorabella R.A., Miniati D.N., Brandt M.L. Laparoscopic obturator hernia repair in an adolescent. J. Pediatr. Surg. 2005;40(12):e39–e41. doi: 10.1016/j.jpedsurg.2005.08.046. [DOI] [PubMed] [Google Scholar]
- 5.Kohga A., Kawabe A., Cao Y., et al. Elective laparoscopic repair after reduction might be useful strategy for incarcerated obturator hernia: a case report. J Surg Case Rep. 2017;2017(9) doi: 10.1093/jscr/rjx180. rjx180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Agha RA, Franchi T, Sohrabi C, Mathew G, Kerwan A, SCARE Group. The SCARE 2020 Guideline: updating consensus surgical CAse REport (SCARE) guidelines. Int. J. Surg. 2020;84:226–230. doi: 10.1016/j.ijsu.2020.10.034. [DOI] [PubMed]
- 7.Chung C.C., Mok C.O., Kwong K.H., Ng E.K., Lau W.Y., Li A.K. Obturator hernia revisited: a review of 12 cases in 7 years. J. R. Coll. Surg. Edinb. 1997;42(2):82–84. https://www.ncbi.nlm.nih.gov/pubmed/9114674 [PubMed] [Google Scholar]
- 8.Mantoo S.K., Mak K., Tan T.J. Obturator hernia: diagnosis and treatment in the modern era. Singap. Med. J. 2009;50(9):866–870. https://www.ncbi.nlm.nih.gov/pubmed/19787172. [PubMed] [Google Scholar]
- 9.Park J. Obturator hernia: clinical analysis of 11 patients and review of the literature. Medicine. 2020;99(34) doi: 10.1097/MD.0000000000021701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Petrie A., Tubbs R.S., Matusz P., Shaffer K., Loukas M. Obturator hernia: anatomy, embryology, diagnosis, and treatment. Clin. Anat. 2011;24(5):562–569. doi: 10.1002/ca.21097. [DOI] [PubMed] [Google Scholar]
- 11.Schizas D., Apostolou K., Hasemaki N., et al. Obturator hernias: a systematic review of the literature. Hernia. 2021;25(1):193–204. doi: 10.1007/s10029-020-02282-8. [DOI] [PubMed] [Google Scholar]
- 12.Yee F.Z.Y., Chok A.Y., Wong T.H. Emergency laparoscopic repair of an incarcerated obturator hernia, a case report. Int. J. Surg. Case Rep. 2020;73:13–14. doi: 10.1016/j.ijscr.2020.06.063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Yip A.W., AhChong A.K., Lam K.H. Obturator hernia: a continuing diagnostic challenge. Surgery. 1993;113(3):266–269. https://www.ncbi.nlm.nih.gov/pubmed/8441961. [PubMed] [Google Scholar]
- 14.Sá N.C., Silva V.C.M., Carreiro P.R.L., Matos Filho A.S., Lombardi I.A. Rare case of incarcerated obturator hernia: case report and review of literature. Int. J. Surg. Case Rep. 2017;37:157–160. doi: 10.1016/j.ijscr.2017.06.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ijiri R., Kanamaru H., Yokoyama H., Shirakawa M., Hashimoto H., Yoshino G. Obturator hernia: the usefulness of computed tomography in diagnosis. Surgery. 1996;119(2):137–140. doi: 10.1016/s0039-6060(96)80160-7. [DOI] [PubMed] [Google Scholar]
- 16.Fevang B.T., Fevang J., Stangeland L., Soreide O., Svanes K., Viste A. Complications and death after surgical treatment of small bowel obstruction: a 35-year institutional experience. Ann. Surg. 2000;231(4):529–537. doi: 10.1097/00000658-200004000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Delgado A., Bhuller S.B., Phan P., Weaver J. Rare case of obturator hernia: surgical anatomy, planning, and considerations. SAGE Open Med Case Rep. 2022;10 doi: 10.1177/2050313X221081371. 2050313X221081371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Chan K.V., Chan C.K.O., Yau K.W., Cheung M.T. Surgical morbidity and mortality in obturator hernia: a 10-year retrospective risk factor evaluation. Hernia. 2014;18(3):387–392. doi: 10.1007/s10029-013-1169-5. [DOI] [PubMed] [Google Scholar]
- 19.Mahendran B., Lopez P.P. StatPearls. StatPearls Publishing; In: 2023. Obturator Hernia. https://www.ncbi.nlm.nih.gov/pubmed/32119416. [PubMed] [Google Scholar]