

Abstract
Purpose:
Language and autism research each typically excludes racially and ethnically minoritized (REM) autistic individuals. In addition, in the case of autistic individuals with language impairment, investigators often approach caregivers to discuss research participation, rather than autistic individuals themselves. This gap limits the ecological validity of language research in autism. To address this gap, this clinical focus article describes strategies for engaging REM autistic young adults with language impairment using lessons learned from 5 years of longitudinal research with this population. This approach involved an ongoing community partnership, as well as participatory partnerships with REM autistic individuals and community stakeholders, consistent with a “slow science” approach.
Conclusions:
The approach yielded excellent retention of participants over 5 years and led to co-development of research projects aimed at priorities described by REM autistic individuals and their families, including understanding self-determination, social determinants of health, and language variability in autistic REM individuals with language impairment. Findings support the utility of community-based methods with autistic REM young adults with language impairment, with key takeaways for diversifying research while replicating, extending, and building theory.
Though autism research infrequently reports participant ethnicity (Pierce et al., 2014), such research largely excludes racially and ethnically minoritized (REM) individuals, who constitute the global majority (Durkin et al., 2015; Rivera-Figueroa et al., 2022; Roux et al., 2015; Steinbrenner et al., 2022; West et al., 2016). Thus, the experiences of autistic REM individuals have been insufficiently represented in the development of diagnostic criteria, assessments, and policies that impact their lives (Buchanan & Wiklund, 2020; National Institutes of Health, 2021). Autism researchers, including self-advocates, have called for removing barriers to participation in research by REM individuals and use of community-based approaches (George et al., 2014; Jones & Mandell, 2020; Maye et al., 2021).
Community-based approaches are congruent with broader arguments for “slow science” or the gradual development of ecologically valid research that promotes reproducibility and development of theory, as well as diversity among researchers and participants (Frith, 2020; Leite & Diele-Viegas, 2021). However, even with community-based approaches, research with REM autistic individuals tends to engage parents and not autistic individuals themselves (DuBay et al., 2018; Ratto et al., 2017; Zamora et al., 2016). These approaches are insufficient for fully understanding the language abilities and experiences of REM autistic individuals varying in language skills and engagement strategies for longitudinal research (Gerhardt & Lainer, 2011; Kuo et al., 2018; Shattuck et al., 2018; Teague et al., 2018; Winter et al., 2018). This clinical focus article provides an illustrative example of a community-based approach to engage REM autistic adolescents and young adults in longitudinal language research.
Systematic Exclusion From Research
The exclusion of autistic REM individuals from research reflects larger sociocultural forces in the research ecosystem (Girolamo, Parker, & Eigsti, 2022). Following the intersectionality theory, REM individuals may have multiple intersecting identities, such as disability and being a minoritized individual, that are each tied to experiences of marginalization and give rise to multiple marginalization that is nuanced, rather than purely additive (Crenshaw, 1989, 1991). The dis/ability studies and critical race theory (DisCrit) centers race and dis/ability as mutually reinforcing social constructs that reflect the reactions of others to individual differences versus individual differences themselves (Annamma et al., 2013, 2018). Though these theories arose from legal and education studies, respectively, they are applicable to clinical research.
Researchers work in an ecosystem that relies on convenience sampling to collect and publish data as quickly and as cheaply as possible in order to meet promotion and tenure guidelines, as well as funding agency expectations (Frith, 2020; Leite & Diele-Viegas, 2021; Wendler et al., 2005). These institutional barriers come at a cost to minoritized individuals. Clinical researchers make assumptions about who is a “good” research participant likely to complete study activities or follow complex instructions; these perceptions may serve to exclude autistic REM individuals prior to recruitment (Joseph & Dohan, 2009). Extending the work of Joseph and Dohan (2009), a “good” research participant is one who taxes the research process the least in terms of time and resources. In general, this might mean a participant who has scheduling flexibility, independent means of transportation, and access to reliable Internet if data collection is remote. In autism research, a “good” research participant might also mean one who examiners perceive as compliant and able to complete standardized protocols. In effect, both convenience sampling and assumptions about the “ideal” research participants can thus contribute to inequitable participation of autistic REM individuals.
Importantly, research design conveys certain values and expectations to participants (DuBay et al., 2018; Lewis & Oyserman, 2016). We note some of the barriers that researchers are responsible for perpetuating, drawing on evidence from research with REM and autistic individuals, respectively, and noting the dearth of evidence on autistic REM individuals. Given that researchers may not know how to better recruit and work with diverse versus primarily White participants (Ellis et al., 2021), we also offer suggestions and useful strategies for future efforts.
Research Sites and Scheduling
One component of research design involves “when” a study takes place; research conducted during bankers' hours may conflict with caregiving, work, or other commitments (Brannon et al., 2013; George et al., 2014). Research often takes place at locations that are less accessible to REM communities (Brannon et al., 2013). For example, a single parent of a REM autistic young adult expressed to the first author that she could not participate in a different university study to access speech-language services for her child because the research took place during working hours and would require over 1 hr of travel on public transportation each way. Sociocultural norms can also influence accessibility. Conducting research in an unfamiliar environment with unfamiliar sociocultural norms, such as in a primarily White academic environment, may place an undue burden on autistic REM individuals and their families (Girolamo et al., 2020).
Fortunately, there are multiple strategies researchers can implement to remove logistical barriers. One such strategy is locating research sites proximally to the neighborhoods of REM autistic individuals and their families (Gowen et al., 2019; Ratto et al., 2017). In some cases, investing in mobile data collection vehicles can enhance accessibility, such as the University of Connecticut's mobile research and outreach unit that contains electroencephalography and eye-tracking devices. If research absolutely cannot take place in community settings, researchers might consider providing transportation, establishing primary or satellite research sites near locations where participants receive other services (e.g., clinics, community centers), and flexible scheduling that allows participants to choose among multiple opportunities and various modalities for completing research activities (Brannon et al., 2013; El-Khorazaty et al., 2007; Ratto et al., 2017). Last, regardless of where research takes place, compensating participants immediately upon completion at an appropriate amount serves to mitigate the time and financial cost participants incur in completing research activities (vs. some other life activity; El-Khorazaty et al., 2007; George et al., 2014; Gowen et al., 2019).
Trust and Community Partnership
A third component of research design entails developing trust and rapport with autistic REM individuals. Researchers should make the effort to establish themselves as a trusted presence in REM communities (Erves et al., 2017), with particular consideration of barriers at the intersection of race and disability (Annamma et al., 2013). For instance, a qualitative study recruitment approach through intermediaries revealed that researchers often failed to meet with adults with intellectual disability prior to enrollment or to ensure research activities were acceptable to individuals with intellectual disability (L. Nicholson et al., 2013). Similarly, a narrative review of assent procedures in behavior-analytic articles (a discipline adjacent to communication sciences and disorders) found that 84% of 226 written reports provided no or minimal details of assent procedures for autistic individuals and individuals with developmental disorders (Morris et al., 2021). One possibility is that participant agency is overlooked in research with autistic individuals, particularly if researchers perceive some autistic individuals to have limited preference by virtue of being ineligible to legally provide informed consent.
Insufficient trust and community partnership from the beginning of research can have cascading effects that exacerbate experiences of marginalization. A meta-analysis of retention strategies in longitudinal studies (Teague et al., 2018) and qualitative studies of Black adults' views on research and underserved populations' research priorities (Erves et al., 2017; Freimuth et al., 2001), respectively, found that minoritized participants commonly believed that clinical research only benefits White people, researchers are dishonest about their research aims, and research staff lack cultural humility. In autism research, Black and Hispanic/Latine families with autistic children report distrust of research as a factor in their decision to not participate (Ratto et al., 2017; Shaia et al., 2020). Some of this distrust may arise from a history of research abuses of the Black community, such as in the case of Henrietta Lacks or Tuskegee airmen (Katz et al., 2006; Skloot, 2010). Some of this distrust may also arise from the systematic exclusion of REM individuals from the research community.
Engaging autistic REM individuals in research may involve building a community partnership and learning about what engagement should look like for each participant; thus, it is not about implementing a universal community-based strategy but about critical thinking. Importantly, though attending to positionality (i.e., where one stands in relation to dynamics of power and privilege) is critical, building community ties may be more important than racial and ethnic concordance for developing trust and rapport with REM communities (El-Khorazaty et al., 2007; Kennedy et al., 2010; Mindlis et al., 2020; Yancey et al., 2006). One way to achieve trust and rapport is by partnering with community leaders or organizations (Erves et al., 2017; Kennedy et al., 2010; Yancey et al., 2006; Zamora et al., 2016). This entails researchers developing a known presence in communities (Erves et al., 2017), treating participants as equals (Kennedy et al., 2010; Lewis & Oyserman, 2016), and letting communities set the tone for interaction norms by letting communities express preferences on how to interact with researchers (Brannon et al., 2013). Community partnership may also include developing advisory boards to advise researchers on study activities or identify community priorities (Brannon et al., 2013; Erves et al., 2017; Haack et al., 2014; Ratto et al., 2017). Personalized recruitment may be especially effective for developing trust with individuals with dis/abilities (Lennox et al., 2005). Other individual strategies that complement community partnership are rolling recruitment, where potential participants can learn about the study and decide later whether to enroll (El-Khorazaty et al., 2007), and dynamic consent, where participants can review their consent over the course of the study (Budin-Ljøsne et al., 2017). In all, these strategies entail centering participants by showing humility and “transparency.”
Communication Practices
Communication practices may also convey to REM individuals that they are welcome or unwelcome in research. Researchers may fail to maintain consistent contact with REM participants or to follow through with promised e-mails, resulting in loss of contact (El-Khorazaty et al., 2007). Implicit cues may also send the message that REM participants are unwelcome. Researchers may fail to use the preferred communication modality of REM participants (Erves et al., 2017), including those with autistic family members (Gowen et al., 2019). For instance, Latine families of autistic children report dissatisfaction with therapists who failed to listen and who spoke to one caregiver rather than including the extended family (DuBay et al., 2018). Similarly, Black and Hispanic/Latine adults (Erves et al., 2017), as well as individuals with intellectual disabilities (L. Nicholson et al., 2013), report that researchers insufficiently explain study activities, with the latter also reporting researchers ignore them in communications. Researchers may fail to use accessible language (Kripalani et al., 2021), share research opportunities with REM individuals (Erves et al., 2017; George et al., 2014), convey the relevance of research to participants, or ensure participants understand their rights (Brannon et al., 2013; Freimuth et al., 2001). These issues all arise from communicative practices of researchers.
Creating effective communication involves cultural responsivity. One strategy is simply to stay in contact throughout research on a regular basis (e.g., weekly or monthly), following up personally, and communicating at the convenience of participants (Brannon et al., 2013; El-Khorazaty et al., 2007; L. M. Nicholson et al., 2011; Yancey et al., 2006; Zamora et al., 2016). Other ways to be culturally responsive to REM families of autistic children is by respecting family perceptions about their child and following their communicative norms (e.g., speaking to and facing the entire family vs. just one caregiver; Ratto et al., 2017; Zamora et al., 2016). In addition, addressing autistic individuals themselves is critical to ensure they are interested in participating in research regardless of whether or not their caregiver is the one providing informed consent (L. Nicholson et al., 2013). Responsive communication could also entail the use of appropriate language register and translation of study materials (Erves et al., 2017; Haack et al., 2014; Kennedy et al., 2010; L. M. Nicholson et al., 2011; Ratto et al., 2017), as well as use of dynamic informed consent and assent (Brannon et al., 2013; George et al., 2014; Gowen et al., 2019). In all, researchers have many opportunities to proactively mitigate communication barriers, thereby increasing the accessibility and inclusivity of language research. Together with other barriers and strategies in research design, there is sufficient evidence for implementing these strategies in research with autistic REM individuals.
Illustrative Research Project Example
We developed a community-based approach in 2015, drawing from prior findings on effective research practices for REM individuals, individuals with dis/abilities, and REM families of autistic children, as well as our own research with autistic individuals and REM individuals varying in developmental profiles. The aim of the broader research project was to characterize the language abilities and transition to adulthood of autistic REM individuals with language impairment (Girolamo & Rice, 2022; Girolamo et al., 2020). This entailed partnering with a community organization serving primarily Black and Hispanic/Latine autistic individuals with language impairment, their families, and community stakeholders to carry out 5 years of longitudinal research from 2018 to 2022 and to develop new directions for research (see Figure 1). This process led to the recruitment of 18 participants, 14 of whom were Black and four of whom were Hispanic/Latine.
Figure 1.
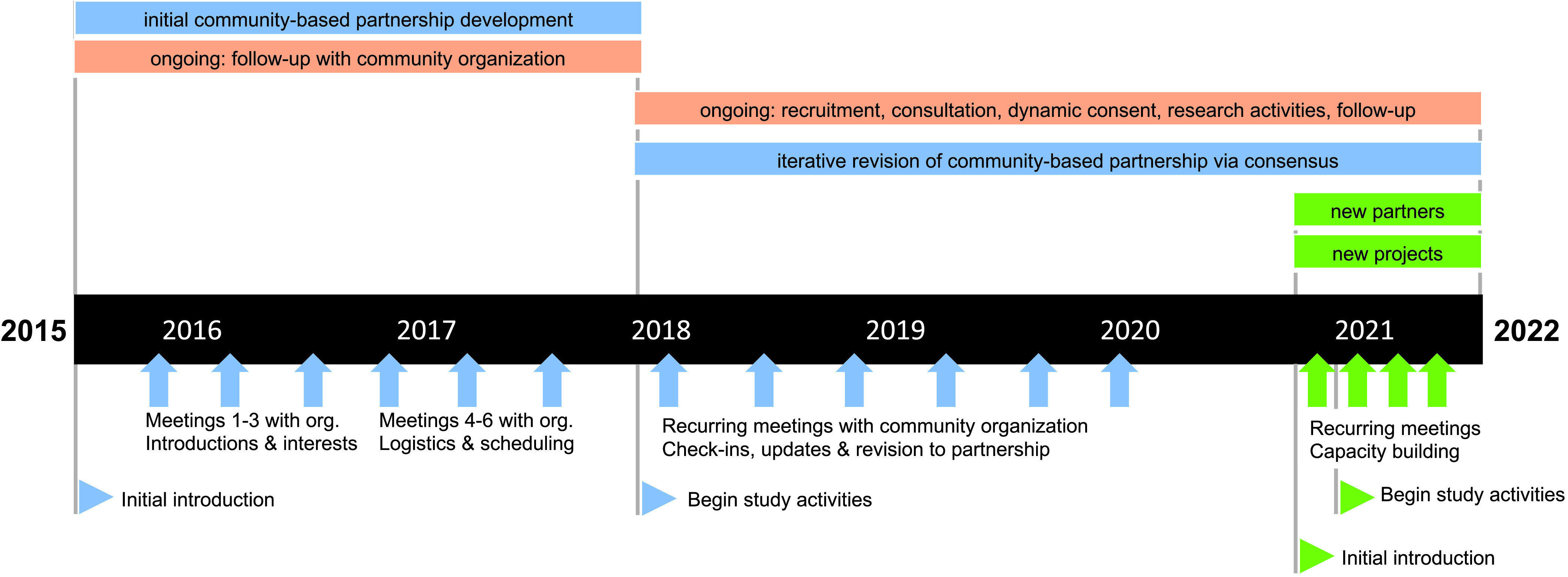
Overview of an illustrative community-based approach. Blue and green indicate individual projects. Orange indicates ongoing activities, with annual assessment per participant. org. = organization.
Developing Trust and Rapport Through Community Partnership
The first author approached a community organization serving primarily REM autistic individuals to partner with them in research. The first author obtained an initial meeting through connections from the REM autism community and established a connection by identifying as a former practitioner (and not an “ivory tower” researcher) with personal ties to REM individuals with developmental disabilities. The approach involved entering the community by being “in community” and showing humility by expressly stating that organizational leadership and staff were experts in their work (vs. implying or believing that a research degree conferred expertise on the lives of the autistic REM individuals they served); this approach facilitated rapport. Most individuals at this organization were Black and/or Hispanic/Latine, with fewer than 10% qualifying as dual language learners. From 2015 to 2018, the first author met multiple times with organizational leadership and staff to discuss study aims and the logistics of study activities. First meetings involved introductions, discussing mutual interests pertaining to outcomes for autistic individuals, and building rapport. A priority for the organization was ensuring that outsiders, such as the first author, understood the work of the organization. Developing trust involved leaving space for the organization to tell the first author who they were and who the individuals they served were, as well as by letting the organization decide when there was sufficient trust (i.e., the organization brought up conducting research). Later meetings involved broad study aims and working out the logistics of recruitment in a way that minimized disruption to organizational programming. Flexibility was key, as the organizational programming could change at a moment's notice. In all, these steps, which took place over 3 years, supported developing a community partnership and led to agreement to begin recruitment in 2018.
Contacting Potential Participants for Initial Recruitment
Per agreement with the organization to minimize disruption to their programming, recruitment entailed distributing and collecting consent-to-contact forms and conducting research off-site in community locations outside of programming hours. At the start of the study in 2018, the first author traveled to the organization, distributed consent-to-contact forms to about 80 autistic adolescents and young adults, and provided a brief explanation of the study in jargon-free language. The organization did not provide contact information, and staff members did not have the burden of distributing or collecting forms. All study materials were in General American English at the average literacy level of adults in the community (i.e., fourth-grade reading level). Potential participants did not have to decide about participation immediately. Rather, individuals were invited to take forms home and discuss with their families before returning the form or contacting the researcher. On the form and in contacting the first author, participants and their families could share their communication preferences (e.g., times during weekdays or weekends; by e-mail, text, or phone) and accessibility needs. These visits to distribute and collect consent-to-contact forms took place early in the morning or later in the afternoon to minimize disruption, with several rescheduled visits due to changes in organizational scheduling or inclement weather. Distributing and collecting these forms over three visits led to the return of 10 forms, with later check-ins leading to an additional three forms.
Providing Personalized Consultation to Potential Participants and Their Families
The first author contacted potential participants and their caregivers to provide a personalized consultation about the study using their preferred communication modality and at their preferred time. The author did not assume any prior research experience or knowledge of research studies, as concepts such as confidentiality and privacy have specific meanings that people outside of research may not know (Girolamo, Castro, et al., 2022). Rather, the author provided a jargon-free study overview, including detailed explanations of consent, assent, and participant rights. Second, the first author sometimes spoke to not only participants and their caregivers but also whoever participants felt was a necessary part of their decision-making process (e.g., some requested the author speak to extended family members and siblings). Throughout consultation, the author encouraged potential participants to ask questions prior to scheduling a time to obtain informed consent and assent. Sample questions pertained to details of study participation, the duration of study activities, and how findings would be used to increase the advocacy base for autistic REM individuals. The first author successfully reached and provided consultation to 11 of 13 (85%) potential participants, all of whom indicated interest in participating. In subsequent years, spontaneous participant referrals led to providing consultation to an additional five enrolled participants.
Obtaining Informed Consent and Assent in a Dynamic Process
The first author implemented a dynamic and interactive informed consent and assent process. When research took place in person, this meant traveling to each participant and their caregiver at a time and place convenient to them in their communities. Participants could select places or tell the first author to provide options within walking distance from their homes. The intention was to allow participants to choose a place that felt accessible to them. The first author sent reminders of meeting times by text or phone, and participants could reschedule at any time. Meetings took place evenings or weekends in community settings (e.g., libraries). The first author explained the informed consent and assent forms line by line using jargon-free language. Using graduated forms adapted from TalkBank (n.d.), participants and caregivers opted what to share of their data and how to share their data (e.g., could elect to share de-identified data or recordings). Participants and caregivers completed checks for understanding and were encouraged to ask questions before providing assent and informed consent. In addition, the first author provided them with copies of the forms and reviewed this information at subsequent time points. If a participant provided consent upon enrolling in the study, they reviewed consents on a yearly basis prior to re-engaging in continued activities and received reminders that they could stop being in the study at any time. This process led to 18 of 18 participants providing informed consent and assent.
Carrying Out Research Activities in Accessible Settings
As with all parts of the study, participants and their caregivers could reschedule at any time. The first author answered questions and concerns on research activities during and after the visit to increase participants' and caregivers' comfort. For example, if a caregiver or participant asked about the purpose of a receptive vocabulary measure, the first author debriefed with them either during or after the task, whichever minimized disruption to the participant. Similarly, if caregivers or participants expressed anxiety about their child's or their own performance, the author listened to their concerns, offered to share a score summary (per institutional review board approval), and reiterated that the only expectation was they try the activities out to the best of their abilities and interests. Upon completion, participants and their caregivers immediately received compensation.
All 18 participants who started assessment completed one or more time points of data assessment. The first two time points of assessment involved an hourlong protocol of age-referenced language and cognitive assessments, with 10 participants assessed at Time 1 and seven participants assessed at Time 2. At Time 2, two participants who had completed assessment at Time 1 were unavailable for assessment but were interested in the study. At Time 3, which coincided with the onset of the COVID-19 pandemic in Spring 2020, 11 participants completed assessment. This necessitated adapting the approach for an online modality. Specifically, online assessment meant leaving space for participants and their caregivers to elect how they were going to participate in the study. For example, one participant who had moved during the pandemic introduced the author to their siblings and extended family members, who each asked questions about the study. This process may have enhanced participation in subsequent time points of data collection, which were also online due to the pandemic, as well as referral of others to this study. By the fifth year of data collection in 2022, five participants participated in their first time point of data collection, four in three time points of data collection, two in four time points of data collection, and seven in their fifth time point of data collection.
Following Up With Participants and Community Partners
Following study visits, the first author remained in contact with participants by sending study communications including a “thank you” card after each session, birthday cards, seasonal greeting cards (including those specific to holidays that participants celebrated), and general greeting cards. These written communications served a dual purpose. First, they ensured that contact information was correct, in that participants were invited to provide updated contact information. Second, these cards provided a friendly, low-stakes way of keeping the study in participants' minds. Furthermore, the first author checked in with participants and their caregivers during the beginning of the COVID-19 pandemic by phone or text. At the same time, the first author also kept in touch by in-person visits, mail, and e-mail with the community organization to check in and revise the partnership as needed. For example, change in the structure of the organization necessitated streamlining communication to minimize burden to the organization.
This strategy led to staying in contact with 16 of 18 participants over the course of 5 years. One participant had contact information that changed, and one stopped responding during the pandemic. However, participants and caregivers typically showed enthusiasm in ways that indicated comfort with the study. One participant sent an unprompted e-mail about their interest in participating in the study and life updates. Caregivers and participants also sent text messages and cards to the first author during the holidays, sharing updates (e.g., experiences with trying to access services). One caregiver shared that although their child typically liked being alone and would disengage from social interactions, the participant reported enjoying the study visits. Others asked detailed questions about the life of the first author (e.g., whether the first author celebrated a given holiday), so that they could be culturally sensitive.
Summary
Though the sample is small, this community approach led to rich interactions with participants and their families. In particular, investing targeted time and effort to partner with a community organization and allowing participants to elect whether, when, and where to complete study activities with transparency throughout the process facilitated sustained trust and rapport. This approach is one illustrative example of a community-based approach to language research when working with autistic REM individuals. In this present case, this approach laid ground for development of ecologically valid research questions and inclusive research methods, congruent with “slow science” (Frith, 2020; Leite & Diele-Viegas, 2021).
New Directions and Lessons Learned
Initially, the research from the community-based approach focused only on individual differences (Girolamo & Rice, 2022), which is consistent with much autism research (Anderson et al., 2018). However, REM autistic and neurodivergent individuals, as well as their family members (e.g., Black parents of young minimally verbal autistic children, who are not part of the neurodiversity self-advocacy space), were highly interested in research with their communities. We describe some of the newly developed areas of research, implemented with new partnerships, as well as lessons learned from this ongoing work (see Figure 1). All activities take place at the time, convenience, and preferred modality of community partners.
New Directions in Research: Social–Ecological Factors
One new line of research arising from the community-based approach aims to holistically characterize social determinants of health in autistic REM individuals with language impairment. A clear finding from the initial study was that assessing only individual difference measures was insufficient for understanding the transition to adulthood in this population. Interactions with participants and their families revealed that environmental factors (i.e., social determinants of health) impacted their responses on individual difference measures, such as a parent sharing that a participant would never socialize on their own independently due to racism and ableism in society, which meant their scores on an adaptive behavior measure were lower due to social–ecological effects instead of individual differences. Thus, we addressed environmental factors.
In attending a community event for REM individuals in the health professions, the first two authors met an REM neurodivergent practitioner. They discussed common interests, as each worked with autistic REM individuals. Over several years, regularly engaging with the practitioner on the practitioner's terms led to a joint decision to build a larger research team to pursue a study examining the role of environmental factors in outcomes that included person-centered measures. This directly supported the practitioner's goal of addressing interests relevant to themselves and their community, as well as the interests of all authors. Research team members included other REM practitioners, autistic and neurodivergent individuals, parents of autistic and neurodivergent children, and established researchers and students who wanted to learn about participatory approaches in clinical research; this included all co-authors of this report. The team set ground rules for inclusion of all perspectives, with the expectation that the most underheard voices would be centered in this work.
Setting ground rules entailed inviting team members to join the project in a graduated procedure: (a) identifying potential team members and meeting with them individually on their terms to talk about conducting research (e.g., at an off-campus location following their preference for modality, whether in person, by Zoom, by phone, or by e-mail); (b) introducing team members to one another; (c) assessing potential for developing trust and rapport with more dominant team members (e.g., White academic researchers) among more minoritized team members (e.g., autistic REM individuals); (d) obtaining agreement from each team member that the team members who research tends to systematically exclude would have priority in terms of meeting agendas, speaking time, and project development; (e) working with more minoritized members to identify ways to remove the burden of conducting research (e.g., going over project development in individual meetings vs. sending a written document for feedback; Teague et al., 2018); and (f) checking in on a monthly basis to gauge the sense of comfort of minoritized team members with the project and fellow team members. Importantly, setting ground rules meant implementing a “zero tolerance” policy for discrimination and disrespect. If at any point a team member does not feel respected or safe, then research will halt until a resolution acceptable to them is reached.
With these rules in place, the team worked collaboratively to identify measures that aimed to recognize the agency of autistic REM individuals with language impairment and their families. This led to identifying validated person-centered measures that were relevant to the experiences of autistic REM individuals and, importantly, that autistic REM individuals from the initial study had shared in years of communication with the first author. Consequently, the research team developed a novel interview support structure to enhance the accessibility in terms of language and cultural sensitivity of the Self-Determination Inventory (Shogren & Wehmeyer, 2017). In an iterative process, research team members identified potential issues with accessibility at the item level, generating a scaffolded interview support structure to allow multiple opportunities for questioning and discussion prior to responding to an item. In this ongoing partnership, autistic and neurodivergent REM individuals (who are not participants) are invited to serve as research partners, with their investment in the project recognized by authorships and roles on funding applications. The objective of this partnership was to share the experiences of autistic REM individuals in a way that did not aim solely to pathologize. We suggest that fully valuing community partners involves including community partners in leadership roles (L. Nicholson et al., 2013).
New Partnerships With Leaders of Geographic and Virtual Communities
In addition to new research, we expanded our partnerships to include community leaders of geographic regions and of virtual communities. Sharing our research to multiple constituents at community events opened new pathways to developing additional community partnerships. First, the Black practitioner from the social determinants of health project coordinated a meeting between the authors and a local community leader with decades of experience in the public schools. The community leader wanted access to resources and supports for Black parents of minimally verbal autistic students, as well as support in applying for grants to obtain resources (e.g., augmentative and alternative communication devices) for these students. The authors provided resources on the terms of the community leader, who then offered to partner in research. Similarly, the practitioner connected the authors with an REM parent of autistic children who is a leader of a large virtual community, which includes a parent support group and programming for parents of autistic children. Again, the authors introduced themselves over time and provided resources on the terms of parent.
We note that while centering the priorities of autistic individuals themselves is critical, in these scenarios, partnering with community leaders and parents was important. This is because autistic REM individuals, such as a minimally verbal 5-year-old autistic child, are extremely unlikely to independently attend a community talk or enter the self-advocacy space (in which autistic REM individuals with language impairment, such as participants in our research, are scarce). Thus, we trusted that family members of autistic REM individuals who knew them best would be able to support autistic REM individuals in communicating what their interest was in research. As for partnering with autistic individuals themselves, speaking about the intersection of race and dis/ability in the health professions led to connecting with an REM autistic self-advocate who co-founded a “for us, by us” autistic self-advocacy organization. As with the first community leader, partnership aligned to mutual interests and areas of expertise. The long-term aim is to implement sustainable partnerships where researcher and community partners are equally valued, as reflected in grants and publications, and bring mutual benefit to communities (Ellis et al., 2021).
Lessons Learned
Both the initial study and subsequent research with new community partners provide examples of how researchers can engage autistic REM individuals in research. Though we recognize that researchers face institutional barriers, amid systemic barriers to engaging autistic REM individuals in research, we offer some lessons learned and a flowchart of possible questions researchers might use to develop community-based approaches (see Figure 2).
Figure 2.
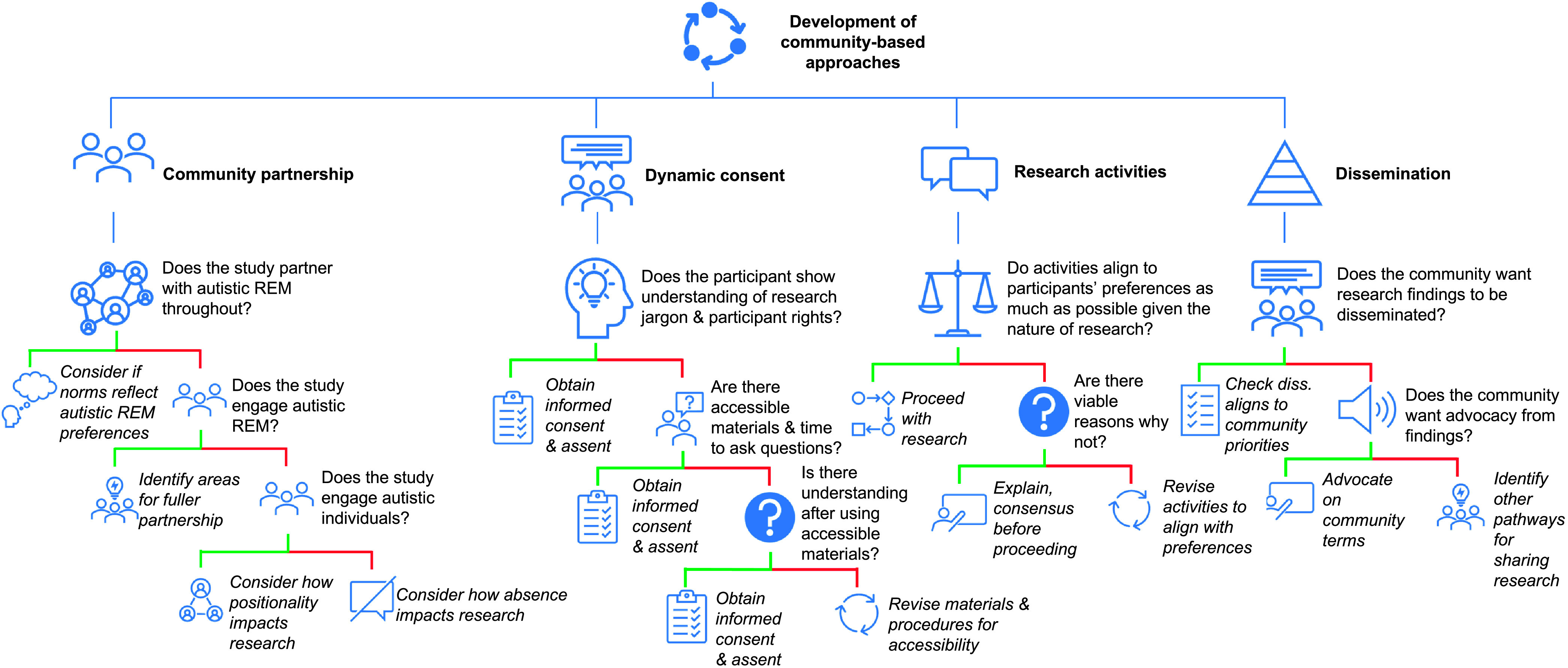
A flowchart for thinking through community-based approaches. diss. = dissemination; REM = racially and ethnically minoritized.
Community Partnership
Overall, researchers must have appropriate expectations for what is feasible in community-based approaches (Frith, 2020; Leite & Diele-Viegas, 2021). Clearly, this research was more labor intensive than convenience sampling and yielded a sample size that is smaller than many researchers may need to satisfy funders. However, regular contact with this sample led to rich information and research that is ecologically valid not just to scientists but also to autistic REM individuals themselves, in terms of how autistic REM individuals see themselves (Buchanan & Wiklund, 2020) and their lived experiences (George et al., 2014; Gowen et al., 2019; Haack et al., 2014). In addition, after developing initial trust and rapport and as trust with the community continued to grow, research was significantly less time and resource intensive.
One question researchers can ask themselves is whether they truly partner with autistic REM individuals on a study from conception through dissemination and whether the norms of the project (e.g., communication frequency and modality) reflect the preferences of autistic REM individuals. If not, then researchers should consider whether the study engages autistic REM individuals and jointly identify areas for fuller partnership, following the goals and priorities of autistic REM individuals. If researchers do not engage autistic REM individuals, they could engage autistic individuals who are White and consider how missing the perspective of autistic REM individuals on the research team affects their research. Similarly, researchers can also ask themselves how not engaging autistic individuals impacts their science.
Be a Good Research Partner
A second broad lesson learned is the importance of being a good research partner. This involves ensuring that the spirit of community partnership, which depends on cultural humility (Erves et al., 2017; Freimuth et al., 2001; George et al., 2014), continues throughout a research study, from dynamic consent to research activities and dissemination.
Dynamic consent
If scientists invest the appropriate time and energy to get to know their participants, communication preferences, and accessibility profiles, scientists can implement dynamic consent and assent. In this process, it is critical to consider how to know autistic REM individuals will show understanding of research jargon pertaining to consent, assent, and participant rights. Relevant questions are whether there are consent and assent materials accessible at an individual level, as well as time built into recruitment for participants to ask questions. Researchers should be proactively mindful of cultural norms. For instance, if a participant and their family are of a culture unlikely to ask questions, regardless of level of understanding, preparing a priori questions about what consent is and is not could be useful. Next, a researcher should consider whether a participant shows understanding “after” implementing consent materials and processes accessible to them. If not, then researchers should revise materials and procedures, ideally with autistic REM community partners.
Research activities
A second domain for being a good research partner is research activities. Researchers must consider whether activities align to the preferences and priorities of autistic REM individuals as much as possible while also considering the requirements of the research. For instance, some participants indicated they largely preferred meeting in person during the COVID-19 pandemic. Clearly, that was not possible. In such cases, researchers should consider whether there are justifiable reasons for not following participant preferences and transparently explain that reasoning to participants. In our case, transparency allowed for reaching consensus on the modality of research activities. However, if, for example, a participant prefers to complete research activities at a place accessible to them and there is no reason for research activities to take place at a fixed location, then researchers should revise activities to provide maximum flexibility and accessibility to participants.
Dissemination
A third area that is critical for community partnership is ensuring research findings are impactful for autistic REM individuals themselves. To start, researchers must ask whether communities want research findings to be broadly disseminated and, if so, what their priorities are for dissemination. If not, researchers might ask whether the community wants some type of advocacy from findings and then advocate following the terms of the community. In our case, autistic REM individuals on the research team, community stakeholders, participants, and their families felt strongly about the experiences, abilities, and perspectives of people like them having a seat at the table. This meant not only sharing the empirical findings but also “advocating” for implementation of community-based strategies as scientifically rigorous and “translating” this appreciation into engagement strategies. For example, knowing that one participant was proud of being in the study and a role model for their nieces, the first author scheduled time at each assessment session to speak with their nieces about the study with family permission (though they were not part of this study). In addition, it was important for the authors to be highly responsive to requests from community partners for resources or assistance to support autistic REM individuals. An example of this was finding resources for autistic REM individuals to support their young adulthood goals, as well as co-developing research projects with autistic REM individuals. These methods likely supported retention, consistent with prior work with families of autistic REM individuals (Zamora et al., 2016).
Mitigate Biases
Of course, an underlying lesson from this research is that all researchers in communication sciences and disorders have the responsibility of co-constructing an accurate narrative of REM engagement in research and practice with REM individuals and other stakeholders in their lives. That is, researchers must deconstruct the narrative that REM individuals are less willing than White counterparts to participate in research through actions (Wendler et al., 2005). Scientists should critically examine how their own judgments of who is a “good” research participant can lead to research designs that exclude autistic REM individuals (Joseph & Dohan, 2009; Zamora et al., 2016). Acting upon this bias could mean working with community partners to build inclusive research methods that leverage community strengths, such as conducting health research that supports community priorities on the weekend at community events such as farmers markets (Lewis & Oyserman, 2016).
Conclusions
In developing a multiyear community approach to longitudinal language research with autistic REM individuals with language impairment when approaching autistic individuals themselves, we generated new research directions and partnerships. Working with community partners underlined the importance of identifying barriers preventing autistic REM individuals with language impairment from achieving their goals, as well as developing person-centered measures that yield valid results by being culturally sensitive to autistic REM individuals. The new directions for research from this approach have strong implications for building meaningful research. It is our hope that the methods and lessons learned are useful to others endeavoring to do this type of research.
Author Contributions
Teresa Girolamo: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Supervision, Visualization, Writing – original draft. Samantha Ghali: Conceptualization, Methodology, Writing – original draft. Inge-Marie Eigsti: Funding acquisition, Writing – review & editing.
Data Availability Statement
All data are reported and available in the article.
Acknowledgments
Teresa Girolamo was supported by a University of Kansas Research Excellence Initiative Grant. Samantha Ghali and Inge-Marie Eigsti were supported by National Institute on Deafness and Other Communication Disorders Grant T32DC017703. Inge-Marie Eigsti was supported by National Institute on Deafness and Other Communication Disorders Grant R01MH112678. Samantha Ghali was supported by National Institute on Deafness and Other Communication Disorders Grant T32DC000052. The authors thank Audra Sterling for providing feedback on an earlier version of this clinical focus article.
Funding Statement
Teresa Girolamo was supported by a University of Kansas Research Excellence Initiative Grant. Samantha Ghali and Inge-Marie Eigsti were supported by National Institute on Deafness and Other Communication Disorders Grant T32DC017703. Inge-Marie Eigsti was supported by National Institute on Deafness and Other Communication Disorders Grant R01MH112678. Samantha Ghali was supported by National Institute on Deafness and Other Communication Disorders Grant T32DC000052.
References
- Anderson, K. A. , Roux, A. M. , Kuo, A. , & Shattuck, P. T. (2018). Social–ecological correlates in adult autism outcome studies: A scoping review. Pediatrics, 141(Suppl. 4), S306–S317. 10.1542/peds.2016-4300H [DOI] [PubMed] [Google Scholar]
- Annamma, S. A. , Connor, D. , & Ferri, B. (2013). Dis/ability critical race studies (DisCrit): Theorizing at the intersections of race and dis/ability. Race Ethnicity and Education, 16(1), 1–31. 10.1080/13613324.2012.730511 [DOI] [Google Scholar]
- Annamma, S. A. , Ferri, B. A. , & Connor, D. J. (2018). Disability critical race theory: Exploring the intersectional lineage, emergence, and potential futures of DisCrit in education. Review of Research in Education, 42(1), 46–71. 10.3102/0091732X18759041 [DOI] [Google Scholar]
- Brannon, E. E. , Kuhl, E. S. , Boles, R. E. , Aylward, B. S. , Benoit Ratcliff, M. , Valenzuela, J. M. , Johnson, S. L. , & Powers, S. W. (2013). Strategies for recruitment and retention of families from low-income, ethnic minority backgrounds in a longitudinal study of caregiver feeding and child weight. Children's Health Care, 42(3), 198–213. 10.1080/02739615.2013.816590 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buchanan, N. T. , & Wiklund, L. O. (2020). Why clinical science must change or die: Integrating intersectionality and social justice. Women & Therapy, 43(3–4), 309–329. 10.1080/02703149.2020.1729470 [DOI] [Google Scholar]
- Budin-Ljøsne, I. , Teare, H. J. , Kaye, J. , Beck, S. , Bentzen, H. B. , Caenazzo, L. , Collett, C. , D'Abramo, F. , Felzmann, H. , & Finlay, T. (2017). Dynamic consent: A potential solution to some of the challenges of modern biomedical research. BMC Medical Ethics, 18(1), 1–10. 10.1186/s12910-016-0162-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crenshaw, K. (1989). Demarginalizing the intersection of race and sex: A Black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. University of Chicago Legal Forum, 140, 25–42. https://chicagounbound.uchicago.edu/uclf/vol1989/iss1/8 [Google Scholar]
- Crenshaw, K. (1991). Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanford Law Review, 43(6), 1241–1499. 10.2307/1229039 [DOI] [Google Scholar]
- DuBay, M. , Watson, L. R. , & Zhang, W. (2018). In search of culturally appropriate autism interventions: Perspectives of Latino caregivers. Journal of Autism and Developmental Disorders, 48(5), 1623–1639. 10.1007/s10803-017-3394-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Durkin, M. S. , Elsabbagh, M. , Barbaro, J. , Gladstone, M. , Happe, F. , Hoekstra, R. A. , Lee, L. C. , Rattazzi, A. , Stapel-Wax, J. , & Stone, W. L. (2015). Autism screening and diagnosis in low resource settings: Challenges and opportunities to enhance research and services worldwide. Autism Research, 8(5), 473–476. 10.1002/aur.1575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- El-Khorazaty, M. N. , Johnson, A. A. , Kiely, M. , El-Mohandes, A. A. , Subramanian, S. , Laryea, H. A. , Murray, K. B. , Thornberry, J. S. , & Joseph, J. G. (2007). Recruitment and retention of low-income minority women in a behavioral intervention to reduce smoking, depression, and intimate partner violence during pregnancy. BMC Public Health, 7(1), 1–18. 10.1186/1471-2458-7-233 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellis, C. , Jacobs, M. , & Kendall, D. (2021). The impact of racism, power, privilege, and positionality on communication sciences and disorders research: Time to reconceptualize and seek a pathway to equity. American Journal of Speech-Language Pathology, 30(5), 2032–2039. 10.1044/2021_AJSLP-20-00346 [DOI] [PubMed] [Google Scholar]
- Erves, J. C. , Mayo-Gamble, T. L. , Malin-Fair, A. , Boyer, A. , Joosten, Y. , Vaughn, Y. C. , Sherden, L. , Luther, P. , Miller, S. , & Wilkins, C. H. (2017). Needs, priorities, and recommendations for engaging underrepresented populations in clinical research: A community perspective. Journal of Community Health, 42(3), 472–480. 10.1007/s10900-016-0279-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freimuth, V. S. , Quinn, S. C. , Thomas, S. B. , Cole, G. , Zook, E. , & Duncan, T. (2001). African Americans' views on research and the Tuskegee Syphilis Study. Social Science & Medicine, 52(5), 797–808. 10.1016/S0277-9536(00)00178-7 [DOI] [PubMed] [Google Scholar]
- Frith, U. (2020). Fast lane to slow science. Trends in Cognitive Sciences, 24(1), 1–2. 10.1016/j.tics.2019.10.007 [DOI] [PubMed] [Google Scholar]
- George, S. , Duran, N. , & Norris, K. (2014). A systematic review of barriers and facilitators to minority research participation among African Americans, Latinos, Asian Americans, and Pacific Islanders. American Journal of Public Health, 104(2), e16–e31. 10.2105/AJPH.2013.301706 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gerhardt, P. F. , & Lainer, I. (2011). Addressing the needs of adolescents and adults with autism: A crisis on the horizon. Journal of Contemporary Psychotherapy, 41(1), 37–45. 10.1007/s10879-010-9160-2 [DOI] [Google Scholar]
- Girolamo, T. , Castro, N. , Hendricks, A. E. , Ghali, S. , & Eigsti, I. M. (2022). Implementation of open science practices in communication sciences and disorders research with Black, indigenous, and people of color. Journal of Speech, Language, and Hearing Research. Advance online publication. 10.1044/2022_JSLHR-22-00272 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Girolamo, T. , Parker, T. C. , & Eigsti, I. M. (2022). Incorporating dis/ability studies and critical race theory to combat systematic exclusion of Black, Indigenous, and people of color in clinical neuroscience. Frontiers of Neuroscience, 16. 10.3389/fnins.2022.988092 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Girolamo, T. , & Rice, M. L. (2022). Language impairment in autistic adolescents and young adults. Journal of Speech, Language, and Hearing Research, 65(9), 3518–3530. 10.1044/2022_JSLHR-21-00517 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Girolamo, T. , Rice, M. L. , & Warren, S. F. (2020). Assessment of language abilities in minority adolescents and young adults with autism spectrum disorder and extensive special education needs: A pilot study. American Journal of Speech-Language Pathology, 29(2), 804–818. 10.1044/2020_AJSLP-19-00036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gowen, E. , Taylor, R. , Bleazard, T. , Greenstein, A. , Baimbridge, P. , & Poole, D. (2019). Guidelines for conducting research studies with the autism community. Autism Policy & Practice, 2(1), 29–45. [PMC free article] [PubMed] [Google Scholar]
- Haack, L. M. , Gerdes, A. C. , & Lawton, K. E. (2014). Conducting research with Latino families: Examination of strategies to improve recruitment, retention, and satisfaction with an at-risk and underserved population. Journal of Child and Family Studies, 23(2), 410–421. 10.1007/s10826-012-9689-7 [DOI] [Google Scholar]
- Jones, D. R. , & Mandell, D. S. (2020). To address racial disparities in autism research, we must think globally, act locally. Autism, 24(7), 1587–1589. 10.1177/1362361320948313 [DOI] [PubMed] [Google Scholar]
- Joseph, G. , & Dohan, D. (2009). Diversity of participants in clinical trials in an academic medical center: The role of the ‘good study patient?’ Cancer, 115(3), 608–615. 10.1002/cncr.24028 [DOI] [PubMed] [Google Scholar]
- Katz, R. V. , Russell, S. L. , Kegeles, S. S. , Kressin, N. R. , Green, B. L. , Wang, M. Q. , James, S. A. , & Claudio, C. (2006). The Tuskegee Legacy Project: Willingness of minorities to participate in biomedical research. Journal of Health Care for the Poor and Underserved, 17(4), 698–715. 10.1353/hpu.2006.0126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kennedy, B. M. , Kumanyika, S. , Ard, J. D. , Reams, P. , Johnson, C. A. , Karanja, N. , Charleston, J. B. , Appel, L. J. , Maurice, V. , & Harsha, D. W. (2010). Overall and minority-focused recruitment strategies in the PREMIER multicenter trial of lifestyle interventions for blood pressure control. Contemporary Clinical Trials, 31(1), 49–54. 10.1016/j.cct.2009.10.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kripalani, S. , Goggins, K. , Couey, C. , Yeh, V. M. , Donato, K. M. , Schnelle, J. F. , Wallston, K. A. , Bell, S. P. , Harrell, F. E., Jr. , & Mixon, A. S. (2021). Disparities in research participation by level of health literacy. Mayo Clinic Proceedings, 96(2), 314–321. 10.1016/j.mayocp.2020.06.058 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuo, A. A. , Crapnell, T. , Lau, L. , Anderson, K. A. , & Shattuck, P. (2018). Stakeholder perspectives on research and practice in autism and transition. Pediatrics, 141(Suppl. 4), S293–S299. 10.1542/peds.2016-4300F [DOI] [PubMed] [Google Scholar]
- Leite, L. , & Diele-Viegas, L. M. (2021). Juggling slow and fast science. Nature Human Behaviour, 5(4), 409–409. 10.1038/s41562-021-01080-1 [DOI] [PubMed] [Google Scholar]
- Lennox, N. , Taylor, M. , Rey-Conde, T. , Bain, C. , Purdie, D. M. , & Boyle, F. (2005). Beating the barriers: Recruitment of people with intellectual disability to participate in research. Journal of Intellectual Disability Research, 49(4), 296–305. 10.1111/j.1365-2788.2005.00618.x [DOI] [PubMed] [Google Scholar]
- Lewis, N. A., Jr. , & Oyserman, D. (2016). Using identity-based motivation to improve the nation's health without breaking the bank. Behavioral Science & Policy, 2(2), 24–38. 10.1353/bsp.2016.0013 [DOI] [Google Scholar]
- Maye, M. , Boyd, B. A. , Martínez-Pedraza, F. , Halladay, A. , Thurm, A. , & Mandell, D. S. (2021). Biases, barriers, and possible solutions: Steps towards addressing autism researchers under-engagement with racially, ethnically, and socioeconomically diverse communities. Journal of Autism and Developmental Disorders, 52(9), 4206–4211. 10.1007/s10803-021-05250-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mindlis, I. , Livert, D. , Federman, A. D. , Wisnivesky, J. P. , & Revenson, T. A. (2020). Racial/ethnic concordance between patients and researchers as a predictor of study attrition. Social Science & Medicine, 255, 113009. 10.1016/j.socscimed.2020.113009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morris, C. , Detrick, J. J. , & Peterson, S. M. (2021). Participant assent in behavior analytic research: Considerations for participants with autism and developmental disabilities. Journal of Applied Behavior Analysis, 54(4), 1300–1316. 10.1002/jaba.859 [DOI] [PubMed] [Google Scholar]
- National Institutes of Health. (2021). NIH-wide strategic plan for fiscal years 2021–2025. U.S. Department of Human Health Services. https://www.nih.gov/about-nih/nih-wide-strategic-plan [Google Scholar]
- Nicholson, L. , Colyer, M. , & Cooper, S. A. (2013). Recruitment to intellectual disability research: A qualitative study. Journal of Intellectual Disability Research, 57(7), 647–656. 10.1111/j.1365-2788.2012.01573.x [DOI] [PubMed] [Google Scholar]
- Nicholson, L. M. , Schwirian, P. M. , Klein, E. G. , Skybo, T. , Murray-Johnson, L. , Eneli, I. , Boettner, B. , French, G. M. , & Groner, J. A. (2011). Recruitment and retention strategies in longitudinal clinical studies with low-income populations. Contemporary Clinical Trials, 32(3), 353–362. 10.1016/j.cct.2011.01.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pierce, N. P. , O'Reilly, M. F. , Sorrells, A. M. , Fragale, C. L. , White, P. J. , Aguilar, J. M. , & Cole, H. A. (2014). Ethnicity reporting practices for empirical research in three autism-related journals. Journal of Autism and Developmental Disorders, 44(7), 1507–1519. 10.1007/s10803-014-2041-x [DOI] [PubMed] [Google Scholar]
- Ratto, A. B. , Anthony, B. J. , Pugliese, C. , Mendez, R. , Safer-Lichtenstein, J. , Dudley, K. M. , Kahn, N. F. , Kenworthy, L. , Biel, M. , & Martucci, J. L. (2017). Lessons learned: Engaging culturally diverse families in neurodevelopmental disorders intervention research. Autism, 21(5), 622–634. 10.1177/1362361316650394 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rivera-Figueroa, K. , Marfo, N. Y. A. , & Eigsti, I.-M. (2022). Parental perceptions of autism spectrum disorder in Latinx and Black sociocultural contexts: A systematic review. American Journal on Intellectual and Developmental Disabilities, 127(1), 42–63. 10.1352/1944-7558-127.1.42 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roux, A. M. , Shattuck, P. T. , Rast, J. E. , Rava, J. A. , & Anderson, K. A. (2015). National autism indicators report: Transition into young adulthood. Life Course Outcomes Research Program, A. J. Drexel Autism Institute, Drexel University. [Google Scholar]
- Shaia, W. E. , Nichols, H. M. , Dababnah, S. , Campion, K. , & Garbarino, N. (2020). Brief report: Participation of Black and African-American families in autism research. Journal of Autism and Developmental Disorders, 50(5), 1841–1846. 10.1007/s10803-019-03926-0 [DOI] [PubMed] [Google Scholar]
- Shattuck, P. T. , Lau, L. , Anderson, K. A. , & Kuo, A. A. (2018). A national research agenda for the transition of youth with autism. Pediatrics, 141(Suppl. 4), S355–S361. 10.1542/peds.2016-4300M [DOI] [PubMed] [Google Scholar]
- Shogren, K. A. , & Wehmeyer, M. L. (2017). Self-determination inventory. Kansas University Center on Developmental Disabilities. [Google Scholar]
- Skloot, R. (2010). The immortal life of Henrietta Lacks. Crown. [Google Scholar]
- Steinbrenner, J. R. , McIntyre, N. , Rentschler, L. F. , Pearson, J. N. , Luelmo, P. , Jaramillo, M. E. , Boyd, B. A. , Wong, C. , Nowell, S. W. , Odom, S. L. , & Hume, K. A. (2022). Patterns in reporting and participant inclusion related to race and ethnicity in autism intervention literature: Data from a large-scale systematic review of evidence-based practices. Autism, 26(8), 2026–2040. 10.1177/13623613211072593 [DOI] [PMC free article] [PubMed] [Google Scholar]
- TalkBank. (n.d.). Graduated consent form. https://talkbank.org/share/irb/consent-UMD.docx
- Teague, S. , Youssef, G. J. , Macdonald, J. A. , Sciberras, E. , Shatte, A. , Fuller-Tyszkiewicz, M. , Greenwood, C. , McIntosh, J. , Olsson, C. A. , & Hutchinson, D. (2018). Retention strategies in longitudinal cohort studies: A systematic review and meta-analysis. BMC Medical Research Methodology, 18(1), 1–22. 10.1186/s12874-018-0586-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wendler, D. , Kington, R. , Madans, J. , Van Wye, G. , Christ-Schmidt, H. , Pratt, L. A. , Brawley, O. W. , Gross, C. P. , & Emanuel, E. (2005). Are racial and ethnic minorities less willing to participate in health research? PLOS Medicine, 3(2), Article e19. 10.1371/journal.pmed.0030019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- West, E. A. , Travers, J. C. , Kemper, T. D. , Liberty, L. M. , Cote, D. L. , McCollow, M. M. , & Stansberry Brusnahan, L. L. (2016). Racial and ethnic diversity of participants in research supporting evidence-based practices for learners with autism spectrum disorder. The Journal of Special Education, 50(3), 151–163. 10.1177/0022466916632495 [DOI] [Google Scholar]
- Winter, S. S. , Page-Reeves, J. M. , Page, K. A. , Haozous, E. , Solares, A. , Cordova, C. N. , & Larson, R. S. (2018). Inclusion of special populations in clinical research: Important considerations and guidelines. Journal of Clinical and Translational Research, 4(1), 56–69. 10.18053/jctres.04.201801.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yancey, A. K. , Ortega, A. N. , & Kumanyika, S. K. (2006). Effective recruitment and retention of minority research participants. Annual Review of Public Health, 27(1), 1–28. 10.1146/annurev.publhealth.27.021405.102113 [DOI] [PubMed] [Google Scholar]
- Zamora, I. , Williams, M. E. , Higareda, M. , Wheeler, B. Y. , & Levitt, P. (2016). Brief report: Recruitment and retention of minority children for autism research. Journal of Autism and Developmental Disorders, 46(2), 698–703. 10.1007/s10803-015-2603-6 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data are reported and available in the article.