

Abstract
Introduction:
The Boston Scientific Swiss LithoClast® Trilogy lithotripter was intended for use in percutaneous nephrolithotomy. We performed, to our knowledge, the first two robotic pyelolithotomies using the Trilogy lithotripter for intracorporeal lithotripsy.
Case Description:
Two cases are presented involving a 65-year-old female with a complete left staghorn calculus and hydronephrosis secondary to a left ureteropelvic junction (UPJ) obstruction, and a 69-year-old male with a large left staghorn calculus and multiple large left sided simple renal cysts. In both cases, a robotic pyelolithotomy was scheduled for stone removal along with concurrent UPJ repair and cyst decortication respectively. Following pyeloplasty and cyst decortication respectively, and following stone visualization, the 2.4-mm Trilogy probe was inserted into the 12-mm assistant port and under direct visualization the stone was fragmented and removed using Trilogy’s built-in mechanisms. Both patients were treated successfully without complications and were found to be stone-free on follow-up.
Conclusion:
The Trilogy lithotripter may be an effective tool for stone management when introduced during robotic pyelolithotomy and provides additional optionality when manual extraction poses challenges.
Keywords: Lithotripsy, Pyelotomy, Robotic surgical procedures
INTRODUCTION
The management of staghorn renal stones is a challenging endeavor in urology. Though stone-free rates are high for many minimally invasive endourologic procedures such as ureteroscopy, percutaneous nephrolithotomy (PCNL), and extracorporeal shock wave lithotripsy, the management of staghorn stones remains a challenge that often requires multiple operations for full stone clearance.1 For this reason, open, laparoscopic, and robotic pyelolithotomy are useful procedures when managing a challenging staghorn stone, as well as in those patients requiring concurrent reconstructive procedures.2–4 However, given the complexity of these procedures, the opportunity for more efficient stone management as well as for options when manual stone removal pose challenges, would provide urologists with alternative options during pyelolithotomy.
The Boston Scientific Swiss LithoClast© Trilogy lithotripter was released in 2019, intended for use in PCNL. It has since been used in both mini PCNL and standard PCNL with high levels of success.5 Trilogy is a single lumen probe utilizing a dual energy source, combining both electromagnetic impact and ultrasonic energy, which together have been shown to efficiently fragment stones and reduce operative time.6 Additionally, it has a built-in suction system which helps remove small stone fragments, which provides the additional benefit of efficient stone removal with reduced need for stone basketing. Together, this makes the “all in one” mechanism of Trilogy (electromagnetic, ultrasonic, and suctioning) a very effective method for stone fragmentation and removal.
Though Trilogy was intended for PCNL, there is little literature on the use of intracorporeal lithotripsy during robotic procedures. Previous literature suggest that intracorporeal lithotripsy during pyelolithotomy is feasible as prior studies have had success with laser fragmentation during laparoscopic pyelolithotomy;7–9 however, the same has not been shown for a robotic approach. Furthermore, this technique has not been described during a concurrent robotic procedure which may introduce secondary challenges to full stone clearance while retaining success in the concurrent procedure. Previous reports have also discussed that when robotic pyelolithotomy has failed to manually remove all stone fragments, an open conversion has been required for full stone removal, suggesting there is room for consideration of other secondary options once manual robotic pyelolithotomy has failed.10 Additionally, while some have described the insertion of other instrumentation through robotic ports for stone basket removal,11 no studies to our knowledge have attempted to utilize intracorporeal lithotripsy which may demonstrate additional challenges to safe and efficient stone clearance. We present the first two uses of the Trilogy lithotripter for renal lithotomy during an intracorporeal robotic pyelolithotomy with concurrent renal robotic procedures.
Case 1
The patient was a 65-year-old female with a history of obesity as well as chronic left nephrolithiasis, previously having undergone PCNL. Following surveillance computed tomography, a recurrence complete left staghorn calculus composed primarily of uric acid (90%) and calcium oxalate dihydrate (10%) was discovered. Her stone measured roughly 500 Hounsfield units and was accompanied by hydronephrosis in the setting of a left ureteropelvic junction (UPJ) obstruction (Figure 1). The combination of a staghorn stone with a UPJ obstruction made a robotic pyelolithotomy an effective method for both stone removal and pyeloplasty for UPJ reconstruction.12 Due to the size and location of the stone, it was decided that if manual robotic attempts failed to provide efficient stone management, Trilogy lithotripsy would be attempted for more efficient stone fragmentation and removal. The patient was consented to undergo a robotic pyelolithotomy for stone fragmentation and removal using the Trilogy lithotripter along with robotic pyelolithotomy for UPJ reconstruction.
Figure 1.

Case 1; pre-operative computed tomography scan depicting complete left staghorn stone.
The patient was placed in the standard flank position for robotic pyelolithotomy, and robotic ports were placed under direct vision. A 12-mm assistant port was placed in the periumbilical area, and four 8-mm ports were placed in a linear configuration parallel to the mid axillary line extending from the subcostal area down to the pelvis, approximately 5 – 6 cm apart from one another. The robot was docked, and following insufflation, initial dissection, and mobilization, a hydronephrotic kidney was identified with significant inflammation and adhesions near the upper ureter. No crossing vessels were identified, and ureterolysis of the proximal ureter was performed until the proximal ureter and renal pelvis were completely freed from surround tissue. A small segment of the stenotic proximal ureter was then excised in order to relieve the obstruction and to gain access to the staghorn stone. At this point, a large staghorn stone branching into the upper, middle, and lower calyces was revealed (Figure 2). Initial attempts were made to completely remove the stone manually which proved to be unsuccessful due to involvement of all calyces. The 2.4-mm Trilogy probe was then passed into the abdomen through the 12-mm assistant's port without difficulty and was easily able to gain access to the stone (Figure 3). Under direct vision the stone was segmented into several large fragments which were able to be manually extracted by the robotic graspers (Figure 4). Renal endoscopy was subsequently performed using a disposable LithoVue™ ureteroscope and small remnant fragments were removed using stone basketing (Figure 5). Once the kidney and ureter were determined to be stone free, a 6 × 6 double-J ureteral stent was placed in a retrograde fashion and a posterior and anterior ureteral anastomosis was completed with full renal pelvis closure in a watertight continuous fashion using 3-0 barbed V-lock sutures. The operation was completed successfully with minimal estimated blood loss and no intraoperative complications. The patient was discharged without complications. Follow-up imaging showed full stone clearance with no signs of hydronephrosis (Figure 6).
Figure 2.
Robotic upper ureter incision to identify staghorn stone in the ureteropelvic junction.
Figure 3.

Introduction of the 2.4-centimeter Trilogy lithotripter probe through the 12-millimeter assistant port and initiation of stone fragmentation.
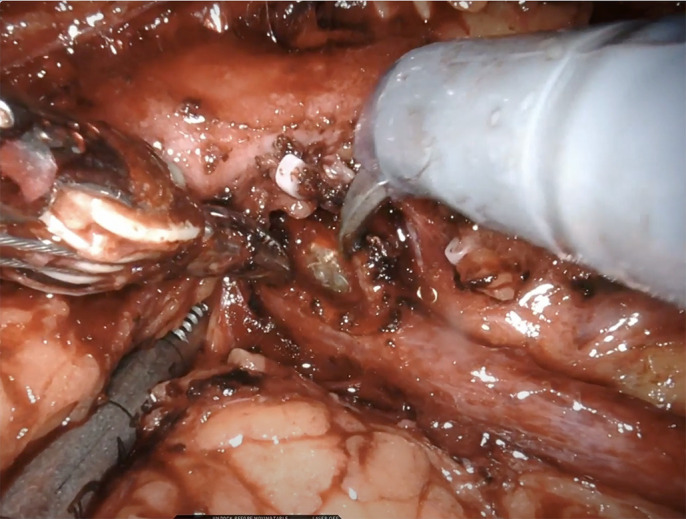
Figure 4.

Intracorporeal stone fragmentation with the Trilogy lithotripter.
Figure 5.

Inspection of the renal calyces using the LithovueTM ureteroscope identified all calyces as being stone-free intraoperatively.
Figure 6.

Case 1; postoperative computed tomography scan depicting a stone-free left kidney without signs of hydronephrosis.
Case 2
The second case occurred three months after the initial case was proven to be successful. The patient was a 69-year-old male with a history of chronic kidney stones and renal cyst formation. Computed tomography demonstrated multiple left-sided kidney stones, in the mid pole measuring at least 2 cm and the lower pole measuring 0.7 cm. Intraoperatively, it was determined to be one large staghorn stone (> 4 cm) involving the mid and lower poles. The stones were composed of 100% uric acid and measured roughly 700 Hounsfield units. Additionally, he presented with multiple simple renal cysts, the largest measuring up to 11.2 cm at the lower pole (Figure 7). For this patient, the combination of a large staghorn stone with a large renal cyst indicated a robotic approach. Following the successful application of the Trilogy lithotripter in case 1, again it was decided that should manual stone removal fail, the Trilogy lithotripter would be used for efficient stone management. The patient was consented to undergo a robotic pyelolithotomy for stone fragmentation and removal with possible use of the Trilogy lithotripter and robotic cyst decortication.
Figure 7.

Case 2; pre-operative computed tomography depicting large left staghorn stone and multiple large left-sided renal cysts.
This procedure followed a similar setup and approach to that of case 1. Following patient positioning, port placement, robot docking, and initial dissection and mobilization, the perirenal fat and Gerota’s fascia were removed from the surface to expose the cysts. The cysts were then excised and drained and the cyst walls were removed from the body for evaluation. Then the renal pelvis was incised to reveal a large staghorn stone. Robotic graspers were able to manually remove over 4 cm of stone; however, several large fragments of stone were lodged into the upper pole. Following a similar approach to case 1, the 2.4-mm Trilogy probe was introduced through the 12-mm assistant's port and under direct visualization the stones were fragmented until they were able to be removed using the robotic graspers, with smaller fragments being removed with endoscopic stone basketing. The calyces were determined to be stone free, a ureteral stent was placed, and the renal pelvis was closed in a watertight continuous fashion using 3-0 barbed V-lock sutures. The operation was completed successfully with minimal estimated blood loss and no intraoperative complications. The patient was discharged without complications and follow-up computed tomography revealed full stone clearance with minor cysts remaining in the lower pole (Figure 8).
Figure 8.

Case 2; postoperative computed tomography depicting full stone clearance.
DISCUSSION
These were the first two documented uses of the Trilogy lithotripter during intracorporeal robotic pyelolithotomy. The feasibility of this technique was determined based on the success of prior literature in intracorporeal lithotripsy during laparoscopic pyelolithotomy. Collins et al. described their technique for intracorporeal ultrasonic lithotripsy within an Endocatch bag during laparoscopic pyelolithotomy, which was then further evaluated by Sandhu et al.8,9 Additionally, Pastore et al. reported their successful utilization of a holmium-YAG laser during laparoscopic pyelolithotomy,7 to suggest that intracorporeal lithotripsy during pyelolithotomy is a feasible technique.
Robotic pyelolithotomy has been shown to be a safe and effective method for removal of large and complex kidney stones,2 as well as for procedures involving concurrent stone management and other renal or ureteral surgeries such as for obstructions, cysts, or masses.12–14 Much of the efficacy of laparoscopic and robotic pyelolithotomy lie in its ability to remove mostly intact large stones that would otherwise require several sessions of percutaneous nephrolithotomy for full stone removal.15,16 However, pyelolithotomy in general, does not always have a 100% extraction rate for large calyceal stones,3,17 and while robotic pyelolithotomy is an effective operation, given the surgical complexity, manual stone extraction can be challenging and timely.18 Therefore, surgeons may benefit from the utilization of lithotripsy technology that has been shown to efficiently fragment complex stones. To our knowledge, there has been no prior documentation regarding the use of intracorporeal lithotripsy during robotic pyelolithotomy.
This novel combined technique proved to be an effective method for fragmentation and extraction of a large staghorn stone while simultaneously treating secondary pathologies such as UPJ obstruction and renal cysts. The Trilogy’s efficacy in stone fragmentation and removal is due to its dual energy and “all in one” built in suctioning which allows for efficient stone fragmentation and removal. While this is true for PCNL, the major advantage of the Trilogy lithotripter during intracorporeal robotic surgery is partially due to its built-in cooling system which allows for use of the Trilogy with minimal need for continuous irrigation. This makes it advantageous for use in intracorporeal robotic surgery which does not allow for large amounts of continuous irrigation. Given Trilogy’s compatibility for intracorporeal robotic surgery, there were no mechanical or anatomical issues regarding the Trilogy placement, access to the stone, or ability to fragment and remove the stone. Had access become an issue, removal of one of the robotic arms to pass in the Trilogy would have been a feasible maneuver to help gain better access to the stone. Thus, this technique may be useful in complex cases where there is an indication for robotic pyelolithotomy, and manual extraction may be unsuccessful. Whether as an initial pre-operative plan, or as a secondary option if manual extraction fails, this technique should be considered as an alternative method for stone fragmentation in future cases, and it is the authors’ intention to continue investigating novel indications for robotic pyelolithotomy using Trilogy lithotripsy. However, while this report suggests the feasibility of this technique, the authors recognize that there are inherent limitations in the use of robotic procedures for stone removal. While this technique may be beneficial during specific instances for those that require robotic procedures for concurrent pathologies and in cases in which manual robotic stone removal has failed, it is not a replacement for gold-standard endourological procedures. This technique may serve as a helpful alternative when properly indicated, and further trials should be conducted with this method to continue to evaluate the long-term efficacy and best practices of this novel technique.
CONCLUSION
The Boston Scientific Swiss LithoClast® Trilogy lithotripter is an effective tool for stone fragmentation in robotic pyelolithotomy for patients with complex renal stones and other secondary pathologies in which a robotic surgery is indicated and manual stone removal has failed.
Footnotes
Acknowledgements: The authors would like to acknowledge that parts of case 1 were previously presented in an abstract form in the American Urological Association 2022 symposium. This case report serves as a more in-depth discussion of this methodology by including a second novel procedure using this method and provides additional information, clinical findings, and discussion on this topic.
Disclosure: none.
Conflict of interests: none.
Funding sources: none.
Informed consent: Mr. Micah Levy declares that written informed consent was obtained from the patient/s for publication of this study/report and any accompanying images.
Contributor Information
Micah Levy, Department of Urology, Icahn School of Medicine at Mt. Sinai, New York, NY..
Chih Peng Chin, Department of Urology, Icahn School of Medicine at Mt. Sinai, New York, NY..
Krishna T. Ravivarapu, Department of Urology, Icahn School of Medicine at Mt. Sinai, New York, NY..
Osama Al-Alao, Department of Urology, Icahn School of Medicine at Mt. Sinai, New York, NY..
Francisca Larenas, Department of Urology, Icahn School of Medicine at Mt. Sinai, New York, NY..
Michael A. Palese, Department of Urology, Icahn School of Medicine at Mt. Sinai, New York, NY..
References:
- 1.Diri A, Diri B. Management of staghorn renal stones. Ren Fail. 2018;40(1):357–362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Corsi P, Daniele D'Agostino D, Giampaoli M, et al. Minimally invasive pyelolithotomy: comparison of robot-assisted and laparoscopic techniques. Surg Technol Int. 2019;34:296–301. [PubMed] [Google Scholar]
- 3.Schulster ML, Sidhom DA, Sturgeon K, Borin JF, Bjurlin MA. Outcomes and peri-operative complications of robotic pyelolithotomy. J Robot Surg. 2020;14(3):401–407. [DOI] [PubMed] [Google Scholar]
- 4.Kramer BA, Hammond L, Schwartz BF. Laparoscopic pyelolithotomy: indications and technique. J Endourol. 2007;21(8):860–861. [DOI] [PubMed] [Google Scholar]
- 5.Sabnis RB, Balaji SS, Sonawane PL, et al. EMS Lithoclast Trilogy™: an effective single-probe dual-energy lithotripter for mini and standard PCNL. World J Urol. 2020;38(4):1043–1050. [DOI] [PubMed] [Google Scholar]
- 6.Large T, Nottingham CU, Brinkman JE, et al. Multi-institutional prospective randomized control trial of novel intracorporeal lithotripters: ShockPulse-SE vs TrilogyTM Trial. J Endourol. 2021;35(9):1326–1332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pastore AL, Palleschi G, Silvestri L, et al. Combined laparoscopic pyelolithotomy and endoscopic pyelolithotripsy for staghorn calculi: long-term follow-up results from a case series. Ther Adv Urol. 2016;8(1):3–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Collins S, Marruffo F, Durak E, et al. Laparoscopic pyelolithotomy with intraperitoneal ultrasonic lithotripsy: report of a novel minimally invasive technique for intracorporeal stone ablation. Surg Laparosc Endosc Percutan Tech. 2006;16(6):435–436. [DOI] [PubMed] [Google Scholar]
- 9.Sandhu JS, Varma V, Mishra M. Laparoscopic laser lithotripsy inside the endocatch bag: an alternative technique for removal of large post lap pyelolithotomy calculi. Med J Armed Forces India. 2018;74(1):72–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Müller PF, Schlager D, Hein S, Bach C, Miernik A, Schoeb DS. Robotic stone surgery - current state and future prospects: a systematic review. Arab J Urol. 2018;16(3):357–364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lee G, Patel HV, Sterling J, Elsamra S. V01-10 robotic-assisted laparoscopic ureterocalicostomy and pyelolithotomy for proximal ureteral stricture. J Urol. 2022;207(Supplement 5):e55. [Google Scholar]
- 12.Siddiqui KM, Albala DM. Robotic-assisted surgery and treatment of urolithiasis. Int J Surg. 2016;36(Pt D):673–675. [DOI] [PubMed] [Google Scholar]
- 13.Andrade HS, Zargar H, Caputo PA, et al. Robotic pyelolithotomy for staghorn nephrolithiasis during partial nephrectomy. Int Braz J Urol. 2016;42(3):623–625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Jensen PH, Berg KD, Azawi NH. Robot-assisted pyeloplasty and pyelolithotomy in patients with ureteropelvic junction stenosis. Scand J Urol. 2017;51(4):323–328. [DOI] [PubMed] [Google Scholar]
- 15.Mao T, Wei N, Yu J, Lu Y. Efficacy and safety of laparoscopic pyelolithotomy versus percutaneous nephrolithotomy for treatment of large renal stones: a meta-analysis. J Int Med Res. 2021;49(1):300060520983136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Madi R, Hemal A. Robotic pyelolithotomy, extended pyelolithotomy, nephrolithotomy, and anatrophic nephrolithotomy. J Endourol. 2018;32(S1):S73–s81. [DOI] [PubMed] [Google Scholar]
- 17.Chander J, Suryavanshi M, Lal P, Singh L, Ramteke VK. Retroperitoneal pyelolithotomy for management of renal calculi. JSLS. 2005;9(1):97–101. [PMC free article] [PubMed] [Google Scholar]
- 18.Atug F, Castle EP, Burgess SV, Thomas R. Concomitant management of renal calculi and pelvi-ureteric junction obstruction with robotic laparoscopic surgery. BJU Int. 2005;96(9):1365–1368. [DOI] [PubMed] [Google Scholar]