

Abstract
The vaginal birth after cesarean (VBAC) rate was last reported as 13.8% in 2019. However, contemporary trends in attempted and successful trial of labor (TOLAC) among individuals with prior cesarean delivery are not known. We performed a repeated cross-sectional analysis of singleton, cephalic, term deliveries in those with history of one or two prior cesarean deliveries in the National Vital Statistics System from 2010 to 2020. Temporal trends in attempted and successful TOLAC, as well as VBAC, were characterized using joinpoint regression. Overall 4,277,800 deliveries were included. Attempted TOLAC increased from 15.3% in 2010 to 21.7% in 2020 with an annual percentage change of 4.25% (95% CI 2.9–5.6%). Successful TOLAC increased from 69.8% to 74.7% with an annual percentage change of 0.91% (95% CI 0.7–1.2%). The VBAC rate similarly increased. Rates of attempted and successful TOLAC, and VBAC, are increasing; efforts should continue to support TOLAC in appropriate candidates.
Précis:
National rates of attempted and successful trial of labor after cesarean increased from 2010 to 2020.
Introduction
Options for delivery in individuals with a history of cesarean in a subsequent pregnancy include planned repeat cesarean, or pursuing trial of labor after cesarean (TOLAC).1–3 The vaginal birth after cesarean (VBAC) rate is tracked in annual vital statistics and was last reported as 13.8% in 2019.4 The VBAC rate does not provide detail on nationwide rates of attempted and successful TOLAC, and recent trends are not known.5 We aimed to evaluate trends in attempted and successful TOLAC, as well as VBAC, using national vital statistics data.
Methods
This was a repeated cross-sectional analysis of singleton, cephalic, term deliveries with history of one or two prior cesarean deliveries in the National Vital Statistics System (NVSS) from 2010 to 2020. The NVSS contains publicly available natality data from all 50 U.S. states.6–8 The study timeframe encompassed use of two birth certificate versions – 1989 and 2003. TOLAC data are only available using the 2003 birth certificate version; thus, only states using the 2003 version during any particular year were included with adoption in all states by 2016. Attempted TOLAC was defined using birth certificate mode of delivery as vaginal, or cesarean with trial of labor attempted. Successful TOLAC was defined by vaginal mode of delivery among those attempting TOLAC. VBAC rate was defined by vaginal mode of delivery among all deliveries with a history of cesarean.
Rates of attempted and successful TOLAC, and VBAC, were described and compared over time using the National Cancer Institute’s Joinpoint Regression Program with the annual percentage change (APC) with 95% CI reported.9 A sensitivity analysis limited to individuals with only one prior cesarean was performed. This study was exempt from Institutional Review Board approval as all data were deidentified.
Results
Overall, 4,277,800 deliveries were included. Of these, 77% had only one prior cesarean delivery and 45% had a prior vaginal delivery. See Appendix 1 for additional population demographics. The rate of attempted TOLAC increased over the study period from 15.3% in 2010 to 21.7% in 2020 with an APC of 4.25% (95% CI 2.9–5.6%; Table 1). The rate of successful TOLAC increased from 69.8% to 74.7% during the study period (APC 0.91%, 95% CI 0.7–1.2%). The VBAC rate similarly increased with an APC of 5.21% (95% CI 3.8–6.7%; Figure 1). In sensitivity analysis limited to those with history of only one prior cesarean, results were similar.
Table 1.
Rates of attempted and successful trial of labor after cesarean, and rates of vaginal birth after cesarean, among singleton, cephalic, term deliveries in the U.S. from 2010 to 2020
| Year | Deliveries* | Attempt TOLAC | Successful TOLAC† | VBAC‡ |
|---|---|---|---|---|
| 2010 | 293,723 | 44,888 (15.3) | 31,324 (69.8) | 31,324 (10.7) |
| 2011 | 328,720 | 52,866 (16.1) | 36,487 (69.0) | 36,487 (11.1) |
| 2012 | 352,190 | 59,936 (17.0) | 41,393 (69.1) | 41,393 (11.8) |
| 2013 | 371,051 | 64,868 (17.5) | 45,500 (70.1) | 45,500 (12.3) |
| 2014 | 408,525 | 73,427 (18.0) | 53,155 (72.4) | 53,155 (13.0) |
| 2015 | 421,722 | 78,422 (18.6) | 57,455 (73.3) | 57,455 (13.6) |
| 2016 | 445,577 | 87,909 (19.7) | 64,060 (72.9) | 64,060 (14.4) |
| 2017 | 441,286 | 88,006 (19.9) | 65,130 (74.0) | 65,130 (14.8) |
| 2018 | 438,610 | 90,537 (20.6) | 67,479 (74.5) | 67,479 (15.4) |
| 2019 | 367,246 | 93,076 (25.3) | 69,971 (75.2) | 69,971 (19.1) |
| 2020 | 409,150 | 88,797 (21.7) | 66,319 (74.7) | 66,319 (16.2) |
Data presented as n(%). Trial of labor (TOLAC); vaginal birth after cesarean (VBAC)
Individuals missing mode of delivery data (0.1%) were excluded from analysis.
Successful TOLAC defined as vaginal mode of delivery among those attempting TOLAC.
VBAC defined as vaginal mode of delivery among all deliveries with a history of cesarean.
Figure 1.
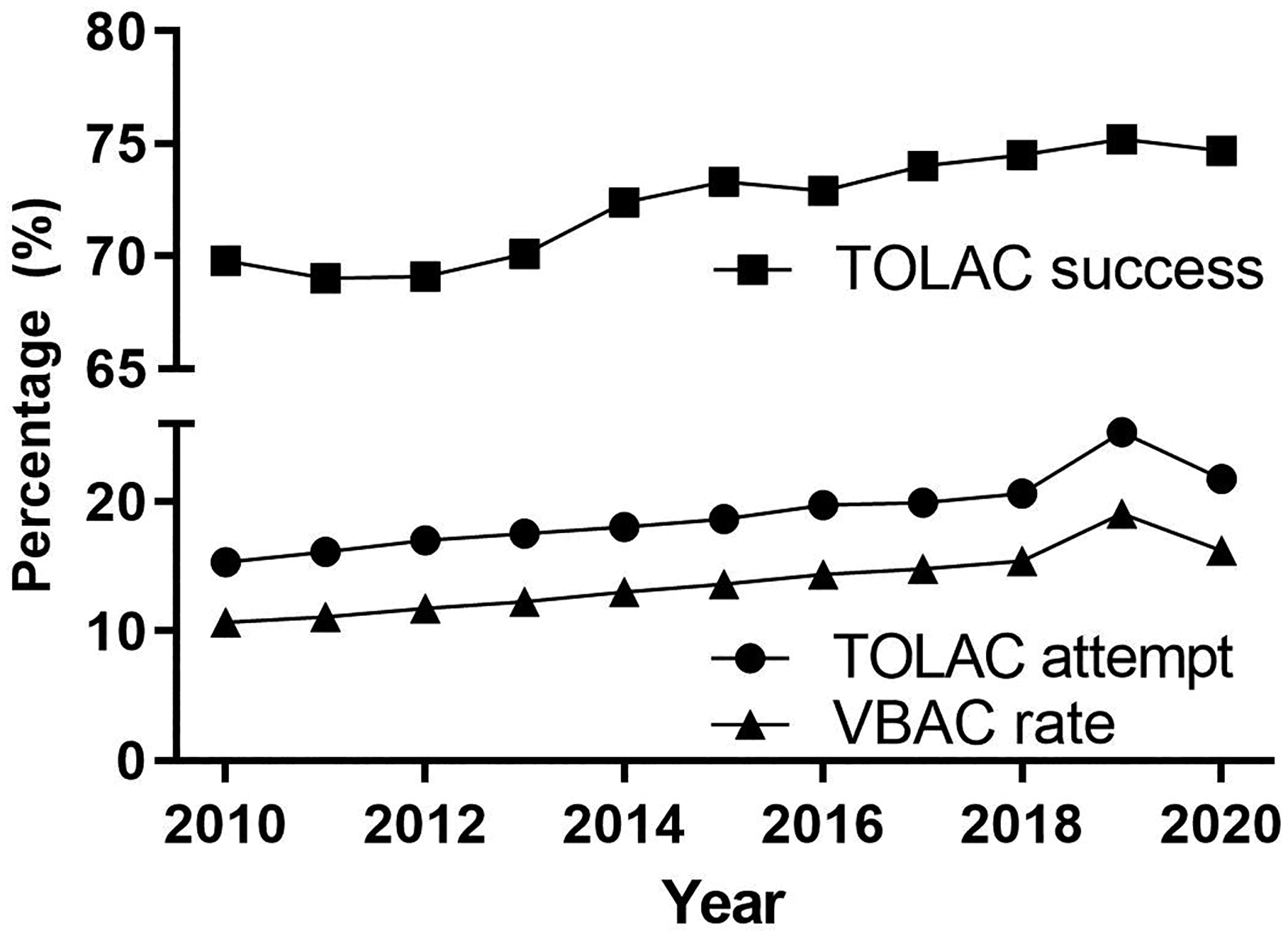
Trends in trial of labor and vaginal birth after cesarean among singleton, cephalic, term deliveries in the U.S. from 2010 to 2020.
Trial of labor (TOLAC); Vaginal birth after cesarean (VBAC)
Discussion
We found the nationwide rate of attempted and successful TOLAC, and VBAC, increased over the last decade.
Using National Hospital Discharge Survey data, Uddin & Simon found rates of attempted TOLAC varied widely from a high of 51.8% in 1995 to a low of 15.9% in 2006.5 They found the rate of attempted TOLAC was increasing (average APC 1.2% from 2005–2009, 95% CI 0.0–2.3%) while the rate of successful TOLAC was decreasing (average APC −3.4% from 2000–2009, 95% CI −4.3 to −2.5%).5 Our findings extend this prior work to a contemporary time frame using national data.
Strengths of this analysis include use of a large, nationally representative sample. Limitations include the absence of granular clinical details and risk of misclassification from birth certificate reporting.
This study provides U.S. population-level trends on attempted and successful TOLAC. It remains unknown whether changes in practitioner and hospital support of TOLAC, state and national level initiatives focused on cesarean reduction, or other factors contributed to these findings. While rates of attempted and successful TOLAC are increasing, the highest annual rate of attempted TOLAC (22%) in 2020 remains below historical peaks and overall increases are modest. Nonetheless, the high TOLAC success rate (75%) supports continued efforts to encourage TOLAC in appropriate candidates.
Supplementary Material
Funding:
There was no funding for this work.
Financial Disclosure:
Torri D. Metz reports personal fees from Pfizer for her role as a medical consultant for a SARS-CoV-2 vaccination in pregnancy study, grants from Pfizer for role as a site PI for SARS-CoV-2 vaccination in pregnancy study, grants from Pfizer for role as a site PI for RSV vaccination in pregnancy study, and grants from Gestvision for role as a site PI for a preeclampsia study outside the submitted work. The other authors report no conflict of interest.
References:
- 1.Vaginal Birth After Cesarean Delivery. ACOG Practice Bulletin No. 205. American College of Obstetricians and Gynecologists. Obstet Gynecol 2019;133(2):e110–e127. doi: 10.1097/aog.0000000000003078 [DOI] [PubMed] [Google Scholar]
- 2.Guise JM, Denman MA, Emeis C, Marshall N, Walker M, Fu R, et al. Vaginal birth after cesarean: new insights on maternal and neonatal outcomes. Obstet Gynecol 2010;115(6):1267–1278. doi: 10.1097/AOG.0b013e3181df925f [DOI] [PubMed] [Google Scholar]
- 3.Silver RM, Landon MB, Rouse DJ, Leveno KJ, Spong CY, Thom EA, et al. Maternal morbidity associated with multiple repeat cesarean deliveries. Obstet Gynecol 2006;107(6):1226–32. doi: 10.1097/01.Aog.0000219750.79480.84 [DOI] [PubMed] [Google Scholar]
- 4.Martin JA, Hamilton BE, Osterman MJK, Driscoll AK. Births: Final Data for 2019. Natl Vital Stat Rep. 2021;70(2):1–51. [PubMed] [Google Scholar]
- 5.Uddin SF, Simon AE. Rates and success rates of trial of labor after cesarean delivery in the United States, 1990–2009. Matern Child Health J 2013;17(7):1309–14. doi: 10.1007/s10995-012-1132-6 [DOI] [PubMed] [Google Scholar]
- 6.Centers for Disease Control and Prevention. About the National Vital Statistics System. Accessed December 12, 2021. https://www.cdc.gov/nchs/nvss/about_nvss.htm
- 7.Centers for Disease Control and Prevention. Natality Information. WONDER System Accessed December 12, 2021. https://wonder.cdc.gov/natality.html
- 8.Ventura SJ. The U.S. National Vital Statistics System: Transitioning Into the 21st Century, 1990–2017. Vital Health Stat 1 2018(62):1–84. [PubMed] [Google Scholar]
- 9.National Cancer Institute. Joinpoint trend analysis software. Accessed March 2, 2022. https://surveillance.cancer.gov/joinpoint/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.