

Abstract
Management of anterior cruciate ligament (ACL) tears has continuously evolved since its first description in approximately 170 A.D. by Claudius Galenus of Pergamum and Rome. The initial immobilization using casts was replaced by a variety of surgical and conservative approaches over the past centuries. The first successful case of ACL repair was conducted by Mayo Robson in 1885, suturing cruciate at the femoral site. In the nineteenth century, surgical techniques were focused on restoring knee kinematics and published the first ACL repair. The use of grafts for ACL reconstruction was introduced in 1917 but gained popularity in the late 1900s. The introduction of arthroscopy in the 1980s represented the greatest milestones in the development of ACL surgery, along with the refinements of indications, development of modern strategies, and improvement in rehabilitation methods. Despite the rapid development and multitude of new treatment approaches for ACL injuries in the last 20 years, autografting has remained the treatment of choice. Compared to the initial methods, arthroscopic procedures are mainly performed, and more resistant and safer fixation devices are available. This results in significantly less trauma from the surgery and more satisfactory long-term results. The most commonly used procedures are still patellar tendon or hamstring autograft. Additionally, popular, but less common, is the use of quadriceps tendon (QT) grafts and allografts. In parallel with surgical developments, biological reconstruction focusing on the preservation of ACL remnants through the use of cell culture techniques, partial reconstruction, tissue engineering, and gene therapy has gained popularity. In 2013, Claes reported the discovery of a new ligament [anterolateral ligament (ALL)] in the knee that could completely change the treatment of knee injuries. The intent of these modifications is to significantly improve the primary restriction of rotational laxity of the knee after ACL injury. Kinematic studies have demonstrated that anatomic ACL reconstruction and anterolateral reconstruction are synergistic in controlling pivot displacement. Recently, there has been an increased focus on the application of artificial intelligence and machine learning to improve predictive capability within numerous sectors of medicine, including orthopedic surgery.
Keywords: Anterior cruciate ligament (ACL), grafts, history, anterolateral ligament (ALL)
Introduction
The history of anterior cruciate ligament (ACL) surgery is characterized by constant development and advances in sustainable approaches (1,2). The discovery of ACL anatomy and biomechanics goes hand in hand with the establishment of methods of diagnosis and management of injuries (3).
From Galenus to the 19th century
The first description of the ACL was made in approximately 170 A.D. by Claudius Galenus of Pergamon and Rome in his tractate “On the usefulness of the parts of the body” (4). Galenus described the anatomy of the knee joint and named the cruciate ligament “ligamenta genu cruciate”, a structure that stabilizes the joint. However, Galenus did not dwell on its function (4-6). Thereafter, there was a long period of time without significant improvement in medicine, and the utterance of Galenus was the “ipse dixit”, the only truth. During the 19th century, new studies on the structure, function, injury patterns, and possible treatment were conducted (5). In 1836, the German brothers Weber published “Mechanik der menschlichen gehwerkzeuge”, an investigation on the kinematics of running and walking (7). Their illustrations showed that the cruciate ligament consists of two distinct and separate bundles, which are tensed differently during movement. Furthermore, they note an anterior translation of the tibia relative to the femur when these bundles are sectioned, which still represents an important sign in the diagnosis of ACL rupture (7-9). The “Traité des maladies des articulations” (treatise on joint diseases) was published in 1845 by Bonnet, an estimated professor of surgery at the University of Lyon, France (10). The author suggested conservative management and early rehabilitation to preserve the cartilage (10). Regrettably, his tractate remained hidden for years, as it was not translated into English. In 1850, James Stark published “Two cases of rupture of the crucial ligament of the knee-joint” (11). Both cases were managed conservatively with a cast for 3 months and a semirigid splint for 10 months (11). In 1875, Noulis, in his thesis entitled “Entorse du genou”, described how to diagnose the rupture of the ACL with an extended knee, which is a vestigial of the “Lachman test” (12). In 1879, Segond first associated a fracture of the anterolateral tibial plateau with a tear of the ACL. Segond described signs and symptoms associated with ACL rupture, including severe joint pain, clicking, effusion, and abnormal anterior tibial translation at the clinical examination (13). In summary, until the 19th century, conservative management of ACL tears was recommended, involving the use of orthosis and prolonged immobilization.
Twentieth century: from ligament repair to reconstruction
The first successful case of ACL repair was conducted by Mayo Robson in 1895, suturing cruciates at the femoral site (14). Good joint function with no signs of instability was found at the 8-year follow-up (14). In 1900, Battle also published the results of open ACL repair in one patient with knee dislocation (15). Perthes first sutured the ligament to the bone using a bronze and aluminum wire, which was then passed through holes illed through the stump of the ligament to the outside of the lateral femoral condyle (16). In 1913, Goetjes recommended direct repair of acute and chronic ruptures and pioneered the examination of the patient under anesthesia to confirm the diagnosis (17). Based on the studies of Perthes (16) and Marshall (18), the direct repair of a ruptured ACL was maintained until the 1980s. In 1903, Fritz Lange of Munich [1864–1952] made the first suggestion that silk may be used as prosthetic ligaments to cure “wobbly knees” after using it effectively to heal paralysed feet in 1895 (19,20). He described four examples of ACL insufficiency in 1907, stabilizing them with hamstring tendons (HTs) and extra-articularly positioned “artificial ligaments made of silk” (Figure 1) (21). Lange complimented the “amazing potential of the silk to develop fibrous tissue under functional stress”, which had been discovered by Max Borst of Würzburg [1869–1946] a few years earlier (19,21). The silk was gradually enveloped by fibrous tissue. Max, the grandson of Lange, announced in 1932 that he had successfully reconstructed an ACL using silk supplemented with fascia (20). Lange understood that silk alone could not provide joint stability; rather, he viewed silk as a scaffold that might initially provide strength while also triggering a process of ligament mending and regeneration.
Figure 1.
In 1903, Lange started using silk sutures as extra-articular augmentation to treat chronic knee instabilities. His grandson Max introduced the technique of partial substitution/reconstruction of the torn ACL with “HydrargyrumoxyzyanatSeide” in the late 1920s. ACL, anterior cruciate ligament.
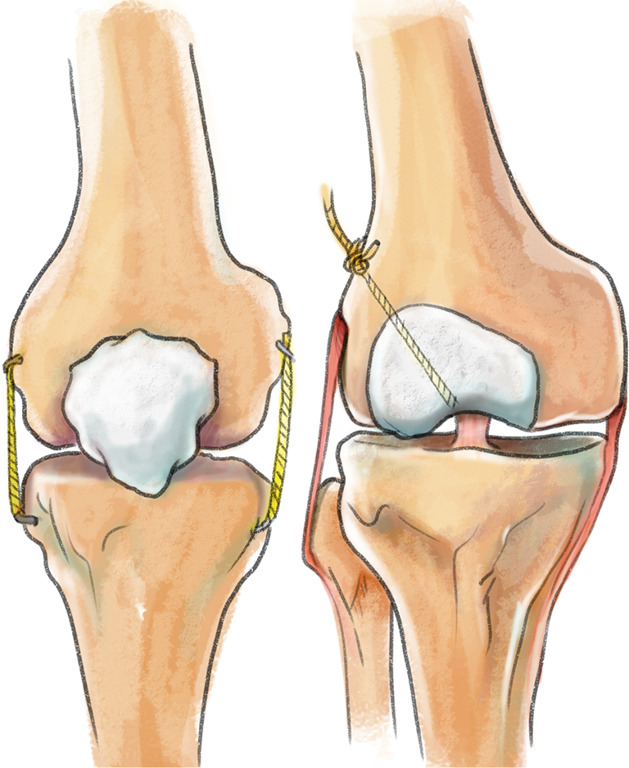
Thereafter, techniques to reconstruct the ACL were developed (22-24). In 1917, Ernest William Hey-Groves published his technical note entitled “Operation for the repair of the crucial ligaments” on how to perform ACL reconstruction using a fascia lata graft (22). Concerning the surgical exposure, the author stated as follows: “anterior horseshoe-shaped incision across the joint, with the deepest point just below the tibial tuberosity and the lateral ends extending to the lines of the hamstrings on each side” followed by an osteotomy of the tibial tuberosity to adequately expose the joint. The incision was widened laterally to allow the removal of a strip of the iliotibial band. The graft was detached from the tibial insertion, passed through the tibial and femoral tunnels and sutured to the periosteum and aponeurosis (22-25). In 1920, the Italian orthopedic surgeon Putti published the results of ACL collateral ligament reconstruction using flaps of the fascia lata. The patient was able to walk again 5 months postoperatively (26). In 1934, Galeazzi first used the hamstring autograft in ACL reconstruction in three patients (Figure 2) (27). He used the semitendinosus tendon autograft, which was prepared from the musculotendinous junction and then passed intraarticularly through a 5 mm tibial tunnel and a tunnel illed over the lateral femoral condyle, where it was attached to the periosteum (28). Galeazzi used three incisions: one for harvesting the semitendinosus tendon, a second for knee arthrotomy, and a lateral incision for fixation. A plaster cast was used for 4 weeks, and partial weight bearing was allowed for 6 weeks (27,28). In the 1950s, D’Aubigne revisited Galeazzi’s method using a pedicled semitendinosus autograft and passed a gracilis autograft through a transfemoral tunnel (29). This technique was reinterpreted and improved by Lange and Cho (30,31). In 1936, Campbell reported 17 patients treated with a “tibial graft” consisting of the medial third of the patellar tendon, part of the QT, and the prepatellar retinaculum (Figure 3) (32). The procedure consisted of two different tunnels and fixation of the tibial graft to the periosteum at the end of the femoral tunnel. A postoperative immobilization orthosis of 3 weeks was recommended. Fifty-three percent (9 of 17) of the operated patients had a stable knee with no pain or stiffness and were able to return to sports within 6 to 10 weeks after surgery (32). In 1963, Kenneth Jones published a surgical technique entitled “Reconstruction of the anterior cruciate ligament. A technique using the central one-third of the patellar ligament” describing the use of the middle third of the patellar tendon and a patellar bone block (33). The graft was still connected to the tibial site, and no tibial tunnel was made. Given the short length of the graft, the femoral tunnel was made from the anterior margin of the intercondylar notch, and the graft was secured to the periosteum at the end of the femoral tunnel (Figures 4,5) (33). This technique was the forebear of modern bone-patellar tendon-bone autografts (BPTB) (18,34-36). In 1979, Macintosh and Marshall introduced the “quadriceps tendon substitution technique”, which involves one-third of the entire central extensor mechanism, with a large portion of prepatellar aponeurotic tissue, which was taken as a graft beyond the top of the femoral condyle through the tunnel and fixed with a suture or metal clip, with the end piece extended posteriorly and anchored to Gerdy’s tuberosity. This technique is also known as “over-the-top repair” (18,37). Some authors suggested continuing to maintain the connection between the patellar tendon and Hoffa’s ligament to ensure vascularization of the ligament, and other authors postulated improving the loading of the neo ligament by internal rotation to connect this intra-articular plastic with lateral tenodesis, thus protecting the graft during the “ligamentization” process (38,39). During that time, a femoral tunnel was still filled from the outside to the inside for the graft. The graft was then fixed using wires and extra-articular screws. In this context, the introduction of interference screws brought a significant improvement (40,41). As these techniques became more reliable and refined, the need for anterolateral tenodesis declined. The innovative interference screw technique achieved greater outcomes and faster rehabilitation (38,39). The overall results were graded as excellent in thirty knees, good in seventeen knees, fair in one knee, and a failure in two knees. One knee that was classified as a failure showed excellent stability (38).
Figure 2.

In 1934, Galeazzi of Milan presented his ACL reconstruction technique with an anatomically placed distally pedicled hamstring graft (semitendinosus). ACL, anterior cruciate ligament.
Figure 3.

ACL reconstruction with the extensor fascia and patellar tendon was performed according to Campbell. Red dashed lines indicate bone profiles. ACL, anterior cruciate ligament.
Figure 4.
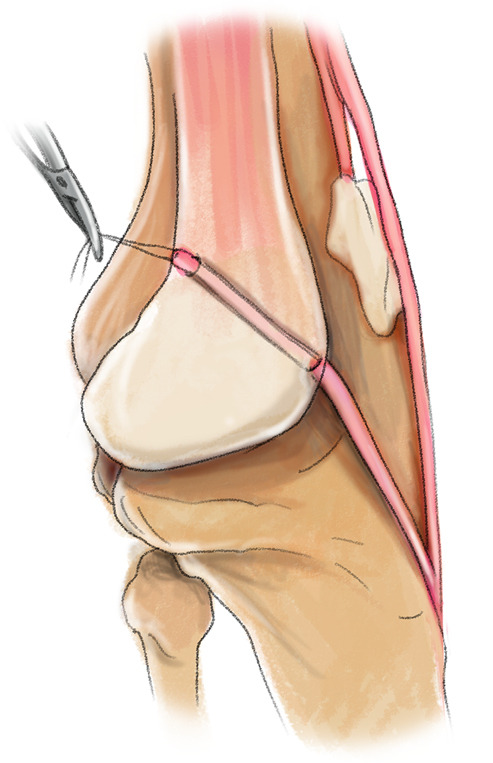
The new ligament is pulled into the drill hole in the femur so that its proximal portion emerges from the lateral surface of the femur. The ligament lies beneath the fat pad.
Figure 5.
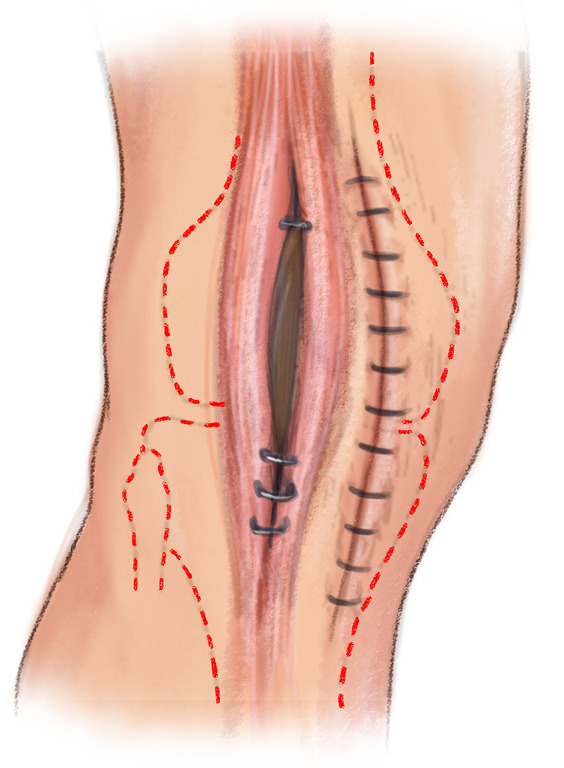
Closure of the medial parapatellar incision and the defect in the patellar tendon. Red dashed lines indicate bone profiles.
In the 1980s, the arthroscope, developed in the late 1970s by Robert Jackson of Toronto and David Dandy of Cambridge for meniscal lesions, was proposed for ACL surgery (42,43). In 1982, Dandy et al. performed the first arthroscopic ACL reconstruction using a synthetic graft (44). Until the mid-1980s, the arthroscope was used to illuminate the tibial tunnel under anterior portal vision; however, arthrotomy was still performed for the femoral tunnel, which was filled from outside-in (OI), using a rear-entry guide (45,46). It was until the introduction of arthroscopic ills and offset guides that the femoral tunnel could be prepared either through the tibial tunnel [transtibial (TT)] or through the medial portal, avoiding a second incision (47-49). However, some inconveniences occurred with the use of the BPTB technique, including anterior knee pain, bone blocks in the femoral tunnel, extension deficits, patellar tendinitis, and patellar fractures. The HT or QT autografts regained attention (50,51). The hamstring procedure was first introduced by Galeazzi in 1934 (27) and subsequently modified by Macey in 1939 (52) and later by Cho in 1975 (31), using either the semitendinosus or gracilis tendons harvested at their proximal insertion. In 1980, Puddu using the same technique, widened the tibial tunnel with an additional joint opening positioned entirely medially, and the internal rotation effect of the semitendinosus was preserved (53). In 1982, Lipscomb published the first combination of semitendinosus and gracilis tendon autografts (54). All surgeons who used this grafting procedure used the same principle, with some variations regarding the freedom or attachment of the graft at its distal end, whether it is single (2 strands) or double (4 strands) bundled, and a plethora of proposed methods for fixation of the graft. Later methods were developed using semitendinosus in triplicate (55). In 1988, Friedman used four ligament strands while experimenting with an arthroscopic-assisted self-grafting technique (56). Howell et al. (57), Rosenberg (58) and Pinczewski (59) followed him in 1993 and 1997. In 1998, Marcacci et al. suggested using one of the strands of the graft for anterolateral tenodesis (60). The HT graft became successful due to an easier postoperative regimen and rehabilitation, less invasiveness, lower risk of stiffness, and decreased anterior pain. The use of QT autografts for ACL replacement (ACLR) was first introduced by Marshall et al. in 1979 (18). He used a pure soft tissue graft that started 5–6 cm proximal to the patella and extended into the patellar tendon, incorporating the prepatellar retinacular tissue (18). The early, negative clinical results of the QT autograft were caused by an outdated surgical procedure that required significant exposure and removal of a substantial portion of the extensor mechanism, including the patellar tendon, prepatellar retinaculum, and QT (18). With this method, positive pivot displacement, increased postoperative knee laxity, and weakening of the extensor mechanisms, especially in women, are observed in 20% of cases (61). Blauth presented the results of a central QT graft with a bone plug in the mid-1980s (62). In the late 1990s, Fulkerson et al. published the first method for harvesting QT without bone (63).
Fulkerson reported clinical outcomes in 28 patients, and 4 of these sustained a new ACL rupture. The author concluded that the QT is thicker and wider than the patellar tendon, thereby providing a plentiful source of tendon for ligament reconstruction purposes (63). The newer methods of QT autografting demonstrated a stronger and more stable graft with fewer soft tissue incisions compared to BPTB and HT autografts (64,65). A recent systematic review concluded that the QT showed better and more significant results with knee flexion than with the hamstring and similar results to the BTB at 6 and 12 months. Compared to QT, hamstrings showed better and more significant results with knee extension at 6 months and similar results at 12 months (64). Furthermore, QT autograft has a lower rerupture rate than hamstrings in ACL reconstruction, with lower donor site morbidity. QT appeared to be slightly better for residual pivot shift, but there was no difference in patient-reported outcomes (65). Furthermore, comparable clinical and functional outcomes and graft survival were found. However, compared to BPTB autografts, QT autografts had significantly less pain at the harvest site and better functional outcomes than HT autografts (66). In addition to conventional autografts, augmentations and arthroscopic procedures, another innovation of this period was the development of allografts. In this context, Kennedy and Willis introduced “Kennedy-ligament augmentation device (LAD)”, a synthetic tape made of polypropylene, in late 1970s (67). In 1971, the Cardiff group started using carbon grafts because of their biological and mechanical potential. However, since 1980, this procedure has been abandoned due to the complications involved (68).
The majority of these complications are effusions and reactive synovitis (68). The etiology of this synovial reaction may be exposure of disrupted ends of the synthetic material in the joint, allowing for particulate migration. Impingement of the reconstructed ligament in the intercondylar notch may be a source of particles, and therefore, these effusions resolve after a notchplasty (68). However, not all patients show wear particles at biopsy, and the true cause of the effusions is therefore unclear. Impingement per se and a possible lack of full extension can cause these effusions. The use of the LAD may be associated with an increased risk of intra-articular infection. In the presence of a superficial infection, the LAD may act as an avenue for intraarticular spread by a wick action (68).
Dandy et al. performed the first arthroscopic reconstructive procedure as previously mentioned and implanted a carbon fiber ligament in this context in 1982 (44). He combined this with a lateral plastic with the McIntosh technique. Because the results did not meet expectations and traces and deposits of carbon were found in the synovial membrane and liver, the use of carbon in ACL reconstruction was quickly discontinued (69). Dacron and Gore-Tex were other material alternatives and became popular in reconstructive surgery as ligament replacements. However, there was a high rate of synovitis and resulting rupture of the operated ligaments, which led to the abandonment of this technique (70,71).
Twenty-first century: double-bundle (DB), regenerative reconstruction, and anterolateral procedures
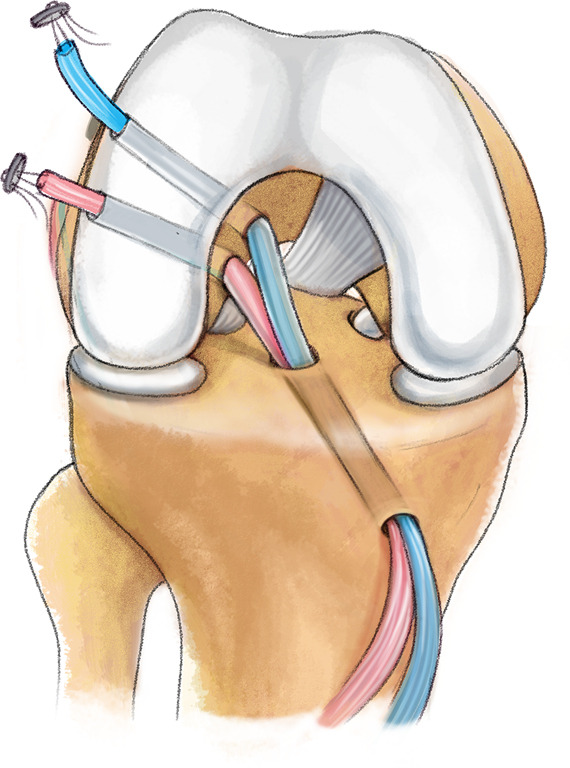
Despite the rapid development and multitude of new treatment approaches for ACL injuries in the last 20 years, autografting has remained the treatment of choice. Compared to the initial methods, arthroscopic procedures are mainly performed, and more resistant and safer fixation devices are available (72). This results in significantly less trauma from the surgery and more satisfactory long-term results. The most commonly used procedures are still BPTB or hamstring autografts (73). Additionally, popular, but significantly less common, is the use of QT grafts and allografts (74). Despite the high-quality optimization of these treatments, a positive “pivot shift” test can still be identified in up to 25% of patients (75). These results prompted further reconsideration of the procedures, with the correction of rotational laxity playing the definitive role. In 1972, Viernstein and Keyl recommended an anatomic reconstruction technique for the first time, now using two separate ACL bundles (Figure 6) (76,77). Based on this, further modified procedures by other surgeons followed (62,78-81) until 1999, when Muneta et al. published the DB technique, which is still current today (82). Modern DB reconstruction aims to restore the original anatomical positioning of the ACL bundles with the goal of restoring physiologic knee kinematics in terms of translation and rotation (Figure 7) (83-86). How this approximately correct anatomical positioning of the grafts can be achieved was described in 2004 by Yasuda et al. (87). In fact, the author discovered that the femur’s footprint has an egg-like form and that its long axis is inclined by 30° towards the posterior direction relative to the femur’s long axis. The long axis line of the ACL attachment and the vertical line (V-line) drawn through the contact point between the femoral condyle and the tibial plateau at 90° of flexion are specifically where the center of attachment [the posterolateral (PL) point] of the PL bundle is situated (87). The medial portal is used to determine the PL point arthroscopically. When measuring using the offset guide, a Kirshner wire should be placed 5 to 6 mm distal from the rear of the femur in order to locate the tunnel for the anteromedial bundle (87).
Figure 6.
The first DB ACL reconstruction performed by Viernstein and Keyl in Munich in 1972. DB, double-bundle; ACL, anterior cruciate ligament.
Figure 7.
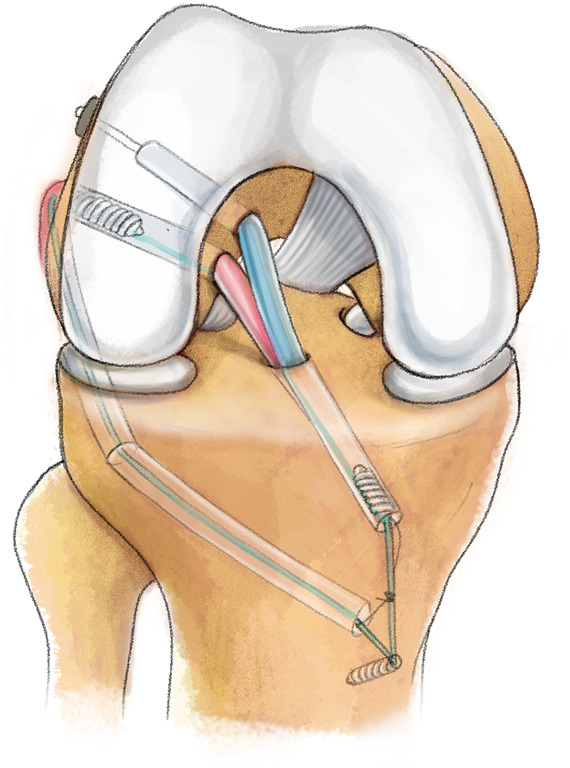
Current double bundle reconstruction technique for ACL. ACL, anterior cruciate ligament.
Over time, several problems were observed with the DB technique, which eventually led to a decline in its popularity and use. Chuaychoosakoon et al. evaluated differences in postoperative pain between SB and DB-ACLR with a hamstring graft. The average postoperative pain scores of the SB group were lower at all time points (88).
By performing a meta-analysis, Oh et al. in 2020 examined the advantages of SB versus DB ACLR in terms of biomechanical outcomes and revealed that both ACLR methods were connected to the restoration of normal knee kinematics. Regarding anteroposterior stability, DB-ACLR is superior to SB-ACLR. Uncertainty persists regarding which technique improves internal rotation laxity and internal rotation laxity (89).
A meta-analysis published in 2019 by Dong et al. included five randomized clinical trials and showed no statistically significant difference between DB and single-bundle (SB) reconstructions (90). In contrast, DB reconstruction requires more surgical time and more fixation material and leads to more technical difficulties during revision (90). It remains unclear whether the increased surgical complexity and trauma associated with this technique can be offset by the anticipated long-term benefits. This suggests that SB techniques may be more suitable than DB techniques for ACL reconstruction (91).
Recently, Yela-Verdú et al. compared the clinical and subjective outcomes of ACL reconstruction using an autologous hamstring DB with an SB after a 10-year follow-up, confirming that ACL reconstruction with an autologous hamstring, both with bundles and DB, shows overall better outcomes compared with the status before surgery (92).
Autograft reconstruction necessitates tissue harvesting from the patient, thereby raising the risks of surgical trauma and morbidity at the donor site as well as lengthening the procedure (93). The avoidance of donor site morbidity, decreased postoperative pain, and shorter operating room times are the main reasons why the usage of allografts has expanded over the past 10 years. Smaller incisions, less donor-site morbidity, greater graft availability, faster postoperative knee range of motion, and shorter surgical times are benefits of using allografts (93). The possibility of an immune response, bacterial infection, and disease transmission from the graft donor are drawbacks. Increased laxity over time, which can cause knee joint instability and failure to resume former levels of activity despite an “intact” graft, is another drawback of using allografts. A recent systematic review compared the clinical outcomes of autografts versus nonirradiated allografts for ACLR reconstruction (93).
Dhillon et al. (94) analyzed a total of 15,502 patients who underwent ACLR with autografts and 1,577 with nonirradiated allografts performing a systematic review. In the autograft group, graft failure ranged from 0% to 9.4% of patients, while in the allograft group, it ranged from 0% to 26.5%. In two studies, younger patients receiving allografts had higher failure rates. In any of the included trials, there were no significant differences in the groups’ patient-reported outcomes, anteroposterior laxity, or objective International Knee Documentation Committee (IKDC) scores (94).
In parallel with surgical reconstruction techniques using grafts, biological reconstruction focusing on the preservation of ACL remnants through the use of cell culture techniques, partial reconstruction, tissue engineering, and gene therapy has gained popularity. Thanks to the improvement of imaging and arthroscopic techniques as well as physiological understanding, it is now possible to successfully perform ACL injuries primarily with augmented repair techniques, including dynamic intraligamentary stabilization (DIS) and internal brace ligament augmentation (IBLA) (95,96). The IBLA technique uses polyethylene tape that is attached to both the femur and tibia to restore the anatomical position of the ACL ligament. The resulting load distribution provides stability that both protects the graft and allows ligamentization (97). The DIS technique also uses polyethylene tape, but it is secured in the tibia by a threaded sleeve with a preloaded spring, from which it is passed through the injured ACL and secured to the lateral distal femur with a button. Patients treated in this manner report near-normal knee function, excellent satisfaction, and, in most cases, an early return to previous activity levels (98). Another alternative is repair with biological substitutes. For this purpose, techniques such as biological scaffolds, platelet-rich plasma (PRP), PRP combined with collagen scaffolds, growth factors, mesenchymal stem cell (MSC) injection, and augmentation are used. These procedures all have in common that they accelerate repair and regeneration through the presence of MSCs (99).
An example of a biological scaffold is the bridge-enhanced anterior cruciate ligament repair (BEAR) technique, also known as bridge-enhanced ACL repair (100). In this procedure, the repair is performed with a suture in combination with a hyophilic extracellular matrix scaffold consisting mainly of extracellular matrix proteins, including collagen, derived from bovine tissue, and stored in the gap between the two torn stumps of the ACL. The patient’s own blood was used for activation. A prospective, multicenter, randomized trial recently compared patients treated with BEAR with patients who underwent ACLR with autografts. At the 2-year follow-up, the BEAR group had a significantly higher mean hamstring muscle strength index than the ACLR group. In addition, 14% of the BEAR group and 6% of the ACLR group had a reinjury that required a second ipsilateral ACL surgical procedure (101,102).
The goal of PRP augmentation is to help the graft mature, but the results are inconclusive. The lack of evidence is thought to be related to differences in harvesting, preparation, and injection site, as well as differences in patient biology. Figueroa et al. published a review of 516 patients on this topic, and the group that received ACL repair plus PRP augmentation showed a tendency for the graft to mature more quickly but had similar patterns of tunnel healing (103). Another therapeutic option in recent years addresses MSCs, which are particularly perivascular and play a role in the area of the ACL (104-106). In vitro studies have shown that bone marrow MSCs have a higher proliferation rate than fibroblasts of the ACL. Together with the use of growth factors, they have the property to positively influence ligamental differentiation. Studies in humans confirming these findings are sporadic to date (107-109). Gobbi et al. reported a technique in which they repaired proximal partial ACL tears by suturing in combination with microfracturing (110). In another study, they investigated the additional injection of PRP glue at the tear site. After half the time, 78% of the athletes were able to resume their sports activities, and the 5-year survival rate was 90% (111). Centeno et al. performed a study in which patients were treated by fluoroscopically guided injection of a platelet lysate, PRP, and bone marrow-derived stem cells. Seventy percent of patients showed changes suggestive of ligament healing on magnetic resonance imaging evaluation at the 3-month follow-up (112). Mahapatra et al. concluded in their recent review of ACL repairs that these techniques show promising results in selected patient groups and should be considered primarily for Sherman type 1 ACL tears with excellent tissue quality in the acute phase to improve the biological joint environment, i.e., with a suture system enhanced by PRP or MSCs (113).
After ACLR, the remodeling of the repaired graft ligament and maintenance of the knee joint’s long-term stability depend on the tendon’s osseointegration and revascularization (114). In beagles, PRP was used to treat ACL grafts. Xie et al. found that PRP changes the expression of some target genes, particularly during the early stages of graft remodeling. The authors also found that PRP may promote revascularization and reinnervation, which may help to explain why PRP has an enhanced effect on ACL graft maturation. However, when graft integration and maturation were measured using magnetic resonance scores, they did not discover any appreciable differences between the two groups (115).
A surgical management “pendulum swing” away from an exclusively mechanocentric focus on ACL reconstruction to increasing consideration of a biocentric repair approach has been sparked by the knowledge base surrounding physiologically mediated tissue healing enhancement (116,117). The more intact neurosensory system of an ACL repair may enable speedier, more accurate neuromuscular activation responses, more robust fast twitch muscle fiber viability, joint position sensing, and kinesthesia, provided it can effectively replicate nonimpaired biomechanical function (118).
In 2013, Claes et al. reported the discovery of a new ligament in the knee that could completely change the treatment of knee injuries (119). This publication led to increased attention to the anterolateral structures of the knee. Claes et al. coined the term anterolateral ligament (ALL), and subsequent anatomic, biomechanical, and clinical studies provided the impulse for a change in the usual treatment approach (120,121). It should be noted that after the American Orthopedic Society of Sports Medicine (AOSSM) consensus conference at Snowmass in 1989, lateral extra-articular procedures (LEAPs), including the previously popular Lemaire and MacIntosh procedures, were almost completely abandoned in the United States because clinical studies failed to demonstrate significant benefit, and complications such as postoperative stiffness and overuse could not be clearly excluded. However, some European centers, particularly in France and Italy, continued to adhere to these procedures (122). Due to renewed interest in LEAPs, these techniques have also been reintroduced in the United States in recent years. The results of a 2017 survey of AOSSM members showed that approximately 40% of respondents had recently used LEAPs at the time of ACLR. Anatomic ALL reconstruction (ALLR) with HT autograft or allograft was the most commonly performed technique (48.2%), followed by the Lemaire or modified Lemaire technique (20.4%). Comparability between historically poor outcomes and current successes is difficult due to only a few published data in the past (123). The first published clinical results of ALLR and combined ACL care date from 2015 (124). The intent of these modifications is to significantly improve the primary restriction of rotational laxity of the knee after ACL injury (125). Kinematic studies have demonstrated that anatomic ACL reconstruction and anterolateral reconstruction are synergistic in controlling pivot displacement (Figure 8) (126-130). A brief summary of the ACL history is reported in Table 1.
Figure 8.
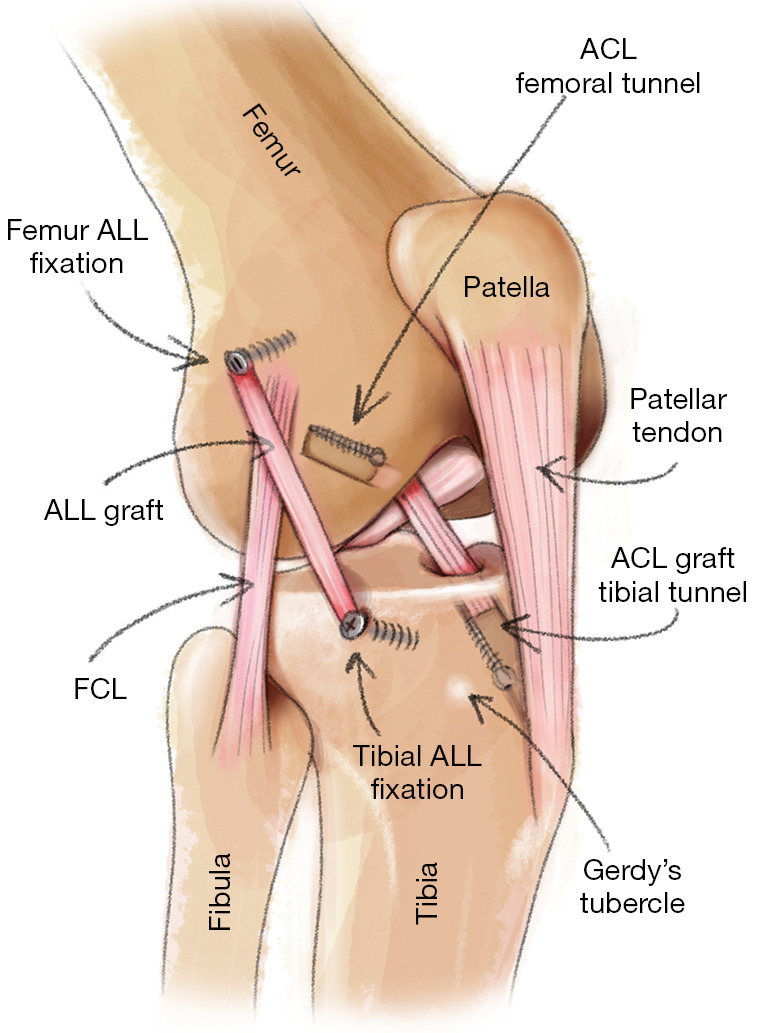
ALLR techniques with one bundle. ACL, anterior cruciate ligament; ALL, anterolateral ligament; FCL, fibular collateral ligament; ALLR, ALL reconstruction.
Table 1. Brief history of ACL reconstruction.
| Year | Author | Technique | Outcomes |
|---|---|---|---|
| 1895 (published in 1903) | Robson AW (14) | Suturing femoral site | Good stability at 8-year |
| 1926 | Perthes G (16) | Sutured the ligament to the bone using a bronze and aluminium wire | Excellent results with this technique at 1–4 years in three patients |
| 1903 | Lange F (19) | Stabilised ACL with HTs and extra-articularly positioned “artificial ligaments made of silk” | 4 cases of ACL deficiency |
| 1917 | Groves EWH (22) | Used fascia lata graft | 23 promising cases |
| 1920 | Putti V (26) | ACL collateral ligaments reconstruction using flaps of the fascia lata | Patient was able to walk again 5 months postoperatively |
| 1933 | Lange M (20) | Silk augmented with ilio-tibial band | Clinical success |
| 1934 | Galeazzi R (27) | Hamstring autograft | 3 cases at 18 months: stable knee with full extension and only a mild reduction of flexion |
| 1936 | Campbell W (32) | “Tibial graft” consisting of the medial third of the patellar tendon, part of the QT, and the prepatellar retinaculum | 53% (9 of 17) of operated patients had an excellent outcome and were able to return to sports within 6 to 10 weeks after surgery |
| 1957 | D’Aubigne RM (29) | Revisited Galeazzi’s method using a pedicled semitendinosus autograft and passed gracilis autograft through a transfemoral tunnel | 55 cases with good success |
| 1963 | Jones KG (33) | Reconstruction of the ACL using the central one-third of the patellar ligament | – |
| 1972 | Keyl W (76) | Anatomic reconstruction technique for the first time, using two separate ACL bundles | – |
| 1976 | Kennedy JC (67) | Kennedy-LAD: a synthetic tape made of polypropylene | Both acute repair and repair with the LAD failed in up to 30% of cases, and the authors hence discouraged any form of repair other than autograft reconstruction |
| 1977 and 1979 | Marshall JL and MacIntosh DL (18,37) | QT substitution technique, which involves one-third of the entire central extensor mechanism, with a large portion of prepatellar aponeurotic tissue | 130 cases with promising good results |
| 1980 | Puddu G (53) | Hamstring harvested proximally, widening the tibial tunnel with an additional joint opening positioned entirely medially, and the internal rotation effect of the semitendinosus was preserved | 12 patients at 8 months with stable knee |
| 1982 | Dandy DJ (44) | First arthroscopic ACL reconstruction using a synthetic graft | 8 patients with good results at 1 year |
| 1982 | Lipscomb AB (54) | Combined the semitendinosus and gracilis tendon autografts | 51 patients, 26.2 months of follow-up; hamstring strength was found to average 99% compared to the normal knee |
| 1984 | Blauth W (62) | Central QT graft with a bone plug | 53 patients with apparently good results |
| 1988 | Friedman MJ (56) | Four ligament strands | Despite several smaller modifications, set the standard for ACL reconstruction with hamstrings for the next 25 years |
| 1998 | Marcacci M (60) | Over-the-top technique | 40 patients; 36 months. Excellent clinical score, full range of motion, 100% return to sport |
| 1999 | Muneta T (82) | Revised DB technique | 54 patients, 2 years of follow-up. two-bundle procedure showed a better trend with respect to anterior stability compared with the SB technique under the same aggressive rehabilitation |
ACL, anterior cruciate ligament; HT, hamstring tendon; QT, quadriceps tendon; LAD, ligament augmentation device; DB, double-bundle; SB, single-bundle.
Advantages and disadvantages of TT, anteromedial portal (AMP), and OI
The location of the ACL femoral tunnel or socket is one of many factors that affect the outcome of knee ACL surgical reconstruction, and there are numerous techniques for creating the ACL femoral socket, including four primary techniques: TT, anteromedial portal (AMP), OI, and OI retrograde drilling (RD). Before 10 years ago, arthroscopy surgeons virtually exclusively used the TT approach to create the ACL femoral socket. Unconstrained or “independent” ACL femoral socket building procedures have grown in favor, but more current ACL work has concentrated on ACL femoral insertional “anatomic” restoration. Independent techniques are said to produce more anatomically precise ACL femoral placement. A recent systematic review analyzed the risks, benefits, advantages, and disadvantages of the TT, AMP, OI, and RD techniques for creating the ACL femoral socket (131).
TT technique advantages/disadvantages
Advantages: less surgical discomfort and morbidity, improved aesthetics without lateral incisions, shorter surgical times, parallel bone tunnels, the ability to center tunnels in footprints, all-inside techniques with RD, the elimination of screw divergence, increased graft tensioning when advancing retrograde screws—all of these features make surgery less painful and difficult technically.
Disadvantages: inability to freely position the femoral tunnel, enlargement of the bone tunnel, potential violation of the posterior cortical wall, posterior cruciate ligament impingement, interference screw-bone divergence, damage to the graft during fixation, vertical tunnel placement leading to rotational instability, graft-tunnel length mismatch, elliptical hole in the lateral wall of the notch from the vertical tunnel, anatomic femoral tunnel compromises the tibial tunnel, fluid leakage through the tibial tunnel, greater long-term osteoarthritis than AMP, graft slippage, increased graft stress, excessive femoral external (tibial internal) rotation at mid-stance, and greater anterior femoral translation in swing phase (131).
AMP technique advantages/disadvantages
Advantages: independent placement of femoral and tibial tunnels; more accurate and anatomic horizontal placement of ACL femoral insertion; preservation of remaining ACL fibers to allow augmentation; tunnel placement independent of graft type, fixation devices, or tunnel guides; flexibility in performing SB or DB reconstruction in primary or revision settings; allowing parallel placement of interference screws; decreasing tunnel widening; allowing all-inside procedures; drilling in hyperflexion to reduce risk of posterior-wall blowout; allowing figure-of-4 position without need for an assistant and hyperflexion; improving visualization during drilling without loss of joint distention due to tibial tunnel fluid extravasation.
Disadvantages: technically challenging, poor visibility, excessive angulation in the sagittal plane, posterior-wall blowout and potential damage to the posterior articular cartilage, distal/inferior beath pin exit with potential damage to the common peroneal nerve, short or bicortical sockets that may limit fixation options, difficulty seating endoscopic aimer, inability to maintain aimer in hyperflexed knee, portal tightening in hyperflexion, iatrogenic damage to medial femoral condyle cartilage, challenges with reamer passage, low portal placement that could damage the anterior horn of the medial meniscus, challenges with graft fixation device passage, hyperflexion necessitating a helper to stabilise the knee, increased graft failure rates and revision risk when compared to TT, and femoral guide breakage (131).
OI technique advantages/disadvantages
Advantages: decreased bone absorption at the bone-graft interface, predictable near-anatomic placement of the femoral tunnel, elimination of graft-tunnel mismatch, avoidance of posterior-wall blowout, ease of use for revision ACL procedures, contact pressure evenly distributed over anterior and lateral portions of the femoral tunnel, and posterior placement of the graft and horizontal femoral tunnel that restores natural knee kinematics.
Disadvantages: greater surgical morbidity with lateral incision, increased graft abrasion at the intraarticular borders of the tunnel, lengthier surgery, more expensive, and worse cosmetic results (131).
OI retrogade drilling advantages/disadvantages
Advantages: unrestricted anatomic placement within the footprint, no fluid leakage, no need for hyperflexion, use of a shorter graft, improved cosmetics, allowing all-epiphyseal technique in skeletally immature patients, being less technically demanding, having an adequate tunnel length, reducing posterior cortical damage with interference screw fixation, allowing measurement of the femoral interosseous distance prior to socket creation, and second-generation adjustable graft-loop buttons allowing.
Disadvantages: horizontal tunnels provide sharp angles that could lead to increased graft wear, need for intraoperative fluoroscopy for all-epiphyseal drilling, lengthen surgery times, and raise fluoroscopy expenditures (131).
Future perspectives
Ribbon-like graft
After removing the synovial membrane, the ACL, including its femoral and tibial insertions, looks flat and “ribbon-like” (132). Therefore, the fundamental idea behind this method of ACL reconstruction is to develop tunnel forms that are more similar to the original insertions rather than using circular tunnels. In vivo investigations comparing ACL-reconstructed patients with matched controls in pivoting and cutting activities revealed that SB ACL reconstruction surgery was not able to completely restore rotational kinematics and stability (133). Two ACL fiber bundles were seen in biomechanical data, each with a different pattern of length changes during knee motion and a corresponding variance in tension (133). However, at present, ACL restoration utilizing rectangular bone tunnels could demonstrate equivalent kinematics. This method may have fascinating biological advantages in addition to biomechanical advantages. The anatomy and makeup of the direct insertion site are not replicated since the graft in ACL restoration is inserted into bone tunnels (133). Instead, the graft generates perpendicular collagen bundles to offset the shear pressures and heals with a fibrovascular scar at the graft-tunnel interface, connecting the tendon to the bone. These bundles mimic an indirect insertion site’s Sharpey fibers. The strength of the graft pull-out is positively connected with their size and number (133,134). Only after 4 weeks does revascularization begin, moving from the graft’s edges to its center. The production of Sharpey-like fibers and vascularization can occur on an enlarged surface, but the distance to the center section of the graft is still constrained because the contact area of a flat ACL graft is approximately three times larger in relation to its volume than one that is spherical (134). The goal is to avoid central necrosis, which is caused by a reduced distance for diffusion during the early stages of graft healing. This beneficial biological impact on tendon-to-bone repair employing a flattened bone tunnel may have been demonstrated in a recent animal study. A stronger regenerated tendon-bone interface and quicker tendon-to-bone healing were the outcomes of the flattened bone tunnel (134).
Machine learning curve and artificial intelligence
Recently, there has been an increased focus on the application of artificial intelligence and machine learning to improve predictive capability within numerous sectors of medicine, including orthopedic surgery (135). These cutting-edge statistical methods use computer algorithms to simulate intricate interactions between variables, which could improve the accuracy of the prediction. To discover the links to the intended outcome measure, machine learning analyses can take into account all potential interactions between variables in a database. The predictive algorithm can then be developed using the parameters that are significant for forecasting results. Frequently, only a small amount of explicit and direct human computer programming is needed, and the resulting algorithms can be utilized to forecast the outcome for a certain patient in the future (135,136).
A recent study used machine learning analysis to identify the most important risk factors associated with subjective failure of primary ACL reconstruction and develop a clinically meaningful model for predicting subjective failure of primary ACL reconstruction. The authors reached the conclusion that machine learning analysis may reasonably estimate subjective failure probability after ACL reconstruction. This method helps the development of a user-friendly point-of-care risk stratification calculator for clinics. When addressing preoperative outcome expectations, clinicians can utilize this calculator to predict subjective failure probability at a patient-specific level (136).
Conclusions
The history of ACL surgery shows a unique effort and continuous research over an enormous period of time with the aim of constantly optimizing the available treatment options. The primary goal is always an individual and effective treatment that allows the restoration of a completely stable joint, the shortest possible and painless regeneration, and the resumption of daily and sporting life. Thus, modern ACL surgery has the common goal of restoring normal knee kinematics and function, which may ultimately help reduce the prevalence of postoperative joint degeneration.
Supplementary
The article’s supplementary files as
Acknowledgments
Special thanks to Silvia Provantini for original medical artworks.
Funding: None.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Footnotes
Peer Review File: Available at https://atm.amegroups.com/article/view/10.21037/atm-23-87/prf
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://atm.amegroups.com/article/view/10.21037/atm-23-87/coif). RDA serves as an unpaid editorial board member of Annals of Translational Medicine from November 2022 to October 2024. The other authors have no conflicts of interest to declare.
References
- 1.Chambat P. ACL tear. Orthop Traumatol Surg Res 2013;99:S43-52. 10.1016/j.otsr.2012.11.012 [DOI] [PubMed] [Google Scholar]
- 2.Musahl V, Engler ID, Nazzal EM, et al. Current trends in the anterior cruciate ligament part II: evaluation, surgical technique, prevention, and rehabilitation. Knee Surg Sports Traumatol Arthrosc 2022;30:34-51. 10.1007/s00167-021-06825-z [DOI] [PubMed] [Google Scholar]
- 3.Schindler OS. Surgery for anterior cruciate ligament deficiency: a historical perspective. Knee Surg Sports Traumatol Arthrosc 2012;20:5-47. 10.1007/s00167-011-1756-x [DOI] [PubMed] [Google Scholar]
- 4.Galen C. On the Usefulness of the Parts of the Body. Ithaca: Cornell University Press, 1968. [Google Scholar]
- 5.Snook GA. A short history of the anterior cruciate ligament and the treatment of tears. Clin Orthop Relat Res 1983;(172):11-3. 10.1097/00003086-198301000-00004 [DOI] [PubMed] [Google Scholar]
- 6.Davarinos N, O'Neill BJ, Curtin W. A brief history of anterior cruciate ligament reconstruction. Advances in Orthopedic Surgery 2014. doi: 10.1155/2014/706042. 10.1155/2014/706042 [DOI] [Google Scholar]
- 7.Weber W, Weber E. Mechanik der menschlichen Gehwerkzeuge: eine anatomisch-physiologische Untersuchung. Göttingen: Dieterichschen Buchhandlung, 1836. [Google Scholar]
- 8.White AE, Van Nest D, Tjoumakaris FP, et al. Journey around the Notch: A Systematic Review on the History of ACL Reconstruction in the United States. J Knee Surg 2022;35:61-71. 10.1055/s-0040-1712947 [DOI] [PubMed] [Google Scholar]
- 9.Weber W, Weber E. Ueber die Mechanik der menschlichen Gehwerkzeuge, nebst der Beschreibung eines Versuchs über das Herausfallen des Schenkelkopfs aus der Pfanne im luftverdünnten Raume. Annalen der Physik 1837;116:1-13. 10.1002/andp.18371160102 [DOI] [Google Scholar]
- 10.Bonnet A. Traité des maladies des articulations. Paris: Baillière, 1845. [Google Scholar]
- 11.Stark J. Two Cases of Rupture of the Crucial Ligament of the Knee-Joint. Edinb Med Surg J 1850;74:267-71. [PMC free article] [PubMed] [Google Scholar]
- 12.Noulis GC. Entorse du genou. Paris: Fac Med, 1875. [Google Scholar]
- 13.Segond P. Recherches cliniques et expérimentales sur les épanchements sanguins du genou par entorse. Paris: Aux Bureaux du Progrès Medical, 1879. [Google Scholar]
- 14.Robson AW. VI. Ruptured Crucial Ligaments and their Repair by Operation. Ann Surg 1903;37:716-8. [PMC free article] [PubMed] [Google Scholar]
- 15.Battle WH. A case after open section of the knee joint for irreducible traumatic dislocation. Clin Soc London Trans 1900;33:232. [Google Scholar]
- 16.Perthes G. Über die Wiederbefestigung des abgerissenen vorderen Kreuzbandes im Kniegelenk. Zentralbl Chir 1926;53:866-72. [Google Scholar]
- 17.Goetjes H. Über verletzungen der ligamenta cruciata des kniegelenks. Deutsche Zeitschrift für Chirurgie 1913;123:221-89. 10.1007/BF02797557 [DOI] [Google Scholar]
- 18.Marshall JL, Warren RF, Wickiewicz TL, et al. The anterior cruciate ligament: a technique of repair and reconstruction. Clin Orthop Relat Res 1979;(143):97-106. 10.1097/00003086-197909000-00014 [DOI] [PubMed] [Google Scholar]
- 19.Lange F. Uber die sehnenplastik. Verh Dtsch Orthop Ges 1903;2:10. [Google Scholar]
- 20.Lange M. Verhandlungen der Deutschen Orthoädischen Gesellschaft. Mannheim: Künstliche Gelenkbänder aus Seide Siebenundzwanzigster Kongress der Deutschen Orthopädischen Gesellschaft; 1933:27:256-8. [Google Scholar]
- 21.Lange F. Künstliche Bänder aus Seide. Münch Med Wochenschr 1907;17:834-6. [Google Scholar]
- 22.Groves EWH. Operation for the repair of the crucial ligaments. Lancet 1917;190:674-6. 10.1016/S0140-6736(01)52502-7 [DOI] [Google Scholar]
- 23.Hamner DL, Brown CH, Jr, Steiner ME, et al. Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-57. 10.2106/00004623-199904000-00013 [DOI] [PubMed] [Google Scholar]
- 24.Järvinen M, Kannus P, Johnson RJ. How to treat knee ligament injuries? Ann Chir Gynaecol 1991;80:134-40. [PubMed] [Google Scholar]
- 25.Groves EWH. The crucial ligaments of the knee-joint: Their function, rupture, and the operative treatment of the same. Journal of British Surgery 1919;7:505-15. 10.1002/bjs.1800072809 [DOI] [Google Scholar]
- 26.Putti V. La ricostruzione dei legamenti crociati del ginocchio. Chir Org Mov 1920;4:96. [Google Scholar]
- 27.Galeazzi R. La ricostruzione dei legamenti crociati del ginocchio. Atti e memorie della Società Lombarda di Chirurgia 1934.
- 28.Sebastin SJ, Chung KC. A historical report on Riccardo Galeazzi and the management of Galeazzi fractures. J Hand Surg Am 2010;35:1870-7. 10.1016/j.jhsa.2010.08.032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.D'Aubigne RM, Ramadier JO, Fayt P. Lesions of the ligaments of the knee; 55 surgical cases. Wiederherstellungschir Traumatol 1957;4:156-80. [PubMed] [Google Scholar]
- 30.Lange M. Critical account on the question of conservative versus operative treatment for severe knee ligament injuries. Reconstr Surg Traumatol 1957;4:197-222. [PubMed] [Google Scholar]
- 31.Cho KO. Reconstruction of the anterior cruciate ligament by semitendinosus tenodesis. J Bone Joint Surg Am 1975;57:608-12. 10.2106/00004623-197557050-00003 [DOI] [PubMed] [Google Scholar]
- 32.Campbell W. Repair of the ligaments of the knee. Report of a new operation for repair of the anterior cruciate ligament. Surgery 1936;62:964-8. [Google Scholar]
- 33.Jones KG. Reconstruction of the anterior cruciate ligament. A technique using the central one-third of the patellar ligament. J Bone Joint Surg Am 1963;45:925-32. 10.2106/00004623-196345050-00003 [DOI] [PubMed] [Google Scholar]
- 34.Maffulli N, Oliviero A. Review of Jones (1963) on 'Reconstruction of the anterior cruciate ligament. A technique using the central one-third of the patellar ligament'. J ISAKOS 2019;4:338-44. 10.1136/jisakos-2019-000374 [DOI] [Google Scholar]
- 35.Brückner H. Eine neue methode der kreuzbandplastik. Chirurg 1966;37:413-4. [PubMed] [Google Scholar]
- 36.Franke K. Clinical experience in 130 cruciate ligament reconstructions. Orthop Clin North Am 1976;7:191-3. 10.1016/S0030-5898(20)31182-2 [DOI] [PubMed] [Google Scholar]
- 37.MacIntosh DL. A follow-up study and evaluation of "over the top" repair of acute tears of the anterior cruciate ligament. J Bone Joint Surg B 1977;59:511. [Google Scholar]
- 38.Clancy WG, Jr, Nelson DA, Reider B, et al. Anterior cruciate ligament reconstruction using one-third of the patellar ligament, augmented by extra-articular tendon transfers. J Bone Joint Surg Am 1982;64:352-9. 10.2106/00004623-198264030-00004 [DOI] [PubMed] [Google Scholar]
- 39.Dejour H, Dejour D, Aït Si Selmi T. Chronic anterior laxity of the knee treated with free patellar graft and extra-articular lateral plasty: 10-year follow-up of 148 cases. Rev Chir Orthop Reparatrice Appar Mot 1999;85:777-89. [PubMed] [Google Scholar]
- 40.Lambert KL. Vascularized patellar tendon graft with rigid internal fixation for anterior cruciate ligament insufficiency. Clin Orthop Relat Res 1983;(172):85-9. 10.1097/00003086-198301000-00016 [DOI] [PubMed] [Google Scholar]
- 41.Kurosaka M, Yoshiya S, Andrish JT. A biomechanical comparison of different surgical techniques of graft fixation in anterior cruciate ligament reconstruction. Am J Sports Med 1987;15:225-9. 10.1177/036354658701500306 [DOI] [PubMed] [Google Scholar]
- 42.Jackson RW, Abe I. The role of arthroscopy in the management of disorders of the knee. An analysis of 200 consecutive examinations. J Bone Joint Surg Br 1972;54:310-22. 10.1302/0301-620X.54B2.310 [DOI] [PubMed] [Google Scholar]
- 43.Dandy DJ, Jackson RW. The impact of arthroscopy on the management of disorders of the knee. J Bone Joint Surg Br 1975;57:346-8. 10.1302/0301-620X.57B3.346 [DOI] [PubMed] [Google Scholar]
- 44.Dandy DJ, Flanagan JP, Steenmeyer V. Arthroscopy and the management of the ruptured anterior cruciate ligament. Clin Orthop Relat Res 1982;(167):43-9. 10.1097/00003086-198207000-00008 [DOI] [PubMed] [Google Scholar]
- 45.Bach BR, Jr, Levy ME, Bojchuk J, et al. Single-incision endoscopic anterior cruciate ligament reconstruction using patellar tendon autograft. Minimum two-year follow-up evaluation. Am J Sports Med 1998;26:30-40. 10.1177/03635465980260012201 [DOI] [PubMed] [Google Scholar]
- 46.Buss DD, Warren RF, Wickiewicz TL, et al. Arthroscopically assisted reconstruction of the anterior cruciate ligament with use of autogenous patellar-ligament grafts. Results after twenty-four to forty-two months. J Bone Joint Surg Am 1993;75:1346-55. 10.2106/00004623-199309000-00009 [DOI] [PubMed] [Google Scholar]
- 47.Bach BR, Jr, Jones GT, Sweet FA, et al. Arthroscopy-assisted anterior cruciate ligament reconstruction using patellar tendon substitution. Two- to four-year follow-up results. Am J Sports Med 1994;22:758-67. 10.1177/036354659402200606 [DOI] [PubMed] [Google Scholar]
- 48.Marans HJ, Hendrix MR, Paterson RS. A new femoral drill guide for arthroscopically assisted anterior cruciate ligament replacement. Arthroscopy 1992;8:234-8. 10.1016/0749-8063(92)90042-A [DOI] [PubMed] [Google Scholar]
- 49.McGuire DA, Hendricks SD, Grinstead GL. Use of an endoscopic aimer for femoral tunnel placement in anterior cruciate ligament reconstruction. Arthroscopy 1996;12:26-31. 10.1016/S0749-8063(96)90215-7 [DOI] [PubMed] [Google Scholar]
- 50.Kartus J, Magnusson L, Stener S, et al. Complications following arthroscopic anterior cruciate ligament reconstruction. A 2-5-year follow-up of 604 patients with special emphasis on anterior knee pain. Knee Surg Sports Traumatol Arthrosc 1999;7:2-8. 10.1007/s001670050112 [DOI] [PubMed] [Google Scholar]
- 51.Shelbourne KD, Trumper RV. Preventing anterior knee pain after anterior cruciate ligament reconstruction. Am J Sports Med 1997;25:41-7. 10.1177/036354659702500108 [DOI] [PubMed] [Google Scholar]
- 52.Macey HB. New operative procedures for the repair of ruptured cruciate ligaments of the knee joint. Surg Gynecol Obstet 1939;69:108-9. [Google Scholar]
- 53.Puddu G. Method for reconstruction of the anterior cruciate ligament using the semitendinosus tendon. Am J Sports Med 1980;8:402-4. 10.1177/036354658000800603 [DOI] [PubMed] [Google Scholar]
- 54.Lipscomb AB, Johnston RK, Snyder RB, et al. Evaluation of hamstring strength following use of semitendinosus and gracilis tendons to reconstruct the anterior cruciate ligament. Am J Sports Med 1982;10:340-2. 10.1177/036354658201000603 [DOI] [PubMed] [Google Scholar]
- 55.Martin SD, Martin TL, Brown CH. Anterior cruciate ligament graft fixation. Orthop Clin North Am 2002;33:685-96. 10.1016/S0030-5898(02)00023-8 [DOI] [PubMed] [Google Scholar]
- 56.Friedman MJ. Arthroscopic semitendinosus (gracilis) reconstruction for anterior cruciate ligament deficiency. Tech Orthop 1988;2:74-80. 10.1097/00013611-198801000-00012 [DOI] [Google Scholar]
- 57.Howell MSM. Arthroscopically assisted technique for preventing roof impingement of an anterior cruciate ligament graft illustrated by the use of an autogenous double-looped semitendinosus and gracilis graft. Oper Tech Sports Med 1993;1:58-65. 10.1016/S1060-1872(10)80030-9 [DOI] [Google Scholar]
- 58.Rosenberg TD. Technique for endoscopic method of ACL reconstruction. Acufex Microsurgical, 1993. [Google Scholar]
- 59.Pinczewski L. Two year results of endoscopic reconstruction of isolated ACL ruptures with quadruple hamstring tendon autograft and interference screw fixation. San Francisco: AAOS Annual Meeting, 1997. [Google Scholar]
- 60.Marcacci M, Zaffagnini S, Iacono F, et al. Arthroscopic intra- and extra-articular anterior cruciate ligament reconstruction with gracilis and semitendinosus tendons. Knee Surg Sports Traumatol Arthrosc 1998;6:68-75. 10.1007/s001670050075 [DOI] [PubMed] [Google Scholar]
- 61.Slone HS, Romine SE, Premkumar A, et al. Quadriceps tendon autograft for anterior cruciate ligament reconstruction: a comprehensive review of current literature and systematic review of clinical results. Arthroscopy 2015;31:541-54. 10.1016/j.arthro.2014.11.010 [DOI] [PubMed] [Google Scholar]
- 62.Blauth W. 2-strip substitution-plasty of the anterior cruciate ligament with the quadriceps tendon. Unfallheilkunde 1984;87:45-51. [PubMed] [Google Scholar]
- 63.Fulkerson JP, Langeland R. An alternative cruciate reconstruction graft: the central quadriceps tendon. Arthroscopy 1995;11:252-4. 10.1016/0749-8063(95)90078-0 [DOI] [PubMed] [Google Scholar]
- 64.Herbawi F, Lozano-Lozano M, Lopez-Garzon M, et al. A Systematic Review and Meta-Analysis of Strength Recovery Measured by Isokinetic Dynamometer Technology after Anterior Cruciate Ligament Reconstruction Using Quadriceps Tendon Autografts vs. Hamstring Tendon Autografts or Patellar Tendon Autografts. Int J Environ Res Public Health 2022;19:6764. 10.3390/ijerph19116764 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Hurley ET, Mojica ES, Kanakamedala AC, et al. Quadriceps tendon has a lower re-rupture rate than hamstring tendon autograft for anterior cruciate ligament reconstruction - A meta-analysis. J ISAKOS 2022;7:87-93. 10.1016/j.jisako.2021.10.001 [DOI] [PubMed] [Google Scholar]
- 66.Mouarbes D, Menetrey J, Marot V, et al. Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Outcomes for Quadriceps Tendon Autograft Versus Bone-Patellar Tendon-Bone and Hamstring-Tendon Autografts. Am J Sports Med 2019;47:3531-40. 10.1177/0363546518825340 [DOI] [PubMed] [Google Scholar]
- 67.Kennedy JC, Willis RB. Synthetic cruciate ligaments: preliminary report. J Bone Jt Surg 1976;58:142. [Google Scholar]
- 68.Jenkins DH. The repair of cruciate ligaments with flexible carbon fibre. A longer term study of the induction of new ligaments and of the fate of the implanted carbon. J Bone Joint Surg Br 1978;60-B:520-2. 10.1302/0301-620X.60B4.711800 [DOI] [PubMed] [Google Scholar]
- 69.Dandy DJ, O'Carroll PF. Arthroscopic surgery of the knee. Br Med J (Clin Res Ed) 1982;285:1256-8. 10.1136/bmj.285.6350.1256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Pinar H, Gillquist J. Dacron augmentation of a free patellar tendon graft: a biomechanical study. Arthroscopy 1989;5:328-30. 10.1016/0749-8063(89)90151-5 [DOI] [PubMed] [Google Scholar]
- 71.Dahlstedt L, Dalén N, Jonsson U. Goretex prosthetic ligament vs. Kennedy ligament augmentation device in anterior cruciate ligament reconstruction. A prospective randomized 3-year follow-up of 41 cases. Acta Orthop Scand 1990;61:217-24. 10.3109/17453679008993504 [DOI] [PubMed] [Google Scholar]
- 72.Taylor SA, Khair MM, Roberts TR, et al. Primary Repair of the Anterior Cruciate Ligament: A Systematic Review. Arthroscopy 2015;31:2233-47. 10.1016/j.arthro.2015.05.007 [DOI] [PubMed] [Google Scholar]
- 73.Arnold MP, Calcei JG, Vogel N, et al. ACL Study Group survey reveals the evolution of anterior cruciate ligament reconstruction graft choice over the past three decades. Knee Surg Sports Traumatol Arthrosc 2021;29:3871-6. 10.1007/s00167-021-06443-9 [DOI] [PubMed] [Google Scholar]
- 74.Grassi A, Carulli C, Innocenti M, et al. New Trends in Anterior Cruciate Ligament Reconstruction: A Systematic Review of National Surveys of the Last 5 Years. Joints 2018;6:177-87. 10.1055/s-0038-1672157 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Chambat P, Vargas R, Fayard JM, et al. Résultat des reconstructions du ligament croisé antérieur sous contrôle arthroscopique avec un recul supérieur à 15 ans. In: Chambat P, Neyret P. editors. Le genou et le sport du ligament à la prothèse. Sauramps Médical 2008;1:147-52. [Google Scholar]
- 76.Keyl W, Viernstein K. Operative Wiederherstellung des Kniebandapparates beim Sportier. Fortschr Med 1972;80:1026. [PubMed] [Google Scholar]
- 77.Viernstein K, Keyl W. Operationen am Kniegelenk. Chirurgische Operationslehre 1973;4:2. [Google Scholar]
- 78.Mott HW. Semitendinosus anatomic reconstruction for cruciate ligament insufficiency. Clin Orthop Relat Res 1983;(172):90-2. 10.1097/00003086-198301000-00017 [DOI] [PubMed] [Google Scholar]
- 79.Buda R, Ferruzzi A, Vannini F, et al. Augmentation technique with semitendinosus and gracilis tendons in chronic partial lesions of the ACL: clinical and arthrometric analysis. Knee Surg Sports Traumatol Arthrosc 2006;14:1101-7. 10.1007/s00167-006-0117-7 [DOI] [PubMed] [Google Scholar]
- 80.Ochi M, Adachi N, Deie M, et al. Anterior cruciate ligament augmentation procedure with a 1-incision technique: anteromedial bundle or posterolateral bundle reconstruction. Arthroscopy 2006;22:463.e1-5. 10.1016/j.arthro.2005.06.034 [DOI] [PubMed] [Google Scholar]
- 81.Sonnery-Cottet B, Lavoie F, Ogassawara R, et al. Selective anteromedial bundle reconstruction in partial ACL tears: a series of 36 patients with mean 24 months follow-up. Knee Surg Sports Traumatol Arthrosc 2010;18:47-51. 10.1007/s00167-009-0855-4 [DOI] [PubMed] [Google Scholar]
- 82.Muneta T, Sekiya I, Yagishita K, et al. Two-bundle reconstruction of the anterior cruciate ligament using semitendinosus tendon with endobuttons: operative technique and preliminary results. Arthroscopy 1999;15:618-24. 10.1053/ar.1999.v15.0150611 [DOI] [PubMed] [Google Scholar]
- 83.Kondo E, Merican AM, Yasuda K, et al. Biomechanical comparison of anatomic double-bundle, anatomic single-bundle, and nonanatomic single-bundle anterior cruciate ligament reconstructions. Am J Sports Med 2011;39:279-88. 10.1177/0363546510392350 [DOI] [PubMed] [Google Scholar]
- 84.Mae T, Shino K, Miyama T, et al. Single- versus two-femoral socket anterior cruciate ligament reconstruction technique: Biomechanical analysis using a robotic simulator. Arthroscopy 2001;17:708-16. 10.1053/jars.2001.25250 [DOI] [PubMed] [Google Scholar]
- 85.Yagi M, Wong EK, Kanamori A, et al. Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med 2002;30:660-6. 10.1177/03635465020300050501 [DOI] [PubMed] [Google Scholar]
- 86.Tashman S, Collon D, Anderson K, et al. Abnormal rotational knee motion during running after anterior cruciate ligament reconstruction. Am J Sports Med 2004;32:975-83. 10.1177/0363546503261709 [DOI] [PubMed] [Google Scholar]
- 87.Yasuda K, Kondo E, Ichiyama H, et al. Anatomic reconstruction of the anteromedial and posterolateral bundles of the anterior cruciate ligament using hamstring tendon grafts. Arthroscopy 2004;20:1015-25. 10.1016/j.arthro.2004.08.010 [DOI] [PubMed] [Google Scholar]
- 88.Chuaychoosakoon C, Parinyakhup W, Wiwatboworn A, et al. Comparing post-operative pain between single bundle and double bundle anterior cruciate ligament reconstruction: a retrospective study. BMC Musculoskelet Disord 2021;22:753. 10.1186/s12891-021-04635-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Oh JY, Kim KT, Park YJ, et al. Biomechanical comparison of single-bundle versus double-bundle anterior cruciate ligament reconstruction: a meta-analysis. Knee Surg Relat Res 2020;32:14. 10.1186/s43019-020-00033-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Dong Z, Niu Y, Qi J, et al. Long term results after double and single bundle ACL reconstruction: Is there any difference? A meta-analysis of randomized controlled trials. Acta Orthop Traumatol Turc 2019;53:92-9. 10.1016/j.aott.2018.12.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Gobbi A, Mahajan V, Karnatzikos G, et al. Single- versus double-bundle ACL reconstruction: is there any difference in stability and function at 3-year followup? Clin Orthop Relat Res 2012;470:824-34. 10.1007/s11999-011-1940-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Yela-Verdú C, Ares O, Albareda D, et al. Anterior Cruciate Ligament Reconstruction with Autologous Hamstring Single- versus Double-Bundle Graft: A Prospective Study with 10-Year Follow-up. J Knee Surg 2023;36:1043-51. 10.1055/s-0042-1748898 [DOI] [PubMed] [Google Scholar]
- 93.D'Ambrosi R, Giorgino R, Corona K, et al. Hamstring tendon autografts and allografts show comparable clinical outcomes and knee stability after anterior cruciate ligament reconstruction in patients over fifty years old with no signs of osteoarthritis progression. Int Orthop 2022;46:2029-39. 10.1007/s00264-022-05465-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Dhillon J, Kraeutler MJ, Belk JW, et al. Autograft and Nonirradiated Allograft for Anterior Cruciate Ligament Reconstruction Demonstrate Similar Clinical Outcomes and Graft Failure Rates: An Updated Systematic Review. Arthrosc Sports Med Rehabil 2022;4:e1513-21. 10.1016/j.asmr.2022.04.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Kohl S, Evangelopoulos DS, Ahmad SS, et al. A novel technique, dynamic intraligamentary stabilization creates optimal conditions for primary ACL healing: a preliminary biomechanical study. Knee 2014;21:477-80. 10.1016/j.knee.2013.11.003 [DOI] [PubMed] [Google Scholar]
- 96.MacKay G, Anthony IC, Jenkins PJ, et al. Anterior cruciate ligament repair revisited. Preliminary Results of Primary Repair with Internal Brace Ligament Augmentation: A Case Series. Orthop Muscul Syst 2015;4:1-5. [Google Scholar]
- 97.Cook JL, Smith P, Stannard JP, et al. A Canine Arthroscopic Anterior Cruciate Ligament Reconstruction Model for Study of Synthetic Augmentation of Tendon Allografts. J Knee Surg 2017;30:704-11. 10.1055/s-0036-1597618 [DOI] [PubMed] [Google Scholar]
- 98.Henle P, Röder C, Perler G, et al. Dynamic Intraligamentary Stabilization (DIS) for treatment of acute anterior cruciate ligament ruptures: case series experience of the first three years. BMC Musculoskelet Disord 2015;16:27. 10.1186/s12891-015-0484-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Musahl V, Nazzal EM, Lucidi GA, et al. Current trends in the anterior cruciate ligament part 1: biology and biomechanics. Knee Surg Sports Traumatol Arthrosc 2022;30:20-33. 10.1007/s00167-021-06826-y [DOI] [PubMed] [Google Scholar]
- 100.Murray MM, Flutie BM, Kalish LA, et al. The Bridge-Enhanced Anterior Cruciate Ligament Repair (BEAR) Procedure: An Early Feasibility Cohort Study. Orthop J Sports Med 2016;4:2325967116672176. 10.1177/2325967116672176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Murray MM, Kalish LA, Fleming BC, et al. Bridge-Enhanced Anterior Cruciate Ligament Repair: Two-Year Results of a First-in-Human Study. Orthop J Sports Med 2019;7:2325967118824356. 10.1177/2325967118824356 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Murray MM, Fleming BC, Badger GJ, et al. Bridge-Enhanced Anterior Cruciate Ligament Repair Is Not Inferior to Autograft Anterior Cruciate Ligament Reconstruction at 2 Years: Results of a Prospective Randomized Clinical Trial. Am J Sports Med 2020;48:1305-15. 10.1177/0363546520913532 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Figueroa D, Figueroa F, Calvo R, et al. Platelet-rich plasma use in anterior cruciate ligament surgery: systematic review of the literature. Arthroscopy 2015;31:981-8. 10.1016/j.arthro.2014.11.022 [DOI] [PubMed] [Google Scholar]
- 104.Caplan AI. All MSCs are pericytes? Cell Stem Cell 2008;3:229-30. 10.1016/j.stem.2008.08.008 [DOI] [PubMed] [Google Scholar]
- 105.Steinert AF, Kunz M, Prager P, et al. Mesenchymal stem cell characteristics of human anterior cruciate ligament outgrowth cells. Tissue Eng Part A 2011;17:1375-88. 10.1089/ten.tea.2010.0413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Cheng MT, Yang HW, Chen TH, et al. Isolation and characterization of multipotent stem cells from human cruciate ligaments. Cell Prolif 2009;42:448-60. 10.1111/j.1365-2184.2009.00611.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Van Eijk F, Saris DB, Riesle J, et al. Tissue engineering of ligaments: a comparison of bone marrow stromal cells, anterior cruciate ligament, and skin fibroblasts as cell source. Tissue Eng 2004;10:893-903. 10.1089/1076327041348428 [DOI] [PubMed] [Google Scholar]
- 108.Ge Z, Goh JC, Lee EH. The effects of bone marrow-derived mesenchymal stem cells and fascia wrap application to anterior cruciate ligament tissue engineering. Cell Transplant 2005;14:763-73. 10.3727/000000005783982486 [DOI] [PubMed] [Google Scholar]
- 109.Haddad-Weber M, Prager P, Kunz M, et al. BMP12 and BMP13 gene transfer induce ligamentogenic differentiation in mesenchymal progenitor and anterior cruciate ligament cells. Cytotherapy 2010;12:505-13. 10.3109/14653241003709652 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Gobbi A, Bathan L, Boldrini L. Primary repair combined with bone marrow stimulation in acute anterior cruciate ligament lesions: results in a group of athletes. Am J Sports Med 2009;37:571-8. 10.1177/0363546508327141 [DOI] [PubMed] [Google Scholar]
- 111.Gobbi A, Karnatzikos G, Sankineani SR, et al. Biological augmentation of ACL refixation in partial lesions in a group of athletes: results at the 5-year follow-up. Tech Orthop 2013;28:180-4. 10.1097/BTO.0b013e318294ce44 [DOI] [Google Scholar]
- 112.Centeno CJ, Pitts J, Al-Sayegh H, et al. Anterior cruciate ligament tears treated with percutaneous injection of autologous bone marrow nucleated cells: a case series. J Pain Res 2015;8:437-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Mahapatra P, Horriat S, Anand BS. Anterior cruciate ligament repair - past, present and future. J Exp Orthop 2018;5:20. 10.1186/s40634-018-0136-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Mengsteab PY, Conroy P, Badon M, et al. Evaluation of a bioengineered ACL matrix's osteointegration with BMP-2 supplementation. PLoS One 2020;15:e0227181. 10.1371/journal.pone.0227181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Xie X, Zhao S, Wu H, et al. Platelet-rich plasma enhances autograft revascularization and reinnervation in a dog model of anterior cruciate ligament reconstruction. J Surg Res 2013;183:214-22. 10.1016/j.jss.2013.01.020 [DOI] [PubMed] [Google Scholar]
- 116.Zhao F, Hu X, Zhang J, et al. A more flattened bone tunnel has a positive effect on tendon-bone healing in the early period after ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 2019;27:3543-51. 10.1007/s00167-019-05420-7 [DOI] [PubMed] [Google Scholar]
- 117.Looney AM, Leider JD, Horn AR, et al. Bioaugmentation in the surgical treatment of anterior cruciate ligament injuries: A review of current concepts and emerging techniques. SAGE Open Med 2020;8:2050312120921057. 10.1177/2050312120921057 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.McRobb J, Kamil KH, Ahmed I, et al. Influence of platelet-rich plasma (PRP) analogues on healing and clinical outcomes following anterior cruciate ligament (ACL) reconstructive surgery: a systematic review. Eur J Orthop Surg Traumatol 2023;33:225-53. 10.1007/s00590-021-03198-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Claes S, Vereecke E, Maes M, et al. Anatomy of the anterolateral ligament of the knee. J Anat 2013;223:321-8. 10.1111/joa.12087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Dodds AL, Halewood C, Gupte CM, et al. The anterolateral ligament: Anatomy, length changes and association with the Segond fracture. Bone Joint J 2014;96-B:325-31. 10.1302/0301-620X.96B3.33033 [DOI] [PubMed] [Google Scholar]
- 121.Helito CP, Demange MK, Bonadio MB, et al. Anatomy and Histology of the Knee Anterolateral Ligament. Orthop J Sports Med 2013;1:2325967113513546. 10.1177/2325967113513546 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Sonnery-Cottet B, Daggett M, Fayard JM, et al. Anterolateral Ligament Expert Group consensus paper on the management of internal rotation and instability of the anterior cruciate ligament - deficient knee. J Orthop Traumatol 2017;18:91-106. 10.1007/s10195-017-0449-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Tramer JS, Fidai MS, Kadri O, et al. Anterolateral Ligament Reconstruction Practice Patterns Across the United States. Orthop J Sports Med 2018;6:2325967118811063. 10.1177/2325967118811063 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Sonnery-Cottet B, Thaunat M, Freychet B, et al. Outcome of a Combined Anterior Cruciate Ligament and Anterolateral Ligament Reconstruction Technique With a Minimum 2-Year Follow-up. Am J Sports Med 2015;43:1598-605. 10.1177/0363546515571571 [DOI] [PubMed] [Google Scholar]
- 125.Mogos Ș, Antonescu D, Stoica IC, et al. Superior rotational stability and lower re-ruptures rate after combined anterolateral and anterior cruciate ligament reconstruction compared to isolated anterior cruciate ligament reconstruction: a 2-year prospective randomized clinical trial. Phys Sportsmed 2022. [Epub ahead of print]. doi: . 10.1080/00913847.2022.2112914 [DOI] [PubMed] [Google Scholar]
- 126.Lai S, Zhang Z, Li J, et al. Comparison of Anterior Cruciate Ligament Reconstruction With Versus Without Anterolateral Augmentation: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Orthop J Sports Med 2023;11:23259671221149403. 10.1177/23259671221149403 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Nazzal EM, Keeling LE, Ryan PM, et al. The Role of Lateral Extra-articular Tenodesis in Anterior Cruciate Ligament Reconstruction and Treatment of Rotatory Knee Instability: a Scoping Review. Curr Rev Musculoskelet Med 2023;16:235-45. 10.1007/s12178-023-09832-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Farshidfar SS, Cadman J, Neri T, et al. Towards a validated musculoskeletal knee model to estimate tibiofemoral kinematics and ligament strains: comparison of different anterolateral augmentation procedures combined with isolated ACL reconstructions. Biomed Eng Online 2023;22:31. 10.1186/s12938-023-01094-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Boksh K, Sheikh N, Chong HH, et al. The Role of Anterolateral Ligament Reconstruction or Lateral Extra-articular Tenodesis for Revision Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Comparative Clinical Studies. Am J Sports Med 2023. [Epub ahead of print]. doi: . 10.1177/03635465231157377 [DOI] [PubMed] [Google Scholar]
- 130.Willinger L, Athwal KK, Holthof S, et al. Role of the Anterior Cruciate Ligament, Anterolateral Complex, and Lateral Meniscus Posterior Root in Anterolateral Rotatory Knee Instability: A Biomechanical Study. Am J Sports Med 2023;51:1136-45. 10.1177/03635465231161071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Robin BN, Jani SS, Marvil SC, et al. Advantages and Disadvantages of Transtibial, Anteromedial Portal, and Outside-In Femoral Tunnel Drilling in Single-Bundle Anterior Cruciate Ligament Reconstruction: A Systematic Review. Arthroscopy 2015;31:1412-7. 10.1016/j.arthro.2015.01.018 [DOI] [PubMed] [Google Scholar]
- 132.Siebold R, Schuhmacher P, Fernandez F, et al. Flat midsubstance of the anterior cruciate ligament with tibial "C"-shaped insertion site. Knee Surg Sports Traumatol Arthrosc 2015;23:3136-42. 10.1007/s00167-014-3058-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Fink C, Smigielski R, Siebold R, et al. Anterior Cruciate Ligament Reconstruction Using a Ribbon-Like Graft With a C-Shaped Tibial Bone Tunnel. Arthrosc Tech 2020;9:e247-62. 10.1016/j.eats.2019.10.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Borque KA, Laughlin MS, Pinheiro VH, et al. Rebranding the 'anatomic' ACL reconstruction: Current concepts. J ISAKOS 2023;8:23-8. 10.1016/j.jisako.2022.11.001 [DOI] [PubMed] [Google Scholar]
- 135.Van Eetvelde H, Mendonça LD, Ley C, et al. Machine learning methods in sport injury prediction and prevention: a systematic review. J Exp Orthop 2021;8:27. 10.1186/s40634-021-00346-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Martin RK, Wastvedt S, Pareek A, et al. Predicting subjective failure of ACL reconstruction: a machine learning analysis of the Norwegian Knee Ligament Register and patient reported outcomes. J ISAKOS 2022;7:1-9. 10.1016/j.jisako.2021.12.005 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The article’s supplementary files as