

Abstract
Background
The treatment of simple rib fractures in older adults can be divided into surgical treatment and nonsurgical treatment, with indications for surgery presently being unclear. This study was conducted to determine whether older adult individuals with simple multiple rib fractures can benefit from surgical treatment.
Methods
A single-center, retrospective study was conducted. All 880 registry-identified patients aged ≥60 years who were admitted to Beijing Jishuitan Hospital with blunt rib fractures between 2013 to 2020 were included. They were divided into 2 groups according to whether internal fixation was performed. After screening of inclusion and exclusion criteria and propensity score matching, there were 226 patients, 113 of whom were placed in the operation group and 113 in the nonoperation group. The demographic characteristics, underlying diseases, number of rib fractures, hospital stay, intensive care unit (ICU) hospital stay, mechanical ventilation duration, fracture comorbidities on admission, pain index, and fracture healing condition were analyzed using chi-squared test and independent samples t test.
Results
The pain score and fracture healing time were significantly improved in the operation group (P<0.05), while the duration of painkiller use was significantly shorter in the operation group (P=0.009). However, there was no significant differences in mortality, the incidence of bone nonunion, length of stay in the ICU, or duration of mechanical ventilation between the 2 groups.
Conclusions
For patients in the clinical study, internal fixation surgery could reduce fracture healing time and minimize the use of painkillers. Surgical treatment was determined to be safe, as it did not increase the mortality of the older adult patients. For older patients with simple rib fractures who have no contraindications to surgery, internal fixation surgery is recommended.
Keywords: Geriatrics, simple multiple rib fractures, surgical treatment, internal fixation
Highlight box.
Key findings
• Internal fixation surgery for older adult individuals with simple multiple rib fractures without contraindication was found to be able to reduce analgesia duration and shorten time to union.
What is known and what is new?
• The treatment of simple multiple rib fractures can be divided into surgical or conservative treatment, but the surgical indications for older adults with rib fractures have not been standardized.
• We conducted a clinical, single-center, retrospective study of simple multiple rib fractures in older adults.
What is the implication, and what should change now?
• It was found that by following the indications practiced by the Beijing Jishuitan Hospital, surgical treatment was beneficial to older adult patients with simple multiple rib fractures; the fracture healing time and time of use of painkillers were also reduced. The status and priority of surgical treatment should be reconsidered in the treatment of simple multiple rib fractures in older adults.
Introduction
Background
Rib fracture is the most common chest injury, with an incidence of approximately 60–90% among chest injuries (1-3). Rib fracture is still treated mainly by internal fixation or conservative treatment. Because of the severe pain and pulmonary complications caused by rib fracture, the quality of life of patients with rib fracture can be degraded. When rib fracture injury is serious, the broken end of the rib is dislocated or even missing, which can easily lead to delayed union or nonunion of rib fracture (4).
With the rapid development of modern industry and transportation in China, the number of patients with chest trauma has increased rapidly. One early study found the mortality rate of patients with flail chest and visceral injuries to be more than 20% (5), but a more recent study reported a lower mortality (6). According to the literature, for older adult patients with rib fractures older than 60 years, the mortality rate increases by 5% for every 1-year increase in age (7). Most of the complications are caused by chest wall pain and limited inspiration (insufficient inspiration caused by pain) leading to atelectasis and pneumonia. Therefore, the incidence of complications after rib fracture in older adult individuals in China is particularly high (up to 20%) (8).
Study rationale and literature review
Rib fractures can be divided into flail chest and simple rib fractures, with the former accounting for 3–5% of these fractures (2,3). Clinically, most rib fractures are simple rib fractures. In the general population, internal fixation is recommended as the treatment for flail chest, but currently, the indication of surgical treatment of simple rib fracture remains controversial. For older adult patients, the treatment of simple rib fracture poses a dilemma: on the one hand, older adults are often complicated with osteoporosis and many basic diseases, and whether these patients can withstand the trauma operation and anesthesia to benefit from the operation is not clear; on the other hand, conservative treatment for older adult patients also entails several risks, including long-term bed rest and unwillingness to cough due pain, which can easily lead to atelectasis, disability, pressure sores, and other complications.
There is compelling evidence indicating that surgical stability of flail chest is beneficial in terms of reducing the incidence of pneumonia, the days in the intensive care unit (ICU), and the days of ventilation (9). Due to the lack of high-level evidence, however, the effect of surgical stabilization on multiple simple rib fractures remains controversial. A study showed that internal fixation operation in nonflail chest fractures is associated with higher rates of complications and mortality (10). However, other some studies reported that operations could improve the outcome of patients with multiple rib fractures but not flail chest (11,12). Thus far, the related studies have included patients with or without flail chest, but few studies have examined patients with simple rib fractures, let alone those who are older adults (13).
Consequently, it is unclear whether operation for simple multiple rib fractures in older adult patients is necessary, and the surgical indications have not been defined. Although this issue is mentioned in some clinical guidelines, the level of recommendation and evidence is not high (3). As no relevant specific clinical guidelines or operating norms yet exist, each trauma center has a different understanding of surgical adaptability in actual clinical work. In addition, for the surgical treatment of simple rib fracture in older adult individuals, there are few studies and reports either in China or internationally. Therefore, this study was conducted to identify a rationale and standardized means to treating simple rib fracture.
Objective
The primary aims of this study were to compare the outcomes and complications of 2 management strategies (internal fixation surgery and conservative treatment). The secondary aim was to describe the incidence and management of simple multiple rib fracture in older adult patients (age older than 60 years) at the Department of Thoracic Surgery of Beijing Jishuitan Hospital. We present this article in accordance with the STROBE reporting checklist (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1829/rc).
Methods
Study design
This single-center, retrospective, observational study was conducted between January 2013 and December 2020. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and was approved by the Beijing Jishuitan Hospital Institutional Review Board (No. 202107-40). Informed consent was obtained from all patients.
Setting
Beijing Jishuitan Hospital is the trauma and burn rescue center of Beijing, with an annual outpatient volume of more than 10,000 patients and an annual emergency volume of more than 1,500 patients. The hospital has rich experience in the treatment of patients with multiple traumas combined with thoracic trauma.
Participants
Inclusion criteria
The inclusion criteria for patients were as follows: (I) older adult patients (≥60 years old) with simple multiple rib fractures, with a simple multiple rib fracture being defined as the fracture of multiple ribs (>2) but without the formation of a flail chest (3 in a row, with 2 or more fractures in each); (II) patients with blunt trauma; and (III) clear imaging evidence to prove fracture of ≥2 ribs.
Exclusion criteria
The exclusion criteria for patients were as follows: (I) use of anticoagulants, (II) without follow-up computed tomography (CT) image data, and (III) no administration of imrecoxib for analgesia after postoperative discharge due to various contraindications to medication.
Variables
Treatment of the operation group
After initial resuscitation, all patients in the operation group underwent open operations under general anesthesia in the supine or lateral position. The broken end of rib fracture was located by ultrasound before operation, and the appropriate surgical incision was selected according to the location and number of rib fractures (horizontal incision or vertical incision, or multiple independent incisions according to the situation). The length of surgical incision was usually between 5 and 15 cm. After the skin and subcutaneous tissue were incised, the muscle tissue was retained as much as possible; a tunnel space was separated to the surface of the ribs; the blood clot around the fracture site was removed; the periosteum around the fracture was peeled off minimally (about 2 cm); reduction forceps, right angle forceps, or duckbill forceps were used for anatomical reduction; and then the appropriate length of internal fixator was cut and placed on the fracture site (Figure 1). The internal fixations are all made of a new pure titanium U-shaped plate (MatrixRIB, Johnson & Johnson Company, New Brunswick, NJ, USA). At least 2 nails were fixed at both ends of the fracture. If the patient was complicated with pleural injury, a no. 12 thoracic drainage tube was placed during the operation. Postoperative analgesia pump was routinely used to relieve the pain of rib fracture. After the patient was discharged, long-term oral administration of imrecoxib tablets (0.1 g bid) for analgesia was applied.
Figure 1.

Internal fixation of a multiple rib fracture. A 75-year-old male with multiple traumas including sternal fractures, fractures of the right ribs 1–3 and 5–11 and left ribs 1 and 6–9, cartilage fractures of the left ribs 1–5, bilateral pleural effusions, and bilateral lung contusions. (A) CT 3D reconstruction prior to surgery suggested fractures of the sternum and ribs. (B) Preoperative plain CT scan revealed transverse sternal fracture and subcutaneous emphysema. (C) Intraoperative image of internal fixation after placement. (D) Postoperative CT 3D reconstruction suggested that the sternal fracture and the fracture of the left ribs 3–5 were repositioned and that the internal fixation was well positioned. CT, computed tomography.
Treatment of the nonoperation group
Patients in the nonoperation group were treated with external fixation of the rib band and chest guard plate, atomization, and pain relief, with anti-inflammatory treatment being provided to patients with pneumothorax or pulmonary infection. Closed thoracic drainage was performed in patients with extensive hemothorax and/or pneumothorax. Patients with severe lung injury were treated with mechanical ventilation. After the patient was discharged, long-term oral administration of imrecoxib tablets (0.1 g bid) for analgesia was applied.
Study size
A total of 880 older adult (≥60 years old) patients hospitalized for blunt chest trauma in the Department of Thoracic Surgery at Beijing Jishuitan Hospital from 2013 to 2020 were initially included in our clinical study, and 438 patients were enrolled through further screening of inclusion and exclusion criteria. The selected 438 patients were then divided into an operation group (n=113) and a nonoperation group (n=325).
Bias
We performed 1:1 propensity score matching for sex, age, underlying diseases, fracture complications at admission, time of visit, injury severity score (ISS), and chest abbreviated injury scale (AIS) score of the patients in the 2 groups. After 1:1 propensity score matching, 226 patients were selected: 113 patients in the operation group and 113 patients in the nonoperation group.
Data collection
A retrospective study designed was used to collect information of the patients from their electronic medical records, nursing records, examination records, and other data. The basic characteristic of patients were recorded, including sex, age, basic pulmonary diseases [chronic obstructive pulmonary disease (COPD) and asthma], smoking history, diabetes history, and basic pulmonary cardiovascular diseases. Additionally, patient information regarding rib fracture was recorded, including visit time, number of rib fractures, AIS score, ISS, fracture comorbidities on admission (lung infections, pleural effusion, pulmonary atelectasis, pneumothorax, lung contusion), hospital stay, ICU hospital stay, mechanical ventilation duration, pain score, the time of fracture healing, and the duration of painkiller use.
Data analysis
The evaluated fracture comorbidities on admission included lung infections, pleural effusion, pulmonary atelectasis, pneumothorax, lung contusion, and death. Among these, pneumothorax, atelectasis, and pleural effusion were judged according to imaging changes, while pulmonary infection and death were judged according to the electrocardiography (ECG) indicators in the relevant guidelines.
The evaluation of fracture healing included the pain score of patients and follow-up of fracture healing. The pain score was determined on admission and discharge judging by visual analogue scale (VAS score); the use and time of painkillers were followed up after discharge; and fracture healing was followed up after discharge mainly via imaging examination, physical examination, and clinical symptoms. In this clinical study, CT scan was chosen to examine whether the rib fractures had healed, as the fracture line can be clearly seen on the axis of CT (Figure 2). In both the operation group and the nonoperation group, reexamination with CT was conducted every 4–6 weeks until CT indicated that the fracture had healed or the fracture had not healed up to 9 months after injury. Nonunion status was recorded if CT showed that the patients had nonunion of rib fracture 9 months after the initial injury.
Figure 2.

CT scan images of a patient with rib fracture. A 63-year-old female with multiple trauma, scaphoid fracture, fracture of the left ribs 2–4, contusion of the left lung, and pulmonary infection. (A) Preoperative CT 3D reconstruction suggested a left scaphoid fracture and fracture of ribs 2–4. (B) Postoperative CT 3D reconstruction suggested good repositioning of the left fractured ribs 2–4 and good position of the internal fixation. (C) Preoperative CT scan suggested left rib fractures, left scaphoid fracture, and left lung contusion. (D) Three months after operation, a CT axial plain scan showed that the fracture of the left rib had healed well and that there was continuous callus formation at the fracture. The cortical bone of the left scapula was discontinuous, and the fracture was not yet healed. CT, computed tomography.
Statistical analysis
Patients were matched with propensity scoring for demographic characteristics in a 1:1 ratio. Statistical analysis was performed using SPSS 26.0 software (IBM Corp., Armonk, NY, USA). The quantitative indices of normal distribution are described by the mean ± standard deviation, and independent samples were evaluated using t-test or corrected t-test. A chi-squared test was used to compare the qualitative data between groups, and P<0.05 was considered to indicate a statistically significant difference. The correlation between the 2 samples was analyzed with Pearson correlation analysis.
Results
Participants
A single-center, retrospective study was conducted at the Department of Thoracic Surgery, Beijing Jishuitan Hospital, Beijing, China, which included 880 patients aged ≥60 years who were admitted from 2013 to 2020 for blunt trauma causing rib fractures. They were screened according to inclusion and exclusion criteria, and 130 patients without follow-up CT data, 110 patients who did not take imrecoxib for analgesia after postoperative discharge, 133 patients with combined flail chest, 32 patients with single rib fracture, and 37 patients using anticoagulants before injury were removed from the study. The remaining 438 patients were divided into a nonoperation group (n=325) and an operation group (n=113) according to whether or not they underwent internal fixation surgery. After propensity score matching, 226 patients were selected: 113 patients in the operation group and 113 patients in the nonoperation group (Figure 3).
Figure 3.

The STROBE diagram for the study. CT, computed tomography; STROBE, The Strengthening the Reporting of Observational Studies in Epidemiology.
Descriptive data
First, statistical analysis was performed on the number of simple rib fracture operations for older adult patients in our hospital in the past 8 years (n=438), as shown in Figure 4. As can be seen from the figure, the operation rate of older adult patients with multiple simple rib fractures in our hospital has been at a stably high level (approximately 26%) over the past 8 years. Statistics on the causes of injury in the patients were calculated. The common causes of injury were falls (61.8%) and traffic injuries (30%) (Table 1). Falls from low places (shorter than 3 meters) were found to be the leading cause of injury in any given year, accounting for over 40% of injuries.
Figure 4.
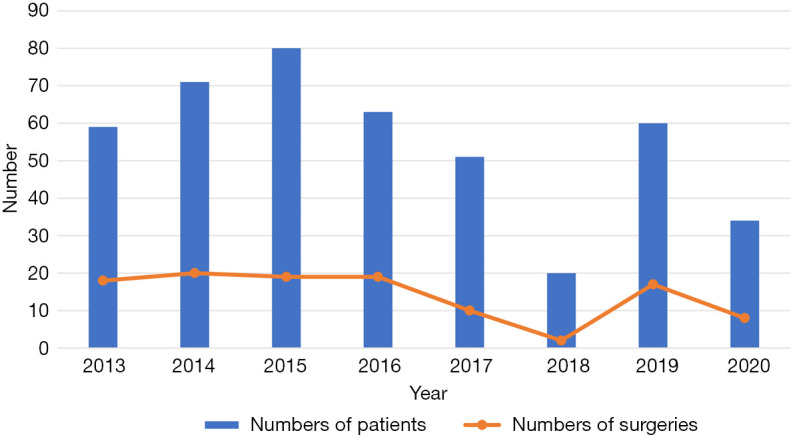
The number of patients and operations over the past 8 years.
Table 1. The common causes of injury.
| Causes | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|
| Truck and car accidents | 5.3 | 9.6 | 3.6 | 17.4 | 9.4 | 26.7 | 8.5 | 6.1 |
| Motorcycle accident | 0 | 0 | 10.8 | 2.9 | 9.4 | 0 | 3.4 | 3 |
| Bicycle accident | 0 | 0 | 4.8 | 7.2 | 3.8 | 0 | 5.1 | 0 |
| Pedestrian accident | 12.3 | 12.3 | 4.8 | 5.8 | 13.2 | 6.7 | 1.7 | 3 |
| Fall from motorcycle or bicycle | 15.8 | 11 | 16.9 | 11.6 | 17 | 6.7 | 10.2 | 18.2 |
| Low fall (<3 m) | 49.1 | 46.6 | 43.4 | 39.1 | 37.7 | 53.3 | 55.9 | 57.6 |
| Fall from a height (≥3 m) | 8.8 | 8.2 | 7.2 | 13 | 7.5 | 0 | 10.2 | 3 |
| Extrusion and burying accident | 7 | 6.8 | 2.4 | 0 | 0 | 6.7 | 5.1 | 9.1 |
| Other (iatrogenic, chronic cough, osteoporosis, and other related fractures) | 0 | 1.4 | 0 | 0 | 0 | 0 | 0 | 0 |
| Fight | 1.8 | 4.1 | 6 | 2.9 | 1.9 | 0 | 0 | 0 |
Outcome data
We further performed statistical analysis on the demographic characteristics of the operation group and the nonoperation group, including for sex, age, basic pulmonary diseases (COPD and asthma), smoking history, diabetes history, basic pulmonary cardiovascular diseases, the number of rib fractures, visit time, and fracture comorbidities on admission (lung infections, pleural effusion, pulmonary atelectasis, pneumothorax, lung contusion). There were significant differences in sex between the 2 groups (Table 2). We then conducted 1:1 propensity score matching on the 2 groups of data, and after matching, there were no significant differences between the 2 groups (Table 3).
Table 2. Patients’ basic condition and medical history before matching.
| Characteristic | Operation group | Nonoperation group | P value |
|---|---|---|---|
| Number of patients | 113 | 325 | |
| Age (years) | 66.60±5.80 | 67.33±5.53 | 0.017 |
| Male | 32 | 156 | 0.235 |
| Underlying disease | |||
| COPD | 2 | 7 | 0.718 |
| Asthma | 2 | 4 | 1.000 |
| Diabetes | 16 | 52 | 0.642 |
| Cardiovascular disease | 32 | 94 | 0.903 |
| Smoking | 36 | 104 | 0.978 |
| Number of fractures | 4.86±1.93 | 4.90±2.12 | 0.838 |
| Fracture comorbidity on admission | |||
| Lung infection | 23 | 63 | 0.823 |
| Pleural effusion | 60 | 170 | 0.885 |
| Pulmonary atelectasis | 23 | 62 | 0.767 |
| Pneumothorax | 24 | 91 | 0.159 |
| Lung contusion | 29 | 82 | 0.927 |
| AIS score | |||
| Chest | 3.06±0.65 | 3.16±0.55 | 0.107 |
| ISS | 12.71±0.53 | 13.33±6.16 | 0.366 |
| Visiting time | 3.34±4.16 | 4.16±8.52 | 0.324 |
Age, numbers of fractures, AIS score, ISS, and visiting time are presented as the mean ± standard deviation. COPD, chronic obstructive pulmonary disease; AIS, abbreviated injury scale; ISS, injury severity score.
Table 3. Patients’ basic condition and medical history after matching.
| Characteristic | Operation group | Nonoperation group | P value |
|---|---|---|---|
| Number of patients | 113 | 113 | |
| Age (years) | 66.60±5.80 | 66.73±4.95 | 0.853 |
| Male | 32 | 71 | 0.784 |
| Underlying disease | |||
| COPD | 2 | 5 | 0.443 |
| Asthma | 2 | 3 | 1.000 |
| Diabetes | 16 | 18 | 0.710 |
| Cardiovascular disease | 32 | 35 | 0.662 |
| Smoking | 36 | 39 | 0.672 |
| Number of fractures | 4.86±1.93 | 4.88±2.11 | 0.948 |
| Fracture comorbidity on admission | |||
| Lung infection | 23 | 26 | 0.628 |
| Pleural effusion | 60 | 56 | 0.594 |
| Pulmonary atelectasis | 23 | 18 | 0.388 |
| Pneumothorax | 24 | 26 | 0.749 |
| Lung contusion | 29 | 24 | 0.432 |
| AIS score | |||
| Chest | 3.06±0.65 | 3.05±0.52 | 0.909 |
| ISS | 12.71±0.53 | 12.34±5.61 | 0.647 |
| Visiting time | 3.34±4.16 | 3.92±6.08 | 0.405 |
Age, numbers of fractures, AIS score, ISS, and visiting time are presented as the mean ± standard deviation. COPD, chronic obstructive pulmonary disease; AIS, abbreviated injury scale; ISS, injury severity score.
Principal results
The outcomes of patients in the operation group were compared with those in the nonoperation group, as shown in Table 4.
Table 4. Outcomes of the patients.
| Outcomes | Operation (n=113) | Nonoperation (n=113) | P value |
|---|---|---|---|
| Length of stay in ICU (d) | 0.67±2.21 | 0.39±1.72 | 0.283 |
| Duration of mechanical ventilation (h) | 8.85±30.98 | 4.35±20.78 | 0.201 |
| Length of stay in hospital (d) | 11.42±4.27 | 8.96±3.67 | 0 |
| Pain score on the day of hospitalization | 8.02±1.18 | 6.95±1.17 | 0 |
| Pain score on the day of discharge | 3.48±1.29 | 4.58±1.11 | 0 |
| Duration of painkiller use (m) | 1.43±0.94 | 1.84±1.35 | 0.009 |
| Fracture healing time (m) | 3.23±0.72 | 3.55±1.38 | 0.033 |
| Bone nonunion | 3 | 5 | 0.778 |
| Death | 1 | 1 |
Length of stay in ICU (d), duration of mechanical ventilation (h), length of stay in hospital (d), pain score on the day of hospitalization, Pain score on the day of discharge, duration of painkiller use (m), and fracture healing time (m) are presented as the mean ± standard deviation. ICU, intensive care unit.
There were no significant differences in the length of stay in the ICU or mechanical ventilation between the 2 groups, but the hospitalization time of the operation group was longer than that of the nonoperation group.
On admission, the pain score in the operation group was significantly higher than that in the nonoperation group (P<0.001), but the pain score at discharge was significantly lower than that in the nonoperation group (P<0.001). Meanwhile, the fracture healing time and duration of painkiller use in the operation group were also significantly shorter than those in the nonoperation group (P<0.05). Moreover, there was no significant difference in the number of patients with bone nonunion and mortality between the operation group and the nonoperation group according to the chi-squared test (P=0.778).
Other results
Among the selected patients, 81 patients in the operation group (71.7%) were performed surgery within 72 hours after injury, while in the nonoperation group, 75 patients (66.4%) presented within 72 hours after injury, which did not represent a significant difference (P=0.388).
Furthermore, 14 patients in the operation group required ICU admission (12.4%), while 6 patients in the nonoperation group (5.3%) required ICU admission, which did not represent a significant difference (P>0.05). However, there was a significant difference between the 2 groups in terms of mechanical ventilation (P=0.049), with 13 (11.5%) and 5 (4.4%) patients in the operation group and nonoperation group, respectively, requiring mechanical ventilation.
Discussion
Principal findings
After propensity score matching, the data from the 2 groups were found to be comparable. The operation group was found to have a lower score for pain than did the nonoperation group, and operation was found to significantly reduce the time of fracture healing and the use of painkillers, which is encouraging. Furthermore, infixation surgery can be considered safe, as there was no significant difference in the mortality. However, there was no significant difference in the proportion of patients with bone nonunion between the operation group and the nonoperation group; thus, surgery may not reduce the risk of bone nonunion.
Strengths and limitations
The strength of this retrospective study is the large sample size and novel focus on older adults with simple multiple rib fractures.
However, there are a few limitations that should be mentioned. First, it has been proven that surgery should be performed within 72 hours after trauma (3), and every extra day of hospitalization before surgery increases the risk of pneumonia by 31% (14). However, as a major trauma center, Jishuitan Hospital receives many referral patients, meaning that some of the patients cannot undergo surgery within 72 hours of the injury, the possible effect of which was not accounted for in this study. Second, in 2018, due to the partial loss of data resulting from a hospital system upgrade, the data were limited and incomplete. Third, we only counted the comorbidities of rib fractures and did not have exact records on the complications of rib fractures during treatment; thus, the statistics for treatment outcomes were limited to the duration of pain and whether the fracture healed or not.
Comparison with similar research
Regarding the worrisome death index, although it differs from the results reported in a 2020 retrospective study by Chen Zhu et al., in which early internal fixation was found to significantly reduce mortality in older adults (15), there was no significant difference between the operation group and the nonoperation group, demonstrating that internal fixation is safe and does not cause unacceptable harm to the patient. In our study, the mortality rate of patients due to rib injury alone was not high (less than 1%), so operation did not result in a significant improvement in mortality.
It is worth noting that the results of this study are significantly different from those of other research on the internal fixation of flail chest in older adult patients. In a prospective study of patients with flail chest undergoing internal fixation surgery in 2005, Granetzny et al. (16) reported that the operation group required significantly less mechanical ventilation and chest ICU and hospital stay than did the conservative group. However, in our study, the hospitalization time of surgical treatment was significantly longer (2.5 days) than that of nonoperative treatment, with more patients in the operation group requiring mechanical ventilation (P=0.49). The reason for this is that the condition of continuous fracture is always more severe than is a simple rib fracture and has a more significant impact on the patient’s respiratory function. Compared with that in young people, the treatment process of rib fracture in older adult patients is risky: while it can accelerate patients’ recovery and improve their quality of life to a certain extent, it also increases the incidence of complications during the perioperative period. This is because surgery, anesthesia, blood loss, and infection can affect the patient’s body to varying degrees. Because simple rib fractures entail a generally mild overall condition, the impact of surgery on the body cannot be ignored in the face of trauma. However, in our opinion, an increase in hospitalization time and a slight increase in the rate of need for mechanical ventilation compared to the long-term pain associated with a rib fracture is not a reason to refuse surgery, but this needs to be adequately communicated and explained to the patient.
Chest pain causes considerable distress in older adult patients with rib fractures. We also noticed that even though the patients in the operation group were greatly improved compared with those in the nonoperation group, the average pain score at discharge was 3.48, and the average duration of painkiller use was 1.43 months after discharge. As pointed out in a 2012 paper and supported by other research (17,18), older adult individuals with rib fractures may be in pain denial for an extended period, which adversely affects their lives.
Explanation of findings
The average hospital stay of patients in the operation group was 2.4 days longer than that in the nonoperation group, the use of nonsteroidal anti-inflammatory drugs (NSAIDs) decreased by 0.4 months on average, and the fracture healing time decreased by 0.3 months. Whether such results are meaningful in clinical practice is a matter worth considering. Operation may reduce the incidence rate of gastrointestinal bleeding in older adult patients caused by NSAIDs. Moreover, by reducing pain scores at hospital discharge, surgical fixation can enable patients to complete bedrest earlier, reducing the incidence rate of hypostatic pneumonia and pressure sores.
Implications and recommendations
As a special group, older adult patients over 60 years of age with rib fractures are more likely to experience adverse outcomes (including chronic chest pain, bone nonunion, disability, and death) (2,19). The reasons for this are mainly the following: first, after the occurrence of rib fracture in older adult patients, they may have a poor ability to recover from physical injury and are often accompanied by osteoporosis. In older adults, the osteogenic ability of osteoblasts decreases, the bone resorption capacity of osteoclasts increases, the quality of fracture healing is reduced, and the proportion of those with delayed union and nonunion is higher (20). Second, limited breathing caused by pain places older adults at greater risk of adverse outcomes (21). Third, older adults are often accompanied by poor cardiopulmonary function and basic diseases, and the physiological reserve is not sufficient. Finally, many older adults take anticoagulants for a long period of time, which reduces their chances of surgery.
According to the 2021 version of Chinese experts’ consensus on the surgical treatment of traumatic rib fractures, patients without surgical contraindications and without flail chest can also benefit from surgical treatment (Ⅱ B). Surgeons are encouraged to treat rib fractures in an active manner. Although there is no clear evidence suggesting that surgical treatment can improve bone healing, it has been shown to improve lung function and pain and reduce the rate of disability and time to return to work (18,22). Thus, it has an incomparable advantage over conservative treatment for the recovery of lung function.
Surgical treatment cannot be applied to all older adult patients with simple multiple rib fractures. Only when we carefully evaluate the benefits and risks of surgery for each patient can we achieve the best results. The basis for the benefits of surgical treatment consisted primarily on preoperative evaluation. We should thus establish a strict standard adaptive sign-evaluation method.
Based on extensive previous clinical experience, our center has formulated the following surgical indications for rib fractures in older adults at this stage:
Surgical treatment is recommended for patients with flail chest and no surgical contraindications.
Surgical treatment is recommended for nonflail chest patients with ≥2 rib fractures and obvious displacement of the broken end.
Surgical treatment is recommended for patients with nonflail chest and early severe pain with poor effects from conservative treatment.
For patients with nonflail chest and complications, conservative analgesia and respiratory management should be routinely administered. If the effect is not good, surgical treatment is recommended without obvious surgical contraindications.
For patients with severe complications, if respiratory deterioration and long-term flail chest persist, internal fixation surgery should be considered unless they are with obvious surgical contraindication.
Overall, our hospital has a high operation rate for simple rib fractures in older adult patients without flail chests. Our hospital has treated a large number of critically ill patients transferred from all over China and has a mortality rate of less than 2%, which is lower than at reported in China and internationally (3,23), demonstrating that our method for the treatment of rib fractures in older adults is advanced and effective. In a study conducted in 2021 on older adult patients with rib fractures, the operative proportion was only 5% of the 295 patients enrolled in the study, although their operative proportion has increased steadily in recent years (24). As the largest trauma center in North China, Jishuitan Hospital shoulders the important burden of development and innovation. We hope that the practical exploration of our experience can enlighten our colleagues and contribute to the development of a clinical guideline.
Conclusions
For simple multiple rib fractures in older adults (≥2 rib fractures), internal fixation can promote fracture healing through anatomical reduction, which is effective in alleviating the use of painkillers in these patients after trauma and reducing the fracture healing time. However, older adult individuals are often associated with osteoporosis and other bone problems, and surgical treatment cannot significantly reduce the risk of fracture nonunion. Nonetheless, surgical treatment does not increase the mortality of older adult patients. Surgical treatment is thus recommended for older adult patients with simple multiple rib fractures and no contraindications to operation.
Supplementary
The article’s supplementary files as
Acknowledgments
We appreciate the kind support and help of Thoracic Surgery Department, Case Department, and Radiology Department of Beijing Jishuitan Hospital.
Funding: This study was supported by Beijing Jishuitan Hospital - Discipline New Star Program (No. XKXX202117).
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and was approved by Beijing Jishuitan Hospital Institutional Review Board (No. 202107-40). Informed consent was obtained from all patients.
Reporting Checklist: The authors have completed the STROBE reporting checklist. Available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1829/rc
Data Sharing Statement: Available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1829/dss
Peer Review File: Available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1829/prf
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1829/coif). The authors have no conflicts of interest to declare.
(English Language Editor: J. Gray)
References
- 1.Senekjian L, Nirula R. Rib Fracture Fixation: Indications and Outcomes. Crit Care Clin 2017;33:153-65. 10.1016/j.ccc.2016.08.009 [DOI] [PubMed] [Google Scholar]
- 2.Coary R, Skerritt C, Carey A, et al. New horizons in rib fracture management in the older adult. Age Ageing 2020;49:161-7. 10.1093/ageing/afz157 [DOI] [PubMed] [Google Scholar]
- 3.Pieracci FM, Majercik S, Ali-Osman F, et al. Consensus statement: Surgical stabilization of rib fractures rib fracture colloquium clinical practice guidelines. Injury 2017;48:307-21. 10.1016/j.injury.2016.11.026 [DOI] [PubMed] [Google Scholar]
- 4.Martin TJ, Eltorai AS, Dunn R, et al. Clinical management of rib fractures and methods for prevention of pulmonary complications: A review. Injury 2019;50:1159-65. 10.1016/j.injury.2019.04.020 [DOI] [PubMed] [Google Scholar]
- 5.Borman JB, Aharonson-Daniel L, Savitsky B, et al. Unilateral flail chest is seldom a lethal injury. Emerg Med J 2006;23:903-5. 10.1136/emj.2006.037945 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Benjamin E, Recinos G, Aiolfi A, et al. Flail Chest: Less Deadly than Originally Thought. World J Surg 2018;42:3927-31. 10.1007/s00268-018-4723-6 [DOI] [PubMed] [Google Scholar]
- 7.Bulger EM, Arneson MA, Mock CN, et al. Rib fractures in the older adult. J Trauma 2000;48:1040-6; discussion 1046-7. 10.1097/00005373-200006000-00007 [DOI] [PubMed] [Google Scholar]
- 8.Iraeus J, Lundin L, Storm S, et al. Detailed subject-specific FE rib modeling for fracture prediction. Traffic Inj Prev 2019;20:S88-95. 10.1080/15389588.2019.1665649 [DOI] [PubMed] [Google Scholar]
- 9.Cataneo AJ, Cataneo DC, de Oliveira FH, et al. Surgical versus nonsurgical interventions for flail chest. Cochrane Database Syst Rev 2015;2015:CD009919. 10.1002/14651858.CD009919.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Haddadin Z, Hanna K, Castanon L, et al. Rib Plating the Non-Flail Chest May Not Be as Good as You Think. J Am Coll Surg 2019;229:e241-2. [Google Scholar]
- 11.Azim A, Khan M, Jehan F, et al. In-Hospital Outcomes after Operative Fixation of Multiple Rib Fractures with Non-Flail Chest: A Propensity Matched Analysis. J Am Coll Surg 2019;229:e232. [Google Scholar]
- 12.Pieracci FM, Leasia K, Bauman Z, et al. A multicenter, prospective, controlled clinical trial of surgical stabilization of rib fractures in patients with severe, nonflail fracture patterns (Chest Wall Injury Society NONFLAIL). J Trauma Acute Care Surg 2020;88:249-57. 10.1097/TA.0000000000002559 [DOI] [PubMed] [Google Scholar]
- 13.Wijffels MME, Prins JTH, Perpetua Alvino EJ, et al. Operative versus nonoperative treatment of multiple simple rib fractures: A systematic review and meta-analysis. Injury 2020;51:2368-78. 10.1016/j.injury.2020.07.009 [DOI] [PubMed] [Google Scholar]
- 14.Pieracci FM, Coleman J, Ali-Osman F, et al. A multicenter evaluation of the optimal timing of surgical stabilization of rib fractures. J Trauma Acute Care Surg 2018;84:1-10. 10.1097/TA.0000000000001729 [DOI] [PubMed] [Google Scholar]
- 15.Chen Zhu R, de Roulet A, Ogami T, et al. Rib fixation in geriatric trauma: Mortality benefits for the most vulnerable patients. J Trauma Acute Care Surg 2020;89:103-10. 10.1097/TA.0000000000002666 [DOI] [PubMed] [Google Scholar]
- 16.Granetzny A, Abd El-Aal M, Emam E, et al. Surgical versus conservative treatment of flail chest. Evaluation of the pulmonary status. Interact Cardiovasc Thorac Surg 2005;4:583-7. 10.1510/icvts.2005.111807 [DOI] [PubMed] [Google Scholar]
- 17.Fabricant L, Ham B, Mullins R, et al. Prolonged pain and disability are common after rib fractures. Am J Surg 2013;205:511-5; discusssion 515-6. [DOI] [PubMed]
- 18.Marasco S, Lee G, Summerhayes R, et al. Quality of life after major trauma with multiple rib fractures. Injury 2015;46:61-5. 10.1016/j.injury.2014.06.014 [DOI] [PubMed] [Google Scholar]
- 19.Lehmann R, Beekley A, Casey L, et al. The impact of advanced age on trauma triage decisions and outcomes: a statewide analysis. Am J Surg 2009;197:571-4; discussion 574-5. 10.1016/j.amjsurg.2008.12.037 [DOI] [PubMed] [Google Scholar]
- 20.Izquierdo-Avino R, Cebollada-Gadea L, Jordan-Jarque M, et al. Risk of osteoporotic fracture and refracture: the importance of index fracture site. Arch Osteoporos 2023;18:27. 10.1007/s11657-023-01213-1 [DOI] [PubMed] [Google Scholar]
- 21.Jeffery Z, Everson M, Carty S. Management of rib fractures. Br J Hosp Med (Lond) 2019;80:C146-9. 10.12968/hmed.2019.80.10.C146 [DOI] [PubMed] [Google Scholar]
- 22.Liu Y, Xu S, Yu Q, et al. Surgical versus conservative therapy for multiple rib fractures: a retrospective analysis. Ann Transl Med 2018;6:439. 10.21037/atm.2018.10.12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Van Vledder MG, Kwakernaak V, Hagenaars T, et al. Patterns of injury and outcomes in the older adult patient with rib fractures: a multicenter observational study. Eur J Trauma Emerg Surg 2019;45:575-83. 10.1007/s00068-018-0969-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Cooper E, Wake E, Cho C, et al. Outcomes of rib fractures in the geriatric population: A 5-year retrospective, single-institution, Australian study. ANZ J Surg 2021;91:1886-92. 10.1111/ans.17064 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The article’s supplementary files as