

Abstract
Objectives:
Early life socioeconomic status (SES) and adversity are associated with late life cognition and risk of dementia. We examined the association between early life SES and adversity and late life cross-sectional cognitive outcomes as well as global cognitive decline, hypothesizing that adulthood SES would mediate these associations.
Methods:
Our sample (N=837) was a racially/ethnically diverse cohort of non-Hispanic/Latino White (48%), Black (27%), and Hispanic/Latino (19%) participants from Northern California. Participant addresses were geocoded to the level of the census tract, and U.S. Census tract 2010 variables (e.g., percent with high school diploma) were extracted and combined to create a neighborhood SES composite. We used multilevel latent variable models to estimate early life (e.g., parental education, whether participant ever went hungry) and adult (participant’s education, main occupation) SES factors and their associations with cross-sectional and longitudinal cognitive outcomes of episodic memory, semantic memory, executive function, and spatial ability.
Results:
Child and adult factors were strongly related to domain-specific cognitive intercepts (0.20–0.48 SD per SD of SES factor); in contrast, SES factors were not related to global cognitive change (0.001–0.01 SD per year per SD of SES factor). Adulthood SES mediated a large percentage (68–75%) of the total early life effect on cognition.
Conclusions:
Early life sociocontextual factors are more strongly associated with cross-sectional late life cognitive performance compared to cognitive change; this effect is largely mediated through associations with adulthood SES.
Keywords: Diversity, Neighborhoods, Socioeconomic Status, Social Determinants, Cognition
INTRODUCTION
The older adult population in the U.S. is rapidly increasing in number. Accompanying this dramatic growth of the diverse, older adult population is the risk for cognitive impairment associated with dementia and Alzheimer’s disease (AD). Cognitive impairment is related to disability and loss of independence (Gill & Richardson, 1995), which can take a toll on older adults and their caregivers. For older racial/ethnic minorities, this can exacerbate existing health disparities. A growing literature has indicated important risk factors for late life cognitive impairment and decline, including the early life environment. Life-course approaches to health posit that factors associated with early life have longstanding effects (Turrell et al., 2002); further, there may be critical or sensitive periods in which early life exposures are most salient, as well as the accumulation of exposures over time that contribute to later life outcomes (Greenfield et al., 2021). In the socioeconomic status (SES) literature, the notion is that early life risk and protective factors operate above and beyond their impact on adulthood SES (Luo & Waite, 2008).
Some positive associations have been shown between late life cognition and various indicators of childhood SES, including county literacy rate (Wilson, Scherr, Hoganson, et al., 2005), birth state (George et al., 2021; Gilsanz et al., 2017), urban versus rural upbringing (Saenz, Downer, Garcia, & Wong, 2018; Zhang, Gu, & Hayward, 2008), parental SES (Everson-Rose, Mendes de Leon, Bienias, Wilson, & Evans, 2003), self-reported childhood SES, and household size (Melrose et al., 2015; Wilson, Scherr, Bienias, et al., 2005). Using data from the Health and Retirement Study, Luo and Waite (2008) found that childhood SES was associated with adult health (i.e., self-rated health, functional limitations, chronic conditions, depressive symptoms, self-rated memory, and cognitive function) in later life partly by its association with childhood self-rated health. However, a much larger proportion of the relationship between childhood SES and adult health operated through its association with adulthood SES (i.e., education and income). That is, while most coefficients of childhood SES variables were attenuated by 0–20% with the inclusion of childhood self-rated health, reductions in the size of the coefficients for childhood SES with the inclusion of adulthood SES ranged from 18–95%. Others have found no relationship between childhood SES and later health once adult SES is taken into account (Brewster et al., 2014; Everson-Rose et al., 2003; Zeki Al Hazzouri et al., 2011).
More recently, using population-based data from the China Health and Retirement Longitudinal Study, Yang and Wang (2020) showed that early life conditions were associated with level and trajectory of cognition: higher childhood SES, operationalized as high paternal education and a non-agricultural job, and food adequacy were associated with a slower rate of cognitive decline in middle-aged Chinese adults. Furthermore, early life adversity (i.e., maternal death) for older Chinese adults was associated with lower baseline cognitive level but that this association was largely attenuated by adulthood education.
Another important measure of adulthood SES is related to neighborhood-level factors. Particularly for older adults, whose income is generally fixed, one measure of SES that may more accurately reflect an older person’s social status is where he/she lives. Older adults who live in more affluent neighborhoods, regardless of education and individual income, may reap certain cognitive health benefits. Neighborhoods may be especially important for older adults who have limited financial and physical mobility (Glass et al., 2006). Low SES neighborhoods have more stressors and fewer resources compared to high SES neighborhoods, and this might lead to cognitive impairments due to restricted opportunities for social and cognitive stimulation (Ertel, Glymour, & Berkman, 2008; Sheffield & Peek, 2009). In contrast, high SES neighborhoods may provide older adults with more opportunities (e.g., parks and recreation, libraries), access to health care, and social norms that promote cognitively stimulating activities. This cognitive and mental stimulation may protect against future cognitive decline by building cognitive reserve (Reed et al., 2011; Stern, 2009).
Although several cross-sectional studies on neighborhood SES (NSES) and cognitive outcomes exist (Clarke et al., 2012; Shih et al., 2011; Wight et al., 2006), only a handful have examined the relation between NSES and cognitive decline. Sheffield and Peek (2009) examined the influence of NSES on cognitive change using a national sample of older Mexican Americans and found that odds and rate of incident cognitive decline increased as a function of poorer NSES. In a sample of older adults, Aartsen and colleagues (2019) found that growing up in disadvantaged childhood socioeconomic conditions was associated with lower levels of cognitive function compared to more advantaged conditions. Similarly, other studies (Meyer et al., 2018; Rosso et al., 2016; Zeki Al Hazzouri et al., 2011) showed that while lower NSES was associated with poorer baseline cognitive scores, it was not associated with rates of decline.
Early life adversity, although related to SES, is a separate construct that has also been associated with poor health and may play a role in later life cognitive function. Children exposed to adverse environments, including maltreatment or abuse, poverty, malnutrition, or death of family members, may have increased risk of cardiovascular disease and mental health problems later (Comijs et al., 2007; Hughes et al., 2017). Korten and colleagues (2014) used data from the Longitudinal Aging Study in Amsterdam and observed that individuals who experienced adverse childhood events showed a faster 10-year decline in processing speed, but only when depressive symptoms were present.
Some research suggests that early life conditions operate by promoting complex and cognitively enriching environments (Oveisgharan et al., 2020) and via their association with adulthood SES. In this study, we examine how the early life environment and adulthood SES are associated with cognitive outcomes (at baseline) and over time (change). Figure 1 displays our conceptual model and delineates the following hypotheses: (1) Higher childhood SES and lower childhood adversity is related to better late-life cognition (at baseline) and less cognitive decline, and (2) Associations between early life environment and later life cognition (both level and change) will be partially mediated by adulthood SES (both individual- and neighborhood-level).
Figure 1.
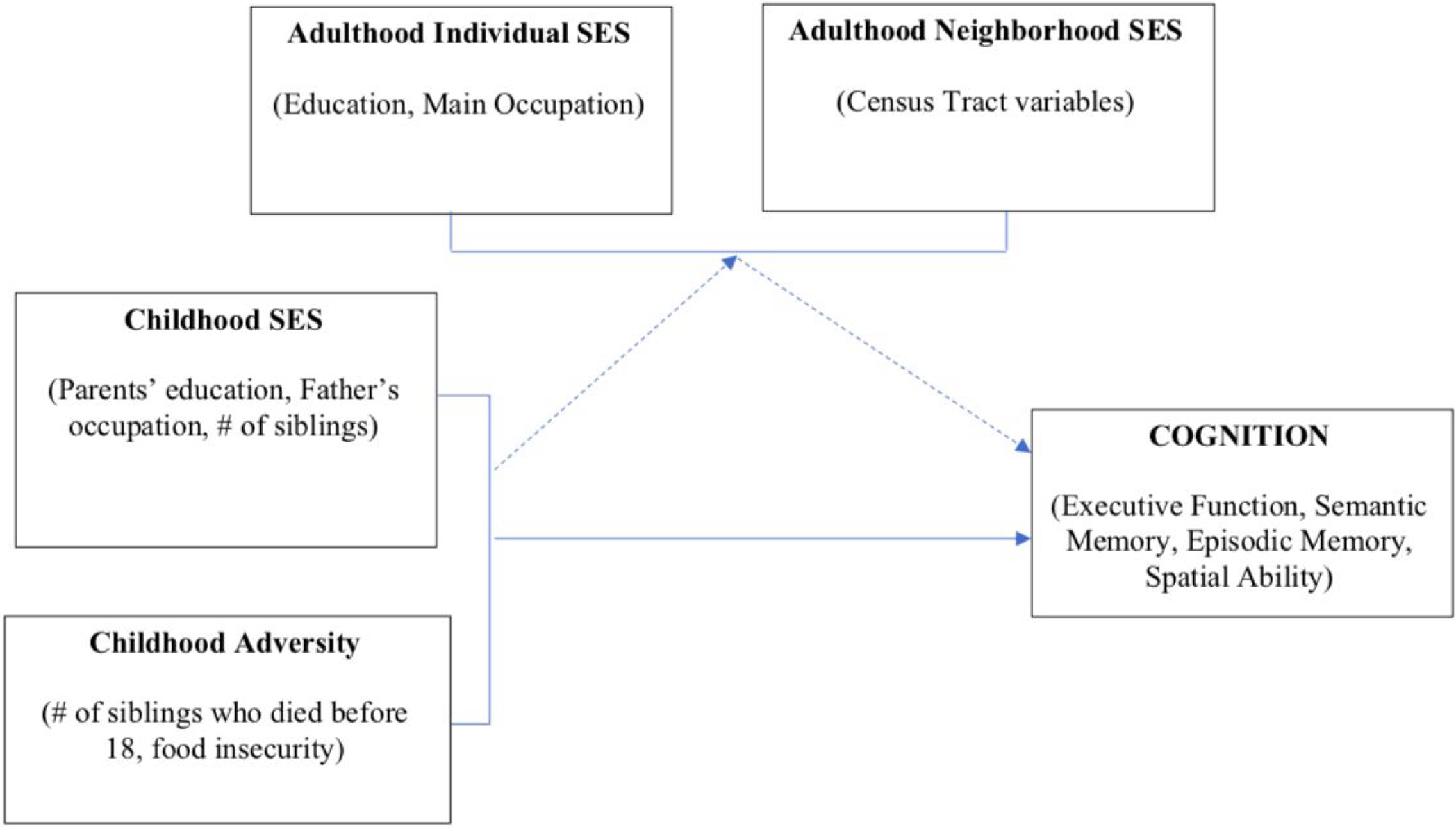
Conceptual model of effect of early life environment on late life cognition, as mediated by adulthood SES.
METHODS
Sample
The sample comprised 837 participants in an ongoing longitudinal study of cognition at the University of California, Davis Health with participants coming from the Sacramento, San Joaquin, and bay areas. There was a rolling enrollment design with initial enrollment in 2002 and additional enrollment to 2021. All participants were followed approximately annually and had at least two evaluations with a mean of 5.2 visits (SD = 3.3) and maximum of 16 visits. Approximately 70% of participants were recruited through community-based recruitment protocols designed to enhance both the racial and ethnic diversity and the spectrum of cognitive dysfunction of the sample. Recruiters utilized various outreach methods such as soliciting in a community hospital lobby, a community survey, health fairs, or word of mouth. The remainder of the sample initially sought a clinical evaluation at a memory clinic and subsequently were recruited for this study. Inclusion criterion was ability to speak English or Spanish. Exclusion criteria included unstable major medical illness, major psychiatric disorder, and active substance abuse or dependence (excluding tobacco-related disorders, see Hinton et al., 2010, for further information about the cohort). This research was approved by the institutional review board at the University of California, Davis and was completed in accordance with Helsinki Declaration; all participants provided informed consent.
Measures
Clinical evaluations.
All participants received multidisciplinary diagnostic evaluations at baseline and at approximately annual intervals. All evaluations followed the same protocol and included a detailed medical history and a physical and neurological exam. Clinical neuropsychological evaluation using standard neuropsychological tests (distinct from the outcome measures used in this study) was performed at each visit. Routine dementia work-up laboratory tests were obtained at baseline for all participants and when clinically indicated at the time of follow-up. Diagnosis of cognitive syndrome (normal, MCI, dementia) and, for individuals with dementia, identification of underlying etiology, were made according to standardized criteria. Each case at baseline was initially diagnosed at a consensus conference by the clinical team evaluating the participant. Follow-up cases were diagnosed at a case conference of the clinical team examining the participant and, in addition, were reviewed at a case adjudication conference when the examining team identified a change in the diagnosis. All diagnoses were made blind to research neuropsychological testing.
Child and Adult History Variables.
Data regarding childhood were drawn from the Life Experiences and Activities Form (LEAF), an interviewer-based instrument used to characterize experience across the participant’s life span (Brewster et al., 2014; Melrose et al., 2015). Variables of interest included mother’s education, father’s education, complexity of the father’s job (Roos & Treiman, 1980), number of siblings, number of siblings who died before age 18 (captured as two indicator variables, one coding for 1 sibling death, the second coding for two or more deaths, both with no sibling deaths as the reference, e.g., those with no siblings), and whether participant ever went hungry (0 = no, 1 = yes). The LEAF also queried participants’ educational attainment and main occupation if they were retired. Occupational complexity (of the father’s and participant’s job) ratings were taken from the Dictionary of Occupational Titles (DOT) and captured the job’s general education requirements, physical strength requirements, and hazardous work environment.
We used QGIS (QGIS Development Team, 2020) and the MMQGIS plug-in (Minn, 2020) to geocode participant addresses (at the time of LEAF assessment) along the U.S. Census Bureau’s road network for the relevant counties to produce an estimate of the geographic location of the address. Similar to prior research, neighborhoods were categorized by census tracts, an administrative boundary designated by the U.S. Census Bureau (Krieger et al., 2003). The average number of people in a census tract is 4,000; however, this number can range from 1,200–8,000 (U.S. Census Bureau, 2010). From U.S. Census Tract 2010 data, we extracted variables that cohere conceptually and correlate empirically to capture the construct of NSES (Meyer et al., 2018), including the percentage of individuals with a high school diploma, the percentage of people who owned their own home, median household income, the percentage not receiving public assistance, and percentage employed.
Cognitive outcomes.
The cognitive outcomes in this study were from the Spanish and English Neuropsychological Assessment Scales (SENAS) and were administered at all evaluations. The SENAS has undergone extensive development as a battery of cognitive tests relevant to diseases of aging (Mungas et al., 2004; Mungas et al., 2005; Mungas, Reed, Haan, et al., 2005; Mungas, Reed, Marshall, & Gonzalez, 2000). Modern psychometric methods based on item response theory were used to create psychometrically matched measures across different scales and across English and Spanish versions and appropriate for individuals with diverse education levels. SENAS tests meant to measure four cognitive domains affected by diseases of aging were assessed: executive function, semantic memory, episodic memory and spatial ability. Executive function is a composite measure constructed from component tasks of category fluency (number of animals named in 60 seconds), phonemic (letter) fluency (words beginning with the /f/ sound, words beginning with the /l/ sound), and working memory (digit-span backward, visual-span backward, list sorting). Semantic memory is a composite of highly correlated verbal (object-naming) and nonverbal (picture- association) tasks. Episodic memory is a composite score derived from a multi-trial word- list-learning test (Word List Learning 1) (Mungas et al., 2004). Spatial ability was measured using the Spatial Localization scale which assesses ability to perceive and reproduce two-dimensional spatial relationships that are increasingly complex. Measure development and psychometric characteristics are described in more detail elsewhere (Crane et al., 2008; Mungas et al., 2004; Mungas, Reed, Haan, et al., 2005). SENAS scores are presented in z- score like units where a score of zero corresponds to the mean and differences from the mean are expressed in standard deviation units.
Data Analysis
The study’s primary goal was to evaluate associations of early life adversity and SES as well as adulthood SES with late life cognitive trajectories. Confirmatory factor analysis (CFA) was used to summarize indicators of early life and adulthood indicators of SES and adversity based on the study’s conceptual model (Figure 1). Cognition was modeled as person-specific baseline levels (random effect intercepts) and linear change rates (random effect slopes) for the four cognitive outcomes. The primary model examining SES and adversity associations with cognitive trajectories regressed cognitive intercepts and global cognitive slope on early life and adulthood SES and adversity factors. We hypothesized that early life effects would be mediated at least partially by adulthood SES and tested specific paths relevant to differentiating independent and mediated effects: direct effects of adult SES on cognitive trajectory components, indirect effect of early life SES and adversity mediated by adulthood SES, and the direct (non-mediated) effects of early life SES and adversity.
Confirmatory Factor Analysis.
Modeling of early life adversity and SES and adulthood SES was conducted using CFA. The latent variable model used to estimate these traits was based on an a priori conceptual model relating the hypothesized factors to their observed indicators. Childhood (SES and adversity) and adulthood SES (individual and neighborhood SES) were conceptualized as hierarchical, second-order factors. That is, in childhood, the first-order factors were early life SES and adversity, and the second-order factor was a general childhood factor. In adulthood, the first-order factors were individual-level adult SES and neighborhood-level SES, with general adulthood SES as the second-order factor (for parsimony, we refer to these second order factors as child and adult SES). Early life SES was indicated by (1) mother’s education level, (2) father’s education level, (3) general education requirements of the participant’s father’s job, (4) strength requirements of the father’s job, and (5) the hazardous work environment of the father’s job. Residual covariances between the three father’s job variables were included a priori to account for shared variance in the source of this information. Early life adversity was indicated by participants’ number of siblings, whether participants ever went hungry as a child, and participants’ number of deceased siblings. We constrained the loading of the first-order adversity factor on the second-order childhood SES factor to be negative to account for the fact that adversity was coded in the opposite direction (higher scores reflected greater adversity) from other variables in the model.
Adulthood individual SES was indicated by (1) years of education, (2) general education requirements of the participant’s job, (3) strength requirements of the participant’s job, and (4) the hazardous work environment of the participant’s job. As with the father’s job variables, residual covariances were modeled to account for shared variance in the source of information pertaining to the participant’s job. Neighborhood-level adult SES was indicated by U.S. census tract variables mentioned above.
Three variables were modeled as categorical variables (one deceased sibling, two or more deceased siblings, and whether the participant went hungry as a child); all other variables were modeled as continuous variables and were standardized prior to analysis. The initial CFA was performed using cross-sectional SES data and the robust weighted least squares (WLSMV) estimator in Mplus version 8.6 (Muthén & Muthén, 1998–2021) to accommodate the categorical indicators. Figure 2 shows a path diagram illustrating the structure of this model. The fit of this model to the data was judged using standard fit statistics (Hu & Bentler, 2009), including the comparative fit index (CFI), Tucker-Lewis Index (TLI; CFI and TLI values > .95 represent good fit), root mean square error of approximation (RMSEA; values < .06 represent good fit), and standardized root mean square residual (SRMR; values < .08 represent good fit). Because this model fit the data well (see Results), it was subsequently incorporated into a structural mediation model, where the general adulthood factor was hypothesized to mediate the effect of the general child factor on cognitive outcomes (Figure 2).
Figure 2.
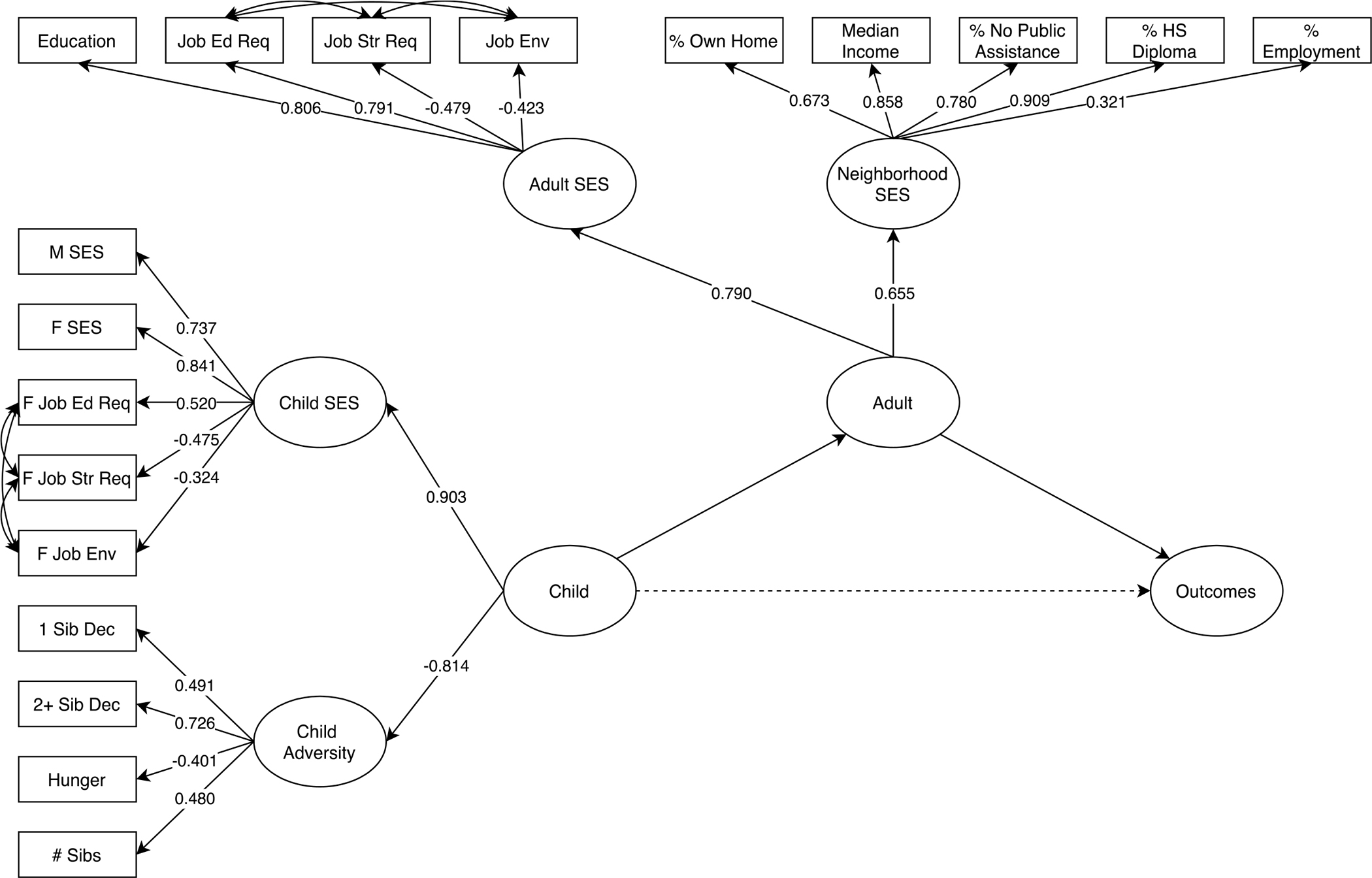
Confirmatory factor analysis model of child and adulthood SES. Covariates included age at baseline (centered at 70 years), sex, race/ethnicity, language of test administration, and recruitment source (clinic versus community). Path labels show standardized parameter estimates.
Modeling of Cognitive Trajectory Components.
SENAS measures of episodic memory, semantic memory, executive function, and spatial ability, obtained at annual study visits, were used as cognitive outcomes. These measures of cognition were transformed using the Blom inverse normal rank order transformation (Blom, 1958) to normalize these variables and establish a common scale (M = 0, SD = 1). Mixed effects, parallel process longitudinal analyses were performed using Mplus version 8.6 multilevel modeling (Muthén & Muthén, 1998–2021). The approach to modeling longitudinal change (Figure 3) in this cohort has been described in detail elsewhere (Fletcher et al., 2018; Gavett et al., 2018). Briefly, in the Within part of this model, each of the four cognitive outcomes was regressed on time (years) in study. The Within model generated person-specific intercept and linear slope random effects for each outcome. These random effects then served as dependent variables in the Between part of the model. The Within model included a term to account for practice effects and a practice effect by Spanish test administration interaction that has been identified in previous studies with this sample (Early et al., 2013; Melrose et al., 2015). We compared a series of models to determine whether intercepts and slopes could be summarized by second-order factors. As described in previous work modeling SENAS outcomes, the best fit was obtained with a model that had a global slope second-order factor that accounted for covariance among the four slope random effects but individual intercept random effects (Fletcher et al., 2018). Modeling late-life cognitive decline as a unitary construct is also consistent with recent meta-analytic studies of cognitive aging (Tucker-Drob, Brandmaier, & Lindenberger, 2019).
Figure 3.
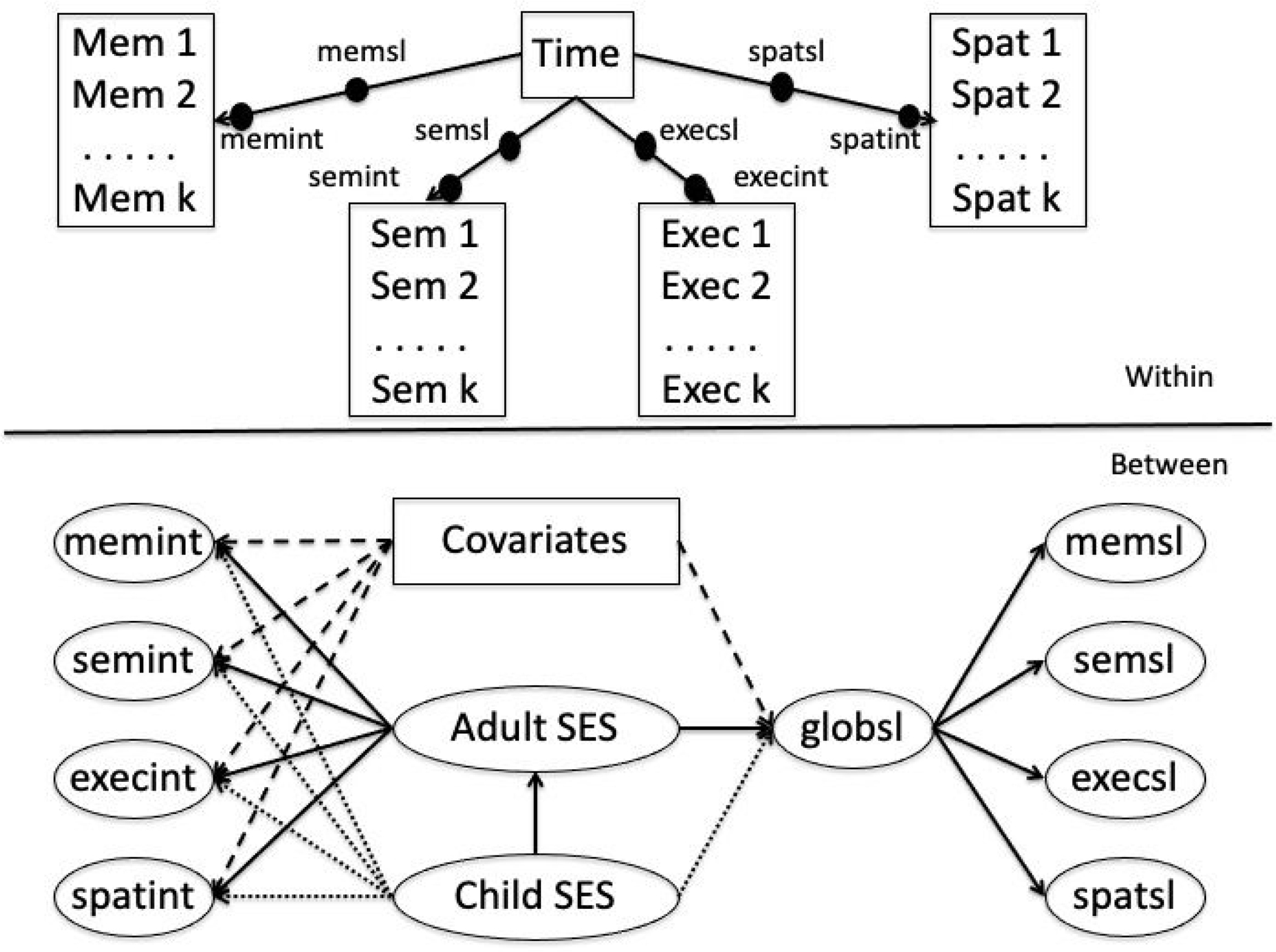
Analytic model to evaluate effects of SES on cognitive trajectory components.
Associations of Child and Adulthood SES with Cognitive Trajectory Components.
The child and adult second-order factors were the predictor and mediator variables of interest, respectively. Covariates included age at baseline (centered at 70 years), sex, race/ethnicity, language of test administration, and recruitment source (clinic versus community). Dichotomous/categorical covariates were transformed into indicator variables such that a variable with k response categories was captured by k-1 dichotomous indicator variables.
SES indicators and covariates were added to the Between part of the multilevel longitudinal models as independent variables to explain cognitive trajectory components. The same hierarchical factor structure that was identified in the cross-sectional CFA was estimated within the Between part of the multilevel longitudinal model. The Within (cognitive trajectory components) and Between (SES first and second order factors, regressions of cognitive intercepts and global slope on SES factors) parts of this model were simultaneously estimated using the Bayes estimator option in Mplus. This estimator employs a Markov Chain Monte Carlo (MCMC) algorithm with a Gibbs (PX1; Asparouhov & Muthén, 2010) sampler. The most extreme 2.5% of values in the lower and upper tails of the posterior distribution (derived from 25,000 MCMC iterations) were chosen as the 95% credible intervals for the parameter estimates. Credible intervals not overlapping 0 indicate a < 5% chance of a null population-level effect.
Child and adult SES were highly correlated (r ~ .70) and there were problems with convergence when independent effects of these two factors on cognitive outcomes were included in the same model. To address this convergence issue, we estimated the direct and mediated effects of interest using a 2-step modeling process. Step 1: cognitive trajectory components were regressed on early life alone, yielding a child total effect. Step 2: cognitive trajectory components were regressed on adult SES, adult SES was regressed on child, and the child direct effects on cognitive intercepts and global slope were fixed at 0. The child indirect effect mediated by adult SES was estimated in this model. Step 3: the child direct (non-mediated) effect was estimated by subtracting the child indirect effect estimated in Step 2 from the child total effect estimated in Step 1.
Missing Data.
The full sample (N=837) had longitudinal cognitive outcomes for two or more assessments. SES and adversity variables were not available for the full sample, and availability of indicators for SES factors ranged from 55% (neighborhood SES) to 100% (adult SES). The missing data analysis option within Mplus was used for the model that simultaneously estimated SES factors and regressed cognitive intercept and slope random effects on these factors. Bayesian modeling with missing data in Mplus gives asymptotically the same results as maximum-likelihood estimation under assumptions of missing at random (MAR), which means that missingness can be a function of observed covariates and observed outcomes (Muthén & Muthén, 1998–2017). Missing at random is also satisfied when missingness is by design; an important reason for missing values in SES and adversity indicators was that this data was collected mid-course in rolling enrollment of this longitudinal cohort and so was obtained only for individuals who were being actively followed at that time.
RESULTS
Sample Characteristics
In this sample, mean follow-up time was 5.2 years (SD = 4.0). Participant characteristics are presented in Table 1. About 40% of the sample were men. Average age was 75 years and average education was 13.6 years. Slightly under 50% of the sample were non-Hispanic/Latino White, 24% were Black, 22% were Hispanic/Latino, and 5.5% were other race/ethnicities (all indicated by self-report). Spanish administration of tests occurred in 97 individuals (12%), all Hispanics/Latinos. All others were tested in English. Seventy percent were recruited from the community. At baseline, about 11% had a diagnosis of dementia, 31% had MCI, and 54% were cognitively normal. Indicators for childhood SES were available for 68% of the sample, while 69% had indicators for childhood adversity; 100% had at least one indicator for adult SES; and neighborhood SES data was available for 55%.
Table 1.
Sample characteristics (N = 837)
| n (%) | |
|---|---|
|
| |
| Gender | |
| Men | 336 (40.1%) |
| Women | 501 (59.9%) |
| Age at baseline (years) | |
| Mean (SD) | 75.3 (7.24) |
| Median [Min, Max] | 75.0 [49.0, 93.0] |
| Education (years) | |
| Mean (SD) | 13.6 (4.41) |
| Median [Min, Max] | 14.0 [0, 20.0] |
| Race/Ethnicity | |
| Black | 201 (24.0%) |
| Hispanic/Latino | 184 (22.0%) |
| White | 406 (48.5%) |
| Other | 46 (5.5%) |
| Language of Test Administration | |
| English | 740 (88.4%) |
| Spanish | 97 (11.6%) |
| Number of Assessments | |
| Mean (SD) | 5.18 (3.26) |
| Median [Min, Max] | 4.00 [2.00, 16.0] |
| Follow-up Time (years) | |
| Mean (SD) | 5.20 (4.00) |
| Median [Min, Max] | 3.96 [0.723, 17.0] |
| Recruitment Source | |
| Clinic | 202 (24.1%) |
| Community | 584 (69.8%) |
| Syndrome Diagnosis | |
| Dementia | 93 (11.1%) |
| MCI | 259 (30.9%) |
| Normal | 454 (54.2%) |
| Child SES Data Available | |
| No | 265 (31.7%) |
| Yes | 572 (68.3%) |
| Child Adversity Data Available | |
| No | 253 (30.2%) |
| Yes | 584 (69.8%) |
| Adult SES Data Available | |
| Yes | 837 (100%) |
| Neighborhood SES Data Available | |
| No | 380 (45.4%) |
| Yes | 457 (54.6%) |
Confirmatory Factor Analysis of Child and Adult SES
Figure 2 shows estimated loadings and path coefficients for the a priori CFA model. When applied to cross-sectional SES indicator data, this model showed adequate fit to the data (RMSEA = 0.035 (90% CI = 0.028–0.041), CLI = 0.934, TLI = 0.919, SRMR = 0.083). There were strong loadings (>0.7) for 8 of the indicators for the 4 first-order factors and at least moderate loadings (>0.3) for the others. There were strong loadings of the first-order factors on the hypothesized second-order factors, supporting the hypothesized associations of these two pairs of variables. The correlation between second-order child and adult factors was 0.70, indicating that child and adult SES were strongly but not perfectly related.
Effects of Child and Adult SES on Cognitive Trajectory Components
Table 2 shows results of models examining direct and mediated effects of child and adult factors on global cognitive slope and individual intercepts. The adult total effect and child indirect effect in Table 2 are from the Step 2 analysis where cognition was regressed on the adult factor (adult total effect) and adult factor was regressed on child (yielding the mediated, child indirect effect). The child total effect is from the Step 1 analysis where child SES alone explains cognition, and the child direct effect is depicted as the percent of the child total effect not explained by the child indirect effect. Global cognitive slope was not significantly explained by the adult total effect, the child total effect, or the child indirect effect (95% credible intervals included 0). The child indirect effect accounted for 87.5% of the child total effect on global cognitive slope. For cognitive intercepts, adult total effect, child total effect, and child indirect effect all were robustly different from 0. Adult and child factors exerted stronger associations with semantic memory, executive function, and spatial ability intercepts than the episodic memory intercept. For the episodic memory intercept, a 1 SD difference in adult SES was associated with a 0.28 SD difference in episodic memory, a 1 SD difference in child SES was associated with a 0.27 SD difference, and the indirect effect of a 1 SD difference in child SES accounted for a 0.20 SD difference. The child indirect effect on episodic memory intercept, mediated via adult SES, accounted for about 75% of the child total effect, whereas the indirect effect accounted for about 69% of the total effect for the other three cognitive intercepts.
Table 2.
Effects of Early Life Factors on Cognitive Trajectory Components: Adult Total Effects, Child Total Effects, and Indirect Effect of Child Mediated by Adulthood SES.
[Child effect on Adult = 0.719 (0.586, 0.852)]
| Cognitive Outcome | Adult Total Effect* | Child Indirect Effect* | Child Total Effect* | Child Direct (% Total) | Percent Mediated by Adult |
|---|---|---|---|---|---|
|
| |||||
| Global Cognitive Slope | 0.010 (−0.004, 0.025) | 0.007 (−0.003, 0.018) | .0008 (−0.007, 0.024) | 12.5% | 87.5% |
| Verbal Episodic Memory Intercept | 0.284 (0.204, 0.370) | 0.203 (0.143, 0.270) | 0.269 (0.182, 0.354) | 24.5% | 75.5% |
| Semantic Memory Intercept | 0.382 (0.299, 0.475) | 0.273 (0.205, 0.351) | 0.401 (0.320, 0.483) | 31.9% | 68.1% |
| Executive Function Intercept | 0.457 (0.367, 0.556) | 0.327 (0.251, 0.410) | 0.475 (0.389, 0.559) | 31.2% | 68.8% |
| Spatial Intercept | 0.344 (0.257, 0.443) | 0.247 (0.179, 0.324) | 0.357 (0.269, 0.447) | 30.8% | 69.2% |
Note. Covariates included age at baseline (centered at 70 years), sex, race/ethnicity, language of test administration, and recruitment source (clinic versus community).
Unstandardized regression coefficients (95% credible intervals in parentheses).
Summary of Results
Child and adult SES factors were related to one another; both showed associations with individual cognitive intercepts that were slightly weaker for episodic memory, and the indirect child SES effect that was mediated by adult SES accounted for 68–75% of the total child effect. Child and adult SES were not related to global cognitive slope.
DISCUSSION
In the current study, we examined the direct and indirect – as mediated by adulthood SES – effects of early life environment (SES and adversity) on cognition. We elaborated upon usual models that study SES and cognition by including early life adversity and SES separately, as well as by examining individual and neighborhood level SES. Our results indicated that child and adult factors were not associated with longitudinal cognitive decline, but both were related to level of (i.e., cross-sectional) cognition. This indicates that sociocontextual factors are associated with level of cognitive performance attained in adulthood more than they are with rate of late-life cognitive change. Our finding is supported by a robust literature suggesting that childhood SES and adversity are associated with initial levels of cognition with which people enter into later life (Everson-Rose et al., 2003; Glymour et al., 2012; Peterson et al., 2021).
The finding SES associations with cognitive intercepts, in contrast to the non-significant associations with cognitive decline, has important implications. Baseline cognition provides an estimate of a person’s performance at a specific point in time, and is the net result of many variables including sociocontextual and life experience variables and even familiarity with cognitive testing. In contrast, changes in brain health (e.g., conversion from MCI to dementia) are strongly associated with late life cognitive decline (see Fletcher, 2018 and others). Our study found no significant effect of SES variables on cognitive change, despite the sample including substantial heterogeneity in brain health, as indicated by heterogeneity of diagnoses (normal, MCI, dementia). In previous work, we did find that the relationship between SES and cognitive change varied as a function of brain health states (normal, MCI, dementia) (Meyer et al., 2018); however, these findings were exploratory given the small sample size and future work with larger samples should explore this question.
We hypothesized that early life effects would be partially mediated by adult SES and this hypothesis was supported. Everson and colleagues (2003) used data from Chicago Health and Aging Project and found that childhood socioeconomic position was associated with global baseline cognition in later life, but not with change in cognition, and that adult SES accounted for some, but not all of the association. Childhood SES may allow for enriched opportunities and fewer stressors that then lead to higher adulthood SES. Coming from a higher SES childhood environment has been associated with increased likelihood of engaging in cognitively stimulating activities as an adult (Beck et al., 2018). These findings are consistent with the majority of research conducted in other national contexts, which has found that SES in adulthood partially accounts for associations between childhood SES and later life cognition (Fors et al., 2009; Horvat et al., 2014; Zhang, Gu, & Hayward, 2008).
In contrast to the mediated effect on episodic memory, the direct effects of early life and adulthood SES were stronger in terms of their association with executive function, semantic memory, and spatial ability. This is also consistent with other studies. Using data from the Wisconsin Longitudinal Study, Greenfield and Moorman (2019) found that childhood SES was more strongly associated with language and executive function than with memory. These results are consistent with research on children, showing that particular environmental conditions—such as SES and cognitive stimulation in the home—are most robustly associated with aspects of cognition such as language, attention, and other executive functions (Peyre et al., 2016). Our own research examining NSES has found its association to be stronger with domains such as semantic memory rather than with episodic memory (Meyer et al., 2018). This suggests that episodic memory is somewhat less influenced by sociocontextual influences than are other cognitive abilities. It may be because neighborhood variables such as SES play a more significant role in cognitive processes that are influenced by social contextual life experiences, which may be captured and reflected in measures of semantic memory (Mungas, Reed, Haan et al., 2005).
Study limitations include the potential lack of generalizability to geographic areas outside Northern California. Given our smaller sample of Black and Hispanic/Latino participants, we did not have the power to detect race/ethnicity-stratified associations of early life experiences and cognition. As with most studies of older adults, our measure of early life adversity and SES was retrospective and may be subject to recall bias. Moreover, there are potentially many other ways individuals experience early life adversity that were not captured in our study (e.g., emotional and physical abuse). Although we accounted for individual and NSES in the models, it is possible that our findings are due to residual confounding of childhood health variables not measured in this study, such as birth weight, child nutrition, and prenatal measures—all which have been found to be associated with adult cognition (e.g., Grove, Lim, Gale, & Shenkin, 2017). The LEAF was collected at various points during the data collection period. Given that we used Census 2010 indicators of NSES and also were not able to assess residential tenure and relocation, there is potential for reverse causality (e.g., those with better cognition move into higher SES neighborhoods) and the inability to capture change in neighborhoods. Lastly, we did not include a measure of SES at distinct points throughout later childhood and adulthood, but this would be a logical next step in future research.
We add to the literature by including an ethnically, linguistically, and educationally diverse sample with long follow-up. Longitudinal studies have methodological advantages over cross-sectional ones in the study of cognitive aging; they allow for the dissociation of baseline cognitive performance from cognitive change, which is essential for understanding the unique – and potentially modifiable – contributors to each. Additionally, having more diversity in ethnicity/race also provides us more diversity and variation in NSES and allows for more generalizability across different ethnic groups. We employed psychometrically sophisticated, clinically relevant cognitive outcome measures—semantic memory, executive function, episodic memory, and spatial ability—that have been developed and validated for culturally and linguistically diverse groups (Mungas et al., 2004; Mungas, Reed, Farias et al., 2005; Mungas, Reed, Haan et al., 2005). These cognitive measures were developed using modern psychometric methods based on item response theory and to have psychometric characteristics that are optimized for longitudinal research. Our sample is also diverse in cognitive function across the full spectrum, from normal function to dementia. This enhances heterogeneity in cognitive trajectories and facilitates exploration of variables that contribute to cognitive decline. Lastly, we used rigorous CFA methods to develop empirically justified factor measures of SES and adversity and evaluated associations of SES factors with cognitive trajectories in a model that simultaneously estimated all parameters.
In conclusion, this study contributes empirical evidence to the literature on early life factors including adversity and SES as important variables associated with cognition, specifically in terms of initial levels of cognition in later life and especially in non-episodic memory domains. Future studies should delineate additional pathways through which early life influences cognition in later life (e.g., health behaviors). Pursuing this line of research has implications for policy, prevention, and intervention to optimize cognition in vulnerable older adults.
Acknowledgements
Funding:
This study was funded by grants from the National Institute on Aging [P30AG072972, R01AG067541, K01AG052646, R01AG052132, RF1AG050782] and the Alzheimer’s Association [AARGD-19-619832].
Footnotes
Conflict of Interest: None to Disclose.
References
- Aartsen MJ, Cheval B, Sieber S, Van der Linden BW, Gabriel R, Courvoisier DS… & Cullati S (2019). Advantaged socioeconomic conditions in childhood are associated with higher cognitive functioning but stronger cognitive decline in older age. Proceedings of the National Academy of Sciences, 116(12), 5478. 10.1073/pnas.1807679116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Asparouhov T, & Muthén B (2010). Bayesian analysis of latent variable models using Mplus (Technical report). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Barnes LL, Wilson RS, Everson-Rose SA, Hayward MD, Evans DA, & Mendes de Leon CF (2012). Effects of early-life adversity on cognitive decline in older African Americans and whites. Neurology, 79(24), 2321. 10.1212/WNL.0b013e318278b607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck A, Franz CE, Xian H, Vuoksimaa E, Tu X, Reynolds CA…& Kremen WS (2018). Mediators of the effect of childhood socioeconomic status on late midlife cognitive abilities: A four decade longitudinal study. Innovation in Aging, 2(1). 10.1093/geroni/igy003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blom G (1958). Statistical Estimates and Transformed Beta-Variables. New York: Wiley. [Google Scholar]
- Brewster PWH, Melrose RJ, Marquine MJ, Johnson JK, Napoles A, MacKay-Brandt A….& Mungas D (2014). Life experience and demographic influences on cognitive function in older adults. Neuropsychology, 28(6), 846–858. 10.1037/neu0000098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clarke PJ, Ailshire JA, House JS, Morenoff JD, King K, Melendez R, & Langa KM (2012). Cognitive function in the community setting: The neighbourhood as a source of “cognitive reserve”? Journal of Epidemiology and Community Health, 66(8), 730–736. 10.1136/jech.2010.128116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Comijs HC, Beekman AT, Smit F, Bremmer M, van Tilburg TT, & Deeg DJ (2007). Childhood adversity, recent life events and depression in late life. Journal of Affective Disorders, 103:243–246. [DOI] [PubMed] [Google Scholar]
- Crane PK, Narasimhalu K, Gibbons LE, Pedraza O, Mehta KM, Tang Y….& Mungas DM (2008). Composite scores for executive function items: Demographic heterogeneity and relationships with quantitative magnetic resonance imaging. Journal of the International Neuropsychological Society 14(5), 746–759. 10.1017/S1355617708081162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Early DR, Widaman KF, Harvey D, Beckett L, Park LQ, Farias ST, … Mungas D (2013). Demographic predictors of cognitive change in ethnically diverse older persons. Psychology and Aging, 28(3), 633–645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ertel KA, Glymour MM, & Berkman LF (2008). Effects of social integration on preserving memory function in a nationally representative US elderly population. American Journal of Public Health, 98(7), 1215–1220. 10.2105/AJPH.2007.113654 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Everson-Rose SA, Mendes de Leon CF, Bienias JL, Wilson RS, & Evans DA (2003). Early life conditions and cognitive functioning in later life. American Journal of Epidemiology, 158(11), 1083–1089. 10.1093/aje/kwg263 [DOI] [PubMed] [Google Scholar]
- Fletcher E, Gavett B, Harvey D, Farias ST, Olichney J, Beckett L… Mungas D (2018). Brain volume change and cognitive trajectories in aging. Neuropsychology, 32(4), 436–449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fors S, Lennartsson C, & Lundberg O (2009). Childhood living conditions, socioeconomic position in adulthood, and cognition in later Life: Exploring the associations. The Journals of Gerontology: Series B, 64B(6), 750–757. 10.1093/geronb/gbp029 [DOI] [PubMed] [Google Scholar]
- Gavett BE, Fletcher E, Harvey D, Farias ST, Olichney J, Beckett L… Mungas D (2018). Ethnoracial differences in brain structure change and cognitive change. Neuropsychology, 32(5), 529–540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- George KM, Peterson RL, Gilsanz P, Barnes LL, Mayeda ER, Glymour MM…. & Whitmer RA (2021). Stroke Belt birth state and late-life cognition in the Study of Healthy Aging in African Americans (STAR). Annals of Epidemiology, 64, 26–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gill TM, Richardson ED, & Tinetti ME (1995). Evaluating the risk of dependence in activities of daily living among community-living older adults with mild to moderate cognitive impairment. The Journals of Gerontology: Series A, 50A(5), M235–M241. 10.1093/gerona/50A.5.M235 [DOI] [PubMed] [Google Scholar]
- Gilsanz P, Mayeda ER, Glymour MM, Quesenberry CP, & Whitmer RA (2017). Association between birth in a high stroke mortality state, race, and risk of dementia. JAMA Neurology, 74, 1056–1062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glass TA, Rasmussen MD, & Schwartz BS (2006). Neighborhoods and obesity in older adults: The Baltimore Memory Study. American Journal of Preventive Medicine, 31(6), 455–463. 10.1016/j.amepre.2006.07.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glymour MM, Tzourio C, & Dufouil C (2012). Is cognitive aging predicted by one’s own or one’s parents’ educational level? Results from the three-city study. American Journal of Epidemiology, 175(8), 750–759. 10.1093/aje/kwr509 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenfield EA, & Moorman SM (2019). Childhood socioeconomic status and later life cognition: Evidence from the Wisconsin Longitudinal Study. Journal of Aging and Health, 31(9), 1589–1615. 10.1177/0898264318783489 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grove BJ, Lim SJ, Gale CR, & Shenkin SD (2017). Birth weight and cognitive ability in adulthood: A systematic review and meta-analysis. Intelligence, 61, 146–158. [Google Scholar]
- Hinton L, Carter K, Reed BR, Beckett L, Lara E, DeCarli C, & Mungas D (2010). Recruitment of a community-based cohort for research on diversity and risk of dementia. Alzheimer Disease and Associated Disorders, 24(3), 234–241. 10.1097/WAD.0b013e3181c1ee01 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horvat P, Richards M, Malyutina S, Pajak A, Kubinova R, Tamosiunas A….& Bobak M (2014). Life course socioeconomic position and mid-late life cognitive function in Eastern Europe. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 69(3), 470–481. 10.1093/geronb/gbu014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C…. & Dunne MP (2017). The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. The Lancet. Public health, 2(8), e356–e366. [DOI] [PubMed] [Google Scholar]
- Korten NCM, Penninx BWJH, Pot AM, Deeg DJH, & Comijs HC (2014). Adverse Childhood and Recent Negative Life Events: Contrasting Associations with Cognitive Decline in Older Persons. Journal of Geriatric Psychiatry and Neurology, 27(2), 128–138. 10.1177/0891988714522696 [DOI] [PubMed] [Google Scholar]
- Luo Y, & Waite LJ (2005). The impact of childhood and adult SES on physical, mental, and cognitive well-being in later life. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 60(2), S93–S101. 10.1093/geronb/60.2.s93 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Melrose RJ, Brewster P, Marquine MJ, MacKay-Brandt A, Reed B, Farias ST, & Mungas D (2015). Early life development in a multiethnic sample and the relation to late life cognition. Journals of Gerontology, Psychological and Social Sciences, 70, 519–531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer OL, Mungas D, King J, Hinton L, Farias S, Reed B, DeCarli C, Geraghty E, & Beckett L (2018). Neighborhood socioeconomic status and cognitive trajectories in a diverse longitudinal cohort. Clinical Gerontologist, 41(1), 82–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer OL, Sisco SM, Harvey D, Zahodne LB, Glymour MM, Manly JJ, & Marsiske M (2017). Neighborhood predictors of cognitive training outcomes and trajectories in ACTIVE. Research on Aging, 39, 443–467. 10.1177/0164027515618242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Minn M (2021). MMQGIS, Version 2020.01.16. https://michaelminn.com/linux/mmqgis/ [Google Scholar]
- Morris JC (1993). The Clinical Dementia Rating (CDR). Neurology, 43(11), 2412. 10.1212/WNL.43.11.2412-a [DOI] [PubMed] [Google Scholar]
- Mungas D, Reed BR, Crane PK, Haan MN, & González H (2004). Spanish and English Neuropsychological Assessment Scales (SENAS): Further development and psychometric characteristics. Psychological Assessment, 16(4), 347. [DOI] [PubMed] [Google Scholar]
- Mungas D, Reed BR, Haan MN, & González H (2005). Spanish and English neuropsychological assessment scales: Relationship to demographics, language, cognition, and independent function. Neuropsychology, 19(4), 466. [DOI] [PubMed] [Google Scholar]
- Mungas D, Reed BR, Marshall SC, & González HM (2000). Development of psychometrically matched English and Spanish language neuropsychological tests for older persons. Neuropsychology, 14(2), 209. [DOI] [PubMed] [Google Scholar]
- Mungas D, Reed BR, Tomaszewski Farias S, & DeCarli C (2005). Criterion-referenced validity of a neuropsychological test battery: Equivalent performance in elderly Hispanics and non-Hispanic Whites. Journal of the International Neuropsychological Society, 11(5), 620–630. 10.1017/S1355617705050745 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén L, & Muthén B (1998–2021). Mplus user’s guide Eighth edition Los Angeles. CA: Muthén & Muthén, 2017. [Google Scholar]
- Noble KG, Engelhardt LE, Brito NH, Mack LJ, Nail EJ, Angal J….& PASS Network. (2015). Socioeconomic disparities in neurocognitive development in the first two years of life. Developmental Psychobiology, 57(5), 535–551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oveisgharan S, Wilson RS, Yu L, Schneider JA, & Bennett DA (2020). Association of early-life cognitive enrichment with Alzheimer Disease pathological changes and cognitive decline. JAMA Neurology, 77(10), 1217–1224. 10.1001/jamaneurol.2020.1941 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson RL, George KM, Gilsanz P, Mayeda ER, Glymour MM, Meyer OL….& Whitmer RA (2021). Lifecourse socioeconomic changes and late-life cognition in a cohort of U.S.-born and U.S. immigrants: Findings from the KHANDLE study. BMC Public Health, 21, 920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peyre H, Bernard JY, Hoertel N, Forhan A, Charles M-A, De Agostini M….& EDEN Mother-Child Cohort Study Group. (2016). Differential effects of factors influencing cognitive development at the age of 5-to-6 years. Cognitive Development, 40, 152–162. [Google Scholar]
- QGIS: QGIS Development Team (2020). QGIS Geographic Information System, Version 3.16.14 QGIS Association. http://www.qgis.org. [Google Scholar]
- Reed BR, Dowling M, Tomaszewski Farias S, Sonnen J, Strauss M, Schneider JA….& Mungas D (2011). Cognitive activities during adulthood are more important than education in building reserve. Journal of the International Neuropsychological Society, 17(4), 615–624. 10.1017/s1355617711000014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosso AL, Flatt JD, Carlson MC, Lovasi GS, Rosano C, Brown AF….& Gianaros PJ (2016). Neighborhood socioeconomic status and cognitive function in late life. American Journal of Epidemiology, 183(12), 1088–1097. 10.1093/aje/kwv337 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saenz JL, Downer B, Garcia MA, Wong R Cognition and context: rural-urban differences in cognitive aging among older Mexican adults. (2018). Journal of Aging and Health, 30, 965–986. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheffield KM, & Peek MK (2009). Neighborhood context and cognitive decline in older Mexican Americans: Results from the Hispanic Established Populations for Epidemiologic Studies of the Elderly. American Journal of Epidemiology, 169(9), 1092–1101. 10.1093/aje/kwp005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shih RA, Ghosh-Dastidar B, Margolis KL, Slaughter ME, Jewell A, Bird CE….& Espeland MA (2011). Neighborhood socioeconomic status and cognitive function in women. American Journal of Public Health, 101(9), 1721–1728. 10.2105/AJPH.2011.300169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stern Y (2009). Cognitive reserve. Neuropsychologia, 47(10), 2015–2028. 10.1016/j.neuropsychologia.2009.03.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tucker-Drob EM, Brandmaier AM, & Lindenberger U (2019). Coupled cognitive changes in adulthood: A meta-analysis. Psychological Bulletin, 145(3), 273–301. 10.1037/bul0000179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turrell G, Lynch JW, Kaplan GA, Everson SA, Helkala E-L, Kauhanen J, & Salonen JT (2002). Socioeconomic position across the lifecourse and cognitive function in late middle age. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 57(1), S43–51. 10.1093/geronb/57.1.s43 [DOI] [PubMed] [Google Scholar]
- U.S. Census Bureau. Glossary. Retrieved from https://www.census.gov/programs-surveys/geography/about/glossary.html#:~:text=Census%20tracts%20generally%20have%20a,optimum%20size%20of%204%2C000%20people.
- Wight RG, Aneshensel CS, Miller-Martinez D, Botticello AL, Cummings JR, Karlamangla AS, & Seeman TE (2006). Urban neighborhood context, educational attainment, and cognitive function among older adults. American Journal of Epidemiology, 163(12), 1071–1078. 10.1093/aje/kwj176 [DOI] [PubMed] [Google Scholar]
- Yang L, & Wang Z (2020). Early-life conditions and cognitive function in middle-and old-aged Chinese adults: A longitudinal study. International Journal of Environmental Research and Public Health, 17(10), 3451. 10.3390/ijerph17103451 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeki Al Hazzouri A, Haan MN, Kalbfleisch JD, Galea S, Lisabeth LD, & Aiello AE (2011). Life-course socioeconomic position and incidence of dementia and cognitive impairment without dementia in older Mexican Americans: Results from the Sacramento Area Hispanic Study on Aging. American Journal of Epidemiology, 173(10), 1148–1158. 10.1093/aje/kwq483 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang Z, Gu D, & Hayward MD (2008). Early life influences on cognitive impairment among oldest old Chinese. The Journals of Gerontology: Series B, 63(1), S25–S33. 10.1093/geronb/63.1.S25 [DOI] [PubMed] [Google Scholar]