

ABSTRACT
Introduction:
Endodontic mistakes, also known as procedural accidents, are those bad events that occur during treatment, some of which are attributable to a lack of attention to detail and others of which are completely unforeseeable. The second most frequent reason for root canal failure is perforation.
Aims and Objective:
The current in vitro study’s objective was to assess the furcal perforation’s potential to be sealed with and without internal matrix by MTA flow, Biodentine, and pro-root MTA.
Materials and Methods:
60 samples were allocated into six groups at random (10 each). In intact permanent mandibular first and second teeth, furcal perforation sites were made and sealed with various materials. Following perforation sealing, the specimens’ capacity for sealing was evaluated using the dye penetration method.
Result:
The current study’s findings indicated that Group 2 has the least amount of microleakage and Group 5 has the most.
Conclusion:
Biodentine has excellent sealing capabilities and can be utilised to heal furcation perforations with or without internal matrix.
KEYWORDS: Endodontic failures, root canal perforation, sealing materials
INTRODUCTION
Procedural accidents, also known as endodontic mishaps, are unlucky events that occur during treatment. Some are caused by a lack of attention to detail, while others are completely unanticipated. Failure to grasp the rationale behind the endodontic treatment and its thorough knowledge can increase the occurrence of various complications.[1] The second most frequent reason for root canal failure is perforation.[1-3]
The location, size, periodontal health, amount of time the perforation is exposed to contamination, ability to seal the perforation, sterility of the canal, biocompatibility of the material, accessibility to the main canal, etc., all affect the prognosis for a tooth with a perforation.[3-5] Internal matrix idea for the treatment of the perforation was introduced in order to prevent the extrusion of the material used for repair material into the surrounding structures, such as periodontal ligament and bone, during root perforation closure either collagen, hydroxyappetite or calcium sulphate make up the interior matrix. The current in vitro study’s objective was to assess the furcal perforation’s potential to be sealed by MTA flow, Biodentine and pro-root MTA employing the dye-penetration method, a leakage assessment technique.
MATERIALS AND METHODS
The samples were cleaned off from debris and residual tissues with the help of an ultrasonic scaler (Woodpecker Ultrasonic Scaler UDS P) and stored in the solution of 2% Glutaraldehyde (Korsolex Rapid, Hartman) for 5 days for disinfection. Inclusion criteria includes freshly extracted intact human permanent mandibular molar teeth, teeth without any caries, calcification, any previous treatment, teeth extracted for periodontal reasons and teeth with non-fused roots and well-developed roots. Teeth with cracks and resorption and fractured teeth were excluded.
A standard endodontic access opening was prepared using carbide round bur followed by Endo-Z (Dentsply, Maillefer, Ballaigeus, Switzerland) bur in specimen. After that, teeth were decoronated with a diamond disc while continuously cooling under water 4 millimetres above the cement-enamel junction. Similar to that, roots were amputed at mid-root level. Temporary filling material (Orafil-G) was placed to seal over the orifice and the apical end of each canal. Perforations were made in the furcation area with No. 4 Round carbide bur which is 2 mm in diameter.
Specimens were separated into six groups each consist of 10 specimen (n = 10) [Table 1].
Table 1.
Study groups
| Group No. | Material | With or without internal matrix |
|---|---|---|
| 1 | Biodentine | Without |
| 2 | Biodentine | With |
| 3 | Pro-root MTA | Without |
| 4 | Pro-root MTA | With |
| 5 | MTA Flow | Without |
| 6 | MTA Flow | With |
Internal matrix of 3 mm was placed at the furcal perforation site in the respective groups. Each repair material was prepared and placed into the perforation defect to the level of the pulpal chamber floor, then mixed as per guidelines. For the purpose of simulating a clinical setting while the root was being repaired, a cotton pellet was used to inertly hydrate it. The access cavity was filled with composite resin after 24 hours. For two days, every tooth was placed in a thermocycling machine.
With the exception of the area around the perforation area, the surfaces of the molars, including the access filling, were entirely covered by two successive coats of clear varnish, allowing the dye to only pass through the perforation location. The specimen was soaked in a 2% methylene blue dye solution for 48 hours, followed by a 30-minute rinse under running water. The level of the pulpal floor to the outer edges of the perforated cavity was used to determine the real value of dye leakage in each area. Using a stereomicroscope, the maximal dye penetration along the buccal and lingual walls of the mesial or distal portion was noted (×10).
RESULTS
Microleakage in group 1 specimen (Biodentine without internal matrix) ranges from 1.26 mm to 1.33 mm. Microleakage in group 2 specimen (Biodentine with internal matrix). ranges from 1.48 mm to 1.53 mm. Specimen of group 3 (pro-root MTA without internal matrix) showed more microleakage than group 4 (pro-root MTA with internal matrix). Specimen of group 5 (MTA flow without internal matrix) showed more microleakage than group 6 (MTA flow with internal matrix). The mean microleakage scores for the experimental groups 1, 2, 3, 4, 5 and 6 are 1.50, 1.29, 1.70, 1.50, 1.90 and 1.70 mm, respectively. Where Group 2 has minimum microleakage and group 5 has maximum microleakage [Figure 1].
Figure 1.
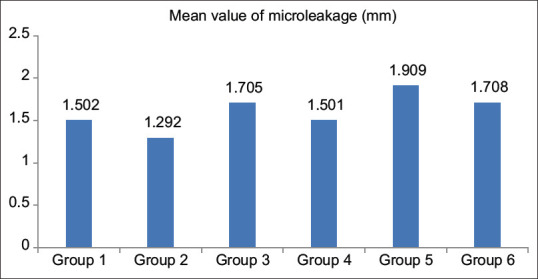
Mean microleakage in all 6 groups
DISCUSSION
Most common endodontic mishaps such as perforation during access cavity preparation, file fractures, zipping, canal transportation, ledging, sodium hypochlorite accidents, occur in insertion of posts; during routine endodontic treatment, removing of due to anatomical variances, the tooth’s inaccessibility, and the operator’s inexperience. The root canal system and the periodontium start to communicate in an unfavourable way because of perforations.[6-9]
In multirooted teeth, pulpal floor perforations end up causing the periodontium to become inflamed, which can cause irreparable attachment loss.[1,10] Evidence of prolonged bleeding into the pulp space is the first sign of an iatrogenic perforation.[11] Guttapercha, super-EBA, composite, conventional GIC, decalcified freeze-dried bone, mineral trioxide aggregate, resin modified GIC, etc., are some of the materials used to repair furcation perforation.[12]
MTA flow, Biodentine and pro-root MTA were chosen in this study to seal the furcal perforation because they are more biocompatible, capable of sealing and properly adapt to the dentinal walls than other materials. The powder known as mineral trioxide aggregate is made up of tiny hydrophilic particles that can set when exposed to moisture.[13-15] When applied in touch with cells and tissues, MTA might prove to be a biocompatible substance.[16] MTA that flows is MTA that hasn’t had any resin, calcium hydroxide, or other chemicals added to it.[17] Biodentine is an excellent good material for the repair of perforation.[18] Resorbable and non-resorbable internal matrix are the two varieties that are available.[19] Collagen is a protein fibre with a triple helix shape made of interconnected fibres that gives it a great degree of strength. The final product serves as a physiological barrier by reflecting the functioning periosteum.[20]
According to the study’s findings, group 2 (Biodentine with internal matrix) had the least amount of microleakage, which was followed by group 1 (Biodentine without internal matrix). Groups 1, 3, 4 and 6 also exhibited major differences. In the current investigation, we discovered that Biodentine has great sealing capacity and recommended to use for perforation repair. These results are in accordance with: A study conducted by Krupalini KS, Udayakumar, Jayalakshmi K.B. (2003).[21]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ford TR, Torabinejad M, McKendry DJ, Hong CU, Kariyawasam SP. Use of mineral trioxide aggregate for repair of furcal perforations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;79:756–63. doi: 10.1016/s1079-2104(05)80313-0. [DOI] [PubMed] [Google Scholar]
- 2.Snyder WR, Hoover J, Khoury R, Farach-Carson MC. Effect of agents used in perforation repair on osteoblastic cells. J Endod. 1997;23:158–61. doi: 10.1016/S0099-2399(97)80266-X. [DOI] [PubMed] [Google Scholar]
- 3.Fuss Z, Trope M. Root perforations:Classification and treatment choices based on prognostic factors. Endod Dent Traumatol. 1996;12:255–64. doi: 10.1111/j.1600-9657.1996.tb00524.x. [DOI] [PubMed] [Google Scholar]
- 4.American association of endodontists glossary of endodontic terms. 7th ed. Chicago, IL: American association of endodontics, 2003; [Google Scholar]
- 5.Cauder T, Shin SJ. Repair of perforations with MTA:Clinical applications and mechanisms of action. Endodontic Topics. 2009;15:32–55. [Google Scholar]
- 6.Hülsmann M, Peters OA, Dummer PMH. Mechanical preparation of root canals:Shaping goals, techniques and means. Endodontic topics. 2005;10:30–76. [Google Scholar]
- 7.Valois CRA, Costa ED., Jr Influence of the thickness of mineral trioxide aggregate on sealing ability of root-end fillings in vitro . Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;97:108–11. doi: 10.1016/s1079-2104(03)00359-7. [DOI] [PubMed] [Google Scholar]
- 8.Alghamdi NS, Algarni YA, Ain TS, Alfaifi HM, AlQarni AA, Mashyakhi JQ, et al. Endodontic mishaps during root canal treatment performed by undergraduate dental students:An observational study. Medicine (Baltimore) 2021;100:e27757. doi: 10.1097/MD.0000000000027757. doi:10.1097/MD.0000000000027757. PMID:34964733;PMCID:PMC8615340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Koulaouzidou EA, Papazisis KT, Economides NA, Beltes P, Kortsaris AH. Antiproliferative effect of mineral trioxide aggregate, zinc oxide-eugenol cement and glass-ionomer cement against three fibroblastic cell lines. J Endod. 2005;31:44–6. doi: 10.1097/01.don.0000132302.03725.50. [DOI] [PubMed] [Google Scholar]
- 10.Arens DE, Torabinejad M. Repair of furcal perforations with mineral trioxide aggregate:two case reports. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;82:84–8. doi: 10.1016/s1079-2104(96)80382-9. doi:10.1016/s1079-2104(96)80382-9. PMID:8843459. [DOI] [PubMed] [Google Scholar]
- 11.Alhadainy HA, Abdalla AI. Artificial floor technique used for the repair of furcation perforations:A microleakage study. J Endod. 1998;24:33–5. doi: 10.1016/S0099-2399(98)80209-4. [DOI] [PubMed] [Google Scholar]
- 12.Sarkar NK, Caicedo R, Ritwik P, Moiseyeva R, Kawashima I. Physicochemical basis of the biological properties of mineral trioxide aggregate. J Endod. 2005;31:97–100. doi: 10.1097/01.don.0000133155.04468.41. [DOI] [PubMed] [Google Scholar]
- 13.Fischer EJ, Arens DE, Miller CH. Bacterial leakage of mineral trioxide aggregate as compared with zinc free amalgam, intermediate restorative material, super EBA as a root-end filling material. J Endod. 1998;24:176–9. doi: 10.1016/S0099-2399(98)80178-7. [DOI] [PubMed] [Google Scholar]
- 14.Torabinejad M, Chivian N. Clinical applications of mineral trioxide aggregate. J Endod. 1999;25:197–205. doi: 10.1016/S0099-2399(99)80142-3. [DOI] [PubMed] [Google Scholar]
- 15.Yaltirik M, Ozbas H, Bilgic B, Issever H. Reactions of connective tissue to mineral trioxide aggregate and amalgam. J Endod. 2004;30:95–9. doi: 10.1097/00004770-200402000-00008. [DOI] [PubMed] [Google Scholar]
- 16.Broon NJ, Bramante CM, de Assis GF, Bortoluzzi EA, Bernardineli N, de Moraes IG, et al. Healing of root perforations treated with mineral trioxide aggregate (MTA) and portland cement. J Appl Oral Sci. 2006;14:305–11. doi: 10.1590/S1678-77572006000500002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lin LM, Rosenberg PA, Lin J. Do procedural errors cause endodontic treatment failure? J Am Dent Assoc. 2005;136:187–93. doi: 10.14219/jada.archive.2005.0140. quiz 231. [DOI] [PubMed] [Google Scholar]
- 18.Sharada HL, Briget B. A comparative evaluation of the sealing ability of mineral trioxide aggregate, high copper silver amalgam, conventional glass ionomer cement and glass cermet as root end filling materials by dye penetration method. J Int Oral Health. 2011;3:31–5. [Google Scholar]
- 19.de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzanch M, Abitbol S, et al. Treatment outcome in endodontics:The Toronto study. Phases 3 and 4:Orthograde retreatment. J Endod. 2008;34:131–7. doi: 10.1016/j.joen.2007.11.003. [DOI] [PubMed] [Google Scholar]
- 20.Kvinnsland I, Oswald RJ, Hasle A, Grønningsaeter AG. A clinical roentgenological study of 55 cases of root perforation. Int Endod J. 1989;22:75–84. doi: 10.1111/j.1365-2591.1989.tb00509.x. [DOI] [PubMed] [Google Scholar]
- 21.Al-Daafas A, Al-Nazhan S. Histological evaluation of contaminated furcal perforation in dogs'teeth repaired by MTA with or without internal matrix. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:e92–9. doi: 10.1016/j.tripleo.2006.09.007. [DOI] [PubMed] [Google Scholar]