

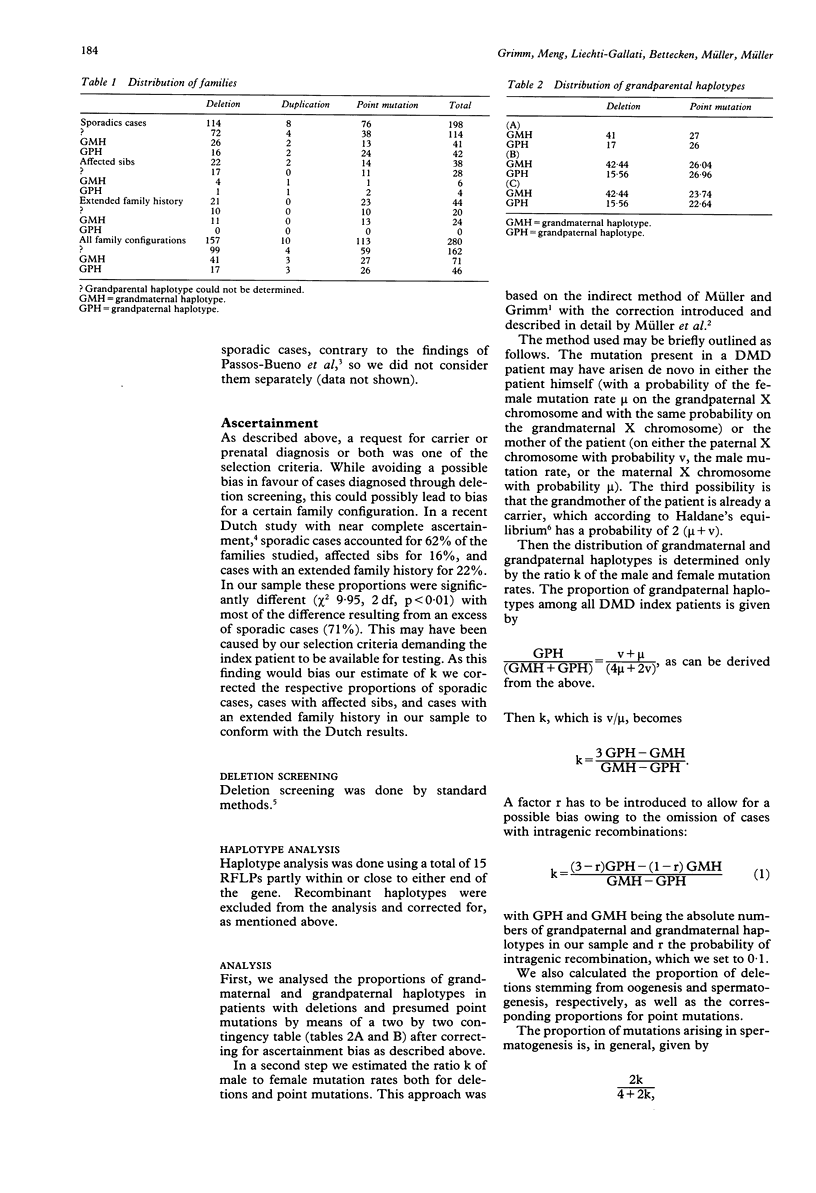
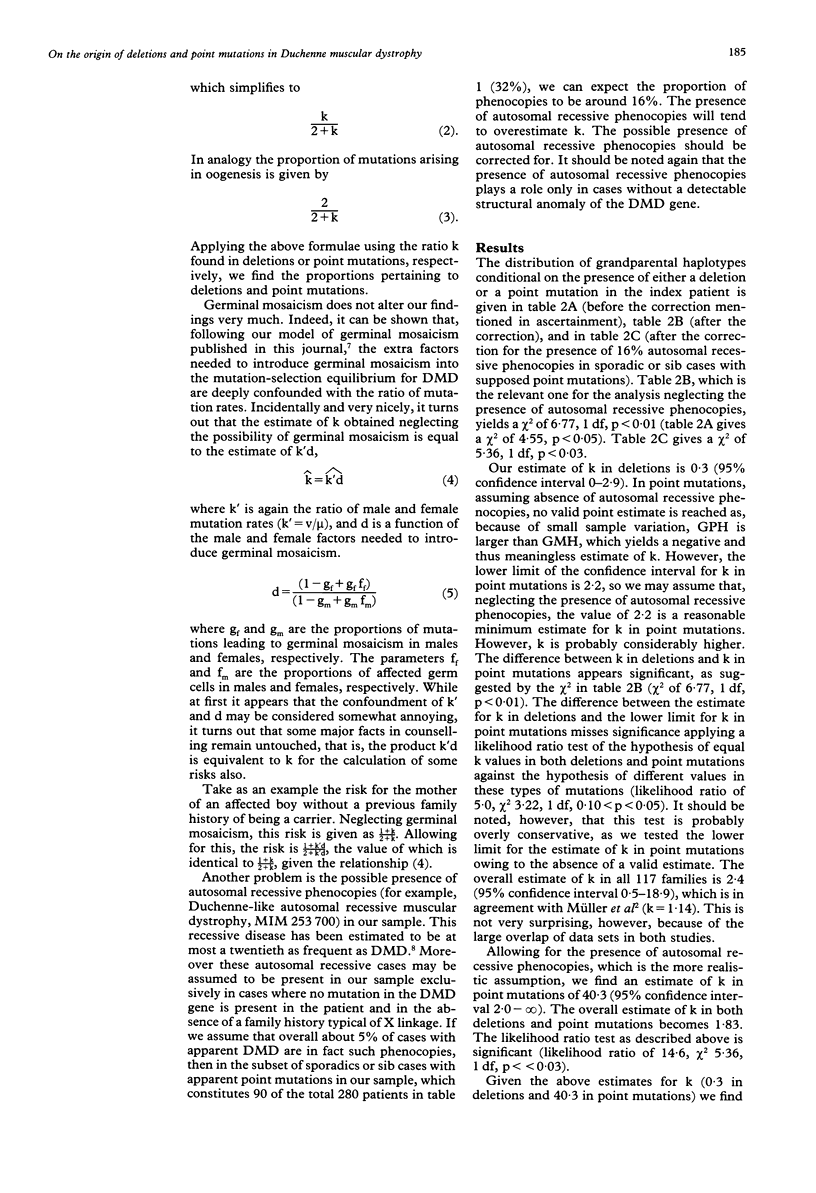
Abstract
We present the results of a study of the rate and origin of mutations in Duchenne muscular dystrophy (DMD). Depending on the type of mutation (deletion/duplication or point mutation) present in the patient, there are widely varying ratios of male to female mutation rates. In deletions, the male mutation rate is only 30% of the female one. In non-deletional/non-duplicational mutations (presumably containing a high proportion of point mutations) the male mutation rate is at least 2.2 as high as the female one and probably much higher. Allowing for the presence of autosomal recessive phenocopies we find that k in non-deletional/non-duplicational mutations is 40.3. These findings mean that the vast majority of deletions arise in oogenesis, while most point mutations stem from spermatogenesis. Previous investigations have shown that in other diseases and genes, most notably haemophilia B and A, but also the ZFY and ZFX genes, the male mutation rate for point mutations tends to be higher than the female one. Our results can be seen as a confirmation of this for the special case of DMD. The influence on risk figures is considerable. As an example, the risk of the mother of an isolated case of DMD without an apparent structural anomaly of the gene of being a carrier increases from 67% to at least 76%. Given the estimate of 40.3 for k, allowing for the presence of autosomal recessive phenocopies mentioned above, it increases even further to 98%. However, as confidence intervals are still large, more data are needed to improve the estimates. Germinal mosaicism in this context is discussed.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bröcker-Vriends A. H., Rosendaal F. R., van Houwelingen J. C., Bakker E., van Ommen G. J., van de Kamp J. J., Briët E. Sex ratio of the mutation frequencies in haemophilia A: coagulation assays and RFLP analysis. J Med Genet. 1991 Oct;28(10):672–680. doi: 10.1136/jmg.28.10.672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Emery A. E. Population frequencies of inherited neuromuscular diseases--a world survey. Neuromuscul Disord. 1991;1(1):19–29. doi: 10.1016/0960-8966(91)90039-u. [DOI] [PubMed] [Google Scholar]
- Grimm T., Müller B., Müller C. R., Janka M. Theoretical considerations on germline mosaicism in Duchenne muscular dystrophy. J Med Genet. 1990 Nov;27(11):683–687. doi: 10.1136/jmg.27.11.683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- HALDANE J. B. Mutation in the sex-linked recessive type of muscular dystrophy; a possible sex difference. Ann Hum Genet. 1956 May;20(4):344–347. doi: 10.1111/j.1469-1809.1955.tb01289.x. [DOI] [PubMed] [Google Scholar]
- Ketterling R. P., Vielhaber E., Bottema C. D., Schaid D. J., Cohen M. P., Sexauer C. L., Sommer S. S. Germ-line origins of mutation in families with hemophilia B: the sex ratio varies with the type of mutation. Am J Hum Genet. 1993 Jan;52(1):152–166. [PMC free article] [PubMed] [Google Scholar]
- Koenig M., Hoffman E. P., Bertelson C. J., Monaco A. P., Feener C., Kunkel L. M. Complete cloning of the Duchenne muscular dystrophy (DMD) cDNA and preliminary genomic organization of the DMD gene in normal and affected individuals. Cell. 1987 Jul 31;50(3):509–517. doi: 10.1016/0092-8674(87)90504-6. [DOI] [PubMed] [Google Scholar]
- Müller B., Dechant C., Meng G., Liechti-Gallati S., Doherty R. A., Hejtmancik J. F., Bakker E., Read A. P., Jeanpierre M., Fischbeck K. H. Estimation of the male and female mutation rates in Duchenne muscular dystrophy (DMD). Hum Genet. 1992 May;89(2):204–206. doi: 10.1007/BF00217124. [DOI] [PubMed] [Google Scholar]
- Müller C. R., Grimm T. Estimation of the male to female ratio of mutation rates from the segregation of X-chromosomal DNA haplotypes in Duchenne muscular dystrophy families. Hum Genet. 1986 Oct;74(2):181–183. doi: 10.1007/BF00282088. [DOI] [PubMed] [Google Scholar]
- Passos-Bueno M. R., Bakker E., Kneppers A. L., Takata R. I., Rapaport D., den Dunnen J. T., Zatz M., van Ommen G. J. Different mosaicism frequencies for proximal and distal Duchenne muscular dystrophy (DMD) mutations indicate difference in etiology and recurrence risk. Am J Hum Genet. 1992 Nov;51(5):1150–1155. [PMC free article] [PubMed] [Google Scholar]
- Shimmin L. C., Chang B. H., Li W. H. Male-driven evolution of DNA sequences. Nature. 1993 Apr 22;362(6422):745–747. doi: 10.1038/362745a0. [DOI] [PubMed] [Google Scholar]
- van Essen A. J., Abbs S., Baiget M., Bakker E., Boileau C., van Broeckhoven C., Bushby K., Clarke A., Claustres M., Covone A. E. Parental origin and germline mosaicism of deletions and duplications of the dystrophin gene: a European study. Hum Genet. 1992 Jan;88(3):249–257. doi: 10.1007/BF00197255. [DOI] [PubMed] [Google Scholar]
- van Essen A. J., Busch H. F., te Meerman G. J., ten Kate L. P. Birth and population prevalence of Duchenne muscular dystrophy in The Netherlands. Hum Genet. 1992 Jan;88(3):258–266. doi: 10.1007/BF00197256. [DOI] [PubMed] [Google Scholar]