

Abstract
To assess resolving-like activity by a novel chemically-modified curcumin (CMC2.24) in a “two-hit” model of diabetes-associated periodontitis. Macrophages from rats were cultured in the presence/absence of either Lipopolysaccharide (LPS, 1st hit); or advanced-glycation-end products (AGE, 2nd hit); or both combined. CMC2.24 was added as treatment. The conditioned media were analyzed for MMP-9, cytokines (IL-1β, IL-6, TNF-α), resolvins (RvD1, RvE1, lipoxin A4), and soluble receptor for AGE (sRAGE). The phenotypes of M1/M2 macrophage were analyzed by flow cytometry. Both LPS/AGE-alone, and two-combined, dramatically increased the secretion of MMP-9 by macrophages. CMC2.24 “normalized” the elevated levels of MMP-9 under all conditions. Moreover, CMC2.24 significantly reduced the secretion of IL-1β and IL-6 with a fewer effects on TNF-α. Importantly, CMC2.24 increased RvD1 and sRAGE secretion by macrophages exposed to LPS/AGE; and both treatment groups exhibited increased M2 relative to M1 populations. Furthermore, scatter-diagram showed the macrophages gradually shifted from M1 towards M2 with CMC2.24-treated, whereas LPS/AGE-alone groups remained unchanged. CMC2.24 “normalized” cytokines and MMP-9, but also enhanced RvD1 and sRAGE in macrophages. Crucially, CMC2.24 appears to be a potent inhibitor of the pro-inflammatory M1 phenotype; and a promotor of the pro-resolving M2 phenotype, thus acting like a crucial “switch” to reduce inflammation.
Subject terms: Dental diseases, Pharmaceutics, Inflammation, Diabetes
Introduction
The connection between diabetes and periodontitis has received constant attention in recent years. Both involve a broad range of inflammatory/collagenolytic cascades. Diabetes is known to promote unusually severe periodontitis when not optimally controlled1, 2, whereas periodontitis has an exuberant “host-response” in the periodontium to generate numerous inflammatory mediators and proteinases. They not only break the collagen-rich deeper periodontal tissues, thus leading to tooth loss; but also cause insulin resistance3, 4. How can disease, in one part of the body transmit signals to the system, or vice versa, affecting each other?
Recently, a “two-hit model” was proposed by Golub et al.5, to demonstrate a bi-directional manner between diabetes and periodontitis. The “1st hit” is caused by microbial biofilm (dental plaque), which acts as a reservoir of periodontal pathogens. The binding of lipopolysaccharide (LPS) or endotoxin from the pathogens to toll-like receptor 2/4 in macrophages (Mφs) or polymorphonuclear leukocytes (PMNs) triggers an inflammatory response. This response leads to the production of excessive pro-inflammatory mediators and proteinases in the periodontium6, which include cytokines [e.g., interleukin-1 beta and 6 (IL-1β, IL-6), tumor necrosis factor-alpha (TNF-α)]; and matrix metalloproteinases (i.e., MMP-2 and 9)7. They contribute to the destruction of both soft and hard periodontal tissues. Additionally, these mediators can be carried through circulation to the liver, resulting in the release of additional inflammatory mediators systemically. These systemic mediators, including C-reactive protein, IL-6, prostaglandin E2, as well as other MMPs, affect overall systemic conditions and might also exacerbate periodontal breakdown. Moreover, diabetes acts as the “2nd hit” during this interaction5. If uncontrolled hyperglycemia exists, advanced-glycation-end products (AGE) are formed to react with their cellular receptors for AGE (RAGE) on the surfaces of macrophages or other inflammatory cells. It leads to adverse events including elevated oxidative stress (i.e., reactive oxygen species); and osmotic stress (causing raised production of proinflammatory cytokines and MMPs). Eventually, these events amplify the inflammatory cascades and exacerbate periodontitis through the circulation as well8, 9. However, the soluble receptor for AGE (sRAGE) counteracts the adverse effects of AGE-RAGE interaction by competing with RAGE for binding with AGE. Low levels of sRAGE have been proposed as early predictors of Type II diabetes10.
At the cellular level, Mφs exhibit extreme heterogeneity both in normal and pathological conditions due to a major feature of “plasticity.” In this regard, Mφs are generally categorized into two broad subsets as either classically activated M1 (pro-inflammatory) or alternatively activated M2 (anti-inflammatory/pro-resolving) phenotypes, indicating their dual role as “killers” (M1) and/or “builders” (M2)11, 12. During chronic inflammation (diabetes and/or periodontitis), relevant cellular and molecular mechanisms drive Mφs in these pathological conditions to become M1 pro-inflammatory phenotypes11–13. In contrast, processes that promote the conversion of M1 to the M2 phenotypes help resolve inflammation, inducing tissue regeneration rather than tissue destruction14.
The emergence of host modulation therapy (HMT), as a targeted treatment strategy, accelerates the development of novel drugs15. Interestingly, recent studies3, 4, 16 indicated that treating diabetic people with an MMP inhibitor, doxycycline, resulted in decreased inflammation and increased insulin sensitivity as well as improved glucose control3. Other examples of pleiotropic MMP-inhibitor drugs, notably the non-antimicrobial formulations of tetracycline compounds can reduce the severity of several systemic diseases (e.g., rheumatoid arthritis, post-menopausal osteoporosis), as well as periodontitis, in humans17–21.
HMT, in part, is to restore the balance between (a) pro-inflammatory mediators and anti-inflammatory mediators; and, (b) destructive enzymes and enzyme inhibitors15. Regarding resolvins and lipoxins, both are pro-resolving lipid mediators derived from omega-3 (or n-3) polyunsaturated fatty acids22. As one category of HMT agents, major resolvins (RvD1 and RvE1) and Lipoxin A4 (LxA4) have a fundamental role in resolving inflammation23–25. In contrast to anti-inflammatory drugs (e.g., nonsteroidal anti-inflammatory drugs and corticosteroids), resolvins and lipoxins do not suppress acute inflammation, which is necessary to combat infectious agents, but prevents this acute inflammatory response from being prolonged which, would be tissue-damaging26.
To date, the only HMT agent for treating patients with periodontitis that has been governmentally approved is Periostat® (doxycycline hyclate) developed by our group27. And recently, we further developed a novel chemically-modified curcumin 2.24 (CMC2.24) (a triketonic phenylaminocarbonyl curcumin). As one of the most effective and newer HMT agents, CMC2.24 is a “lead” compound. It was found to be safer and most effective based on in vitro, cell and tissue culture, and in vivo studies on rat and dog models of experimental periodontitis and diabetes28–36. In this current study, we describe the additional mechanisms which were not previously identified. The objective is to expand on and discover additional host modulatory activities of this pleiotropic CMC2.24, using a “two-hit” Mφ cell-culture model of diabetes-associated periodontitis. We hope that CMC2.24 can be a beneficial and novel therapeutic HMT agent in the management of chronic inflammatory diseases, including diabetes and periodontitis.
Material and methods
Animals (source of monocytes/macrophages) and ethical approval
Sprague–Dawley (SD) rats (Body Weight/Age: 301–325 g/66–71 days) were purchased from Charles River (Stone Ridge, NY, USA). All rats were housed in the Division of Laboratory Animal Resources (DLAR) at Stony Brook University, with care provided by the center’s personnel. All procedures were conducted at the same location. DLAR is an AAALAC International accredited facility; and follows the Animal Welfare Act (USDA enforced), the Public Health Service Act (OLAW enforced), and NY State law (DOH enforced). Protocols for animal studies were approved by Stony Brook University’s Institutional Animal Care and Use Committee (IACUC# 230,617–23). Sixteen male adult SD rats were used to collect peritoneal and blood-derived Mφs. All experiment methods were carried out in accordance with relevant guidelines and complied with ARRIVE 2.0 guidelines37.
Chemical reagents
CMC 2.24 was synthesized and provided by Chem-Master Intl. Inc. (99.5% pure, Stony Brook, NY, USA). All cell culture reagents and other chemical reagents were purchased from Thermo Fisher Scientific (Waltham, MA, USA).
Cell culture studies
Peritoneal Mφs
Mφs were obtained from peritoneal washes (PW) of 8 SD rats. Briefly, 15 mL of cold sterile PBS (pH7.4) containing 3 mM of ethylenediaminetetraacetic acid (EDTA) intraperitoneally (i.p.) was injected into the peritoneal cavity, and the peritoneum was gently massaged for 1 min. Approximately 12 mL/per rat of PW was collected and stored on ice (4 °C). These lavages were centrifuged (1000 rpm, 4 °C, 5 min) to separate supernatant cell-free peritoneal fractions (CFPFs) and resident mixed cells that were re-suspended in 25 mL/each sample of PBS/3 mM EDTA. The cell suspension was layered onto Lymphoprep™ (Accurate Chemical & Scientific Corporation, Westbury, NY, USA) at a ratio of 2 to 1–1.5 (v/v) and centrifuged at 1,800 rpm for 30 min at 25 °C. The resident peritoneal Mφs were isolated and purified from the mixed cells by density gradient centrifugation and adherence as described previously38. The peritoneal Mφs were cultured in macrophage serum-free media (SFM) (Thermo Fisher Scientific Inc., Boston, MA, USA) in 24-well plates. Each well contained 106 cells/mL, supplemented with 100 units/mL penicillin, and 100 μg/mL streptomycin, in a humidified atmosphere of 5% CO2 and 95% air at 37 °C.
The Mφs were distributed into 10 groups (triplicates/group) to mimic the “two-hit” model. The “1st hit” involved the absence (Normal control, N) or presence of P.g. LPS (L) at a final concentration of 100 ng/mL; the “2nd hit” involved the absence (N) or presence of AGE (A) at a final concentration of 100 µg/mL; or the “two hits” combined (L + A). CMC2.24 was added to the cultures at final concentrations of 2 or 5 μM [L + 2.24 (2 or 5); A + 2.24 (2 or 5); L + A + 2.24 (2 or 5)]. (Fig. 1a). P.g. LPS was purchased from Invitrogen (San Diego, CA, USA). AGE-BSA-II (glycated Bovine Serum Albumin) was purchased from BioVision, Inc. (Milpitas, CA, USA).
Figure 1.

The study design of a “two-hit” cell-culture model of diabetes-associated periodontitis. (a) Resident peritoneal and blood-derived Mφs were harvested from the rat, and separated by density gradient centrifugation, respectively. In an ex-vivo cell culture, Mφs were incubated in the absence (normal control), or presence of either LPS (L, the “1st hit”); or AGE (A, “2nd hit”); or both combined (L + A). CMC2.24 was added to the cultures at 2 or 5 μM. MMP-9 activity was measured by gelatin zymography and scanned densitometrically. Effects of CMC2.24 on MMP-9 in the peritoneal Mφs challenged by LPS-alone (b,c), AGE-alone (d,e), or the “two-hit” (f,g). N, the normal group without any challenge or treatment. L, the LPS-alone challenged group. L + 2.24 (2 or 5), the low (2 μM) and high (5 μM) concentrations of CMC2.24-treated groups. A, the AGE-alone challenged group. A + 2.24 (2 or 5), the low (2 μM) and high (5 μM) concentrations of CMC2.24-treated groups. L + A, the “two-hit” challenged group. L + A + 2.24 (2 or 5), the low (2 μM) and high (5 μM) concentrations of CMC2.24-treated groups. Each value represents the mean (n = 3/group) ± the standard error. *p < 0.05, **p < 0.005, values were compared between N and L/A/(L + A)-challenged groups at 18-h. #p < 0.05, ##p < 0.005, values were compared between L/A/(L + A)-challenged and L/A/(L + A) + 2.24 (2 or 5)-treated groups at 18-h. The grouping of gels were cropped from different parts of the same gel. The full-length gels were included in the Supplementary Information files (S1-4.)
After 18-h incubation, the conditioned media were collected and analyzed for pro- (92 kDa) and active- (82 kDa) MMP-9 by gelatin zymography, and for cytokines (IL-1β, IL-6, and TNF-α), sRAGE, and resolvins (RvD1, RvE1, and LxA4), all by enzyme-linked immunosorbent assay (ELISA).
Blood-derived Mφs
Resident blood-derived Mφs were isolated from the heart of 8 SD rats by cardiac puncture. In brief, 10–15 mL of whole blood from each rat was drawn, then transferred to the heparin-coated tubes (anti-clotting). Mφs isolation was achieved by the same procedure as described above (Fig. 1a), then cultured in the Teflon Beakers (Savillex, MN, USA) to prevent cell attachment (no adherence)39, 40. At time 0, Mφs were isolated and distributed into 6 groups (triplicates/group) to mimic the “two-hit” model of diabetes-associated periodontitis: in the absence (N), or presence of either LPS (L) or AGE (A). CMC2.24 was added to the cultures of different groups at a final concentration of 5 μM (N + 2.24, L + 2.24, and A + 2.24), then harvested at 0, 6, and 18 h for flow cytometry analysis.
Flow cytometry
At 0, 6, and 18 h, Mφs were harvested and immediately labeled by fluorescence-conjugated antibodies against different cell surface markers to identify M0, M1, and M2 phenotypes. The CD11b/c+ (1:100 dilution, BioLegend Inc., San Diego, CA, USA) was used as a pan-macrophage marker to gate the total populations of macrophage, including M0 phenotype and the nonpolarized resting Mφs41–44. The CD38+ (1:100 dilution, BioLegend Inc., San Diego, CA, USA) was used for labeling M1 phenotype (CD11b/c+ CD38+)44, 45; and the CD163+ (1:200 dilution, BioRad Laboratories Inc., Hercules, CA, USA) was used for labeling M2 phenotype (CD11b/c+ CD163+)46–48. Flow cytometry analysis was using FACSCalibur™ (BD Biosciences, San Jose, CA, USA). The M2/M1 ratio was calculated by using the percentage of gating for the M2 phenotype divided by the M1 phenotype at 0, 6, and 18 h, respectively49.
Gelatin zymography for MMP-9 analysis
After 18-h incubation, the conditioned media from cultured peritoneal Mφ were collected and analyzed for pro- (92 kDa) and active- (82 kDa) MMP-9 by gelatin zymography as described previously32, 33, 50, 51. The clear zones of lysis against a background indicated gelatinolytic activity and were scanned densitometrically with Invitrogen™ iBright™ FL1000 Imaging Systems (Thermo Fisher Scientific, Inc., Boston, MA, USA). Results were analyzed by Image J to quantitatively assess gelatinase activity31. MMP-9 standard was purchased from R&D Systems, Inc. (Minneapolis, MN, USA).
ELISA
Quantikine® ELISA kits for IL-1β (RLB00, SRLB00, PRLB00), IL-6 (R6000B, SR6000B, PR6000B), and TNF-α (RTA00, SRTA00, PRTA00) were purchased from R&D Systems, Inc. (Minneapolis, MN, USA). RvD1 (Cat# 500,380) was purchased from Cayman Chemical. (Ann Arbor, Michigan, USA). RvE1 (Cat# MBS2604861) and soluble receptor of AGE (sRAGE) (Cat# MBS722302) were purchased from MyBioSource, Inc. (San Diego, CA, USA), and LxA4 (Cat# 407,010) was purchased from Neogen Corporation (Lexington, Kentucky, USA). All measurements were performed according to the kit manufacturer’s instructions.
Statistical analysis
SPSS21.0 (Statistical Package for Social Sciences, IBM) was used to analyze the data. The levels of MMP-9, pro-inflammatory cytokines, resolvins, sRAGE, and the percentage of different Mφ populations were determined using analysis of variance (ANOVA), and also using Student’s t-test (two investigators carried out the data analysis, separately), with p < 0.05 taken as statistically significant. Each value represented the mean (n = 3/group) ± the standard error of the mean (S.E.M.). All experiments were independently performed at least three times.
Results
Effects of CMC2.24 on MMP-9
Gelatin zymography analysis showed that both LPS (the “1st hit”) and AGE-alone (the “2nd hit”) challenged groups significantly increased total-MMP-9 levels by 20.9% and 20.1% (p < 0.05; p < 0.05), compared to the N group (Fig. 1b–e). which reflected both elevated pro- and active-forms of this MMP (Fig. 1b,d). A trend towards reduction in the total-MMP-9 levels towards normal was seen in both low (2 μM) and high (5 μM) concentrations of CMC2.24-treated groups, although both concentrations of CMC2.24 treatment were not statistically significant (p > 0.05) compared to the L-alone (Fig. 1c). Importantly, the total-MMP-9 levels in these CMC2.24-treated groups were not different from those in the N group (p > 0.05), indicating the “normalizing effect” of CMC2.24. In addition, treatment with 2 and 5 µM of CMC2.24 did significantly reduce the total-MMP-9 levels by 65.1% and 74.4% (p < 0.05; p < 0.005), respectively, compared to the A-alone (Fig. 1e). Also, there appeared to be a dose–response effect in the CMC2.24-treated groups since the higher concentration (5 µM) of CMC2.24 produced a greater reduction in the total-MMP-9 levels (Fig. 1e).
When the two-hit system (L + A) was used, it dramatically increased the total-MMP-9 levels by 42.1% (p < 0.005) compared to the N group (Fig. 1f–g). It appeared to reflect elevated pro- and active-forms of this MMP as well (Fig. 1f). Treatment with 2 and 5 µM of CMC2.24 largely reduced total-MMP-9 levels by 67.2% and 63.1% (p < 0.005; p < 0.05), respectively, compared to the L + A group (Fig. 1g).
Effects of CMC2.24 on pro-inflammatory cytokines
As shown in Fig. 2a, IL-1β concentrations were significantly increased in both L and A-alone (p < 0.001; p < 0.005) challenged groups, and with a synergistic and significant increase in the L + A challenged group (p < 0.05), respectively, compared to the N group. IL-1β concentrations in the L + A group were also significantly greater than each “hit” (L or A) alone (p < 0.05; p < 0.05). When the L-alone was treated with 2 and 5 µM of CMC2.24, the higher concentration (5 µM) of CMC2.24 produced a significant reduction in IL-1β concentrations (p < 0.05), as well as a trend of reduction at the lower concentration (2 µM) of CMC2.24 (p > 0.05). In addition, when the A-alone was treated with 2 and 5 µM of CMC2.24, both concentrations of CMC2.24 treatment significantly reduced IL-1β concentrations (p < 0.05; p < 0.05) in an apparent dose–response manner. Impressively, when the “two-hit” (L + A) group was treated with 2 and 5 µM of CMC2.24, both concentrations of CMC2.24 significantly decreased IL-1β concentrations (p < 0.05; p < 0.05) and brought them back to normal levels in a similar dose–response relationship (Fig. 2a).
Figure 2.

Effects of CMC2.24 on pro-inflammatory cytokines. The effects of CMC2.24 on the concentrations (pg/mL) of IL-1β (a), IL-6 (b) and TNF-α (c) in rat peritoneal Mφs challenged by LPS-alone, AGE-alone, or the “two-hit”, respectively; and treated with different concentrations (2 or 5 μM) of CMC2.24 at 18-h. N, the normal group without any challenge or treatment. L, the LPS-alone challenged group. L + 2.24 (2 or 5), the low (2 μM) and high (5 μM) concentrations of CMC2.24-treated groups. A, the AGE-alone challenged group. A + 2.24 (2 or 5), the low (2 μM) and high (5 μM) concentrations of CMC2.24-treated groups. L + A, the “two-hit” challenged group. L + A + 2.24 (2 or 5), the low (2 μM) and high (5 μM) concentrations of CMC2.24-treated groups. Each value represents the mean (n = 3/group) ± the standard error. *p < 0.05, **p < 0.005, ***p < 0.001, values were compared between N and L/A/(L + A)-challenged at 18-h. #p < 0.05, values were compared between L/A/(L + A)-challenged and L/A/(L + A) + 2.24 (2 or 5)-treated groups at 18-h.
In addition, IL-6 concentrations were significantly increased in both L and A-alone (p < 0.05; p < 0.005) groups, also with a similar synergistic and significant increase in the L + A challenged group (p < 0.05), respectively, compared to the N group (Fig. 2b). IL-6 concentrations in the “two-hit” (L + A) group were significantly greater than each “hit”-alone (both p < 0.05). Moreover, the CMC2.24-treated group (5 µM) significantly reduced IL-6 concentrations (p < 0.05), compared to the L-alone. When the A-alone was treated with 2 and 5 µM of CMC2.24, both concentrations significantly reduced IL-6 concentrations (both p < 0.05) compared to the A-alone. Furthermore, when the L + A group was treated with 2 and 5 µM of CMC2.24, both concentrations significantly decreased IL-6 concentrations (both p < 0.05), again, in the apparent dose–response fashion, and brought them back to normal levels.
Next, we examined TNF-α concentrations in the same culture media. As shown in Fig. 2c, TNF-α levels were significantly increased in all three challenged groups: L and A-alone, as well as the L + A groups (all p < 0.001), respectively, compared to the N group. However, the combination of “two-hit” did not increase TNF-α concentrations over the already (apparently) maximum increase in this cytokine produced by each “hit” separately. Impressively, when the L-alone was treated with 2 and 5 µM of CMC2.24, both concentrations significantly reduced TNF-α concentrations (both p < 0.05) in a dose–response manner. However, when the A-alone was treated with 2 and 5 µM of CMC2.24, only the higher concentration (5 µM) of CMC2.24 appeared to produce a more significant reduction in TNF-α concentrations (p < 0.05), although a trend of reduction was seen in the lower concentration (2 µM) of CMC2.24-treated group (p > 0.05). Finally, when the L + A group was treated with 2 and 5 µM of CMC2.24, a lesser effect on the “two-hit” group was observed (p > 0.05), even though there was still a trend of reduction in TNF-α concentrations.
Effects of CMC2.24 on resolvins
Regarding RvD1, as shown in Fig. 3a, the concentrations of this resolvin were significantly reduced to undetectable levels both in the L and A-alone groups (both p < 0.001), respectively, compared to the N group. When the L-alone was treated with 2 and 5 µM of CMC2.24, both concentrations significantly increased RvD1 concentrations (both p < 0.001) in a dose–response manner, compared to the L-alone. It should also be noted that the higher concentration (5 µM) of CMC2.24 treatment, but not the lower concentration (2 µM) tremendously increased RvD1 concentrations by eightfold above the L-alone challenged group and by 6-folds above normal (N) levels. Similarly, when the A-alone was treated with 2 and 5 µM of CMC2.24, the higher concentration (5 µM) of CMC2.24 significantly increased this resolvin by sixfold above the A-alone and 4-folds above N levels (both p < 0.05). However, these effects were less prominent in the “two-hit” group.
Figure 3.
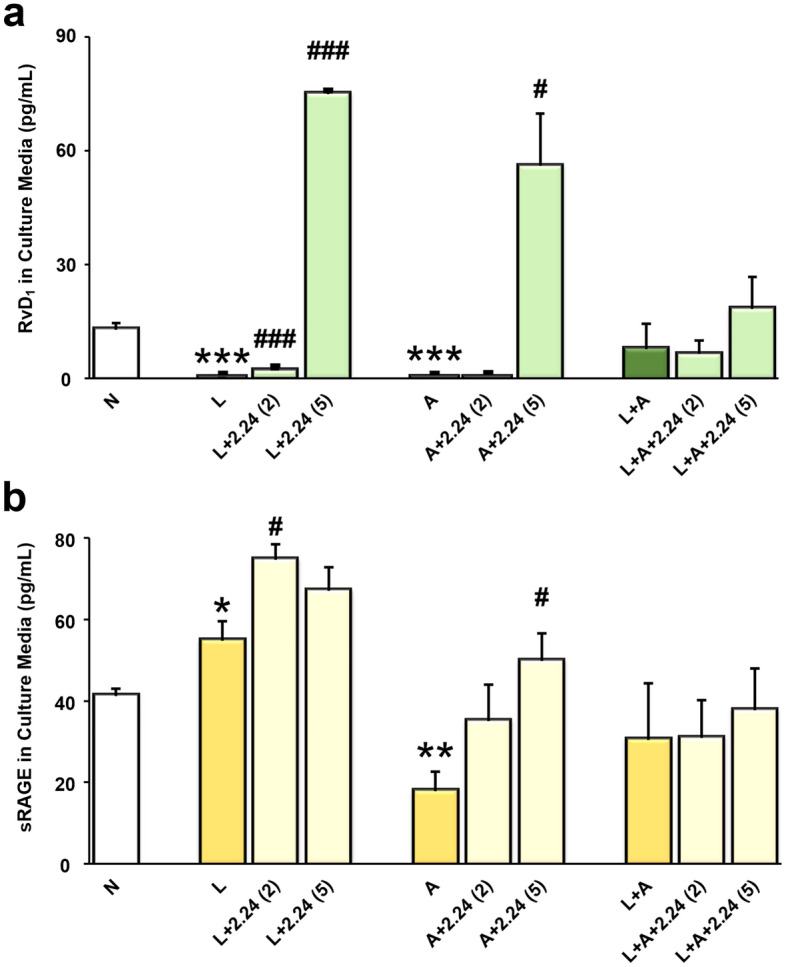
Effects of CMC2.24 on Resolvin D1 and soluble RAGE. The effects of CMC2.24 on the concentrations (pg/mL) of RvD1 (a) and sRAGE (b) in rat peritoneal Mφs challenged by LPS-alone, AGE-alone, or the “two-hit”, respectively; and treated with different concentrations (2 or 5 μM) of CMC2.24 at 18-h. N, the normal group. L, the LPS-alone challenged group. L + 2.24 (2 or 5), the low (2 μM) and high (5 μM) concentrations of CMC2.24-treated groups. A, the AGE-alone challenged group. A + 2.24 (2 or 5), the low (2 μM) and high (5 μM) concentrations of CMC2.24-treated groups. L + A, the “two-hit” challenged group. L + A + 2.24 (2 or 5), the low (2 μM) and high (5 μM) concentrations of CMC2.24-treated groups. Each value represents the mean (n = 3/group) ± the standard error. *p < 0.05, **p < 0.005, ***p < 0.001, values were compared between N and L/A/(L + A)-challenged at 18-h. #p < 0.05, ###p < 0.001, values were compared between L/A/(L + A)-challenged and L/A/(L + A) + 2.24 (2 or 5)-treated groups at 18-h.
Concentrations of RvE1 were not statistically different among the normal, the challenged groups (L-, A-alone, and L + A), and the CMC2.24-treated groups. In addition, concentrations of LxA4 were undetectable in the rat peritoneal Mφs culture media (data not shown).
Effects of CMC2.24 on sRAGE
Although LPS-challenge did not reduce the levels of sRAGE, the 2 µM of CMC2.24-treated group significantly raised the levels of sRAGE (p < 0.05); and a trend towards increase of the levels of this molecule was seen in the 5 µM of CMC2.24-treated group as well, both compared to the L-alone (Fig. 3b). Besides, the concentrations of sRAGE were dramatically reduced in the A-alone challenged group (p < 0.005) compared to the N group. Both concentrations of CMC2.24-treated groups increased the sRAGE concentrations. But the higher concentration (5 µM) of CMC2.24 seemed to be more potent than the lower one (2 µM), to bring the levels of sRAGE back to normal (p < 0.05), compared to the A-alone. In addition, the L + A group had a trend toward reduction in sRAGE levels, compared to the N group. However, there were fewer effects of CMC2.24 on sRAGE levels in the “two-hit” group (p > 0.05).
Conversion of Mφs from M1 to M2 phenotype
LPS-challenged Mφs
At 0, 6, and 18 h, the ratio of M2/M1 was indicated in Fig. 4a. With 6 to 18-h treatment of CMC2.24, this ratio was dramatically increased in the L + 2.24 group, and was significantly higher than the L-alone group (p < 0.005). Interestingly, the ratio of M2/M1 in N + 2.24 was also higher at these time points compared to the untreated (N and L-alone) groups. Thus, treatment with CMC2.24 appeared to “prime” the normal monocyte/macrophage to develop to the M2 phenotype. In the absence of CMC2.24, the ratio of M2/M1 in the L-alone and N groups was maintained at low levels at each time point (Fig. 4a). Consistent with the ratio change of M2/M1, the percentage of M1 population was dramatically decreased in the L + 2.24 group at 18 h, compared to the L-alone (p < 0.005) (Fig. 4b). However, the percentage of M2 population was significantly increased in the CMC2.24-treated group at 6 h, compared to the L-alone (p < 0.005) (Fig. 4c).
Figure 4.

Conversion of LPS-challenged Mφs from M1 to M2 phenotype. At 0, 6, and 18 h, the effects of CMC2.24 on the ratio of M2 to M1 phenotype of L-challenged Mφs were indicated in (a) and analyzed by flow cytometry. The effects of CMC2.24 on each phenotype of L-challenged Mφs were indicated in (b) (for the percentage of M1), and (c) (for the percentage of M2), respectively. N, the normal group (grey line). N + 2.24, the CMC2.24 treated N group (black line). L, the LPS-alone challenged group (red line). L + 2.24, the CMC2.24-treated L group (green line). (d) Scatter diagrams of flow cytometry analysis showed the effects of CMC2.24 on the phenotype conversion of L-challenged Mφs, the “shift” from M1 to M2 phenotype after CMC2.24 treatment. Scatter diagrams of four groups (N, N + 2.24, L, L + 2.24) were present together at 0 h, 6 h, and 18 h. Each scatter diagram has 4 quadrants, UL: CD38+CD163− (M1-only); UR: CD38+CD163+ (M1 and M2 mixed); LL: CD38−CD163− (M0); LR: CD38−CD163+ (M2-only). Each value represents the mean (n = 3/group) ± the standard error. *p < 0.05, **p < 0.005, values were compared between L-challenged and L + 2.24-treated groups at 0, 6, and 18 h.
These observations were further confirmed by the scatter diagrams of flow cytometry analysis (Fig. 4d). In the L + 2.24 group, we observed a population of Mφs that was gradually “shifting” from M1 towards M2 phenotype during the time. This “shifting” population was indicated in the CMC2.24-treated Mφs (L + 2.24; N + 2.24). However, the population of Mφs remained unchangeable in the N and L-alone groups.
AGE-challenged Mφs
A similar trend was observed in the AGE-challenged group (Fig. 5a). At 0, 6, and 18 h, the ratio of M2/M1 in the A + 2.24-treated group was markedly increased after 6 to 18-h treatment with CMC2.24 (p < 0.05), and was significantly higher than the A-alone group (p < 0.005). Consistent with the previous observation, the ratio of M2/M1 in N + 2.24 was also higher at these time points, compared to the untreated (N and A-alone) groups. Again, treatment with CMC2.24 “primed” the normal monocyte/macrophage to convert to the M2 phenotype under these conditions. However, in the absence of CMC2.24, the ratio of M2/M1 in the A-alone and N groups was maintained at low levels at each time point (Fig. 5a). This can be indicated in Fig. 5b,c, respectively. The M1 population appeared to be slightly decreased in the A + 2.24 group at 18 h, compared to the A-alone (p < 0.05) (Fig. 5b). However, the M2 population was significantly increased in the A + 2.24 group at 6 and 18 h, compared to the A-alone (p < 0.05; p < 0.005) (Fig. 5c).
Figure 5.

Conversion of AGE-challenged Mφs from M1 to M2 phenotype. At 0, 6, and 18 h, the effects of CMC2.24 on the ratio of M2 to M1 phenotype of A-challenged Mφs were indicated in (a) and analyzed by flow cytometry. The effects of CMC2.24 on each phenotype of A-challenged Mφs were indicated in (b) (for the percentage of M1), and (c) (for the percentage of M2), respectively. N, the normal group (grey line). N + 2.24, the CMC2.24 treated N group (black line). A, the AGE-alone challenged group (red line). A + 2.24, the CMC2.24-treated A group (green line). (d) Scatter diagrams of flow cytometry analysis showed the effects of CMC2.24 on the phenotype conversion of A-challenged Mφs, the “shift” from M1 to M2 phenotype after CMC2.24 treatment. Scatter diagrams of four groups (N, N + 2.24, A, A + 2.24) were present together at 0 h, 6 h, and 18 h. Each scatter diagram has 4 quadrants, UL: CD38+CD163− (M1-only); UR: CD38+CD163+ (M1 and M2 mixed); LL: CD38−CD163− (M0); LR: CD38−CD163+ (M2-only). Each value represents the mean (n = 3/group) ± the standard error. *p < 0.05, **p < 0.005, values were compared between A-challenged and A + 2.24-treated groups at 0, 6, and 18 h.
Again, these observations were further confirmed by the scatter diagrams of flow cytometry analysis (Fig. 5d). A population of Mφs was gradually “shifting” from M1 towards M2 phenotype in the A + 2.24 group during the time. This “shifting” population was indicated in the CMC2.24-treated Mφs (A + 2.24; N + 2.24). However, the population of Mφs remained unchangeable in the N and A-alone groups.
Discussion
In this study, we demonstrated the current view on the pathogenesis of diabetes-associated periodontitis, which includes a series of dysregulated host inflammatory/collagenolytic responses. HMT is a novel therapeutic strategy to resolve uncontrolled and unresolved inflammation, which could be an adjunct to conventional treatment of diabetes-associated periodontitis.
A NON-antimicrobial formulation of doxycycline (NAD), as the first generation of HMT agents developed by our group, has been and still is the only governmentally-approved agent for clinically treating periodontitis in humans52. A second generation of HMT agents, namely chemically-modified tetracyclines (CMTs, especially CMT-3), has also shown evidence of safety and efficacy in cell and tissue culture, in vivo (rat models), and in clinical studies51–54. Many recent studies indicate that curcumin can modulate macrophage polarization through its anti-inflammatory effects55, 56. As the latest generation of HMT agents, CMC2.24 is a phenylaminocarbonyl curcumin which has a triketonic structure at its C-4 position, resulting in higher bioactivity, better solubility, and greater zinc-binding capability than natural curcumin, as well as no evidence of toxicity even at high doses36, 57, 58. The novelty of CMC2.24 has also been tested in different models and conditions as we described previously28–30, 32–34. For example, we examined the signaling and transcriptional factors in two in vivo models of diseases (diabetes and periodontitis)28, 29, 31, 32. The results demonstrated that CMC2.24 significantly reduced TLR-2 and p38 MAPK expressions involved in the inflammatory signaling cascade in a dog model of natural periodontitis; and inhibited NF-κB activation and inflammatory bone loss in murine models of LPS-induced experimental periodontitis and diabetes-associated natural periodontitis.
More importantly, our group also has compared the effects of the oral administration of natural curcumin and a chemically-modified curcumin (CMC2.24) on osteoclast-mediated bone resorption, apoptosis, and inflammation in a rat model of experimental periodontitis59. We found that CMC2.24 and curcumin inhibit inflammation by different mechanisms, CMC2.24 was capable of reducing alveolar bone resorption in the LPS-induced model of periodontitis. In addition, we did an in vitro study regarding the inhibitory concentration at 50% (IC50) of CMC2.24 and natural curcumin. It demonstrated that CMC2.24 exhibited inhibitory IC50 values in vitro, ranging from 2–8 μM against two collagenases (MMP-8 and MMP-13), two gelatinases (MMP-2 and MMP-9), MMP-3, MMP-7 and MMP-12, which were much lower than curcumin, ranging from 3 to 52 μM57. Therefore, CMC2.24 exhibited stronger potency and efficacy than natural curcumin on MMPs inhibition.
For these reasons, currently, we focused on the multiple mechanisms of efficacy of CMC2.24. This ex-vivo study provided insights that CMC2.24 can restore the balance between the pro-inflammatory and the anti-inflammatory/pro-resolving responses, (a) by decreasing the production of pro-inflammatory mediators (IL-1β, IL-6, and TNF-α), as well as the collagenolytic MMP (MMP-9); and (b), by also dramatically increasing RvD1 levels, as well as sRAGE levels. Many studies showed that the cytokines, like IL-1β, TNF-α, and IL-6 were involved in MMPs upregulation60, and connective tissue breakdown, including bone resorption17. Therefore, our results indicate that CMC2.24 is a potent regulator with additional mechanisms to resolve inflammation and restore homeostasis. The pleiotropic mechanisms of this novel compound on resolving inflammation have been summarized in Fig. 6.
Figure 6.

A scheme to summarize the pleiotropic mechanisms of the novel chemically-modified curcumin 2.24 on resolving inflammation in a “two-hit” model. This “two-hit” model demonstrates a bi-directional manner between diabetes (or other systemic diseases) and periodontitis. Treatment with CMC2.24 can inhibit inflammatory and tissue-destructive mediators including cytokines and MMPs; upregulate resolvin-enhancing (RvD1) activity; and promote the expression of sRAGE; as well as contribute to macrophage polarization from the M1 towards M2 phenotype.
RvD1 is a well-characterized D-series resolvin that is generated in situ from DHA by two sequential lipoxygenation steps61. Many researchers have found that RvD1 is important in (a) ameliorating LPS-induced inflammatory diseases62; (b) improving insulin sensitivity by resolving the chronic inflammation that is associated with diabetes and obesity63; and importantly, (c) activating the anti-inflammatory response, partially by the conversion of Mφs from classically-activated (M1 phenotype) to alternatively activated (M2 phenotype) cells14. This “shift” accelerates the resolution of persistent inflammation at the cellular level. And our study identified that RvD1, not the other resolvins or lipoxins such as RvE1 and LxA4, is the main target for the resolvin-like activity of CMC2.24. This did provide the additional mechanisms that help explain its potent efficacy in the resolution of tissue-destructive effects of chronic inflammation.
Besides, the role of AGE-RAGE interaction in promoting chronic inflammatory diseases has been increasingly recognized. AGE is formed when reducing sugars nonenzymatically bind to proteins or lipids, a process that is enhanced by hyperglycemic and hyperlipidemic environments of numerous metabolic disorders including diabetes and its complications (e.g., periodontitis)9. sRAGE, a decoy receptor for AGE, is associated with diabetes when a lower level of this soluble receptor which present in the circulation. In this study, AGE-challenged Mφs showed a decrease in the levels of sRAGE. But CMC2.24-treated Mφs significantly increased the levels of sRAGE and brought them back to normal. This indicated an additional mechanism that CMC2.24 resolve inflammation through AGE-RAGE/sRAGE signaling.
Moreover, another mechanism of CMC2.24’s pleiotropic efficacy is indicated by the conversion of the M1 pro-inflammatory phenotype to the M2 pro-resolving phenotype. In terms of both phenotype and function, Mφs have remarkable heterogeneity64, reflected in their specialization and also the marked changes in their activity and gene expression when facing challenges in the microenvironment. Our study demonstrated that the CMC2.24-treated Mφs significantly increased the ratio of M2/M1, and enhanced the conversion of Mφs from the M1 to M2 phenotype. This effect appeared to be attributed primarily due to the suppression of the M1 phenotype population; and due to the early promotion of the M2 phenotype population. As we observed, at 18 h, the challenge with either LPS or AGE and treatment with CMC2.24 can dramatically suppress the M1 phenotype as indicated by a lower expression of the M1 cell surface marker, CD38, compared to the non-treated or challenge-only groups. In contrast, the M2 phenotype population under the same conditions was markedly increased at 6 h after CMC2.24 therapy. This early effect can be lasting for 18 h as made evident by a high expression of the M2 cell-surface marker, CD163. The scatter diagram confirmed our hypothesis that CMC2.24 produced a “shifting” of Mφs from the M1 towards the M2 phenotype using flow cytometry (Figs. 4d, 5d). Therefore, CMC2.24 appears to be a highly potent inhibitor of the M1 phenotype (probably related to the inhibition of the M1 macrophage differentiation or maturation, or both); and a promoter of the pro-resolving M2 macrophage, thus acting like a “switch”.
Conclusion
Taken together, these results continue to expand the pleiotropic mechanisms of the novel chemically-modified curcumin 2.24, by (a) inhibiting inflammatory and tissue-destructive mediators including cytokines and MMPs; (b) upregulating resolvin-enhancing (RvD1) activity; and (c) promoting the expression of sRAGE; as well as (d) contributing to macrophage polarization from the M1 towards M2 phenotype (Fig. 6). Therefore, CMC2.24 can be a promising drug in treating diabetes-associated periodontitis. And the challenge for the future will be to demonstrate the safety and efficacy of this pleiotropic compound for the treatment of human chronic inflammatory diseases including diabetes, periodontitis, and others.
Supplementary Information
Acknowledgements
This study was funded by Stony Brook University Research Foundation (SUNY RF) Project (grant number 1050308), the National Natural Science Foundation of China (Grant Numbers: #82201063; 82071172), and the National Key Clinical Specialty Construction Project (Grant Number PKUSSNMP-201902). The authors of this study thank the veterinary and technical personnel of the DLAR for their assistance during animal handling and experimental procedures. The authors also thank Hou-Lin Hong (Department of Public Health, School of Medicine, Stony Brook University, NY, USA) for assistance with the cell study and data acquisition.
Abbreviations
- AGE/A
Advanced-glycation-end products
- CFPFs
Cell-free peritoneal fractions
- CMC2.24
Chemically-modified curcumin 2.24
- EDTA
Ethylenediaminetetraacetic acid
- ELISA
Enzyme-linked immunosorbent assay
- HMT
Host modulation therapy
- IL-1β
Interleukin-1 beta
- IL-6
Interleukin-6
- LPS/L
Lipopolysaccharide
- LxA4
Lipoxin A4
- Mφs
Macrophages
- MMPs (e.g., MMP-2 or -9)
Matrix metalloproteinases
- P.g.
Porphyromonas gingivalis
- PMNs
Polymorphonuclear leukocytes
- PW
Peritoneal washes
- RAGE
Receptors for AGE
- RvD1
Resolvins D1
- RvE1
Resolvins E1
- sRAGE
soluble receptor for AGE
- TNF-α
Tumor necrosis factor-alpha
Author contributions
J.D. was the principal experiment investigator, had substantial contributions to the acquisition, analysis, and interpretation of data, and was a major contributor to writing the manuscript. L.G., H-M.L., and Y.G. made substantial contributions to the conception, design of the work, acquisition, interpretation of data, and substantively revised the manuscript. H–D.B. helped to perform experiments and contributed to the acquisition and data analysis. F.J. and T-M.X. revised the main manuscript. All authors reviewed the manuscript and approved the submitted version.
Data availability
Data supporting the findings of the current study are available from the corresponding author upon reasonable request.
Competing interests
LM Golub is listed as an inventor on several related patents, including CMC2.24, and these have been fully assigned to his institution, Stony Brook University, The State University of New York (SUNY). F Johnson is also listed as an inventor on several related patents, including CMC2.24, which have been fully assigned to Stony Brook University and to Chem-Master Int. Inc., on a shared basis. In addition, Traverse Biosciences Inc. has exclusively licensed patents from the Research Foundation for the State University of New York (RF/SUNY) covering the structure and use of the chemically-modified curcumins for the purpose of commercialization in human and animal health. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
The online version contains supplementary material available at 10.1038/s41598-023-42848-x.
References
- 1.Wu YY, Xiao E, Graves DT. Diabetes mellitus related bone metabolism and periodontal disease. Int. J. Oral. Sci. 2015;7:63–72. doi: 10.1038/ijos.2015.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Caton JG, et al. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018;45(Suppl 20):S1–S8. doi: 10.1111/jcpe.12935. [DOI] [PubMed] [Google Scholar]
- 3.Frankwich K, et al. Proof of Concept: Matrix metalloproteinase inhibitor decreases inflammation and improves muscle insulin sensitivity in people with type 2 diabetes. J. Inflamm. (Lond.) 2012;9:35. doi: 10.1186/1476-9255-9-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.DeLano FA, Schmid-Schonbein GW. Proteinase activity and receptor cleavage: Mechanism for insulin resistance in the spontaneously hypertensive rat. Hypertension. 2008;52:415–423. doi: 10.1161/HYPERTENSIONAHA.107.104356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Golub LM, Payne JB, Reinhardt RA, Nieman G. Can systemic diseases co-induce (not just exacerbate) periodontitis? A hypothetical "two-hit" model. J. Dent. Res. 2006;85:102–105. doi: 10.1177/154405910608500201. [DOI] [PubMed] [Google Scholar]
- 6.Socransky SS, Haffajee AD, Cugini MA, Smith C, Kent RL., Jr Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998;25:134–144. doi: 10.1111/j.1600-051X.1998.tb02419.x. [DOI] [PubMed] [Google Scholar]
- 7.Cekici A, Kantarci A, Hasturk H, Van Dyke TE. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol. 2014;2000(64):57–80. doi: 10.1111/prd.12002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Singh VP, Bali A, Singh N, Jaggi AS. Advanced glycation end products and diabetic complications. Kor. J. Physiol. Pharmacol. 2014;18:1–14. doi: 10.4196/kjpp.2014.18.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ruiz HH, Ramasamy R, Schmidt AM. Advanced glycation end products: Building on the concept of the "Common Soil" in metabolic disease. Endocrinology. 2020;161:1. doi: 10.1210/endocr/bqz006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Farhan SS, Hussain SA. Advanced glycation end products (AGEs) and their soluble receptors (sRAGE) as early predictors of reno-vascular complications in patients with uncontrolled type 2 diabetes mellitus. Diabetes Metab. Syndr. 2019;13:2457–2461. doi: 10.1016/j.dsx.2019.06.019. [DOI] [PubMed] [Google Scholar]
- 11.Parisi L, et al. Macrophage polarization in chronic inflammatory diseases: Killers or builders? J. Immunol. Res. 2018;2018:8917804. doi: 10.1155/2018/8917804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Yu T, et al. Enhanced activity of the macrophage M1/M2 phenotypes and phenotypic switch to M1 in periodontal infection. J. Periodontol. 2016;87:1092–1102. doi: 10.1902/jop.2016.160081. [DOI] [PubMed] [Google Scholar]
- 13.Guo Y, et al. AGEs induced autophagy impairs cutaneous wound healing via stimulating macrophage polarization to M1 in diabetes. Sci. Rep. 2016;6:36416. doi: 10.1038/srep36416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kang JW, Lee SM. Resolvin D1 protects the liver from ischemia/reperfusion injury by enhancing M2 macrophage polarization and efferocytosis. Biochim Biophys Acta. 1861;1025–1035:2016. doi: 10.1016/j.bbalip.2016.06.002. [DOI] [PubMed] [Google Scholar]
- 15.Preshaw PM. Host response modulation in periodontics. Periodontol. 2008;2000(48):92–110. doi: 10.1111/j.1600-0757.2008.00252.x. [DOI] [PubMed] [Google Scholar]
- 16.Lauhio A, et al. Association of MMP-8 with obesity, smoking and insulin resistance. Eur. J. Clin. Invest. 2016;46:757–765. doi: 10.1111/eci.12649. [DOI] [PubMed] [Google Scholar]
- 17.Golub LM, et al. Tetracyclines inhibit connective tissue breakdown by multiple non-antimicrobial mechanisms. Adv. Dent. Res. 1998;12:12–26. doi: 10.1177/08959374980120010501. [DOI] [PubMed] [Google Scholar]
- 18.Payne JB, Reinhardt RA. Potential application of low-dose doxycycline to treat periodontitis in post-menopausal women. Adv. Dent. Res. 1998;12:166–169. doi: 10.1177/08959374980120011401. [DOI] [PubMed] [Google Scholar]
- 19.O'Dell JR, et al. Treatment of early seropositive rheumatoid arthritis: Doxycycline plus methotrexate versus methotrexate alone. Arthritis Rheum. 2006;54:621–627. doi: 10.1002/art.21620. [DOI] [PubMed] [Google Scholar]
- 20.Brandt KD, et al. Effects of doxycycline on progression of osteoarthritis: Results of a randomized, placebo-controlled, double-blind trial. Arthritis Rheum. 2005;52:2015–2025. doi: 10.1002/art.21122. [DOI] [PubMed] [Google Scholar]
- 21.Gu Y, Walker C, Ryan ME, Payne JB, Golub LM. Non-antibacterial tetracycline formulations: clinical applications in dentistry and medicine. J. Oral. Microbiol. 2012;4:1. doi: 10.3402/jom.v4i0.19227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Serhan CN, Chiang N, Dalli J, Levy BD. Lipid mediators in the resolution of inflammation. Cold Spring. Harb. Perspect. Biol. 2014;7:a016311. doi: 10.1101/cshperspect.a016311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Serhan CN. Systems approach with inflammatory exudates uncovers novel anti-inflammatory and pro-resolving mediators. Prostagland. Leukot Essent Fatty Acids. 2008;79:157–163. doi: 10.1016/j.plefa.2008.09.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rey C, et al. Resolvin D1 and E1 promote resolution of inflammation in microglial cells in vitro. Brain Behav. Immun. 2016;55:249–259. doi: 10.1016/j.bbi.2015.12.013. [DOI] [PubMed] [Google Scholar]
- 25.Ariel A, Serhan CN. Resolvins and protectins in the termination program of acute inflammation. Trends Immunol. 2007;28:176–183. doi: 10.1016/j.it.2007.02.007. [DOI] [PubMed] [Google Scholar]
- 26.Spite M, Serhan CN. Novel lipid mediators promote resolution of acute inflammation: impact of aspirin and statins. Circ. Res. 2010;107:1170–1184. doi: 10.1161/CIRCRESAHA.110.223883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Caton J, Ryan ME. Clinical studies on the management of periodontal diseases utilizing subantimicrobial dose doxycycline (SDD) Pharmacol. Res. 2011;63:114–120. doi: 10.1016/j.phrs.2010.12.003. [DOI] [PubMed] [Google Scholar]
- 28.Deng J, et al. A novel modified-curcumin promotes resolvin-like activity and reduces bone loss in diabetes-induced experimental periodontitis. J. Inflamm. Res. 2021;14:5337–5347. doi: 10.2147/JIR.S330157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Deng J, et al. Chemically-modified curcumin 2.24: A novel systemic therapy for natural periodontitis in dogs. J Exp Pharmacol. 2020;12:47–60. doi: 10.2147/JEP.S236792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Deng J, et al. A novel chemically-modified curcumin 2.24: Short-term systemic therapy for natural periodontitis in dogs. Front. Dent. Med. 2021;2:1. doi: 10.3389/fdmed.2021.609795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Elburki MS, et al. A chemically modified curcumin (CMC 2.24) inhibits nuclear factor kappaB activation and inflammatory bone loss in murine models of LPS-induced experimental periodontitis and diabetes-associated natural periodontitis. Inflammation. 2017;40:1436–1449. doi: 10.1007/s10753-017-0587-4. [DOI] [PubMed] [Google Scholar]
- 32.Elburki MS, et al. A novel chemically modified curcumin reduces inflammation-mediated connective tissue breakdown in a rat model of diabetes: periodontal and systemic effects. J. Periodontal. Res. 2017;52:186–200. doi: 10.1111/jre.12381. [DOI] [PubMed] [Google Scholar]
- 33.Elburki, M. S. A Novel Chemically Modified Curcumin as a Pleiotropic MMP-Inhibitor: Therapeutic Potential in Locally- and Systemically-Induced Periodontal (and other) Connective Tissue Breakdown Doctor of Philosophy thesis, Stony Brook University (2015).
- 34.Elburki MS, et al. A novel chemically modified curcumin reduces severity of experimental periodontal disease in rats: Initial observations. Mediat. Inflamm. 2014;2014:9571. doi: 10.1155/2014/959471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Elburki MS, Goren AD, Lee HM, Golub LM. Chemically-modified curcumins and alveolar bone loss in diabetic rats. J. Dent. Res. 2011;90:2295. [Google Scholar]
- 36.Bhatt HD, et al. The maximum-tolerated dose and pharmacokinetics of a novel chemically modified curcumin in rats. J. Exp. Pharmacol. 2022;14:73–85. doi: 10.2147/jep.S341927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Percie du Sert N, et al. Reporting animal research: Explanation and elaboration for the ARRIVE guidelines 2.0. PLoS Biol. 2020;18:3011. doi: 10.1371/journal.pbio.3000411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Liao G, Simone J, Simon SR. Paracrine downregulation of Fc gamma RIII in human monocyte-derived macrophages induced by phagocytosis of nonopsonized particles. Blood. 1994;83:2294–2304. doi: 10.1182/blood.V83.8.2294.2294. [DOI] [PubMed] [Google Scholar]
- 39.Helinski EH, Bielat KL, Ovak GM, Pauly JL. Long-term cultivation of functional human macrophages in Teflon dishes with serum-free media. J. Leukoc. Biol. 1988;44:111–121. doi: 10.1002/jlb.44.2.111. [DOI] [PubMed] [Google Scholar]
- 40.Petit-Bertron AF, Fitting C, Cavaillon JM, Adib-Conquy M. Adherence influences monocyte responsiveness to interleukin-10. J. Leukoc. Biol. 2003;73:145–154. doi: 10.1189/jlb.0802388. [DOI] [PubMed] [Google Scholar]
- 41.Miao X, Leng X, Zhang Q. The current state of nanoparticle-induced macrophage polarization and reprogramming research. Int. J. Mol. Sci. 2017;18:1. doi: 10.3390/ijms18020336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Gabrusiewicz K, et al. Glioblastoma-infiltrated innate immune cells resemble M0 macrophage phenotype. JCI Insight. 2016;1:1. doi: 10.1172/jci.insight.85841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Wentworth JM, et al. Pro-inflammatory CD11c+CD206+ adipose tissue macrophages are associated with insulin resistance in human obesity. Diabetes. 2010;59:1648–1656. doi: 10.2337/db09-0287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Jablonski KA, et al. Novel markers to delineate murine M1 and M2 macrophages. PLoS ONE. 2015;10:e0145342. doi: 10.1371/journal.pone.0145342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lam JH, et al. Expression of CD38 on macrophages predicts improved prognosis in hepatocellular carcinoma. Front. Immunol. 2019;10:2093. doi: 10.3389/fimmu.2019.02093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Etzerodt A, Moestrup SK. CD163 and inflammation: Biological, diagnostic, and therapeutic aspects. Antioxid. Redox Signal. 2013;18:2352–2363. doi: 10.1089/ars.2012.4834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Lau SK, Chu PG, Weiss LM. Cd163: A specific marker of macrophages in paraffin-embedded tissue samples. Am. J. Clin. Pathol. 2004;122:794–801. doi: 10.1309/qhd6yfn81kqxuuh6. [DOI] [PubMed] [Google Scholar]
- 48.Chen S, So EC, Strome SE, Zhang X. Impact of detachment methods on M2 macrophage phenotype and function. J. Immunol. Methods. 2015;426:56–61. doi: 10.1016/j.jim.2015.08.001. [DOI] [PubMed] [Google Scholar]
- 49.Yang J, et al. Enhanced activity of macrophage M1/M2 phenotypes in periodontitis. Arch. Oral. Biol. 2018;96:234–242. doi: 10.1016/j.archoralbio.2017.03.006. [DOI] [PubMed] [Google Scholar]
- 50.Golub LM, et al. A chemically modified nonantimicrobial tetracycline (CMT-8) inhibits gingival matrix metalloproteinases, periodontal breakdown, and extra-oral bone loss in ovariectomized rats. Ann. NY Acad. Sci. 1999;878:290–310. doi: 10.1111/j.1749-6632.1999.tb07691.x. [DOI] [PubMed] [Google Scholar]
- 51.Lee HM, et al. CMT-3, a non-antimicrobial tetracycline (TC), inhibits MT1-MMP activity: Relevance to cancer. Curr. Med. Chem. 2001;8:257–260. doi: 10.2174/0929867013373660. [DOI] [PubMed] [Google Scholar]
- 52.Golub LM, et al. Non-antibacterial tetracycline formulations: Host-modulators in the treatment of periodontitis and relevant systemic diseases. Int. Dent. J. 2016;66:127–135. doi: 10.1111/idj.12221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Dezube BJ, Krown SE, Lee JY, Bauer KS, Aboulafia DM. Randomized phase II trial of matrix metalloproteinase inhibitor COL-3 in AIDS-related Kaposi's sarcoma: An AIDS Malignancy Consortium Study. J. Clin. Oncol. 2006;24:1389–1394. doi: 10.1200/JCO.2005.04.2614. [DOI] [PubMed] [Google Scholar]
- 54.Golub LM, Lee HM. Periodontal therapeutics: Current host-modulation agents and future directions. Periodontol. 2020;2000(82):186–204. doi: 10.1111/prd.12315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Zhou Y, et al. Curcumin modulates macrophage polarization through the inhibition of the toll-like receptor 4 expression and its signaling pathways. Cell Physiol. Biochem. 2015;36:631–641. doi: 10.1159/000430126. [DOI] [PubMed] [Google Scholar]
- 56.Gao S, et al. Curcumin induces M2 macrophage polarization by secretion IL-4 and/or IL-13. J. Mol. Cell Cardiol. 2015;85:131–139. doi: 10.1016/j.yjmcc.2015.04.025. [DOI] [PubMed] [Google Scholar]
- 57.Zhang Y, et al. Design, synthesis and biological activity of new polyenolic inhibitors of matrix metalloproteinases: A focus on chemically-modified curcumins. Curr. Med. Chem. 2012;19:4348–4358. doi: 10.2174/092986712802884295. [DOI] [PubMed] [Google Scholar]
- 58.Zhang Y, Golub LM, Johnson F, Wishnia A. pKa, zinc- and serum albumin-binding of curcumin and two novel biologically-active chemically-modified curcumins. Curr. Med. Chem. 2012;19:4367–4375. doi: 10.2174/092986712802884240. [DOI] [PubMed] [Google Scholar]
- 59.Curylofo-Zotti FA, et al. Differential effects of natural Curcumin and chemically modified curcumin on inflammation and bone resorption in model of experimental periodontitis. Arch. Oral. Biol. 2018;91:42–50. doi: 10.1016/j.archoralbio.2018.04.007. [DOI] [PubMed] [Google Scholar]
- 60.Nee L, Tuite N, Ryan MP, McMorrow T. TNF-alpha and IL-1 beta-mediated regulation of MMP-9 and TIMP-1 in human glomerular mesangial cells. Nephron. Exp. Nephrol. 2007;107:e73–86. doi: 10.1159/000108645. [DOI] [PubMed] [Google Scholar]
- 61.Serhan CN, Petasis NA. Resolvins and protectins in inflammation resolution. Chem. Rev. 2011;111:5922–5943. doi: 10.1021/cr100396c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Zhang HW, et al. RvD1 ameliorates LPS-induced acute lung injury via the suppression of neutrophil infiltration by reducing CXCL2 expression and release from resident alveolar macrophages. Int. Immunopharmacol. 2019;76:105877. doi: 10.1016/j.intimp.2019.105877. [DOI] [PubMed] [Google Scholar]
- 63.Yin Y, Chen F, Wang W, Wang H, Zhang X. Resolvin D1 inhibits inflammatory response in STZ-induced diabetic retinopathy rats: Possible involvement of NLRP3 inflammasome and NF-kappaB signaling pathway. Mol. Vis. 2017;23:242–250. [PMC free article] [PubMed] [Google Scholar]
- 64.Lawrence T, Natoli G. Transcriptional regulation of macrophage polarization: enabling diversity with identity. Nat. Rev. Immunol. 2011;11:750–761. doi: 10.1038/nri3088. [DOI] [PubMed] [Google Scholar]
- 65.Shu B, et al. Blockade of CD38 diminishes lipopolysaccharide-induced macrophage classical activation and acute kidney injury involving NF-kappaB signaling suppression. Cell Signal. 2018;42:249–258. doi: 10.1016/j.cellsig.2017.10.014. [DOI] [PubMed] [Google Scholar]
- 66.Alvarado-Vazquez PA, et al. Macrophage-specific nanotechnology-driven CD163 overexpression in human macrophages results in an M2 phenotype under inflammatory conditions. Immunobiology. 2017;222:900–912. doi: 10.1016/j.imbio.2017.05.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Schaer CA, Schoedon G, Imhof A, Kurrer MO, Schaer DJ. Constitutive endocytosis of CD163 mediates hemoglobin-heme uptake and determines the noninflammatory and protective transcriptional response of macrophages to hemoglobin. Circ Res. 2006;99:943–950. doi: 10.1161/01.RES.0000247067.34173.1b. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data supporting the findings of the current study are available from the corresponding author upon reasonable request.