

Abstract
Policy Points.
The erosion of electoral democracy in the United States in recent decades may have contributed to the high and rising working‐age mortality rates, which predate the COVID‐19 pandemic.
Eroding electoral democracy in a US state was associated with higher working‐age mortality from homicide, suicide, and especially from drug poisoning and infectious disease.
State and federal efforts to strengthen electoral democracy, such as banning partisan gerrymandering, improving voter enfranchisement, and reforming campaign finance laws, could potentially avert thousands of deaths each year among working‐age adults.
Context
Working‐age mortality rates are high and rising in the United States, an alarming fact that predates the COVID‐19 pandemic. Although several reasons for the high and rising rates have been hypothesized, the potential role of democratic erosion has been overlooked. This study examined the association between electoral democracy and working‐age mortality and assessed how economic, behavioral, and social factors may have contributed to it.
Methods
We used the State Democracy Index (SDI), an annual summary of each state's electoral democracy from 2000 to 2018. We merged the SDI with annual age‐adjusted mortality rates for adults 25–64 years in each state. Models estimated the association between the SDI and working‐age mortality (from all causes and six specific causes) within states, adjusting for political party control, safety net generosity, union coverage, immigrant population, and stable characteristics of states. We assessed whether economic (income, unemployment), behavioral (alcohol consumption, sleep), and social (marriage, violent crime, incarceration) factors accounted for the association.
Findings
Increasing electoral democracy in a state from a moderate level (defined as the third quintile of the SDI distribution) to a high level (defined as the fifth quintile) was associated with an estimated 3.2% and 2.7% lower mortality rate among working‐age men and women, respectively, over the next year. Increasing electoral democracy in all states from the third to the fifth quintile of the SDI distribution may have resulted in 20,408 fewer working‐age deaths in 2019. The democracy–mortality association mainly reflected social factors and, to a lesser extent, health behaviors. Increasing electoral democracy in a state was mostly strongly associated with lower mortality from drug poisoning and infectious diseases, followed by reductions in homicide and suicide.
Conclusions
Erosion of electoral democracy is a threat to population health. This study adds to growing evidence that electoral democracy and population health are inextricably linked.
Keywords: democracy, elections, voting, US states, working‐age mortality
Mortality rates among working‐age adults are high and rising in the United States, an alarming fact that predates the COVID‐19 pandemic. 1 The trend has occurred across numerous causes of death (although suicides and drug poisoning have garnered the most attention), defying a simple explanation. 1 , 2 In addition, working‐age mortality rates have become increasingly unequal across geographic areas of the country. For instance, in 2017, the age‐adjusted mortality rate among working‐age adults in West Virginia (568 deaths per 100,000 persons aged 25–64) was 2.2 times greater than the rate in Minnesota (259 deaths per 100,000 persons aged 25–64). 2
The reasons for the high and rising mortality of working‐age adults have not been fully identified. However, a 2021 National Academies of Sciences, Engineering, and Medicine (NASEM) report provided a helpful framework of potential explanations. 1 It proposed explanations at the macro level (e.g., federal and state policies), meso level (e.g., work and family environments), and micro level (e.g., health behaviors). The NASEM report emphasized the macro level because it influences meso‐ and micro‐level factors. As an example, state policies on paid sick leave and abortion (macro level) can affect work and family environments (meso level), and state policies on tobacco control and marijuana legalization can affect health behaviors (micro level). Several studies find compelling evidence that state policies have played a role in the high and rising working‐age mortality rates. 3 , 4 , 5 Policies on gun safety, labor, tobacco tax, environment, economic taxes, criminal justice, and marijuana appear to be important, with more liberal versions of each policy domain (except marijuana) associated with lower mortality. 5 Studies also conclude that changes in education levels and income of states’ populations do not explain diverging trends in working‐age mortality across states. 3 Although the policy contexts of US states in recent decades appear to have played a role in the rise of working‐age mortality, they are not the only explanation.
One macro‐level factor that has been largely overlooked as a potential explanation is democracy. Despite alarm bells from scientists 6 , 7 , 8 , 9 , 10 and journalists 11 , 12 about democratic backsliding in the United States and its pernicious consequences, the role of democracy has been largely absent from studies of the high and rising working‐age mortality. Democratic backsliding refers to “the processes through which elected rulers weaken checks on executive power, curtail political and civil liberties, and undermine the integrity of the electoral system.” 13 Several events in recent decades have greased the wheels of the backsliding, such as the 2013 Supreme Court decision in Shelby County v. Holder to eliminate a key provision of the Voting Rights Act and the Court's 2010 decision in Citizens United v. Federal Election Commission to remove spending limits on elections from corporations and special interest groups. Importantly, the degree of democratic backsliding has differed dramatically across US states. In fact, a study of the 2000–2018 period documented backsliding in some states juxtaposed against democratic expansion in others. 7
If democracy matters for population health, then democratic backsliding in many US states may have contributed to the high mortality rates of working‐age adults. Conceptually, democracy profoundly matters for population health. 14 As Wise and Sainsbury asserted, democracy matters because 1) “active participation in societies’ decision‐making structures and processes confers recognition and respect that are essential to the health of individuals and populations,” 2) “participation is necessary to ensure that decisions are based on consideration of a full range of perspectives on problems and solutions,” and 3) “participation occurs at the levels of power where decisions over the allocation of material resources are made, thereby ensuring that the distribution of material resources is more likely to be fair and just.” 14 A core theme in all three assertions is the societal distribution of power. Democratic functioning is inextricably tied to the distribution of power resources across key institutions, notably business, labor unions, political parties, and electoral processes. 15 , 16 , 17 In general, places with strong labor power, left‐leaning political parties, and robust electoral processes have more egalitarian distribution of resources, more generous social policies, and better population health. 15 , 16 , 17 , 18 , 19 The next sections highlight evidence on the overall democracy–health association and electoral democracy in particular.
Democracy and Population Health in International Studies
Studies of the democracy–health association have largely relied on international comparisons. 18 Most find that stronger democracies have longer life expectancy and better health than weaker democracies or autocracies. 14 , 18 , 20 In fact, a systematic review found that over 80% of studies examining democracy and health across countries documented a strong positive association, even when accounting for country‐level characteristics such as education levels, income, and income inequality. 18 Although there is some disagreement about whether the association between democracy and health is a causal one, an analysis of changes in democratic functioning over 46 years and across 170 countries provided compelling evidence of a causal effect on mortality. 21 A country's level of democratic functioning may even have affected excess deaths during the COVID‐19 pandemic. A study of 78 countries found that those with stronger democratic governance had significantly fewer excess deaths during the first 18 months of the pandemic, net of confounding factors such as COVID‐19 case rates and vaccination rates. 22
To better understand why democracy matters for population health, it is instructive to consider various components of democracy. Blunt measures of democracy, such as democratic versus autocratic, obscure specific components that may be most salient for population health. 18 , 20 Patterson speculated that electoral democracy (referring to free and fair elections) may be key to understanding the democracy–health association and asserted that this component is key for health for two main reasons. 20 One is accountability to constituents. To appease constituents and ensure reelection, leaders may advocate policies that improve their constituents’ well‐being and health. The second reason is redistribution. Democratic elections allow constituents to vote for egalitarian policies or for leaders who support those policies, which directly or indirectly impact the social determinants of health such as income inequality, poverty, and discrimination.
A few studies have examined how components of democracy, including electoral democracy, impact health. A study of how democratic governance predicted excess deaths in 78 countries during the first 18 months of the COVID‐19 pandemic examined several components in the Varieties of Democracy (V‐Dem) Liberal Democracy Index. 22 , 23 Most important was the deliberative principle. Countries scoring high on it make decisions based on respectful dialogue, the common good, consultation with a range of stakeholders, and an engaged and informed society. These countries fared best in excess deaths. Another study of 170 countries over a 46‐year period examined how components of the V‐Dem's Multiplicative Polyarchy Index predicted mortality and found the “free and fair elections” component to be most important. 21 Its authors concluded that such elections benefit population health by holding lawmakers accountable to a wide swath of the population rather than special interest groups. An analysis of 168 countries during the 1960–2010 period found that life expectancy rose by two years and infant mortality fell by 12.7% the first year after a country transitioned to an electoral democracy. 24
Democracy and Population Health in US States
Despite the large number of studies examining democracy and health across countries, little attention has been given to democracy and health across US states. Noting this glaring omission, a recent study examined how US states’ democratic institutions predicted mortality. 25 It used two annual measures of democratic institutions during the 1975–2016 period. One measure, political accountability, included factors such as states’ campaign finance regulations, ballot initiatives, and term limits. The other measure, checks and balances, included factors such as states’ veto override rules and gubernatorial power. The study reported that higher levels of political accountability predicted lower infant mortality, whereas stronger checks and balances predicted longer life expectancy, net of states’ policy liberalism and political party control, leading the authors to conclude that democratic institutions are critical for population health.
Building on that study 25 and the importance of electoral democracy highlighted above, the current study examines how US states’ electoral democracy is associated with working‐age mortality. Electoral democracy is the component of democracy that varies most across states in recent decades. 7 We use the newly‐developed State Democracy Index (SDI), an annual summary measure of 51 indicators of electoral democracy for each state from 2000 to 2018. 6 , 7 Examples of the indicators include absentee voting, early voting, felony disenfranchisement, partisan symmetry of gerrymandering, and differences between constituents’ opinions and their states’ policies on economic and social issues. Trends in the SDI differ across states, exhibiting five archetypes. Specifically, the trends can be characterized as 1) gradually increasing, 2) gradually decreasing, 3) abruptly decreasing, 4) fluctuating, or 5) exhibiting little change. Figure 1 illustrates these five archetypes by showing trends in one state within each archetype; these states are Arizona, Oklahoma, North Carolina, Michigan, and Iowa, respectively. The figure also shows how the range in SDI scores across these five states widened over time. The widening is also apparent across all 50 states: the SDI scores across all states ranged from −2.1 to 1.5 (a gap of 3.6) in 2000 and from −3.1 to 1.9 (a gap of 5.0) in 2018.
Figure 1.
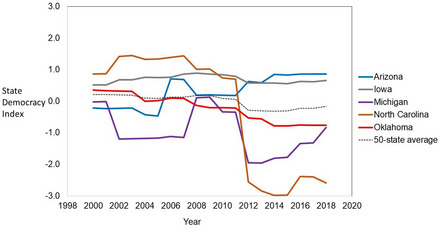
The SDI Over Time for Five Archetype Trends [Colour figure can be viewed at wileyonlinelibrary.com]
The State Democracy Index (SDI) comes from Grumbach. 6 , 7 The five archetype trends among the 50 states include gradually increasing SDI (e.g., Arizona), gradually decreasing SDI (e.g., Oklahoma), abruptly decreasing SDI (e.g., North Carolina), fluctuating SDI (e.g., Michigan), and little change in SDI (e.g., Iowa).
States’ electoral democracy may impact working‐age mortality directly and indirectly. This study considers three factors that may be affected by electoral democracy and that may, in turn, affect mortality. The first is economic circumstances. Democracy in general, and electoral democracy in particular, can shape the levels and distribution of economic well‐being (via taxation, social spending, etc.) and the responsiveness of policymakers to the economic well‐being of various constituents such as workers and corporations. 20 , 21 A few studies have tested whether economic well‐being helps explain the democracy–health association. An analysis of 171 countries examined income, income inequality, health expenditures, and education levels, finding that only income helped explain part of the association. 26 Similarly, another international study found a role for economic prosperity, but not income inequality. 24 A study of US states’ democratic institutions and mortality examined income inequality and health insurance and found that neither explained the association. 25 Consequently, we include income and unemployment rates.
We also examine two behavioral factors. Conceptually, states with strong democracy in general and strong electoral democracy in particular make policy decisions that represent the preferences of their populations, with the greater good in mind. 20 , 21 These decisions can directly and indirectly impact health behaviors. For instance, states might raise excise taxes on alcohol, with population health in mind, or keep excise taxes low to appease businesses. States might mandate paid leave and enact a high minimum wage (with workers in mind) or offer neither and prohibit their municipalities from doing so (with businesses in mind). 27 Such policies can affect individuals’ stress and stress‐related behaviors. For instance, states’ paid leave policies reduce financial and emotional stress and working‐age women's risk of death from alcohol‐related causes. 28 , 29 It is also conceivable that perceiving democratic disfunction may be sufficient to affect health behaviors. A 2021 survey found that two‐thirds of US adults believed democracy is “under threat.” 30 A 2022 survey found that 70% percent of US adults did not think that the government cared about them, 64% felt their rights were under attack, 45% did not feel protected by US laws, and importantly, 75% of adults said that such stressors affected their anxiety, depression, substance use, and/or sleep problems 31 —all of which elevate mortality risk. The current study examines two behaviors—alcohol consumption and sleep—that may be quickly affected by changes in states’ democratic functioning and may be affected directly (e.g., via alcohol excise taxes) or indirectly (e.g., via stress). A prior study examined smoking as an explanation for why states’ democracy predicted working‐age mortality but found little evidence that it played a role. 25
The third factor is social functioning. We examine crime, incarceration, and a key social tie—marriage. Democracy in general, and electoral democracy in particular, could affect social functioning in myriad ways. In general, democracy can enhance social functioning by making political and policy decisions aligned with voters’ preferences, resulting in higher levels of happiness, life satisfaction, and subjective well‐being. 14 , 32 , 33 Democracy is also thought to reduce crime (and hence incarceration) through improved economic conditions, expansion of public schooling, social and economic equality, crime deterrence, judicial systems, perceived legitimacy of the government, respect for the law, social cohesion, and more. 34 , 35 , 36 International studies provide empirical support. 34 , 36 For instance, a study of 18 countries found that democracy (measured by an index that “concerns mainly the right of election”) increased minor crimes but significantly decreased serious crimes. 34 Crime and incarceration rates, in turn, have collateral consequences for families and entire communities. 37 , 38 , 39 , 40 , 41 Studies examining trends across multiple decades have shown that, when county‐level incarceration rates rise, county‐level mortality rates rise within one year. 39 , 40 Those collateral consequences are pronounced for deaths from infectious diseases, chronic lower respiratory diseases, substance use, and suicide. 39 Studies on the topic offer a range of explanations for incarceration's widespread impact on mortality, including the sudden destruction of psychological and material well‐being, dissolution of social ties such as marriage and friendships, and infectious disease spread. Rising rates of violent crime also appear to have widespread effects on mortality. A study of Chicago neighborhoods found that those experiencing a rise in violent crime saw a rise in cardiovascular mortality. 41 Explanations for the widespread impact of violent crime on mortality point to factors such as psychosocial distress, delays in seeking medical care, elevated blood pressure, and acute myocardial infarction. 41
Aims
This study has three main aims. The first aim is to estimate the association between electoral democracy and working‐age mortality within US states, net of states’ political party control, safety net policy generosity, union coverage, immigrant share of the population, and stable characteristics of states. The second aim is to estimate how many lives might be saved if all states expanded their electoral democracy. The third aim is to glean insights into potential explanations for the democracy–mortality association. For this aim, we first examine six causes of death. We speculate that their associations with electoral democracy will be stronger for causes most likely to be affected within the one‐year lag used in the study (e.g., drug poisoning, homicide, suicide) than causes such as heart disease. We then assess how economic, behavioral, and social factors may contribute to the association. The findings provide novel insights into how electoral democracy and democratic backsliding may affect life and death of working‐age Americans.
Data and Methods
Mortality Rates
Mortality data are from the restricted Multiple Cause of Death files, accessed through a data use agreement with the National Center for Health Statistics. Using that data, we calculated mortality rates for working‐age adults (ages 25–64 years) by state and year. The rates are sex specific, age adjusted to the 2000 US population, and calculated for 2000 through 2019. We included these years because our measure of electoral democracy spans 2000 to 2018. Including mortality data through 2019 provided another year of data for our analyses, allowed us to examine a lag between the last year of the electoral democracy measure and mortality, and avoided complications starting in 2020 from COVID‐19. We also examined six major causes of death. These causes and their International Classification of Diseases codes include heart disease (I00‐I09, I11, I13, I20‐I51), cancer (C00‐C97), suicide (X66‐X84, Y87.0), homicide (X86–X99, Y00–Y09, Y87.1), drug poisoning (X40‐X44, X60‐X64, X85, Y10‐Y14), and non‐HIV/AIDS infectious and parasitic diseases (A00‐A99, B00‐B19), hereafter “infectious diseases.” Suicide and drug poisoning deaths are mutually exclusive, as suicides by drugs are included in the drug poisoning deaths. 1
SDI
The SDI is an annual summary measure of 51 indicators of electoral democracy for each state from 2000 to 2018. 6 , 7 The indicators capture various measures of gerrymandering, electoral policies that affect the eligibility and cost of voting such as felony disenfranchisement, electoral policies that affect election integrity such as postelection audits, and democratic outcomes such as the similarity between constituents’ opinions and their states’ policies on social issues. Using Bayesian latent factor analysis, 42 Grumbach developed the SDI, finding that the 51 indicators of electoral democracy loaded onto a single latent factor and exhibited construct and convergent validity. 7 Appendix Figure S1 contains a histogram of the SDI. As explained below, our models use SDI quintiles: [−3.1, −0.51], (‐−0.51, −0.02], (−0.02, 0.292], (0.292, 0.674], and (0.674, 1.92].
Time‐Varying Covariates
We included political party control, safety net policy generosity, union coverage, and share of the population that were immigrants, based on conceptual frameworks and prior studies. 4 , 5 , 16 , 19 , 25 , 43 These covariates fluctuated considerably across the study period. They likely confound the association between electoral democracy and mortality (i.e., political party can affect democracy 7 but may also affect mortality 44 ). They could also operate as structural mediators of the association (i.e., electoral democracy may affect political party, which, in turn, affects mortality 25 ). Because of this inherent complexity, we avoid claiming that any covariate definitively precedes or follows changes in electoral democracy. Such claims are unnecessary for our study because its goal is to estimate how electoral democracy predicts working‐age mortality, net of these covarying structural factors.
Annual political party control was measured dichotomously such that 1 = Republican control in all branches (Governor, Senate, and House) and 0 = otherwise. The information used to construct the measure came from the National Welfare Data of the University of Kentucky's Center for Poverty Research (UKCPR). 45 Republicans controlled the Senate and House when they occupied more than 50% of the seats in each chamber. Nebraska is a special case because it has a unicameral form of government, so there are no formal party alignments or groups within its Senate. Its senators are officially listed as nonpartisan even though most are affiliated with a political party. Thus, for Nebraska, our annual measure of Republican control = 1 if the governor was Republican and the majority of senators were affiliated with the Republican party or 0 = otherwise. During the 2000–2018 period, 30 states experienced changes in this measure.
We measured safety net policy generosity using the same measures from Fenelon and Witko 43 in their study of state policy environments and mortality. It captures annual per capita expenditures (in thousands of dollars) on “programs that provide cash assistance, health insurance and care, or in‐kind benefits to the poor,” 43 among which the main programs are Medicaid, Temporary Assistance for Needy Families, Children's Health Insurance Program, and Supplemental Nutrition Assistance Program. We obtained the expenditure data from the Government Finance Database. 46 Other summary measures of state policy environments exist but do not capture recent years (e.g., the policy liberalism scores from Grumbach 47 and Caughey and Warshaw 48 end in 2014).
Annual data on union coverage came from the Union Membership and Coverage Database. 49 , 50 It captures the percentage of civilian, employed, wage and salary workers aged 16 and older who were covered by a union contract regardless of whether they were members of the union. 50 Lastly, the annual age‐adjusted share of each state's working‐age immigrant population was computed from the American Community Survey.
Potential Contributing Factors
We examined three groups of factors that may contribute to the association between electoral democracy and working‐age mortality: economic, behavioral, and social factors. We chose measures of each factor that could be affected by democratic functioning in a relatively short time period. For example, we include income instead of wealth and sleep instead of smoking.
One economic measure is median household income, in 2021 US dollars, from the US Census Bureau. 51 The other economic measure is the unemployment rate among the working‐age, civilian, noninstitutional population in the labor force from the UKCPR National Welfare Data.
The behavioral measures include alcohol consumption and sleep. Alcohol consumption is the per capita consumption, in gallons, of all types of alcoholic beverages among persons aged 14 and older. These annual data are provided by the National Institute on Alcohol Abuse and Alcoholism. 52 Two potential sources of state‐level sleep data are the Behavioral Risk Factor Surveillance System (BRFSS) and the Americans Time Use Survey (ATUS). We use the ATUS because, unlike the BRFSS, it asks respondents about sleep every calendar year. The downside of the ATUS is that it began in 2003. We imputed the sleep variable for the years 2000–2002 using linear time trends for each state. We created a binary measure to account for elevated health risks associated with short or long sleep. 53 Specifically, we categorized working‐age adults as has having sleep problems if they reported sleeping less than seven or more than nine hours per night. Using this information, we estimated the age‐adjusted percentage of the state's population in a given year with sleep problems.
We included three indicators of social functioning. We used the American Community Survey to estimate the age‐adjusted percentage of the working‐age population that was married in each year. Data on the incarcerated population were taken from the National Corrections Reporting Program, an offender‐level data set collected by states’ Departments of Corrections and maintained by the Bureau of Justice Statistics. 54 We computed the total number of offenders for each state and year, divided it by each state's total population, and multiplied it by 100,000 to obtain an incarceration rate per 100,000. Lastly, data on state‐level violent crime came from the Federal Bureau of Investigation's Crime Data Explorer (CDE). 55 Violent crimes in the CDE include murder and nonnegligent manslaughter, rape, robbery, and aggravated assault. We converted the crime data into a state‐year measure of violent crime per 100,000 individuals in the state. Both the incarceration and violent crime rates have eight missing observations. Like the sleep variable, we imputed the small number of missing values from state‐specific linear time trends.
Statistical Analyses
The general form of our regression model is shown in Equation 1. It estimates the natural log of the sex‐specific age‐adjusted mortality rate (AAMR), where s and t pertain to state and year, respectively. To control for stable differences among states, a conventional one‐way fixed‐effects model includes indicator variables for each state, and a two‐way fixed‐effects model also adds time indicators. To address critiques of those models in certain applications, 56 we used the recommended Mundlak regression 57 , 58 , 59 and converted the continuous measure of SDI into quintiles. The Mundlak regression is equivalent to one‐ and two‐way fixed‐effects estimators, but it is more flexible in incorporating covariates and potentially heterogeneous treatment effects. 57 , 59
| (1) |
Equation 1 contains a β1 vector of four coefficients for the SDI quintile indicators (quintile 3 is the omitted reference) and a β2 vector of four coefficients for the covariates. As a Mundlak regression, it includes interactions among the SDI quintile indicators and the difference between each state‐year observation of a covariate (and the covariate's average across time within the state. With five SDI quintiles and four covariates, the β3 vector contains 20 coefficients. The coefficient, δ, is for the linear year term. The β1 vector contains the coefficients of interest. In a causal framework, they are interpreted as average treatment effects. 59 Note that we do not claim that our estimates represent causal effects; we refer to them as associations. Standard errors were clustered by state and robust to heteroskedasticity and autocorrelation.
We estimated two sets of models. The first set used data in which each state's SDI in year “t” was merged with mortality in year “t.” Because changes in states’ electoral democracy may have delayed consequences, the second set of models used a one‐year lag such that each state's SDI in year “t” was merged with its mortality in year “t + 1.” This is a relatively short lag, but we note that changes in country‐level democracy affect population health and mortality within one year. 21 , 24
Results
The SDI is significantly associated with working‐age mortality rates. Figure 2 summarizes the model results for men (detailed results are in Appendix Tables S1 and S2). Panel A shows results from models without a time lag between the SDI score and mortality rates. The bars show the estimated percentage change in men's mortality rates if a state changed its SDI score from the third quintile to another quintile, net of the time‐varying covariates, stable characteristic of the state, and year. If a state were to increase its SDI from the third to the fifth quintile, the models estimated that men's all‐cause mortality rates would be a significant 2.9% (p = 0.02) lower. The association largely reflects deaths from drug poisoning, infectious diseases, and homicide. If a state were to increase its SDI from the third to the fifth quintile, the models estimated that men's mortality would be 16.8% lower for drug poisoning (p = 0.002), 10.9% lower for infectious diseases (p = 0.01), and 9.2% lower (p = 0.05) for homicide. If a state were to decrease its SDI from the third to the second quintile, the models estimated that men's suicide mortality would be 3.9% (p = 0.01) higher. States’ SDI scores were not associated with men's heart disease or cancer mortality.
Figure 2.
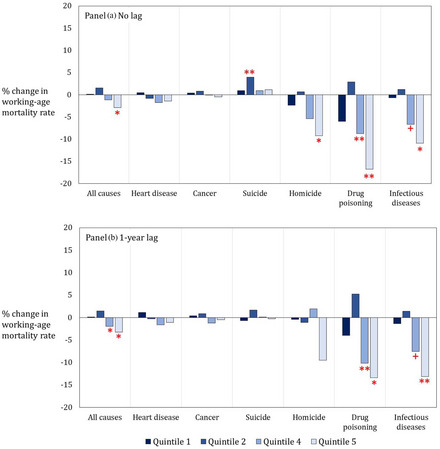
Estimated Percentage Change in Working‐Age Men's Mortality Rate if a State's Democracy Index Changed from Quintile 3 to Another Quintile [Colour figure can be viewed at wileyonlinelibrary.com]
** p < 0.01, * p < 0.05, + p < 0.10.
Figure 2, Panel B shows results from models with a one‐year lag between a state's SDI score and men's working‐age mortality rates in a state. Like the no‐lag models, moving from the third to the fifth quintile predicted a significantly lower all‐cause mortality rate (3.2% lower, p = 0.03). Unlike the no‐lag models, moving from the third to the fourth quintile also predicted a significantly lower all‐cause mortality rate (2.0% lower, p = 0.05). The association primarily reflected deaths from drug poisoning and infectious diseases. Moving from the third to the fifth SDI quintiles and from the third to the fourth SDI quintiles predicted significantly lower mortality rates from those two causes of death.
Figure 3 shows results for women (detailed results are in Appendix Tables S3 and S4). In Panel A, the results were similar to those for men. If a state increased its SDI score from the third to the fifth quintiles, women's all‐cause mortality was estimated to be 2.7% lower (p = 0.07). That same increase in the SDI predicted 12.0% lower drug poisoning mortality (p = 0.06) and 8.2% lower infectious disease mortality (p = 0.09). A state's SDI score also predicted women's suicide and homicide mortality rates in the state. Specifically, decreasing the SDI score in a state from the third to the second quintile predicted a 6.6% higher suicide rate (p = 0.05), whereas decreasing it from the third to the first quintile predicted a 7.9% higher homicide rate (p = 0.09). Similarly, in Panel B, the models with a one‐year lag show strong associations between the SDI and women's mortality from drug poisoning, infectious diseases, homicide, and suicide. Associations with heart disease and cancer appear, although they are much smaller in magnitude than those for drug poisoning, infectious diseases, and homicide.
Figure 3.
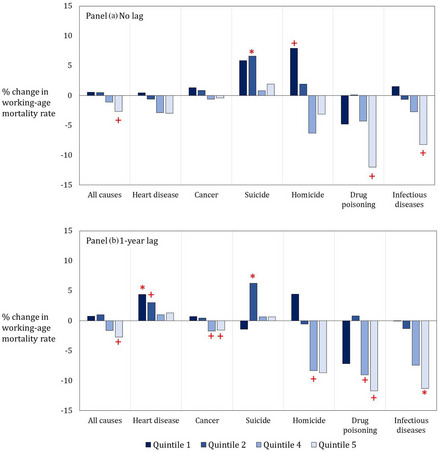
Estimated Percentage Change in Working‐Age Women's Mortality Rate if a State's Democracy Index Changed from Quintile 3 to Another Quintile [Colour figure can be viewed at wileyonlinelibrary.com]
*** p < 0.001, ** p < 0.01, * p < 0.05, + p < 0.10.
To address our second aim, we estimated the number of working‐age deaths in 2019 that could potentially have been averted if the SDI improved across all states in 2018 from the third to the fifth quintiles of the SDI distribution, ceteris paribus. Recall from above, using the one‐year lag models, that the estimated reduction in all‐cause mortality if a state's SDI changed from the third to the fifth quintile was 2.7% for women and 3.2% for men. We obtained the actual sex‐ and age‐specific mortality rates, death counts, and population sizes for working‐age adults in 2019 from CDC WONDER. 60 We then reduced those actual rates by 2.7% (women) and 3.2% (men) to estimate the number of working‐age deaths that would have occurred under the lower counterfactual mortality rates. The counterfactual estimates indicate that increasing the SDI score from the third to the fifth quintiles across all states in 2018 may have resulted in 20,408 fewer deaths in 2019 (6,914 among women and 13,494 among men). The detailed calculations are provided in Appendix Table S5. Moving from the first to the fifth or from the fifth to the first SDI quintiles would provide even larger estimates of averted deaths, but moving between the quintiles’ extremes was highly unusual during the period.
We now turn to the third aim of the study, which is to assess how economic, behavioral, and social factors may help account for the SDI–mortality association. Table 1 contains the main model results using a one‐year lag and examining all‐cause mortality. We focus on the coefficients for SDI quintile 5 to interpret the results (detailed model results are in Appendix Table S6). Model 1 for men is the same model estimated in aim 1. That is, men's working‐age mortality is estimated to be 3.2% lower (100 × [e−0.033 − 1]) if a state increased its SDI from the third to the fifth quintile, net of the controls. Economic conditions do not appear to account for that association as shown in model 2. The association remained and even increased to a small degree when median household income and unemployment were included in model 2 (it increased because the correlation between SDI and unemployment was sometimes positive during the study period). Including health behaviors reduced the SDI–mortality association by 11.5%, from −0.0330 (p = 0.03) in model 1 to −0.0292 (p = 0.05) in model 3. Including social functioning reduced it by 26.7% from model 1 to 4 (p = 0.08). Including all economic, behavioral, and social factors in model 5 did not further attenuate the association. The results for women are similar. Model 6 for women is the same model estimated in aim 1. That is, if a state increased its SDI from the third to the fifth quintile, women's mortality would be an estimated 2.9% lower (100 × [e−0.0277 − 1]), net of controls. Economic factors do not appear to account for the association, as shown in model 7. Including health behaviors reduced the association by 8.7%, from −0.0277 (p = 0.09) in model 6 to −0.0253 (p = 0.09) in model 8. Including social functioning reduced it by 29.2% from model 6 to 9 (p = 0.21). Including all factors in model 10 did not further attenuate the association.
Table 1.
Model Coefficients Predicting ln(Mortality Rates) from the SDI and Covariates
| Men | Women | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Predictors | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | Model 8 | Model 9 | Model 10 |
| SDI: (reference: quintile 3) | ||||||||||
| Quintile 1 | 0.0015 | −0.0135 | 0.0004 | −0.0070 | 0.0005 | 0.0073 | −0.0063 | 0.0053 | ‐0.0006 | 0.0004 |
| Quintile 2 | 0.0149 | 0.0047 | 0.0120 | 0.0001 | 0.0071 | 0.0101 | 0.0011 | 0.0077 | −0.0033 | −0.0013 |
| Quintile 4 | −0.0200+ | −0.0232* | −0.0189+ | −0.0187* | −0.0356* | −0.0162 | −0.0194* | −0.0148 | −0.0140 | −0.0297* |
| Quintile 5 | −0.0330* | −0.0380** | −0.0292+ | −0.0242+ | −0.0411+ | −0.0277+ | −0.0341* | −0.0253+ | −0.0196 | −0.0414+ |
| Covariates | ||||||||||
| Median HH income | −0.1034*** | −0.0741*** | −0.0941*** | −0.0703*** | ||||||
| Unemployment rate | 0.0674*** | ‐0.0032 | 0.0705*** | 0.0063 | ||||||
| % Problem sleeping | 0.0362*** | 0.0154*** | 0.0347*** | 0.0167*** | ||||||
| Alcohol consumption | −0.0725* | −0.0485** | −0.0902* | −0.0486** | ||||||
| % Married | −0.0206*** | −0.0077+ | −0.0113* | 0.0027 | ||||||
| Incarceration rate | 0.0004** | 0.0001 | 0.0006*** | 0.0002+ | ||||||
| Violent crime rate | 0.0004*** | 0.0004*** | 0.0004*** | 0.0004*** | ||||||
| % Immigrants | −0.0046+ | −0.0033* | −0.0077*** | −0.0114*** | −0.0075*** | −0.0065** | −0.0056*** | −0.0096*** | −0.0125*** | −0.0087*** |
| Republican control | −0.0520 | −0.0609 | −0.0429 | −0.0246 | −0.0650* | −0.0156 | −0.0232 | −0.0105 | −0.0175 | −0.0568+ |
| Policy generosity | 0.0645 | −0.0087 | −0.0314 | −0.0288 | −0.0625* | 0.0400 | −0.0297 | −0.0555 | −0.0305 | −0.0625** |
| % Union coverage | −0.0150** | −0.0073+ | −0.0083* | −0.0041 | 0.0004 | −0.0126** | −0.0057 | −0.0058+ | −0.0014 | 0.0019 |
Abbreviations: HH, household; SDI, State Democracy Index.
*** p < 0.001, ** p < 0.01, * p < 0.05, + p < 0.10.
The form of the regression model is shown in Equation 1. For parsimony, the year and interaction terms estimated in Equation 1 are not included in the above table. N = 950 state‐year observations. Detailed model results are available in Appendix Table S6. The data are lagged by one year such that the SDI in year “t” is merged with all covariates and mortality rates in year “t + 1.”
Discussion
Democracy is a core determinant of health. 14 Democracy in general, and electoral democracy in particular, shapes the nature of political decision making, policies, and power distributions, with potentially profound consequences for life and death. However, electoral democracy has eroded in recent decades in the United States, especially in some states. At the same time, the mortality rates of working‐age adults have risen, especially in some states. This study examined the association between states’ electoral democracy and their working‐age mortality and assessed how economic, behavioral, and social factors may have contributed to the association. Although our study estimated associations, not causal effects, it adds to a growing body of evidence that “democratic governance may be an especially powerful kind of preventive medicine” 24 and “elections and the health of the people are increasingly inseparable.” 21 Below, we summarize three key findings from our study and discuss the implications for the future of US population health.
The first finding is that the degree of electoral democracy in US states, as measured by the SDI, was significantly associated with working‐age adult mortality rates in recent decades. Our models estimated that, if a state were to move from a moderate level of electoral democracy (defined as the third quintile of the SDI distribution) to a high level of electoral democracy (defined as the fifth quintile of the SDI distribution), working‐age mortality rates in that state would be 3.2% lower among men and 2.7% lower among women, net of time‐varying political party control, safety net policy generosity, union coverage, share of immigrants, and time‐invariant characteristics of the state. Our finding concurs with international studies of the association between democracy and various measures of population health. 21 , 22 , 23 , 24 It also corresponds with the only study to date that we are aware of that examined how US states’ democratic institutions predict mortality. 25 That study used two measures of democratic functioning (political accountability and checks and balances) during the 1999–2016 period and found that a higher degree of checks and balances, but not political accountability, predicted lower working‐age mortality, net of states’ policy liberalism and political party control.
Our second main finding is that improving states’ electoral democracy could potentially avert a sizable number of deaths among working‐age adults. Using a counterfactual approach, we estimated that increasing the SDI score in all states from the third to the fifth quintile of the SDI distribution might have resulted in 20,408 fewer deaths in 2019. To put this number in perspective, 20,410 working‐age adults died from cerebrovascular disease in 2019. 60 Other studies have also found the democracy–mortality association to be of a meaningful magnitude. In a study of 170 countries, democratic functioning was more important than gross domestic product per capita in predicting major causes of death such as cardiovascular disease. 21 How the effects of democratic functioning on working‐age mortality compare with those of other state policies is less clear. We can make imperfect comparisons to a study of state policy domains and working‐age mortality during 1999 to 2019. 5 Using a one‐year lag, it estimated the percent change in working‐age mortality in a state if it altered certain policy domains from a maximum conservative to maximum liberal configuration. Altering the criminal justice domain in this way predicted a 1.4% reduction in working‐age women's mortality, whereas altering the health and welfare domain predicted a 3.8% reduction. Altering other policy domains in this way predicted larger reductions in working‐age women's mortality (11.3% for labor, 13.3% for environment, 14.1% for economic taxes, and 23.1% for gun safety). We estimated that changing a state's SDI from lowest to highest quintile (which are not maxima) was associated with 3.6% lower mortality among women.
Our third finding offers insights into potential explanations for the association between electoral democracy and working‐age mortality. Some insights derive from our analyses of specific causes of death. Increases in electoral democracy were associated with the largest declines in deaths from drug poisoning and infectious diseases. If a state were to increase their SDI score from the third to the fifth quintile, our models estimated that, over the next year, 1) drug poisoning mortality would be 13.4% lower among men and 11.7% lower among women and 2) infectious disease mortality would be 13.1% lower among men and 11.3% lower among women. Homicide mortality would be an estimated 9.5% lower among men and 8.7% lower among women. Electoral democracy also had a sizable association with suicide among women. In describing the aims of this study, we speculated that we would find weak associations between the SDI and mortality from the two chronic conditions (heart disease and cancer) given the one‐year lag in our models between the SDI and mortality. Our findings bear this out. We found no association among men, regardless of whether the models used no lag or a one‐year lag. We also found no association among women when we used no lag. With a one‐year lag, associations with heart disease and cancer emerged among women, but their importance paled in comparison with drug poisoning, infectious diseases, and homicides. The association with infectious diseases for women and men may be partly tied to drug use. Injection drug use elevates the risk of a host of life‐threatening infections such as viral hepatitis and bacteria that cause heart infections such as endocarditis. 61 Taken together, these findings suggest that electoral democracy has its strongest associations with deaths reflecting social disfunction and deleterious behaviors.
We derived similar insights about potential explanations from analyses of several economic, behavioral, and social factors that may contribute to the SDI–mortality association. The most important factor appeared to be social functioning, followed by health behaviors. More than one‐quarter of the SDI–mortality association (26.7% for men and 29.2% for women) was accounted for by the three indicators of social functioning included in our study—marriage, incarceration rates, and violent crime rates. Among those three indicators, violent crime appeared particularly important. These findings are novel because “the analysis of potential mediators is uncommon in this literature.” 24 Furthermore, to the best of our knowledge, social functioning has not been previously examined as a potential link between democracy and population health.
In fact, prior evidence finds robust linkages from democracy to violent crime and incarceration and from those factors to mortality. As noted in the introduction, democracy can affect violent crime (and hence incarceration) through myriad factors such as economic conditions, social and economic equality, crime deterrence, judicial systems, perceived legitimacy of the government, and respect for the law. 34 , 35 , 36 Indeed, international studies find that higher democratic functioning predicts lower rates of violent crime. 34 , 36 Crime and incarceration, in turn, have collateral consequences for the broader population. 37 , 38 , 39 , 40 , 41 For example, a study of county‐level incarceration rates over the 1987–2017 period found that rising incarceration rates increased county‐level mortality rates within one year, with the strongest effects on deaths from infectious disease, chronic lower respiratory disease, substance use, and suicide. 39 Explanations for incarceration's widespread impact on mortality include factors such as destruction of psychological and material well‐being, dissolution of social ties such as marriage, and infectious disease spread, 37 , 39 , 40 and explanations for violent crime's widespread impact encompass factors such as psychosocial distress, delays in seeking medical care, elevated blood pressure, and acute myocardial infarction. 41
Implications
Taken together, our findings shine a light on a critical yet understudied determinant of population health in the United States—democracy. The degree of erosion of democracy in general and electoral democracy in particular in the United States in recent decades is striking and unusual compared with most other high‐income countries. 9 In 2021, more than 150 scholars of US democracy signed a document imploring Congress to pass the Freedom to Vote Act and, if necessary, suspend the Senate filibuster so that a simple majority would be necessary to pass it. 10 The signatories warned that failure to pass it would “undermine the minimum condition for electoral democracy—free and fair elections—[and] have grave consequences not only for our democracy, but for political order, economic prosperity, and the national security of the United States as well.” To this list of grave consequences, our findings add premature death.
The diverging trends in electoral democracy across US states are also stunning. According to the Brennan Center for Justice, in 2021 alone, 11 states passed voting laws that were entirely restrictive, and 17 states passed laws that were entirely expansive. 62 It warned that free and fair elections increasingly depend on which state a person lives in and that this divergence will continue unless Congress acts. 62 Importantly, the fact that democratic backsliding has occurred predominately and most severely in certain states does not restrict its consequences to those states. On the contrary, it has profound national consequences. Extreme partisan gerrymandering and electoral policies designed to create obstacles to voting for marginalized citizens in some states also affects state elections for national offices and subverts democracy for the entire country. 6 , 63
Our findings underscore the role of governance as a determinant of population health. The role of democratic governance—in particular, its erosion—as a cause of the troubling trends in working‐age mortality in recent decades has largely been absent from scientific studies and the public narrative. 9 Yet, this is precisely what the historical record would predict. According to historians such as Szreter 64 , 65 and Colgrove, 66 real improvements in population health in the mid‐ to late 1800s in industrializing countries such as England came about largely because of increased voting power of the public and, partly as a consequence, the rise of government interventions such as sanitation and clean water systems to improve social conditions for everyone. The historical association between rising democratic functioning and declining mortality is the flip side of today's association between declining democratic functioning and rising mortality.
Lastly, our findings contribute to a growing body of research on the impact of US states on population health. Some of these studies document a growing role of states’ policy contexts on working‐age mortality and life expectancy, particularly for policies on labor, firearm safety, tobacco, the environment, and economic taxes. 4 , 5 A burgeoning area of research has shown how structural sexism at the state level (measured by indicators such as the percentage of legislative seats held by men) is harmful for women's and men's health. 67 Another growing area examines the health impacts of structural racism at the state level. For example, it has shown how racialized disenfranchisement in a state predicts a host of health outcomes such as depressive symptoms, functional limitations, and disability. 68 Collectively, these research areas have been systematically unpacking the myriad ways that states shape population health. Our study and that of Pacheco and LaCombe 25 expand this work by investigating the role of state‐level electoral democracy.
Limitations and Future Directions
Our study is not without limitations. Although it used two decades of data, included key state‐level time‐varying covariates, controlled for time‐invariant characteristics of states, and incorporated a lag between the democracy measure and mortality, the estimates represent associations, not causal effects, between electoral democracy and working‐age mortality. We did not include all possible state‐level time‐varying covariates. Our selection of covariates is aligned with recent empirical studies on the associations between US state democracy and mortality, 25 state policy contexts and mortality, 4 , 5 , 43 established conceptual frameworks, 1 , 16 , 17 , 19 and guidelines on selecting proper controls. 69 Confidence in our findings is bolstered by the existing literature on democracy and population health reviewed in the introduction. Like our findings, that (mostly international) literature reports robust, positive associations between democracy and population health.
Another consideration is the lag time between changes in electoral democracy and changes in a state's mortality. We estimated models using no lag and a one‐year lag. Given that the pathways between electoral democracy and mortality are likely be myriad, indirect, and take time to fully materialize, it is possible that the longer‐term association is stronger than that estimated from our models. Like our findings, other studies report that changes in a country's democratic functioning predict rapid changes in population health. A study on how changes in countries’ electoral democracy predicted changes in mortality and life expectancy found that “the improvement in adult health after the transition to democracy is immediate” and grows over time. 21 Similarly, another study found that the first year a country converted to democratic rule resulted in a two‐year increase in life expectancy and 12.7% decrease in infant mortality, and those effects grew over time. 24 With a longer time horizon, the impact of democracy on mortality may spread to more causes of death.
More research on how US state democratic functioning affects population health is needed. The measure of electoral democracy that we used may be more or less salient for mortality across different demographic groups and stages of the life span. Lastly, the magnitude of the estimated associations between electoral democracy and mortality could be conservative because of interstate migration, 70 , 71 so future studies could potentially merge the SDI with a survey data set containing information on respondents’ interstate migration. However, the downside of a survey data set is potentially insufficient statistical power and representation across the 50 states. Although we cannot rule out an effect of interstate migration, we note that prior work has concluded that changes in states’ population composition in terms of average education levels and income did not explain trends in working‐age mortality in recent decades. 3
Conclusions
The erosion of electoral democracy is a significant threat to population health. Although the erosion has not occurred in every US state, it nevertheless has deleterious consequences for the country overall. Electoral democracy may be a fundamental determinant of health. It affects the distribution of political power, accountability of lawmakers to constituents, policy decisions, policing, distribution of economic resources, and more. Democratic erosion may be the “cause of the cause of the cause” 72 of rising mortality and declining life expectancy in the United States.
Acknowledgments: This project was supported by R01AG055481 (PI: Montez) from the National Institute on Aging. The content is solely the responsibility of the authors and does not necessarily represent the views of the National Institute on Aging or National Institutes of Health. We are grateful to Hugo Jales for expert guidance on our modeling strategy. We thank three anonymous reviewers for insightful comments on earlier versions of the manuscript.
Supporting information
Online Appendix
References
- 1. National Academies of Sciences, Engineering, and Medicine . High and Rising Mortality Rates Among Working‐Age Adults. The National Academies Press; 2021. [PubMed] [Google Scholar]
- 2. Woolf SH, Schoomaker H. Life expectancy and mortality rates in the United States, 1959–2017. JAMA. 2019;322(20):1996‐2016. 10.1001/jama.2019.16932 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Couillard BK, Foote CL, Gandhi K, Meara E, Skinner J. Rising geographic disparities in US mortality. J Econ Perspect. 2021;35(4):1‐27. 10.1257/jep.35.4.123 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Montez JK, Beckfield J, Cooney JK, et al. US state policies, politics, and life expectancy. Milbank Q. 2020;28(3):668‐699. 10.1111/1468-0009.12469 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Montez JK, Mehri N, Monnat SM, et al. US state policy contexts and mortality of working‐age adults. PLoS ONE. 2022;17(10):e0275466. 10.1371/journal.pone.0275466 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Grumbach JM. Laboratories Against Democracy: How National Parties Transformed State Politics. Princeton University Press; 2022. [Google Scholar]
- 7. Grumbach JM. Laboratories of democratic backsliding. Amer Polit Sci Rev. Published online December 1, 2022. 10.1017/S0003055422000934 [DOI] [Google Scholar]
- 8. Levitsky S, Ziblatt D. How Democracies Die. Broadway Books; 2018. [Google Scholar]
- 9. Willison CE, Falkenbach M, Greer SL, Singer PM. Backsliding among indicators of democratic stability relevant to public health: risks in OECD nations. World Med Health Policy . Published online December 25, 2022. 10.1002/wmh3.558 [DOI]
- 10. Statement in Support of the Freedom to Vote Act . New America. November 21, 2021. Accessed December 31, 2022. https://www.newamerica.org/political‐reform/statements/statement‐in‐support‐of‐the‐freedom‐to‐vote‐act/
- 11. Berger M. U.S. listed as a ‘backsliding’ democracy for first time in report by European think tank. The Washington Post . November 22, 2021. Accessed December 27, 2022. https://www.washingtonpost.com/world/2021/11/22/united‐states‐backsliding‐democracies‐list‐first‐time/
- 12. Bouie J. The U.S. thinks ‘it can't happen here.’ It already has. New York Times . October 18, 2022. Accessed May 1, 2023. https://www.nytimes.com/2022/10/18/opinion/democracy‐america‐authoritarianism‐midterms.html
- 13. Haggard S, Kaufman R. Backsliding. Democratic Regress in the Contemporary World. Cambridge University Press; 2021. [Google Scholar]
- 14. Wise M, Sainsbury P. Democracy: the forgotten determinant of mental health. Health Promot J Austr. 2007;18:177‐183. 10.1071/he07177 [DOI] [PubMed] [Google Scholar]
- 15. Brady D, Sosnaud B. The politics of economic inequality. In: Leicht KT, Jenkins JC, eds. Handbook of Politics: State and Society in Global Perspective. Springer; 2010:521‐541. [Google Scholar]
- 16. Reynolds MM. Health power resources theory: a relational approach to the study of health inequalities. J Health Soc Behav. 2021;62(4):493‐511. 10.1177/00221465211025963 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Navarro V, Muntaner C, Borrell C, et al. Politics and health outcomes. Lancet. 2006;368:1033‐1037. 10.1016/S0140-6736(06)69341-0 [DOI] [PubMed] [Google Scholar]
- 18. Muntaner C, Borrell C, Ng E, et al. Politics, welfare regimes, and population health: controversies and evidence. Sociol Health Illn. 2011;33(6):946‐964. 10.1111/j.1467-9566.2011.01339.x [DOI] [PubMed] [Google Scholar]
- 19. Navarro V, Shi L. The political context of social inequalities and health. Soc Sci Med. 2001;52(3):481‐491. 10.1016/s0277-9536(00)00197-0 [DOI] [PubMed] [Google Scholar]
- 20. Patterson AC. Not all built the same? A comparative study of electoral systems and population health. Health Place. 2017;47:90‐99. 10.1016/j.healthplace.2017.07.003 [DOI] [PubMed] [Google Scholar]
- 21. Bollyky TJ, Templin T, Cohen M, Schoder D, Dieleman JL, Wigley S. The relationships between democratic experience, adult health, and cause‐specific mortality in 170 countries between 1980 and 2016: an observational analysis. Lancet. 2019;393(10181):1628‐1640. 10.1016/S0140-6736(19)30235-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Jain V, Clarke J, Beaney T. Association between democratic governance and excess mortality during the COVID‐19 pandemic: an observational study. J Epidemiol Community Health. 2022;76(10):863‐860. 10.1136/jech-2022-218920 [DOI] [PubMed] [Google Scholar]
- 23. Lührmann A, Maerz SF, Grahn S, et al. Autocratization Surges ‐ Resistance Grows. Varieties of Democracy Institute. 2020. Accessed November 12, 2022. https://www.v‐dem.net/publications/democracy‐reports/
- 24. Patterson AC, Veenstra G. Politics and population health: testing the impact of electoral democracy. Health Place. 2016;40:66‐75. 10.1016/j.healthplace.2016.04.011 [DOI] [PubMed] [Google Scholar]
- 25. Pacheco J, LaCombe S. The link between democratic institutions and population health in the American states. J Health Polit Policy Law. 2022;47(5):527‐554. 10.1215/03616878-9978103 [DOI] [PubMed] [Google Scholar]
- 26. Klomp J, de Haan J. Is the political system really related to health? Soc Sci Med. 2009;69(1):36‐46. 10.1016/j.socscimed.2009.03.033 [DOI] [PubMed] [Google Scholar]
- 27. Briffault R. The challenge of the new preemption. Stanford Law Rev. 2018;70:1995‐2027. [Google Scholar]
- 28. Coombs E, Theobald N, Allison A, et al. Explaining the positive relationship between state‐level paid family leave and mental health. Community Work Fam . Published online November 11, 2022. 10.1080/13668803.13662022.12140029 [DOI]
- 29. Wolf DA, Montez JK, Monnat SM. U.S. state preemption laws and working‐age mortality. Am J Prev Med. 2022;63(5):681‐688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Montanaro D. Poll: more Americans are concerned about voting access than fraud prevention. NPR. July 2, 2021. Accessed March 23, 2023. https://www.npr.org/2021/07/02/1012302107/poll‐more‐americans‐are‐concerned‐about‐voting‐access‐than‐fraud‐prevention
- 31. American Psychological Association . Stress in America 2022 . 2022. Accessed March 22, 2023. https://www.apa.org/news/press/releases/stress/2022/concerned‐future‐inflation
- 32. Frey BS, Stutzer A. Happiness, economy and institutions. Econ J. 2000;110(466):918‐938. 10.1111/1468-0297.00570 [DOI] [Google Scholar]
- 33. Frey BS, Stutzer A. Happiness prospers in democracy. J Happiness Stud. 2000;1:79‐102. 10.1023/A:1010028211269 [DOI] [Google Scholar]
- 34. Lin M‐J. Does democracy increase crime? The evidence from international data. J Comp Econ. 2007;35(3):467‐483. 10.1016/j.jce.2007.06.001 [DOI] [Google Scholar]
- 35. Nivette A. Legitimacy and crime: theorizing the role of the state in cross‐national criminological theory. Theor Criminol. 2014;18(1):93‐111. 10.1177/1362480613499793 [DOI] [Google Scholar]
- 36. Stamatel J. Democratic cultural values as predictors of cross‐national homicide variation in Europe. Homicide Stud. 2016;20(3):239‐256. 10.1177/1088767915611178 [DOI] [Google Scholar]
- 37. Hatzenbuehler ML, Keyes K, Hamilton A, Uddin M, Galea S. The collateral damage of mass incarceration: risk of psychiatric morbidity among nonincarcerated residents of 0high‐incarceration neighborhoods. Am J Public Health. 2015;105(1):138‐143. 10.2105/AJPH.2014.302184 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Chesney‐Lind M, Mauer M, eds. Invisible Punishment: The Collateral Consequences of Mass Imprisonment. The New Press; 2003. [Google Scholar]
- 39. Kajeepeta S, Mauro PM, Keyes KM, El‐Sayed AM, Rutherford CG, Prins SJ. Association between county jail incarceration and cause‐specific county mortality in the USA, 1987–2017: a retrospective, longitudinal study. Lancet Public Health. 2021;6(4):e240‐e248. 10.1016/S2468-2667(20)30283-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Kajeepeta S, Rutherford CG, Keyes KM, El‐Sayed AM, Prins SJ. County jail incarceration rates and county mortality rates in the United States, 1987–2016. Am J Public Health. 2020;110(S1):S109‐S115. 10.2105/AJPH.2019.305413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Eberly LA, Julien H, South EC, et al. Violent crime and cardiovascular mortality in Chicago: a longitudinal analysis. J Amer Heart Assoc. 2022;11(14):e025168. 10.1161/JAHA.122.025168 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Quinn KM. Bayesian factor analysis for mixed ordinal and continuous responses. Polit Anal. 2004;12(4):338‐353. 10.1093/pan/mph022 [DOI] [Google Scholar]
- 43. Fenelon A, Witko C. Emerging political and demographic divides: state politics, welfare generosity, and adult mortality in U.S. states 1977–2017. Health Place. 2021;71:106244. 10.1016/j.healthplace.2021.102644 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Rodriguez JM, Bound J, Geronimus AT. US infant mortality and the president's party. Int J Epidemiol. 2014;43(3):818‐826. 10.1093/ije/dyt252 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. University of Kentucky Center for Poverty Research . UKCPR national welfare data, 1980–2019. 2021. Accessed March 15, 2022. http://ukcpr.org/resources/national‐welfare‐data
- 46. Pierson K, Hand ML, Thompson F. The Government Finance Database: a common resource for quantitative research in public financial analysis. PLoS One. 2015;10(6):e0130119. 10.1371/journal.pone.0130119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Grumbach JM. From backwaters to major policymakers: policy polarization in the states, 1970–2014. Perspect Politics. 2018;16(2):416‐435. 10.1017/S153759271700425X [DOI] [Google Scholar]
- 48. Caughey D, Warshaw C. The dynamics of state policy liberalism, 1936–2014. Am J Pol Sci. 2016;60(4):899‐913. 10.1111/ajps.12219 [DOI] [Google Scholar]
- 49. Hirsch BT, Macpherson DA, Even W. Union membership and coverage database. 2023. Accessed March 29, 2023. https://unionstats.com/
- 50. Hirsch BT, Macpherson DA. Union membership and coverage database from the Current Population Survey: note. Ind Labor Relat Rev. 2003;56(2):349‐354. 10.2307/3590942 [DOI] [Google Scholar]
- 51. US Census Bureau . Median Household Income by State (Table H‐8) . 2022. Accessed April 8, 2023. https://www.census.gov/data/tables/time‐series/demo/income‐poverty/historical‐income‐households.html.
- 52. Slater ME, Alpert HR. Apparent per capita alcohol consumption: national, state, and regional trends, 1977–2019. National Institute on Alcohol Abuse and Alcoholism. 2021. Accessed October 1, 2022. https://pubs.niaaa.nih.gov/publications/surveillance117/SR‐117‐Per‐Capita‐Consumption.pdf [Google Scholar]
- 53. Watson NF, Badr MS, Belenky G, et al. Recommended amount of sleep for a healthy adult: a joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep. 2015;38(6):843‐844. 10.5665/sleep.4716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. National Corrections Reporting Program Serie s. National Corrections Reporting Program, 1991–2019: Selected Variables . 2021. Accessed September 18, 2022. https://www.icpsr.umich.edu/web/NACJD/studies/38048
- 55. Federal Bureau of Investigation Crime Data Explorer. 2022. Accessed September 20, 2022. https://www.cde.ucr.cjis.gov/LATEST/webapp/#/pages/home
- 56. de Chaisemartin C, D'Haultfoeuille X. Two‐way fixed effects and difference‐in‐differences with heterogeneous treatment effects: a survey. Econom J. Published online June 8, 2022. 10.1093/ectj/utac017 [DOI] [Google Scholar]
- 57. Baltagi BH. The two‐way Mundlak estimator. Econom Rev. 2023;42(2):240‐246. 10.1080/07474938.2023.2178139 [DOI] [Google Scholar]
- 58. Mundlak Y. On the pooling of time series and cross section data. Econometrica. 1978;46(1):69‐85. [Google Scholar]
- 59. Wooldridge JM. Two‐way fixed effects, the two‐way Mundlak regression, and difference‐in‐difference estimators. 2021. Accessed March 28. https://www.researchgate.net/publication/353938385_Two‐Way_Fixed_Effects_the_Two‐Way_Mundlak_Regression_and_Difference‐in‐Differences_Estimators
- 60. CDC WONDER . Centers for Disease Control and Prevention. Accessed December 3, 2022. https://wonder.cdc.gov/
- 61. Levitt A, Mermin J, Jones CM, See I, Butler JC. Infectious diseases and injection drug use: public health burden and response. J Infect Dis. 2020;222(Suppl 5):S213‐217. 10.1093/infdis/jiaa432 [DOI] [PubMed] [Google Scholar]
- 62. Brennan Center for Justice . Voting laws roundup: December 2021. 2022. Accessed March 23, 2022. https://www.brennancenter.org/our‐work/research‐reports/voting‐laws‐roundup‐december‐2021
- 63. Rocco P. Laboratories of what? American federalism and the politics of democratic subversion. In: Lieberman RC, Mettler S, Roberts KM, eds. Democratic Resilience: Can the United States Withstand Rising Polarization? Cambridge University Press; 2021:297‐319. [Google Scholar]
- 64. Szreter S. The population health approach in historical perspective. Am J Public Health. 2003;93(3):421‐431. 10.2105/ajph.93.3.421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Szreter S. Rethinking McKeown: the relationship between public health and social change. Am J Public Health. 2002;92(5):722‐725. 10.2105/ajph.92.5.722 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Colgrove J. The McKeown thesis: a historical controversy and its enduring influence. Am J Public Health. 2002;92(5):725‐729. 10.2105/ajph.92.5.725 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Homan P. Structural sexism and health in the United States: a new perspective on health inequality and the gender system. Am Sociol Rev. 2019;84(3):486‐516. 10.1177/0003122419848723 [DOI] [Google Scholar]
- 68. Homan PA, Brown TH. Sick and tired of being excluded: structural racism in disenfranchisement as a threat to population health equity. Health Aff (Millwood). 2022;41(2):219‐227. 10.1377/hlthaff.2021.01414 [DOI] [PubMed] [Google Scholar]
- 69. Cinelli C, Forney A, Pearl J. A crash course in good and bad controls. Sociol Methods Res. Published online May 20, 2022. 10.1177/00491241221099552 [DOI] [Google Scholar]
- 70. Montez JK, Zajacova A, Hayward MD, Woolf S, Chapman D, Beckfield J. Educational disparities in adult mortality across U.S. states: how do they differ and have they changed since the mid‐1980s? Demography. 2019;56(2):621‐644. 10.1007/s13524-018-0750-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Xu W, Engelman M, Palloni A, Fletcher J. Where and when: sharpening the lens on geographic disparities in mortality. SSM Popul Health. 2020;12:100680. 10.1016/j.ssmph.2020.100680 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Bambra C, Smith KE, Pearce J. Scaling up: the politics of health and place. Soc Sci Med. 2019;232:36‐42. 10.1016/j.socscimed.2019.04.036 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Online Appendix