

Introduction
The term hallux valgus (HV) was introduced by Carl Hueter to define a static subluxation of the first metatarsophalangeal (MTP) joint characterized by lateral deviation of the great toe and medial deviation of the first metatarsal. 3 Over time, it has been understood that HV is a multidimensional foot disorder that includes deformities in 3 planes: frontal, transverse, and sagittal, with up to 87% of valgus cases presenting with a pronated first metatarsal bone. 5
Some studies have focused on the complexity of the hallux valgus deformity, particularly on the pronation of the first metatarsal and its risk of recurrence. A systematic review revealed that the postoperative sesamoid position is a crucial factor that contributes significantly to HV recurrence. 1 This finding emphasizes the importance of proper rotation correction during the surgical treatment of HV to achieve long-term success.
In recent years, there has been a significant increase in the number of publications on the topic of hallux valgus correction, with a particular focus on the development of percutaneous techniques. 8 This growth in minimally invasive techniques reflects the better patient experience in the correction of hallux valgus, with less scarring and, mainly, less perioperative pain, as demonstrated by a recent published systematic review. 2
Therefore, focusing on multiplanar correction, the Metaphyseal Extra-Articular Transverse and Akin Osteotomies (META) technique has been developed. This technique is considered a fourth generation of minimally invasive surgical technique used for correcting hallux valgus deformity. 7
The method entails correcting a multiplanar rotational deformity by manipulating an extra-articular distal first metatarsal osteotomy, which is then stabilized using 2 screws for rigid fixation. In this study, which had a minimum follow-up period of 12 months, it was found that the META technique significantly improved clinical and radiographic outcomes in 50 feet with hallux valgus deformity. 7
The objective of our article is to provide a technical tip for correcting excessive first metatarsal pronation in hallux valgus during the execution of the META procedure in cases with moderate or severe hallux valgus deformity.
Description of Technique
The procedure is typically performed with the patient in a supine position, under first-ray field block or ankle peripheral nerve block with sedation and without the use of a tourniquet. The foot is positioned at the end of the table to facilitate obtaining intraoperative radiographs.
The surgical steps are as follows (Figure 1):
Figure 1.
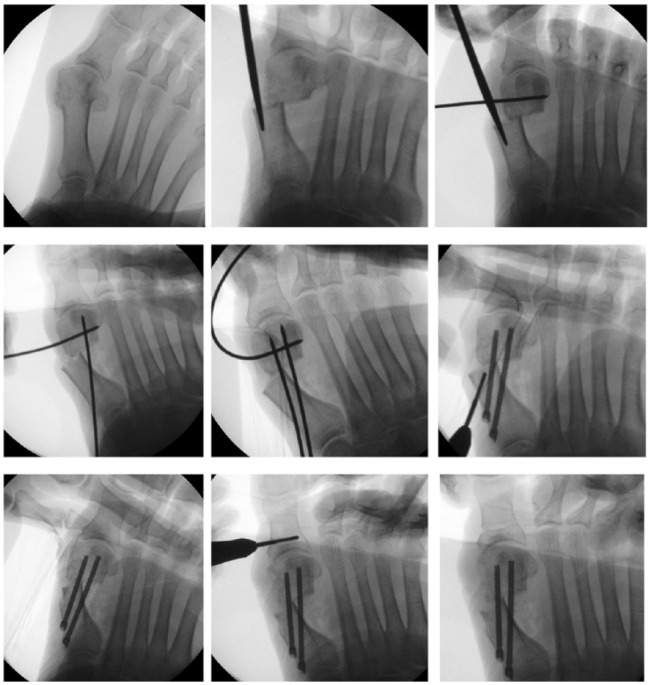
Intraoperative radioscopy image.
Perform the osteotomy using a transverse cut in the coronal plane as previously described according to the META procedure. 7
Pull the hallux while performing internal rotation of the toe, use an intramedullary reduction tool such as a mosquito clamp or periosteal elevator to shift the first metatarsal head lateral relative to the shaft, closer to the second metatarsal. It simultaneously will tension the first tarsometatarsal (TMT) joint in varus.
If the above maneuvers are not sufficient to position the metatarsal head over the sesamoids, with persistent sesamoid subluxation, the metatarsal is likely presenting with ongoing moderate or severe pronation.
In this case, place a 2-mm K-wire through the metatarsal head in the midline in medial to lateral angulation of around 30 degrees from plantar to dorsal and rotate it dorsally supinating the head. The correction of the rotation can be evaluated with fluoroscopy, by absence of sesamoid subluxation and presence of straight angle on the lateral aspect of the metatarsal head and using clinical parameters like the toenail orientation (Figure 2).
Place 2 additional 2-mm K-wires to stabilize the osteotomy.
Remove the 2-mm k-wires (one at a time) and insert 2 chamfered screws, keeping the instrument that is pushing the head and the 2-mm K-wire controlling the rotation.
Remove the 2.0-mm K-wire that was controlling the rotation and remove the medial prominence.
If needed, perform an Akin osteotomy percutaneously.
Figure 2.

Intraoperative clinical position.
Discussion
The pronation of the first metatarsal is increasingly being studied in relation to hallux valgus deformity and surgical corrections. Studies have found that patients with hallux valgus exhibit a greater degree of first metatarsal pronation compared to control patients. 6
Correcting the pronation of the first metatarsal is essential for achieving long-term success in hallux valgus surgery. Failure to address this issue can lead to recurrence of the deformity and dissatisfaction among patients. 4 Therefore, surgeons must be aware of the importance of correcting the pronation during the surgical procedure.
This rationale was also applied to minimally invasive techniques, such as the fourth-generation Metaphyseal Extra-Articular Transverse and Akin Osteotomy (META) technique, in which a percutaneous transverse osteotomy of the metatarsal neck is performed to correct rotation, and fixation is achieved using chamfered screws. 7
However, it has been observed that in some cases, particularly in moderate to severe cases, rotation correction is incomplete when manually rotating the hallux. Therefore, a technical tip has been proposed to correct this pronation as effectively as possible.
The use of the Kirschner wire technique for correcting pronation is simple, inexpensive, and easily reproducible. This technique is particularly useful in moderate to severe cases where correction of rotation is not possible through manual manipulation alone. Moreover, the control of the rotation can be seen in static and video fluoroscopy during the procedure, further highlighting its efficacy.
After correcting the pronation, fixation should be performed in the same manner as described in the META technique. During the fixation of the osteotomy with screws, there is a risk of partial loss of the pronation correction. Therefore, it is important that the Kirschner wire placed in the head of the first metatarsal must be kept in its corrected position until the end of the procedure to prevent any type of loss during screw placement.
The simplicity and cost-effectiveness of the Kirschner wire technique make it an attractive option for surgeons, and its usefulness in moderate to severe cases provides a wider range of treatment options for patients.
Conclusion
The correction of first metatarsal pronation is a crucial step in the surgical correction of hallux valgus deformity. The Kirschner wire technique is a simple, inexpensive, and easily reproducible method for correcting pronation in severe hallux valgus deformity cases.
Supplemental Material
Supplemental material, sj-pdf-1-fao-10.1177_24730114231198527 for Correction of First Metatarsal Pronation in Metaphyseal Extra-articular Transverse Osteotomy for Hallux Valgus Correction by Gabriel Ferraz Ferreira, Gustavo Araujo Nunes, Davy Sevilla Dorado, Mauro Cesar Mattos e Dinato, Thomas Lorchan Lewis, Robbie Ray and Miguel Viana Pereira Filho in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval: Ethical approval was not sought for the present study because it is a technique tip.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs: Gabriel Ferraz Ferreira, MD, MSc,  https://orcid.org/0000-0001-8032-3077
https://orcid.org/0000-0001-8032-3077
Gustavo Araujo Nunes, MD,
https://orcid.org/0000-0003-4431-5576
Thomas Lorchan Lewis, MBChB(Hons), BSc(Hons), MRCS,
https://orcid.org/0000-0002-4167-7427
Robbie Ray, MBChB, ChM(T&O), FRCS(T&O), FEBOT,
https://orcid.org/0000-0002-7411-9720
Miguel Viana Pereira Filho, MD, MSc,
https://orcid.org/0000-0002-2320-9769
References
- 1. Ezzatvar Y, Lopez-Bueno L, Fuentes-Aparicio L, Duenas L. Prevalence and predisposing factors for recurrence after hallux valgus surgery: a systematic review and meta-analysis. J Clin Med. 2021;10(24):5753. doi: 10.3390/jcm10245753 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Ferreira GF, Borges VQ, Moraes LVM, Stefani KC. Percutaneous chevron/akin (PECA) versus open scarf/akin (SA) osteotomy treatment for hallux valgus: a systematic review and meta-analysis. PLoS One. 2021;16(2):e0242496. doi: 10.1371/journal.pone.0242496 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Hueter C. Klinik der Gelenkkrankheiten mit Einschluss der Orthopadie. Vogel. 1871. [Google Scholar]
- 4. Kaufmann G, Sinz S, Giesinger JM, Braito M, Biedermann R, Dammerer D. Loss of correction after chevron osteotomy for hallux valgus as a function of preoperative deformity. Foot Ankle Int. 2019;40(3):287-296. doi: 10.1177/1071100718807699 [DOI] [PubMed] [Google Scholar]
- 5. Kim Y, Kim JS, Young KW, Naraghi R, Cho HK, Lee SY. A new measure of tibial sesamoid position in hallux valgus in relation to the coronal rotation of the first metatarsal in CT scans. Foot Ankle Int. 2015;36(8):944-952. doi: 10.1177/1071100715576994 [DOI] [PubMed] [Google Scholar]
- 6. Kimura T, Kubota M, Taguchi T, Suzuki N, Hattori A, Marumo K. Evaluation of first-ray mobility in patients with hallux valgus using weight-bearing CT and a 3-D analysis system: a comparison with normal feet. J Bone Joint Surg Am. 2017;99(3):247-255. doi: 10.2106/JBJS.16.00542 [DOI] [PubMed] [Google Scholar]
- 7. Lewis TL, Lau B, Alkhalfan Y, et al. Fourth-generation minimally invasive hallux valgus surgery with metaphyseal extra-articular transverse and akin osteotomy (META): 12 month clinical and radiologic results. Foot Ankle Int. 2023;44(3):178-191. doi: 10.1177/10711007231152491 [DOI] [PubMed] [Google Scholar]
- 8. Lewis TL, Ray R, Robinson P, et al. Percutaneous chevron and akin (PECA) osteotomies for severe hallux valgus deformity with mean 3-year follow-up. Foot Ankle Int. 2021;42(10):1231-1240. doi: 10.1177/10711007211008498 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-pdf-1-fao-10.1177_24730114231198527 for Correction of First Metatarsal Pronation in Metaphyseal Extra-articular Transverse Osteotomy for Hallux Valgus Correction by Gabriel Ferraz Ferreira, Gustavo Araujo Nunes, Davy Sevilla Dorado, Mauro Cesar Mattos e Dinato, Thomas Lorchan Lewis, Robbie Ray and Miguel Viana Pereira Filho in Foot & Ankle Orthopaedics