

Abstract
This paper sets out to discover more about the name ‘Tarrant’ whose ophthalmic paintings have regularly featured in ophthalmic textbooks over the past 50 years. Through a series of telephone calls, I have spoken to Tarrant about his life and work while I research the origins of ophthalmic illustrations charting the story behind this art movement. The paper also explores the eventual decline of retinal painting and the emergence of photography, concluding that due to the continuing advance of technology the ophthalmic photographer may eventually succumb to the same fate as the artist.
Subject terms: Education, Health occupations
Introduction
When Albrecht von Graefe first examined the eye using Hermann von Helmholtz’s ophthalmoscope he exclaimed ‘Helmholtz has discovered for us a new world’. The early explorers of this new world documented the retinal landscapes, unlocking its secrets equipped with a paintbrush and an ophthalmoscope. My interest in paintings of the retina began while working with John Salmon on the tenth edition of Kanski’s Clinical Ophthalmology. As well as the conventional ophthalmic photographs and scans, this latest edition contains 33 paintings of the retina. These feature a single name, Tarrant, in the bottom corner of the paintings. As I later discovered, this name is widely known throughout the field of ophthalmology and his work is highly revered. I was curious to find out more about the artists involved in this movement, its history, and specifically the paintings and the person behind the name.
For the purpose of this paper, I have viewed Tarrant’s original paintings at the Institute of Ophthalmology and met Richard Keeler, Honorary Archivist for the Moorfields (Alumni) Association located in the joint library at the Institute of Ophthalmology. I have been in contact with Judith Wright, Senior Archivist at Boots UK, and discovered the story behind the drawing department at Theodore Hamblin where Tarrant began his career. With the assistance of the archives team at the Wellcome Collection I discovered seminal retinal paintings in numerous ophthalmic atlases that are held in their collection, uncovering the paintings that first illustrated this new unexplored world.
I am grateful for the assistance from all the departments mentioned above, most notably Richard Keeler and Wendy Franks, whose knowledge of the history of ophthalmic artists and ophthalmology has been invaluable. I have been fortunate to speak to the artist, Mr Tarrant, on many occasions and talk to him about his life and discover how he became arguably the most prolific and well-known of ophthalmic artists.
Terence R. Tarrant1
Terence R. Tarrant was born in 1930 in Kings College Hospital, London, and was brought up in Newington Causeway close to the Elephant and Castle. His father worked as a station master for the London Underground and was also a gifted artist, creating paintings using oil and watercolour. In his spare time he used these artistic skills to generate extra income as a sign writer for local shops and businesses. It was evident at an early age that Tarrant had inherited his father’s artistic abilities as he showed a proficiency for drawing. When he left school in 1944 he hoped to find a job where he could utilise his artistry. He was specifically interested in creating illustrations for the Metal Box Company. Hand painted tins were highly popular at this time and many homes had large collections. After an unsuccessful visit to the labour exchange (the forerunner of the modern jobcentre) with his father he focused his attention away from the arts to his other interest which was optics. As a young child Tarrant was fascinated with microscopes and optics in general and would construct rudimentary telescopes out of cardboard. Accompanied by his father, Tarrant returned to the labour exchange and found a vacancy at Theodore Hamblin Ltd, Dispensing Opticians, located at 15 Wigmore Street, London.
Theodore Hamblin
Henry Thomas Hamblin founded Theodore Hamblin an affluent optician and optical instrument maker whose patrons included the royal family. Tarrant successfully applied as an optical assistant in Theodore Hamblin’s factory at 28-32 Aybrook Street, close to Marylebone Lane. One lunchtime, while working at the factory he sustained a serious injury to his back. The following day Tarrant was unable to stand and a visiting physician suspected he might have polio and he was admitted to Mount Vernon hospital in Middlesex. During his stay his father brought him art materials where he occupied his time making copies of drawings from natural history books. He was discharged from hospital with a clean bill of health and the drawings he made while convalescing were brought to the attention of the managing director at Theodore Hamblin, Richard Smellie. Smellie was impressed with Tarrant’s artistic ability and he was called into the offices at Wigmore Street. On the strength of his drawings he was offered an apprenticeship as an ophthalmic draughtsman for £2 per week. Tarrant was thrilled to be offered a job that combined both drawing and optics and traded his khaki overcoat he wore in the factory for a white overcoat that was worn by the draughtsman. Tarrant described this as ‘moving up in the world’.
Painting the retina
The historical milestones of ophthalmic photography have been well documented. The first published in-vivo human retinal photographs taken in 1886 by Jackman and Webster and the first fundus fluorescein angiogram in 1961 have been cited in many papers. However, the history of ophthalmic artists is less well-known. External eye conditions have been documented in publications dating back from as early as Georg Bartisch’s Ophthalmodouleia. Published in 1583 the work contains a total of 92 woodcuts depicting eye disorders including ‘disease of the eye caused by witchcraft’ and ophthalmic surgical techniques. Another example illustrating conditions of the external eye is a 1675 compendium of medicines and surgery compiled for the use of the House of the Franciscan Order. Arzneibuch contains over one hundred pages that are devoted to ophthalmology with approximately 60 colour illustrations. Both books also include a fold-out section showing anatomical diagrams of the structures of the eye including the retina. Retinal disorders remained a mystery as they could not be visualised with dissection being the only way to examine the internal structures. It wasn’t until 1850 with the development of the ophthalmoscope that physicians were able to unlock its secrets and begin to understand the true causes of sight loss due to retinal disorders.
Exploring unknown worlds
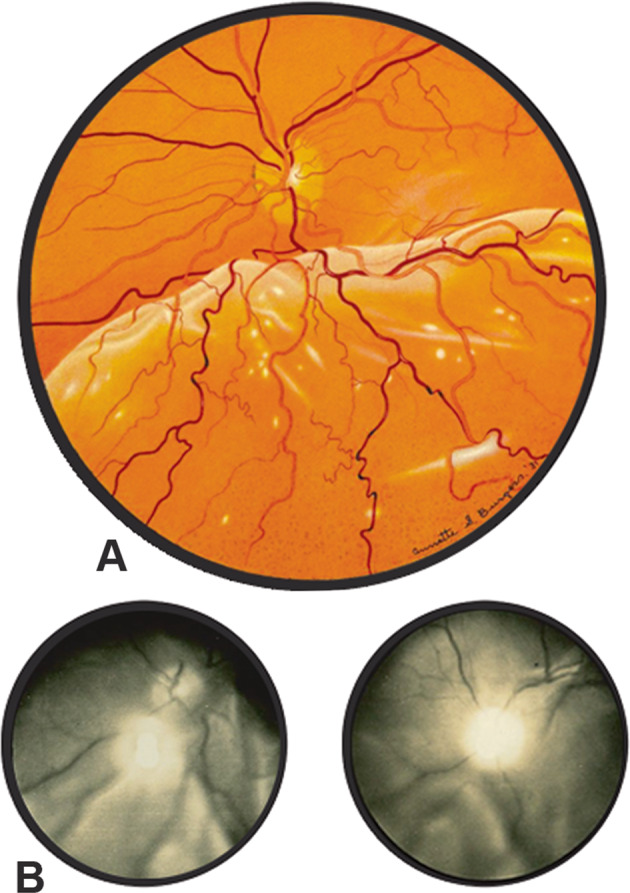
The invention of the ophthalmoscope by Hermann von Helmholtz in 1850 allowed these previously unseen worlds to be explored. The first published paintings of the retina from a living subject featured in a medical school dissertation by A.C. Van Trigt (Fig. 1A). Van Trigt came from an artistic family and was a notable painter. After his 1853 publication, paintings of the retina started to feature frequently alongside the descriptions in ophthalmology textbooks and atlases. The paintings in these early textbooks were mostly created by physicians due to their experience in using the ophthalmoscope. Richard Liebreich, who was Hermann von Helmholtz’s assistant and worked with him observing patient’s fundi on the original model of the ophthalmoscope published the first colour ophthalmic atlas in 1863. Liebreich was an incredibly skilled artist and his ‘Atlas der Ophthalmoscopie’ features 57 paintings of the retina (Fig. 1B). The founder of the Royal Eye Hospital in London, John Zachariah Laurence, described the images contained within the Atlas as “scrupulous copies of nature”. This atlas was shortly followed by Eduard von Jaeger’s ‘Ophthalmoskopischer Hand-Atlas’ in 1869. This publication contained 29 colour lithograph plates made directly from his original paintings (Fig. 1C). Jaeger reported that it took between 2 and 3 hours over the course of 20 to 40 sittings to examine the patient and produce these meticulous paintings. More than 50 ophthalmic atlases were published over the next 60 years each containing an increasing number of paintings depicting retinal disorders. Demand for paintings to be included in ophthalmic textbooks increased as did the ophthalmologist’s understanding of the many retinal conditions. Due to this demand and the time taken to examine the patient and produce the paintings it wasn’t long before artists were employed to document the retina replacing the role that was once restricted to physicians.
Fig. 1. Three examples of early retinal paintings.
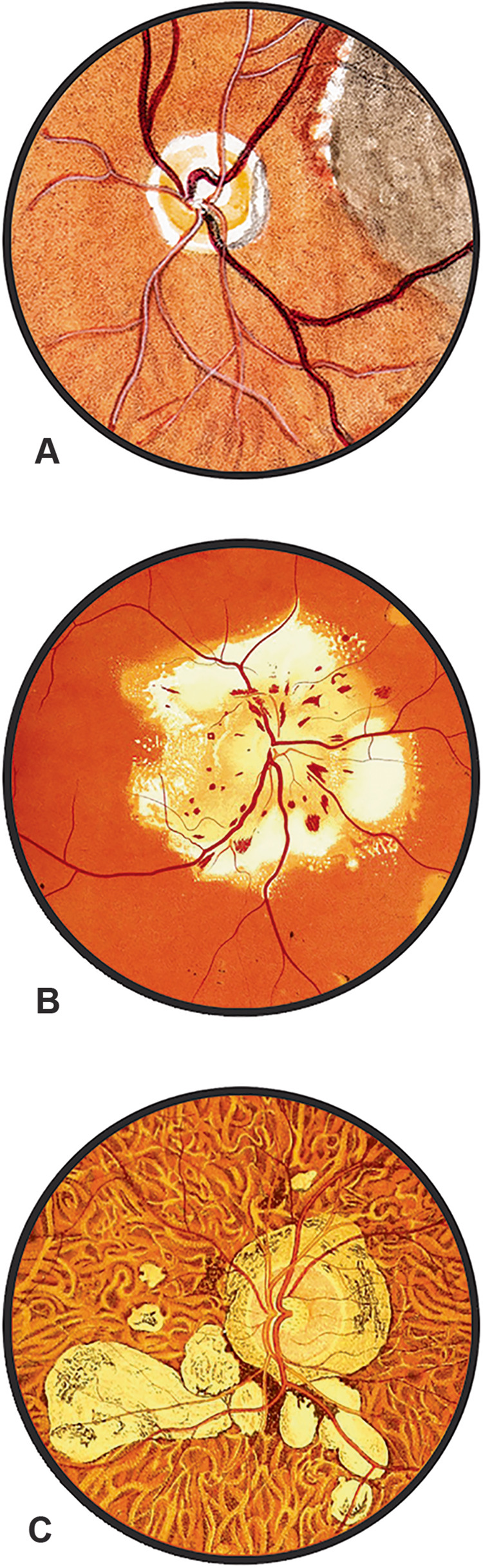
This shows the different approaches and styles present in early paintings of the retina., A A.C. Van Trigt (1853), B Richard Liebreich (1863), C Eduard von Jaeger (1869) (Images B and C courtesy of the Wellcome Collection).
The first ophthalmic artists
Charles Bader was a student of Sir William Bowman (ophthalmic surgeon at Moorfields) and was taught how to use an ophthalmoscope when Bowman acquired one in 1851. Bader employed the first ophthalmic artist at Moorfields (R. Schweizer) to make drawings of the retina under his supervision for his 1868 book ‘The Natural and Morbid Changes of the Human Eye’. When compared to Jaeger’s paintings which were published in the following year, Schweizer’s paintings are simplistic and show minimal detail (Fig. 2). This may be due to the limited size of his paintings (which were one and a quarter inch in diameter), his artistic ability, or his proficiency in examining the patient using an ophthalmoscope.
Fig. 2. Comparison showing the difference of artists ability.
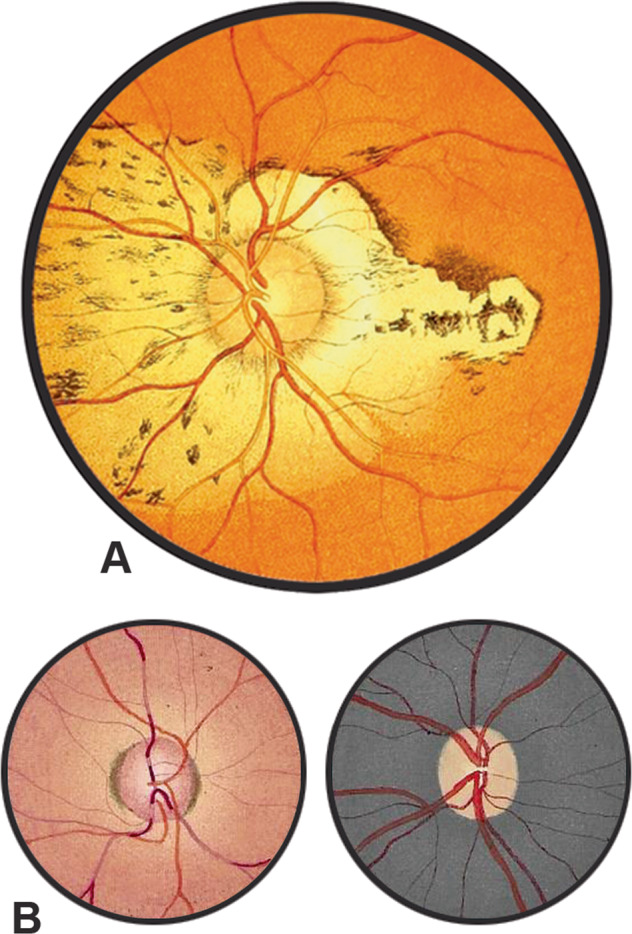
When compared, Jaeger’s painting (A) is more accomplished than Schweizer work (B). This may be due to artistic ability or their experience in using the ophthalmoscope. (Image A courtesy of the Wellcome Collection, image B courtesy of the Institute of Ophthalmology).
The employment of the first dedicated retina artist at Moorfields signifies a shift in the mindset of how the paintings were created as this was no longer the privilege of those with a medical background. Although some surgeons at Moorfields were continuing to produce paintings (William Spicer Holmes and Andrew Stanford Morton), it was mainly because they were accomplished artists (similar to Van Trigt). Edward Nettleship, who trained under Sir Jonathan Hutchinson at Moorfields, has an example of his work in the archives at the Institute of Ophthalmology. Nettleship’s painting (Fig. 3) is basic and devoid of detail, which may explain why he employed Alice and Mary Boole to produce drawings and paintings for the surgeons at Moorfields. It is believed that the artist John Nettleship (Edward’s brother), taught the Boole sisters how to paint and it would be reasonable to assume that Edward Nettleship taught them how to use an ophthalmoscope. Mary Boole mastered examining the patients using the ophthalmoscope and examples of her retinal paintings begin in 1883 in the ‘Transactions of Ophthalmological Society for the United Kingdom’ (TOSUK). Boole’s meticulous illustrations accompany the physician’s description in many subsequent volumes along with an ever-growing list of artists (for example, E. Burgess, A. Stone, A. Head). This suggests the employment of trained artists was both beneficial in the time taken to produce the paintings and the level of artistic quality that was required for publication.
Fig. 3. Example of an early painting highlighting the importance of employing artists.
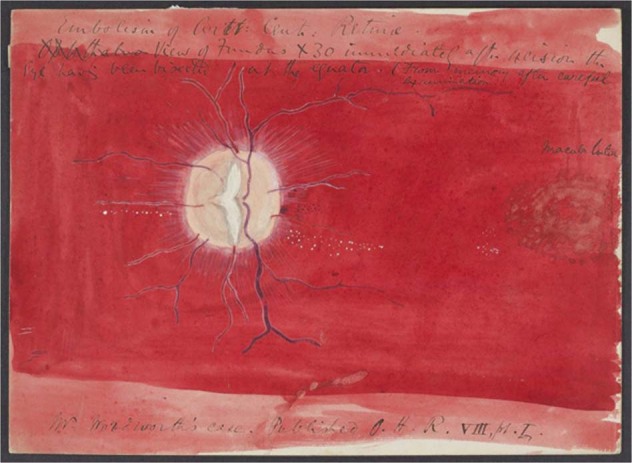
This example by Nettleship may illustrate why he employed the Boole sisters to produce work as it is very basic and below the standards of work that were published in this era (Image courtesy of the Institute of Ophthalmology).
Ophthalmologist and retinal artist William Wallace discusses the importance of the quality of the ophthalmic painting in an article that featured in the British Journal of Ophthalmology [1] ‘By this time the technique of drawing the fundus had advanced to a stage while it was clear that they must reach an assured standard if destined for publication’. Wallace continues ‘the year 1886 should have seen the publication of two books with plates far behind in the quality demanded by the Ophthalmological Society for its Transactions’.
Wallace describes the drawings in Loring’s ‘Textbook of Ophthalmology’ as ‘coarse’ and the colouring ‘weak’. When compared to work that features in TOSUK from the same year, Loring’s paintings appear simplistic, lacking artistic aptitude (Fig. 4). The desire to accurately replicate what was observed when examining the retina through the ophthalmoscope is evident in the evolution of the paintings produced in this era. Wallace states, ‘From this date draughtsmen of the fundus appear to have vied with one another in producing work which had to be accurate in order to lay a claim to possess permanent value.’ There is one artist from this era whose work achieved this, subsequently becoming a leading figure in this field due to the quality of his paintings and observational skills.
Fig. 4. These two examples were produced in 1886 and highlight the differences in standards of the paintings that were being produced.
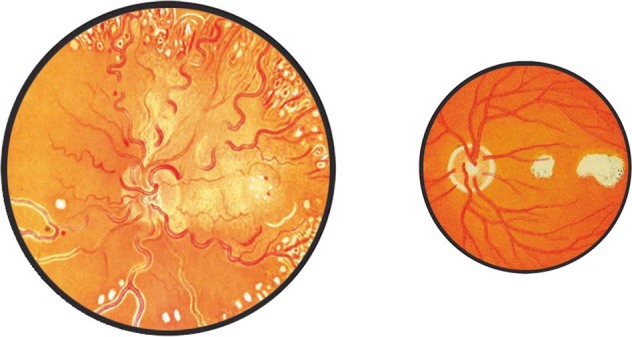
The painting on the left is by E. Burgess and the painting on the right is by Loring. (Image on the right courtesy of the Wellcome Collection).
Arthur Head
Arthur Head studied at the Slade school of Art and later became a landscape painter using oils and watercolour. There is no documented information as to how and why he started producing painting of the retina, but this may have been to earn extra income. In a letter from Richard Smellie, managing director of Theodore Hamblins (who later employed Head), it describes how the regular income of working as an ophthalmic artist allowed him to indulge in activates that he was unable to do in his earlier life suggesting Head struggled to make a living from selling his paintings. This was not uncommon for artists to undertake commissions to supplement their income. Tinus De Jough who later became a renowned artist also experienced financial difficulty during the early part of his career and was employed to produce ophthalmic paintings by David James Wood, the first ophthalmologist and first medical specialist in South Africa.
The earliest examples of Head’s work features in volume 8 of TOSUK which was published in 1888/9. Head was trained how to operate an ophthalmoscope by George Lindsay Johnson, Ophthalmic Surgeon at the Westminster Ophthalmic Hospital and went on to produce work for his publication ‘Extra-Papillary Coloboma’ in 1890. This is believed to be the first book that Head worked on producing 12 colour paintings of the retina documenting a variety of Colobomas. In 1896 Head collaborated with William Adams Frost on the publication ‘The Fundus Oculi’ and is acknowledged in the preface ‘I am greatly indebted to the artist, Mr A. W. Head, for the care and skill with which he has executed the drawings’. This Atlas features 107 colour retinal paintings by Head and shows a greater level of detail and luminescence when compared to early examples of his work (Fig. 5). Head went on to work with Lindsay Johnson on the 1901 publication ‘Contributions to the comparative anatomy of the mammalian eye’ where he produced 50 colour retinal paintings of animals ranging from the common squirrel to an African Elephant. Lindsay Johnson credits Head’s work in the preface‘ I was fortunate enough to obtain the assistance of that well-known artist and excellent draughtsman, Mr A.W. Head F.Z.S. It is entirely due to his talent that I have been able to obtain a great number of excellent and faithful drawings of the fundus oculi of most of most of the Mammals to be found in the menageries and zoological gardens of Europe’. In an article by Marcus Woodward in the 1902 December edition of Pearson’s [2] Head’s accounts of working on Lindsay Johnson’s book is described along with how he began painting the retina of animals starting with a visiting terrier. While teaching ophthalmoscopic drawing to a student who was accompanied by their dog, Head picked up the animal and examined it, making a quick sketch of the retina. He was so pleased with the result that he took the painting to Lindsay Johnson who immediately asked for more examples. It is thought Head examined more than one thousand animals and produced over 200 drawings for Lindsay Johnson. As the article finishes Head mentioned his interest in drawing the retina of birds which he would later complete for Casey Wood’s publication ‘The Fundus Oculi of Birds’ in 1917, which contained 145 drawings and sixty-one coloured paintings. In a letter from Richard Smellie (who later became good friends with Head) it describes how a series of animal encounters while working on Lindsay Johnson’s book had a profound effect on Head’s mental health and it paints a different picture than the article in Pearson’s. The letter explains how after a skirmish while examining a tiger ‘left him in a highly nervous state from which he never fully recovered’. After this experience ‘he spent much of his time in his own company, not wanting to mix with anyone’. Head was the greatest expert in ophthalmic paintings of this era and was the first artist whose name featured alongside the authors as seen in the front pages of Lindsay Johnson’s ‘A Pocket Atlas and Text-Book of the fundus Oculi’ published in 1911 (Fig. 6).
Fig. 5. These two examples of Arthur Head’s work show how his style evolved.
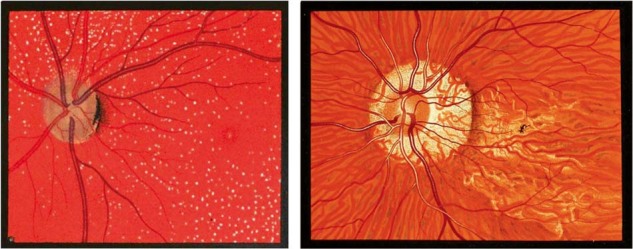
The image on the left featured in TOSUK in 1888 and the image on the right is from 1896. (Right image courtesy of the Wellcome Collection).
Fig. 6. Text showing acknowledgment of artist on inside cover below authors detail.
In Lindsay Johnson’s 1911 publication Head’s name features below the author. (Images courtesy of the Wellcome Collection).
In the early 1920s there was a shift to the commercialisation of ophthalmic painting from a hospital setting. Rayner Batten, senior consultant at the Western Ophthalmic Hospital required a painting of a patient’s retina so he approached Theodore Hamblin. A junior draughtsman, Richard Smellie, who went on to become managing director, was volunteered and produced adequate results. Batten mentioned to Hamblin that a drawing service would be of great value to local ophthalmic surgeons and in 1922 the drawing department was opened under the supervision of Arthur Head.
The drawing department at Theodore Hamblin
Theodore Hamblin eventually became part of the opticians Dollond & Aitchison Ltd, which in turn was merged with Boots Opticians in 2009. The archives of Boots contain historical records of Theodore Hamblin as well as information about the ophthalmic drawing department. Head advised on setting up the department in 1922 at Wigmore Street and seven ophthalmic draughtsmen were originally employed under his supervision (Fig. 7). Theodore Hamblin produced a handbook on ophthalmic drawing which is in the archives at Boots and it describes the draughtsman’s training and how the work was standardised. The handbook states ‘Applicants have in the first place been carefully selected, all having some knowledge of drawing and skill in the use of pencil and brush, and having no material error through refraction in either eye. They are then given a thorough course of training in observation and memory drawing by an artist who has given special attention to this branch; simultaneously they are taught the use of the Ophthalmoscope, and the observation of external disease and of the fundus conditions. They are educated in the technique of fundus drawing and the use of materials by Mr A. W. Head’. The handbook continues ‘In organising the department the paramount importance of standardisation has been kept permanently in view. This standardisation has not been introduced to simplify production, but to render the drawing comparable with each other’. ‘The drawing staff has been trained to a degree where drawings by two different draughtsmen are indistinguishable from each other, both being accurate’. The paintings were housed in large glass cabinets and formed an impressive reference library for medical professionals to access.
Fig. 7. This illustration shows Hamblin’s ophthalmic drawing department.
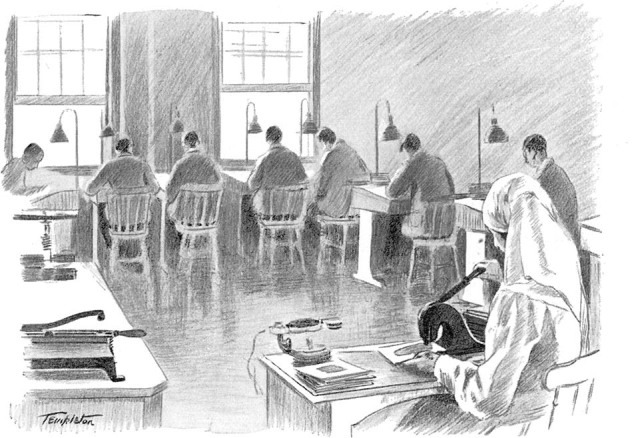
The draughtsmen were all required to wear white coats to give the impression that this was a medical procedure (Image courtesy of The Boots Archive).
As Tarrant looked through these glass cabinets and the hundreds of paintings they contained he was staggered at the level of artistry. Each time a physician requested a painting, a copy was produced and placed in the cabinets so they could be used for reference or selected to be reproduced for publication. The charges for examining a patient and producing a painting were one pound, one shilling for a private patient and 10 shillings, 6 pence for a hospital patient. If the draughtsman was required to visit the patient the charges were doubled. These paintings played a vital role in the education of eye conditions and were a valuable resource. Some of this collection still exists today and is stored in the archives of the Institute of Ophthalmology under the stewardship of Richard Keeler.
When Tarrant started at the drawing department, Tom Hooper was the only remaining artist from the original seven draughtsmen in 1922. It is very difficult finding examples of Hooper’s work because of the department’s standardisation, making it impossible to identify an artist from their own unique style or painting technique. The artists were not permitted to sign their names on the paintings, instead, each artwork featured a stamp with the name ‘Hamblins’. This is illustrated in Fig. 8 taken from an article by Arnold Sorsby where the Hamblins logo is at the bottom of the painting. This gave Theodore Hamblin national and international exposure as the paintings featured in ophthalmic journals and textbooks. Hooper taught Tarrant the same technique for examining the patients (using either an ophthalmoscope or slit lamp) and methods for producing the paintings as Head had taught him. Tarrant would sit next to Hooper and observe him examining the patient and learn how he produced the paintings in the ‘Hamblins’ style. Tarrant’s aptitude in drawing and previous interest in optics allowed him to start seeing patients and producing paintings after 6 months training. During this time he regularly visited the Wallace Collection (which was a short distance from the drawing department on Wigmore Street) during his lunchbreak to study the paintings, specifically the work by Jean Louis Ernest Meissonier. The Wallace Collection also holds 334 miniaturist paintings covering a span of 400 years. Tarrant would collect postcards from the museum and make copies using the miniaturist’s style. The miniaturist’s employed a technique known as stippling as shown in Jean-Baptiste Isabey’s self-portrait (Fig. 9). Stippling refers to applying small dots of paint that are layered to create subtle changes in colour and the exercise of replicating the postcards and copying this technique help shape Tarrant’s painting style.
Fig. 8. Adding the Hambins stamp to the paintings gave Theodore Hamblin free advertising in journals and publications.
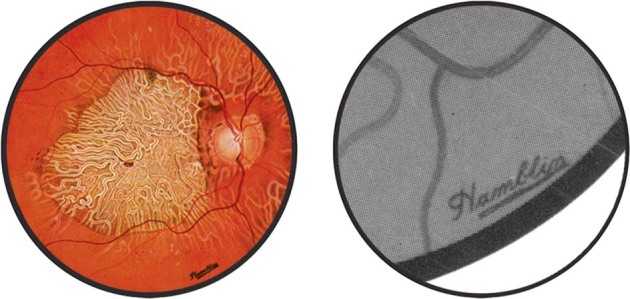
This brought recognition to the brand and associated Hamblins as medical practitioners.
Fig. 9. The three images at the top show magnified views of the stippling technique used by the miniaturists (Images courtesy of the Wallace Collection).
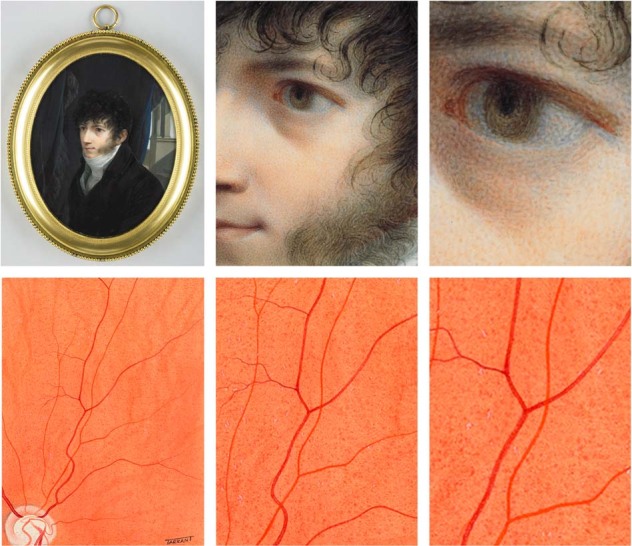
The bottom three show a detailed view of Tarrant’s painting utilising the same technique.
Painting Technique
I discussed with Tarrant the process of creating the paintings, the equipment he used, and experiences he had while working at Theodore Hamblin. A surgeon would identify a patient who required their eye to be documented and would arrange for them to have an appointment at the drawing department. Tarrant would first dilate, then examine the patient with an ophthalmoscope (if looking at the retina). This could take anywhere between 1 to 2 hours where sketches would be made using coloured pencils and a drawing pad. Once Tarrant was satisfied that he had enough information the patient would be free to go. The painting would be prepared by dry mounting high-quality cartridge paper on to a sheet of card. Using a compass, a thin circle in India ink would then be drawn on the cartridge paper (this is also how you can identify if it’s an original artwork due to the small compass hole in the centre). Tarrant would then get a sheet of thinner paper and use (low tack) masking tape to fix it to the cartridge paper. A hospital scalpel would then be used to cut a circular window in the paper following the thin black circle below so when adding the first watercolour wash it would not bleed over the edges of the cartridge paper below. The basic retinal base colour would be a Windsor and Newton scarlet vermillion and Tarrant would use different size sable brushes, 4 to 6 for the wash, 0 for the detail and move up to a 1 or 2 for the pathology (this numbering system refers to the size of the brush, the larger the number the bigger the brush). After the washes Tarrant would use a stipple technique similar to the miniaturist’s paintings that he studied at the Wallace Collection. However, instead of using dabs or spots, Tarrant would paint small marks, building up the layers, with the vessels and the pathology being added last. These paintings took Tarrant between half a day to a day to complete.
Like Arthur Head before him Tarrant also produced paintings of animal retinas. A local surgeon requested examples for a publication and Tarrant accompanied Hooper to London Zoo. Armed only with their ophthalmoscopes, pencils, and sketchbooks they examined all manner of animals, fish, and birds. Thankfully the zookeepers were more proficient with the anaesthetic than when Arthur Head visited, and this passed without incident.
After a year at Theodore Hamblin Tarrant started to travel around the country examining and documenting patients on request as this service was not available locally to other hospitals. At the request of the surgeon around a dozen patients would be invited to attend a clinic over 2 to 3 days to see the visiting artist. Tarrant would travel by train to the hospital and stay locally while he examined and sketched the patients. He would then return to Theodore Hamblin where the paintings would be completed before being sent to the surgeon who requested them. Tarrant continued to produce paintings for Theodore Hamblin until he was called up for national service at the age of 18 where he reported to the Royal Army Medical Corps at Crookham barracks, Hampshire. After 6 weeks basic first aid training the squadron was sent abroad but somehow a senior medical officer was notified of Tarrant’s artist ability and it was decided that he would be better placed to work at the eye department at the Queen Alexandra’s Military Hospital at Millbank, London. He was given a consultation room which contained a drawing board and slit lamp and continued to paint eye conditions of army personnel. Tarrant also travelled to military camps to examine soldiers and make sketches before returning to Queen Alexandra’s to complete the paintings. Towards the end of his national service Tarrant was told about an upcoming vacancy at the Institute of Ophthalmology. This position of retinal artist had been created because of the new medical illustration department that was being set up by Peter Hansell on the request of Sir Stewart Duke Elder.
Institute of ophthalmology
Hansell is credited for establishing the first department of medical photography and illustration in the United Kingdom at the Westminster Hospital Medical School. He was a pioneer in medical photography and audio-visual media and was at the forefront of the development of ophthalmic photography, which was still in its experimental phase. Tarrant applied along with Tom Hooper (his previous tutor at Theodore Hamblin) and was interviewed by Hansell who was impressed with the quality of his work. Hansell sent Tarrant’s portfolio off to Gabriel Donald to get his opinion as he was a leading figure in medical illustration and also a well-respected ophthalmic artist. Donald recommended Tarrant for the job on the strength of his portfolio, and he was offered the position which he accepted being paid £330 per year with annual rises of £25 per annum. Tarrant joined the Institute in 1950 (Fig. 10) and never returned to Theodore Hamblin, to whom he was grateful for giving him the draughtsman’s job. When Tarrant started at the Institute, Hansell asked him to meet Joy Brand (nee Trotman) who was an established ophthalmic artist employed by Moorfields. Brand worked on many publications including Ophthalmic Medicine by James Hamilton Doggart which was published in 1949 and features many of her paintings. In the acknowledgments, it states ‘Miss Joy Trotman has exhibited her customary skill and care in the drawing of illustrations’. As well as producing meticulous drawings of the retina, Brand taught fellow artists the techniques required to paint the retina. There are 88 examples of her paintings, both posterior and anterior segments in the archives at the Institute of Ophthalmology. Brand’s work is more of an artistic representation, focusing on the pathology giving the paintings a clean, soft, illustrative appearance. When we compare Brand’s work with Tarrant’s paintings there is a subtle difference in the style. Tarrant’s unembellished depiction includes a greater level of depth and information, most notability his inclusion of choroidal vessels (Fig. 11) which gives the painting an extraordinary level of realism. Tarrant visited Brand at Moorfields and they worked together for a few weeks. It was felt that because of Tarrant’s considerable experience there was little value in collaborating and Tarrant continued to work independently at the Institute. They were both members of the newly formed Medical Artists Association (MAA) whose goal was to gain recognition and safeguard the professional status of qualified artists. Tarrant and Brand both attended meetings regularly and exhibited their work. In 1952 the chairman of the MAA stated, ‘The Joint Exhibition with the Photographers was demonstrating to the Medical Profession the individuality and scope of the Medical Artist as opposed to the camera’ [3]. The MAA was keen to raise awareness of the quality and diversity of the artist’s work featured in this exhibition in light of the increasing threat of the number of emerging medical photographic departments.
Fig. 10. Black and white photograph taken in 1950 of Terence Tarrant at the Institute of Ophthalmology.
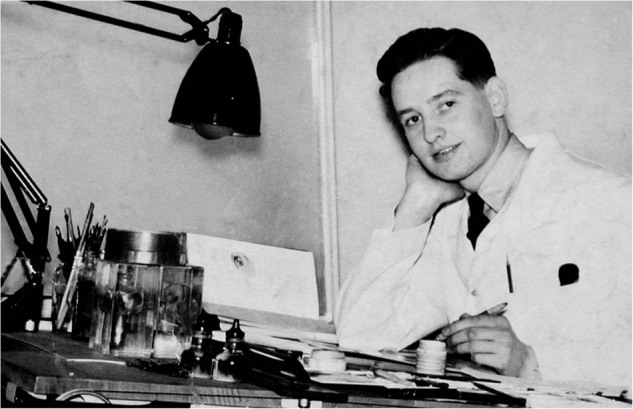
Photograph taken in 1950 of Tarrant at his drawing board at the Institute of Ophthalmology (Image courtesy of the Institute of Ophthalmology).
Fig. 11. Comparison showing subtle differences in two artists painting styles.

Although both artists have similar styles, Brand’s painting (left image) is softer, with less detail, whereas Tarrant’s painting shows a greater level of realism (right image) (Images courtesy of the Institute of Ophthalmology).
Tarrant began to establish himself as a talented artist who was adept at using an ophthalmoscope. He was now able to sign his work, something that he previously was unable to do during his time at Theodore Hamblin (Fig. 12). This raised his profile and associated his name with the paintings. Tarrant worked in a room adjacent to Duke Elder’s office and produced paintings, illustrations, and diagrams for the publication ‘System of Ophthalmology’. In the acknowledgments it reads ‘In preparing the illustration I have had the willing co-operation of Dr Peter Hansell and the Department of Medical Illustration of the Institute of Ophthalmology, the assistance of which, particularly that of Mr T. R. Tarrant, the Medical Artist, has been invaluable’.
Fig. 12. Example of Tarrant’s name on painting.
The joining of the two T’s was the suggestion of Peter Hansell, (Images courtesy of the Institute of Ophthalmology).
Tarrant’s reputation reached as far as America where he was offered a job with a lucrative salary ($7000 in the first year with a top salary of $10,000). Charles Schepens was one of the leading figures in retinal surgery and was working on a peripheral retinal publication. He was aware of Tarrant’s work and in 1961 he invited Tarrant to Boston to work in his clinic for 3 weeks. Unsurprisingly Schepens was suitably impressed with Tarrant’s paintings and he was offered the position. Being of a cautious nature and having recently married, Tarrant was unsure whether to accept. He returned to London and discussed Schepens offer with Hansell and decided to stay at the Institute, the following week they doubled Tarrant’s salary to ensure his services. While in Boston Tarrant used Schepen’s binocular indirect ophthalmoscope which had a great impact on his paintings. He became an expert in using this new technique and it gave him the ability to observe a greater area of the retina in three dimensions. As the means of examining the eye were improving, camera technology advanced, and the quality of the photographs started to challenge the role of the ophthalmic artist.
Camera technology
It took 33 years from when the first painting of the retina appeared in print to when the first fundus photograph from a living subject was published. If we compare paintings that appear in TOSUK from 1886 by M. Boole against Jackman and Websters grainy black and white photographs it illustrates the difference in quality and clinical usefulness (Fig. 13). It’s clear from these examples which method would be more desirable for publication in ophthalmic atlases as the reflex in the photograph obscures most of the retina and the colour painting has a greater visual appeal. It wasn’t until 1899, that Frederick Dimmer presented the first reflex-free fundus photograph at the Ninth International Congress of Ophthalmology. Dimmer continued to refine his technique and collaborated with Zeiss Jena to design and build a reflex-free fundus camera. In 1907 Dimmer completed the first retinal photographic atlas that contained 58 black and white photographs of the retina. The quality of these photographs is sufficient to establish a diagnosis and gives a clear view of the back of the eye. This instrument was so expensive that only one was ever built, and it wasn’t until 1926 that the first commercially available fundus camera was produced. Johan Wilhelm Nordenson developed a camera based on Allvar Gullstrand’s principle of reflex-free ophthalmoscopy and the Nordenson made fundus photography more practical and became the predominant commercial fundus camera.
Fig. 13. Comparison of the first retinal photograph and a retinal painting both from 1886.
When comparing Jackman and Websters photograph (on the left) against a painting by M. Boole (on the right) both from 1886 it is clear to see the differences in quality and how far away photography was to competing with ophthalmic artists.
Arthur J Bedell utilised the Nordenson for his 1930 publication ‘Photographs of the Fundus Oculi. A Photographic Study of Normal and Pathological Changes Seen Under the Ophthalmoscope’. These black and white photographs offer a detailed, clear view of the retina. However, the size of the printed image (3.5 cm in diameter) makes it difficult to examine the pathology closely. In the preface, Bedell states ‘To preserve an impression of a fundus, it was necessary to make hand drawings which were too often of value to the artist. The profession has therefore, depended upon word pictures supplemented by an occasional illustration or watercolour. The details for these drawings are painstakingly obtained by a laborious process for the artist and often a fatiguing ordeal for the patient. Even after hours of co-operation, the picture usually leaves much to be desired. The necessary expense of paintings is so great that even in the famous collections there are very few serial studies. He continues ‘By the use of photographs, it is possible for physicians to get a clearer idea of the disease with a better conception of the outline of the blood-vessels, the optic nerve and the innumerable retinal and choroidal variations. The absence of colour in the picture tends to emphasize these details. Although there is a greater level of detail in the photographs, the size, field of view and lack of colour make it difficult to agree when we compare against artists such as Annette Smith Burgess. When comparing Bedell’s photographs and Burgess’s paintings the most apparent difference is how striking Burgess’s work is compared to the photographs. Although the photographs could be deemed to be more accurate, the colour paintings give the publication a greater visual appeal and clearly depicts the pathology (Fig. 14). William Wilmer challenges Bedell’s notion regarding the superiority of photography and in the foreword of his 1934 Atlas Fundus Oculi, he states ‘Photography of the fundus has made great advances in recent years; but it cannot take the place of reproductions in colour by the brush’. This is made evident by the paintings by Burgess whose meticulous paintings accompany Wilmer’s text and clearly illustrate the pathology. Burgess was originally trained as an artist and became a full-time ophthalmic illustrator at the Wilmer Institute where she worked for 35 years. Burgess was skilled at using the ophthalmoscope and slit lamp and produced one hundred colour paintings for Wilmer’s Atlas Fundus Oculi. Burgess’s paintings are exceptional, not just for their ability to accurately illustrate retinal conditions but also her level of artistry. Wilmer continues in the forward ‘Photography in colour still has its limitations, and very few ophthalmologists have found the application of this method to be successful. For fundus changes which are minute but important are not always very clearly reproduced’. This is testament to the observation skill of the artists such as Burgess, mastering the use of the ophthalmoscope, and faithfully reproducing the appearance of the retina.
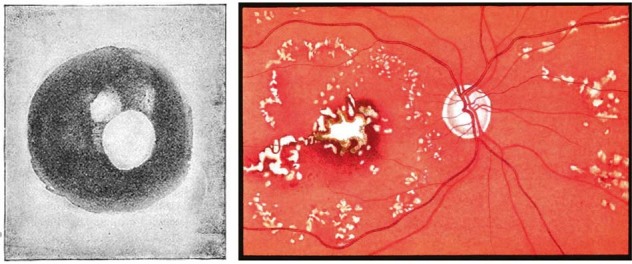
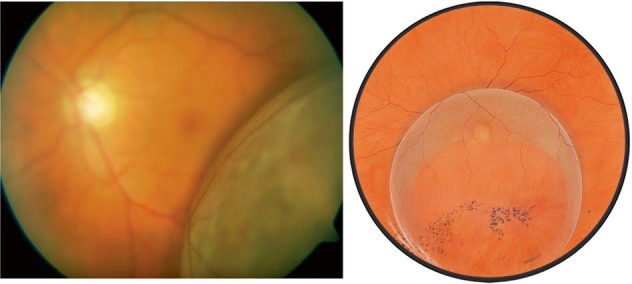
Fig. 14. Comparison of examples of retinal detachments.
Burgess’s painting (A) and Bedell’s photographs (B), both depict retinal detachments. Although the photographs are deemed to be more accurate does the painting give a clearer representation of the pathology?
Colour photography of the retina began to be used successfully the year after Wilmer’s atlas was published with the introduction of Kodachrome, the most favoured camera for this use was still the Nordenson. Camera technology continued to evolve and in 1955 the Zeiss Littmann retinal camera replaced the Nordenson. This ushered in a new era of retinal photography and the Littmann camera became the workhorse for ophthalmic photography departments. Other manufacturers started to develop cameras and in 1967 there were nine cameras that were commercially available increasing to twenty cameras by 1977. The availability of this technology had a direct effect on the demand for Tarrant’s retina paintings as most hospitals now had dedicated ophthalmic photography departments. Requests for Tarrant’s paintings were limited to mainly anterior segment work and documenting areas of the peripheral retina. Using the binocular indirect ophthalmoscope allowed Tarrant to see as far as the ora serrata (where the retina terminates) and as cameras of this era had a limited view peripheral photography was challenging. It was possible for Tarrant to show the whole of the retina in his paintings which was preferable for teaching and publication as opposed to photographic montages which only show a section of the retina when stitched together. His paintings of retinal tears and detachments illustrate the pathology better than any camera from this era (Fig. 15).
Fig. 15. This comparison illustrating retinoschisis highlights the limited field of view of a conventional retinal camera.
Peripheral photography was challenging and to document the whole of the area would require multiple photographs using different focal planes (Painting courtesy of the Institute of Ophthalmology).
Towards the start of the 1980’s ophthalmic photography was well established and demand for retinal paintings had considerably reduced. The Institute was running out of money and in 1981, to the surprise of Tarrant, the audio-visual department was closed. Tarrant was given early retirement but was then immediately rehired by Moorfields and relocated to the High Holbon branch. To understand the decision to re-employ Tarrant we need to look no further than in Peter Leavers book documenting the History of Moorfields [4]. Leaver describes Tarrant as ‘a draughtsman of outstanding ability, who developed a skill in painting the ocular fundus unmatched either before or since’. Leaver continues ‘As it was several years before fundus photography developed sufficiently to enable wide-angle views of the fundus that were of equivalent quality, and because all his work was outstanding, he became indispensable, producing exquisite drawings and diagrams to illustrate every aspect of the human eye, healthy or diseased, and contributing to vast numbers of scientific publications’.
Tarrant continued to produce work for clinicians and publications including Clinical Ophthalmology for Jack Kanski. In the acknowledgments of Clinical Ophthalmology, it reads ‘I am greatly indebted to Miss Daphne Barrister for taking most of the photographs, the artwork is due to the genius of Terry Tarrant’. This acknowledgment gives an insight as to Kanski’s opinion of the value of the artist when compared to that of the photographer.
The last retinal artist
The value of Tarrant’s retinal paintings was starting to be questioned due to the emerging photographic departments. The low costs involved in processing and printing and level of skill required to take a photograph challenged the perception of the value of the artist. Acquiring examples of pathology were no longer reliant on the ability of the ophthalmic artist. The accessibility of retinal photographs increased as more photographic departments opened, thus affecting the material value of Tarrant’s painting. This may explain why all of Tarrant’s paintings that featured in Kanski’s publications are missing and believed to have been destroyed by the author as these objects were deemed to be replaceable. As the demand for retinal photographs increased, the requests for paintings reduced and photographs inevitably replaced Tarrant’s paintings in the majority of clinical textbooks. In 1985, after working at the Institute for 35 years and creating thousands of paintings Tarrant retired.
After leaving the Institute Tarrant continued to work, setting up a drawing board at his home in Dorset. He continued to receive requests for paintings and illustrations for publications and surgeons would visit him at his home to discuss their requirements. Included in these were the subsequent volumes of Clinical Ophthalmology by Jack Kanski. Tarrant worked with Kanski up to the fourth edition where retinal photography would prominently feature. The first edition of Clinical Ophthalmology (published in 1984) contained 128 retinal paintings and 85 colour photographs of the back of the eye. The fourth edition (published in 1999) contained 503 retinal photographs and 118 retinal paintings. This trend continued and the number of photographs increased to 625 in the eight edition (published in 2016) and the number of paintings fell to 23. There is no mention of Tarrant in the acknowledgments of the fourth edition, instead it reads ‘I am extremely grateful to Anne Bolton for her great skill in taking many of the photographs’. The tenth edition of Kanski’s Clinical Ophthalmology continues to use Tarrant’s retinal paintings and this latest edition contains 33 examples of his work. I asked the author of this edition, John Salmon, why they are still included? His response was ‘I have included Terry Tarrant’s superb paintings of the fundus in the latest edition of Kanski’s Clinical Ophthalmology because of his ability to capture rare pathology with remarkably accuracy and precision of colour. What is truly amazing is that he was able to do this many years before wide-field photography was available’. The introduction of widefield photography replaced the majority of Tarrant’s remaining paintings in the eighth edition of Kanski which only includes 23 of his retinal paintings (105 less that the first edition). If we compare a widefield photograph taken on the Optomap against a painting of the same condition it highlights Wallace’s sentiment on the colour and physical obstacles, in this case the false colour and the eye lashes and lids which are the source of much frustration when using this device (Fig. 16). Wallace discussed in his paper the future of the profession and summarised ‘Before concluding this subject, we may look ahead and ask what help photography may afford us in the future. I am not very sanguine, but science has her own way of circumventing difficulties, and I trust I may yet see photographs which will surpass the best drawings of to-day, just as our draughtsmen have thrown into the shade the pristine attempts which we have just been considering. It is said that “ satisfactory’“ photographs have been made, but hitherto I have not met with any that can replace drawings by hand. Even were we provided with a perfect apparatus which could focus the concavity of the fundus uniformly, avoiding reflexes, and were research and ingenuity to put at our disposal a wide range of colour, physical obstacles would still remain’ [1]. The artist selects what to include in the painting whereas the camera is unbiased and records what is in the frame. Ophthalmic paintings can often better represent abnormal conditions when compared to photography because of the artists ability to ‘clean up’ the image, as seen in the works by Brand. The imperfections of photography have been generally accepted due to the convenience of the acquisition of instantaneous results.
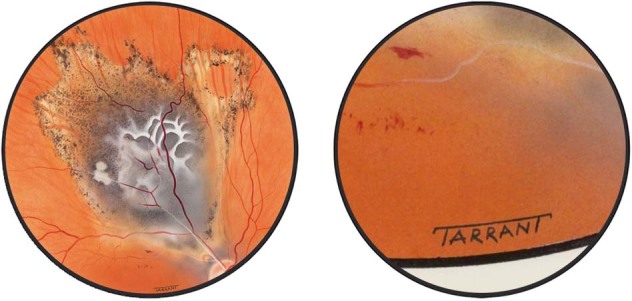
Fig. 16. Comparison of widefield photograph and painting illustrating a retinal detachment.
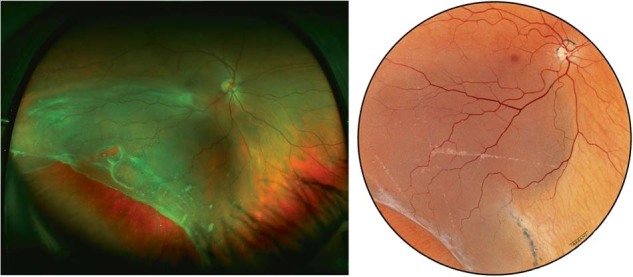
This highlights Wallace’s concerns about the colour and physical obstacles that the camera records which are not present in Tarrant’s painting (Painting courtesy of the Institute of Ophthalmology).
The evolution of imaging
While working at the Institute Hansell experimented with fundus photography using the Nordsenson camera. Tarrant witnessed the camera’s evolution and I asked him whether he had used the equipment and taken a photograph of the retina during his career. His reply was that he was aware of the technology but never took a photograph of the retina. Did Tarrant foresee that this would eventually replace painting and he purposely distanced himself from the technology? Like the miniaturist painters of the 18th century, which remained highly popular until the development of photography in the mid-19th century, the requests for Tarrant’s work diminished as retinal photography became established. Technological development of imaging equipment continues, and ophthalmic photographers may now face the same fate as ophthalmic painters. Camera automation already exists with the Optomap widefield camera having an automatic function where the photographer is only required to position the patient and the camera takes the photograph when the eye is aligned. Kaplan et al. [5] evaluated the use of an Optovue Optical Coherence Tomography (OCT) scanner in out-of-hours clinics (when a photographer is not available). This camera employs computerised voice directives instructing the patient on positioning and fixation. They concluded that automated OCT showed promise for diagnosis and residents and fellows reported that this availability changed clinical management in after-hours settings. A robot-mounted OCT scanner was developed by Draelos et al. [6] for autonomous imaging without the need for operator invention. Draelos concluded that this technology may enable the diagnosis and monitor patients with eye conditions in non-specialist clinics. These clinics could be similar to how automation is utilised in supermarkets following the ‘self-checkout’ model and specifically developed for screening the retina. The advances in artificial intelligence (AI) such as the DeepMind health project at Moorfields Eye Hospital [7] may also decide on the patient’s pathway, eliminating the need for a trained photographer or ophthalmologist to interpret the results, therefore removing the human element altogether. This is in line with the projected number of 20 million manufacturing jobs lost to robotics and automation by 2030 [8] and may rewrite the role of the ophthalmic photographer, consigning the profession to the same fate as the retinal artist.
Ophthalmic art
I was interested in finding out whether an ophthalmic journal would feature a retinal painting and if there is still a role for ophthalmic artists. I followed Tarrant’s technique and produced a series of paintings of the optic disc (Fig. 17) which were then submitted to Eye (previously known as TOSUK where the early artists such as Boole and Head’s work was featured) for possible use on the cover. I felt the paintings were better than Loring’s work in 1886 but the exercise was more challenging than I expected and gave me a greater respect for the artists mentioned in this article. The editor accepted the paintings for publication as cover artwork which suggests there is still an interest in this art form. Tarrant viewed the paintings and commented ‘that they were very professional looking’ and asked whether I was thinking of a career as an ophthalmic artist before advising against it due to his experiences. We spoke at length about how photography replaced the ophthalmic artist and I shared my thoughts that although there is no clinical need due to the advances in imaging, there is still a place for retinal paintings. The paintings in Figs. 15 and 16 clearly illustrate pathology better that a photograph due to Tarrant’s observational and artistic skills, which is why they are still selected for publication. Retinal paintings are now mainly appreciated for their artistic quality and this may explain why the artwork was selected for the cover of Eye.
Fig. 17. Watercolour paintings of the retina created following Tarrant’s instruction.
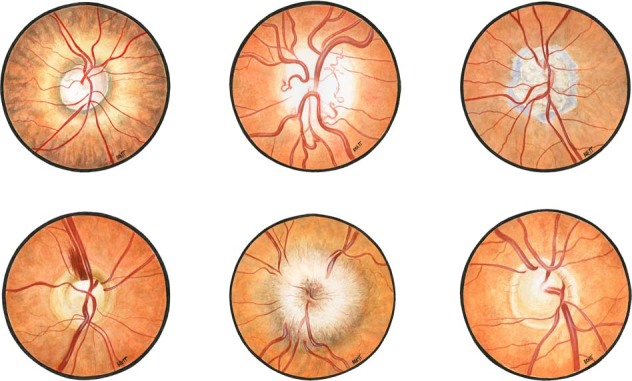
This collection was chosen to feature on the cover of Eye (formally known as TOSUK).
Tarrant’s paintings should be viewed alongside the early artists such as Jaegar, Liebreich and Head, and apricated in an art historiography context, charting the evolution, development, and eventual decline of this art movement.
Recognition
When Tarrant visited the labour exchange with his father in 1944 and found the vacancy at Theodore Hamblin, he could not have foreseen the journey that was ahead of him. Through chance encounters, good fortune, and a natural artistic ability, Tarrant became a prolific and highly respected ophthalmic artist. His drawings and illustrations continue to feature in many publications and 347 of his original paintings are housed in the archives of the Institute of Ophthalmology. This represents only a small fraction of the number of paintings Tarrant produced during his career and a vast number are still unaccounted for. It is the hope of Wendy Franks and Richard Keeler that one day these can be reunited with the rest of Tarrant’s work at the Institute.
Tarrant laid down his paintbrush for the last time in 1990 and retired after 46 years of working as an ophthalmic artist. His paintings and name are recognised both nationally and internationally in ophthalmology yet when looking at his handwritten CV, which is a single side of A4, and given all his achievements through his career, it illustrates his humility, something that came across during our conversations. In 2001 Tarrant was awarded Honorary Fellowship of the Royal College of Ophthalmologists, the highest accolade it can bestow. This is given in recognition to individuals who have made a significant contribution to ophthalmology.
The cycle of recording the appearance of the retina, once restricted to medical professionals, trained artists, and photographers, has returned to a model similar to Head’s drawing department. Due to the advancements in camera technology opticians can once again offer the service of documenting the retina. It is commonplace for a photograph to be taken during the appointment for an extra charge (a figure that is considerably more than Theodore Hamblin’s fee of one pound, one shilling for a painting). These technological advances, along with the introduction of automation and AI have furthered our ability to observe the retina and may one day replace the human element. The acknowledgments for the photographs and scans that appear in future ophthalmic atlases may mention software companies and camera manufacturers instead of artists and photographers. One name however will still survive in these publications and be kept alive in the diagrams, illustrations, and retinal paintings that feature in its pages.
Funding
No applicable funding sources.
COMPETING INTERESTS
The authors declare no competing interests.
Footnotes
Whilst writing this article I received the news that Terence Tarrant sadly passed away aged 93 after a short illness. For 46 years Tarrant examined and documented patient’s eyes and the paintings he produced significantly contributed to British Ophthalmology. When studying his artwork one can easily identify if it’s a ‘Tarrant’. His signature and paintings are as recognisable as any long-established artist that features in any national gallery. It has been the honour of this author to share his story, covering the life and career of the last retinal artist.
The original online version of this article was revised: The name ‘Terence R. Tarrant’ was incorrectly given as ‘Terance R. Tarrant’. Additonally, the following footnote was added: “Whilst writing this article I received the news that Terence Tarrant sadly passed away aged 93 after a short illness. For 46 years Tarrant examined and documented patient’s eyes and the paintings he produced significantly contributed to British Ophthalmology. When studying his artwork one can easily identify if it’s a ‘Tarrant’. His signature and paintings are as recognisable as any long-established artist that features in any national gallery. It has been the honour of this author to share his story, covering the life and career of the last retinal artist”. The original online version of this article was revised due to a retrospective Open Access cancellation.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Change history
8/10/2023
A Correction to this paper has been published: 10.1038/s41433-023-02663-0
References
- 1.Wallace W. The beginnings of fundus illustration. Br J Ophthalmol. 1919;3:102–10. doi: 10.1136/bjo.3.3.102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Woodward M. Eye to eye with wild beasts. Pearson’s Mag. 1902;8:69–79. [Google Scholar]
- 3.Archer, P. A History of the Medical Artists’ Association of Great Britain. 1949–1997, 326 (1998).
- 4.Leaver, P. The History of Moorfields Eye Hospital, Forty Years On. 3rd ed. (Royal Society of Medicine Press Ltd, 2004).
- 5.Kaplan RI, Chen M & Gupta M. Impact of automated OCT in a high-volume eye urgent care setting (2019). https://bmjophth.bmj.com/content/4/1/e000187.info [DOI] [PMC free article] [PubMed]
- 6.Draelos M, Ortiz P, Qian R, Viehland C, McNabb R, Hauser K, et al. Contactless optical coherence tomography of the eyes of freestanding individuals with a robotic scanner. Nat Biomed Eng. 2021;5:726–36. doi: 10.1038/s41551-021-00753-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.De Fauw J, Ledsam JR, Romera-Paredes B. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat Med. 2018;24:1342–50. doi: 10.1038/s41591-018-0107-6. [DOI] [PubMed] [Google Scholar]
- 8.Oxford Economics. How Robots Changed the World 2019. https://cdn2.hubspot.net/hubfs/2240363/Report%20-%20How%20Robots%20Change%20the%20World.pdf?utm_medium=email&_hsenc=p2ANqtz--S_yv5LZTWzdC5IER_NtSl3PcknlmRKCRLWkiY7DXoc24tLeHNQmxbfIluLCA4PrkWMen4_J_hWSH49WG3OQvHF61Jlg&_hsmi=74013545&utm_content=74013545&utm_source=hs_automation&hsCtaTracking=07b1855a-24f4-4b99-bcb8-b0d2a13b715e%7C53b7a48e-9591-4179-8eab-694443190b4f