

Abstract
Background:
There is substantial heterogeneity in how people react to potentially traumatic events (PTEs). Although some literature has explored this heterogeneity, there are only a few studies identifying factors associated with it within the disaster literature.
Objective:
The current investigation identified latent classes of post-traumatic stress disorder (PTSD) symptoms and differences between these classes after exposure to Hurricane Ike.
Methods:
Adults living in Galveston and Chambers County, Texas, (n = 658) completed a battery of measures during an interview conducted two to five months after Hurricane Ike. Latent class analysis (LCA) was performed to identify latent classes of PTSD symptoms. Additionally, gender, age, racial or ethnic minority status, depression severity, anxiety severity, quality of life, perceived need for services, and disaster exposure were examined to explore class differences.
Results:
LCA supported a 3-class model with low (n = 407, 61.9%), moderate (n = 191, 29.0%), and high PTSD symptoms (n = 60, 9.1%). Women appeared most at-risk for a moderate-severity presentation as compared to a low-severity presentation. Further, racial or ethnic minority groups appeared most at-risk for a high-severity presentation as compared to a moderate-severity presentation. Overall, the high symptom class had the poorest well-being, the most perceived need for services, and the highest exposure to the disaster, followed by the moderate symptom class, and finally the low symptom class.
Conclusions:
PTSD symptom classes appeared to be differentiated primarily by overall severity as well as important psychological, contextual, and demographic dimensions.
Keywords: Latent class analysis, Natural disaster, Post-traumatic stress disorder, Anxiety, Depression, Quality of life, Psychological services
Most people experience at least one potentially traumatic event (PTE) throughout their lifespan. For example, in a national sample of U. S. adults, the lifetime prevalence of exposure to a PTE was 89.7% (Kilpatrick et al., 2013). There is substantial heterogeneity in how people react to such events. One such reaction is post-traumatic stress disorder (PTSD). PTSD symptoms can be highly disparate as they are determined by multiple factors such as type of event, maintenance factors, and risk and resilience factors (see reviews: DiMauro et al., 2014; Galatzer-Levy et al., 2018). Interestingly, there are 636,120 possible symptom combinations that meet the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) PTSD criteria (American Psychiatric Association, 2013; Galatzer-Levy and Bryant, 2013). This suggests the need to address trauma as a dynamic system on a continuous dimension, as opposed to a dichotomy of absence or presence of psychopathology based on cutoffs (Bonanno et al., 2011). In addition to this, experiencing a PTE may lead to increased risk of psychological problems. Empirical studies have shown that PTSD is highly comorbid with other psychiatric conditions in diverse populations (for e.g. see: Kaltman et al., 2010; Keane and Kaloupek, 1997; Macdonald et al., 2010; Sautter et al., 1999). Understanding the nature of PTSD and the heterogeneity within its presentation is essential since symptom presentations and comorbid mental health problems can vary vastly. Such an understanding can pave the way for development of therapeutic models to address diverse needs.
Latent class analysis (LCA) is a statistical method used to identify latent classes (or subgroups) within a population based on a number of observed indicators (Nylund-Gibson and Choi, 2018). LCA allows the study of a heterogeneous population wherein these latent classes can differ based on unique components of a construct of interest, such as PTSD (Hagenaars and McCutcheon, 2002). LCA is a person-centered approach that identifies latent classes based on the diversity of responses from participants, as opposed to a variable-centered approach that is focused on total levels of a unitary construct (Nylund-Gibson and Choi, 2018). Thus, LCA can capture interactive effects in ways that a variable-centered approach cannot (Bámaca-Colbert and Gayles, 2010).
Person-centered approaches, such as LCA, have become increasingly common in understanding trauma (Howard and Hoffman, 2018; O’Donnell et al., 2017). For instance, in a sample of 122 African refugees, three distinct latent classes were identified based on intrusive, avoidant, and arousal PTSD symptoms: a pervasive class with higher likelihood of all symptoms (32.0%), a high-threat class with higher intrusion and avoidance symptoms (45.9%), and a moderate-avoidance class with higher thoughts/feelings of avoidance (22.1%; Barbieri et al., 2021). Further, in a sample of 158 U.S. military Veterans that screened positive for PTSD, three distinct latent classes were identified based on probabilities of PTSD symptoms: a dysphoric class with higher negative affect, anhedonia, and externalizing behavior (36.2%), a threat class with higher intrusion and avoidance (29.8%), and a high symptom class (34.0%) with high probabilities of all symptoms (Byrne et al., 2019). Similarly, in a sample of 4,352 World Trade Center responders after the 9/11 attacks, three distinct latent classes were identified based on probabilities of PTSD symptoms: a high-symptom class with high probabilities of all PTSD symptoms (45.3%), a dysphoric class with higher emotional numbing and dysphoric arousal (31.5%), and a threat class characterized by higher re-experiencing, avoidance, and anxious arousal (23.2%; Horn et al., 2016). Thus, research has begun to identify subpopulations based on PTSD symptoms, with some studies finding classes that have high probabilities of experiencing specific PTSD symptoms in addition to classes with high probabilities of experiencing all PTSD symptoms.
Importantly, latent classes of PTSD symptoms have been found to vary along several important dimensions. For example, Byrne and colleagues (2019) found that the dysphoric class was especially likely to have lifetime history of major depressive disorder (MDD), and the high symptom class was especially likely to have current generalized anxiety disorder (GAD), lower quality of life, and attempted suicide or current suicidality. Additionally, both the dysphoric and high symptom class were more likely to have engaged in mental health treatment (Byrne et al., 2019). Similarly, Horn et al. (2016) also found that the high symptom class was most likely to screen positive for MDD. Assessing correlates of latent classes, such as other mental health concerns and treatment utilization, helps identify what distinguishes the classes and, in applied settings, may inform targeted service delivery based on the unique needs of each class.
Natural disasters are particularly important PTEs to study using LCA. Along with adverse economic and physical health effects, natural disasters have adverse psychological effects (see systematic review and meta-analysis: Beaglehole et al., 2018). They affect a large population at a given time point and thus have critical public health importance. Yet, to date, only one study used LCA to identify classes of PTSD symptoms after exposure to a natural disaster (Rosellini et al., 2014). In this study, in a sample of 810 adults living in Mississippi during Hurricane Katrina, LCA suggested four latent classes based on PTSD symptom severity: a severe symptom class (10.2%), a moderate symptom class (28.3%), a mild symptom class (29.8%), and a negligible symptom class (31.7%) (Rosellini et al., 2014). This study indicated that membership to the severe and moderate symptom class was associated with co-occurring depression symptom severity and suicidal ideation (Rosellini et al., 2014). This indicates that as with other PTEs, PTSD symptoms following natural disasters vary substantially and correspond with other important mental health variables. Examining heterogeneity within the population after exposure to a natural disaster is important as the nature of the event can create traumatic reactions specific to it. Further, evaluating differences between latent classes can allow us to understand differences specific to the individuals within these subgroups. This can help develop targeted interventions to address issues that can arise after exposure to a natural disaster.
Building on existing literature, the present study used LCA to identify subgroups based on PTSD symptoms after experiencing Hurricane Ike in 2008. We also examined differences among the classes based on demographic variables (gender, age, and race/ethnicity), health variables (depression, anxiety, quality of life, and perceived need for services), and disaster exposure severity. Since the LCA approach is data-driven, we had no specific hypothesis about the number or nature of the latent classes. However, based on previous studies, we expected to see either a three-class solution or a four-class solution, as well as differences among the classes in terms of demographics, health variables, and disaster exposure severity.
1. Methods
1.1. Participants
The present study used the Galveston Bay Recovery Study dataset (GBRS; National Center for Disaster Mental Health Research et al., 2016). Data were collected from Galveston County and Chambers County, Texas. This study area was comprised of five strata characterized by the maps of flooding after Hurricane Ike as based on the Federal Emergency Management Agency (FEMA) and on poverty levels in the year 2000 based on United States Census data. Sampling strata were divided over a spectrum, with Stratum 1 expected to have experienced the greatest Hurricane damage and Stratum 5 expected to have experienced the least damage (for more information, see Tracy et al., 2011, p. 668). Of note, to ensure inclusion of individuals that most likely had experienced hurricane-related traumatic events, Strata 1 and 2 were oversampled relative to the remaining strata to maximize selection of participants from the most affected areas.
All participants (n = 658) were interviewed once, two to five months after Hurricane Ike (November 2008–March 2009). The sample of 658 represented the 40% of participants among those recruited who provided at least partial data; all 658 participants with at least partial data were included in the present analyses (Smith, 2016). In interviews, participants were asked to verbally respond to several validated self-report measures that assessed mental health symptoms and functioning after exposure to Hurricane Ike.
In terms of gender, 60% of participants were female. All participants were age 18 or older; 9% were between ages 18 to 24, 16% were between ages 25 to 34, 16% were between ages 35 to 44, 18% were between the ages 45 to 54, 18% were between ages 55 to 64, and 23% were above the age of 64. In terms of race, the majority of participants identified as White (62.61%), some (19.14%) identified as Asian (0.76%), Black (14.89%), Native Hawaiian or Pacific Islander (0.15%), or American Indian or Alaska Native (0.91%). Few (2.43%) belonged to two or more races, and for the remaining participants (18.25%) race was unknown. In terms of ethnicity, 19.03% identified as Hispanic, and 80.97% identified as non-Hispanic. In sum, 38.17% belonged to racial or ethnic minority groups, identifying as non-White and/or Hispanic, and 61.83% did not belong to a racial or ethnic minority group, identifying as White non-Hispanic.
1.2. Measures
1.2.1. Post-traumatic stress
Post-traumatic stress symptoms were assessed with the PTSD Checklist-Civilian Version (PCL-C; Weathers et al., 1993). The PCL-C assessed three symptom criteria based on DSM-IV (American Psychiatric Association, 1994) PTSD symptoms: Criterion B, re-experiencing symptoms; Criterion C, avoidance symptoms; and Criterion D, arousal symptoms. Participants were asked to refer to the time since Hurricane Ike when indicating if they had experienced each symptom. Responses to each item were coded as “yes” (1) or “no” (0), “yes” meaning symptom was endorsed and “no” meaning symptom was not endorsed. Thus, during data collection, the PCL-C was modified to be administered with binary item scoring rather than the usual Likert item scoring.
For re-experiencing symptoms (5 items), participants were asked if they had experienced: “repeated, disturbing memories of Ike”, “repeated, disturbing dreams of Ike”, “suddenly acting or feeling as if Ike were happening again”, “feeling very upset when something reminded you of Ike”, and “having physical reactions when something reminded you of Ike”. For avoidance symptoms (7 items), participants were asked if they had experienced: “avoiding thinking or talking about Ike”, “avoiding activities or situations because they reminded you of Ike”, “trouble remembering important parts of Ike”, “loss of interest in activities you used to enjoy”, “feeling distant or cut off from people”, “feeling emotionally numb”, and “feeling as if the future will be cut short”. Finally, for arousal symptoms (5 items), participants were asked if they had experienced: “trouble falling or staying asleep”, “feeling irritable or having angry outbursts”, “having difficulty concentrating”, “being ‘super-alert’ or watchful or on guard”, and “feeling jumpy or easily startled”. The scale also showed good re-test reliability and favorable patterns of convergent and discriminant validity (Conybeare et al., 2012; Weathers et al., 1993). For the purposes of conducting LCA, we analyzed the individual items separately.
1.2.2. Depression
Depression severity was assessed using the Patient Health Questionnaire-9 (PHQ-9; Kroenke and Spitzer, 2002). Participants were asked to refer to the past month while reporting symptoms. Scores on each item were measured on a continuum of 0 to 3 (0 = “not at all” to 3 = “nearly every day”). The current study used a total score ranging from 0 to 27 for each participant. The scale showed good validity and reliability (Kroenke et al., 2001) It also demonstrated good internal consistency in the current study (Cronbach’s α = 0.87).
1.2.3. Anxiety
Anxiety severity was assessed based on the General Anxiety Disorder-7 (GAD-7; Spitzer et al., 2006). Participants were asked to refer to the past month while reporting symptoms. Scores on each item were measured on a continuum of 0 to 3 (0 = “not at all” to 3 = “nearly every day”). The current study used a total score ranging from 0 to 21 for each participant. The GAD-7 demonstrated good internal consistency in the current study (Cronbach’s α = 0.87). It also showed good validity and reliability in the general population (Löwe et al., 2008).
1.2.4. Perceived need for services
Perceived need for services was assessed using items adapted from the Perceived Need for Care Questionnaire (PNCQ; Meadows et al., 2000). Participants were asked to report their perceived needs for various mental health and economic support services (6 items) since Hurricane Ike. Responses for each item were coded as “yes” (1) or “no” (0): “felt the need for information about common stress reactions”, “felt the need for medicine to help with emotional problems”, “felt the need to discuss causes of distress”, “felt the need to change thoughts, feelings, or behaviors”, “felt the need to talk through problems”, and “felt the need to get help sorting out housing, employment.” For the present study, each item was examined separately. This scale has demonstrated acceptable validity and reliability (Meadows et al., 2002).
1.2.5. Quality of life
Quality of life was assessed using the short form version of the Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q-SF; Endicott et al., 1993). Participants were asked to refer to the past month while responding. Scores on each item were measured on a continuum of 1 to 5 (1 = “not at all” to 5 = “extremely”). Q-LES-Q-SF assessed participants’ satisfaction with various aspects of their lives (14 items): “physical health”, “mood”, “work”, “household activities”, “social relationships”, “family relationships”, “leisure time activities”, “ability to function in daily life”, “sexual drive, interest and/or performance”, “economic status”, “living/housing situation”, “ability to get around physically without feeling dizzy or unsteady or falling”, “your eyesight in terms of ability to do work or hobbies”, “overall sense of well being”. The current study used a total score ranging from 14 to 71 for each participant. The scale demonstrated good internal consistency in the current study (Cronbach’s α = 0.91). It also possessed good validity and reliability (Stevanovic, 2011).
1.2.6. Disaster exposure severity
Disaster exposure was assessed by asking participants if they experienced each of several forms of actual or threatened danger or loss as a result of Hurricane Ike (9 items): “personally present during Hurricane force winds or major flooding”, “unsure about safety or whereabouts of family members/close friends”, “stranded during or after storm”, “involved in rescue or recovery efforts”, “self or household member performed dangerous activity during storm”, “displaced from home for more than one week”, “any personal property loss”, or “any loss of or damage to sentimental possessions”. Responses for each item were coded as “yes” (1) or “no” (0). A composite score of all items was computed to represent disaster exposure severity with higher numbers representing more severe exposure.
1.3. Data analysis
LCA was conducted using Mplus Version 8.2 (Muthén & Muthén, 1998–2017). The 17 items from the PCL-C that assessed PTSD symptoms were used as latent class indicators. Model fit was assessed using the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), Adjusted Lo-Mendell-Rubin Likelihood Ratio Test (LMR-LRT). Classification quality was assessed using entropy. We examined the fit for various models starting from a two-class model and increasing the number of classes until model fit did not improve. Smaller values of AIC and BIC indicated superior fit (Nylund-Gibson and Choi, 2018). Adjusted LMR-LRT has associated p values, where p < .05 indicates a significant difference in fit between a less complex and a more complex model (Nylund et al., 2007; Nylund-Gibson and Choi, 2018). Further, although entropy is not a direct indicator of model fit, higher values indicated that people were classified with more confidence and showed better between-group distinction (Kline, 2015; van de Schoot et al., 2017).
To understand PTSD symptoms among the latent classes, we examined the proportion of each latent class endorsing each PTSD symptom. Based on previous latent class analyses of PTSD symptoms, probability estimates ≥ 0.60 suggest high probability, esimates ≤ 0.59 and ≥ 0.15 suggest moderate probability, and estimates < 0.15 suggest low probability (Burstein et al., 2012; Eisma et al., 2019; Lenferink et al., 2017).
For the selected latent class model, latent class membership was used as a predictor of each of the demographic, health, and disaster variables (gender, age, racial and ethnic minority status, anxiety, depression, perceived need, quality of life, disaster exposure) using the BCH method1 (Vermunt, 2010).
2. Results
2.1. Model selection
Table 1 provides model fit results. The three-class model fit better than the two-class model according to AIC, BIC, and adjusted LMR-LRT. Additionally, the three-class model had good classification quality based on entropy. However, the four-class model did not fit significantly better than the three-class model according to LMR-LRT, and it fit worse than the three-class model according to the BIC. Thus, model fit ceased improving beyond three-classes, and we selected the three-class model.
Table 1.
Fit statistics.
| Model | LL | AIC | BIC | Adjusted LMR-LRT p-value | Entropy |
|---|---|---|---|---|---|
| 2-class | −4968.459 | 7384.690 | 7541.812 | 0.0000*** | 0.935 |
| 3-class | −3657.345 | 6881.935 | 7119.863 | 0.0000*** | 0.921 |
| 4-class | −3387.968 | 6821.320 | 7140.054 | 0.2620 | 0.892 |
Note.
p < .05
p < .01
p < .001; AIC = Akaike information criterion; BIC = Bayesian information criterion; LL = log-likelihood; LMR-LRT = Lo-Mendell-Rubin likelihood ratio test.
2.2. Model results
Fig. 1 shows the probability estimates of endorsed PTSD symptoms per class. The largest class (n = 407, 61.9%) had low probability of endorsement of 17 out of 17 PCL-C symptoms and we thus termed it the “Low Symptom Class.” The second largest class (n = 191, 29.0%) had moderate probability of endorsement of 16 out of 17 as well as low probability of endorsement of 1 out of 17 PCL-C symptoms (trouble remembering Hurricane Ike) and we thus termed it the “Moderate Symptom Class.” Finally, the smallest class (n = 60, 9.1%). had high probability of endorsement of 17 out of 17 PCL-C symptoms and we termed it the “High Symptom Class.” Of note, there did appear to be spikes in avoidance and arousal symptoms for the high symptom class (C4 Anhedonia, C5 detachment, D1 sleep problems, and D4 hypervigilance) as well as several spikes in a few of the re-experiencing symptoms for the moderate symptom class (B1 intrusive memories and B4 distress due to reminders).
Fig. 1.
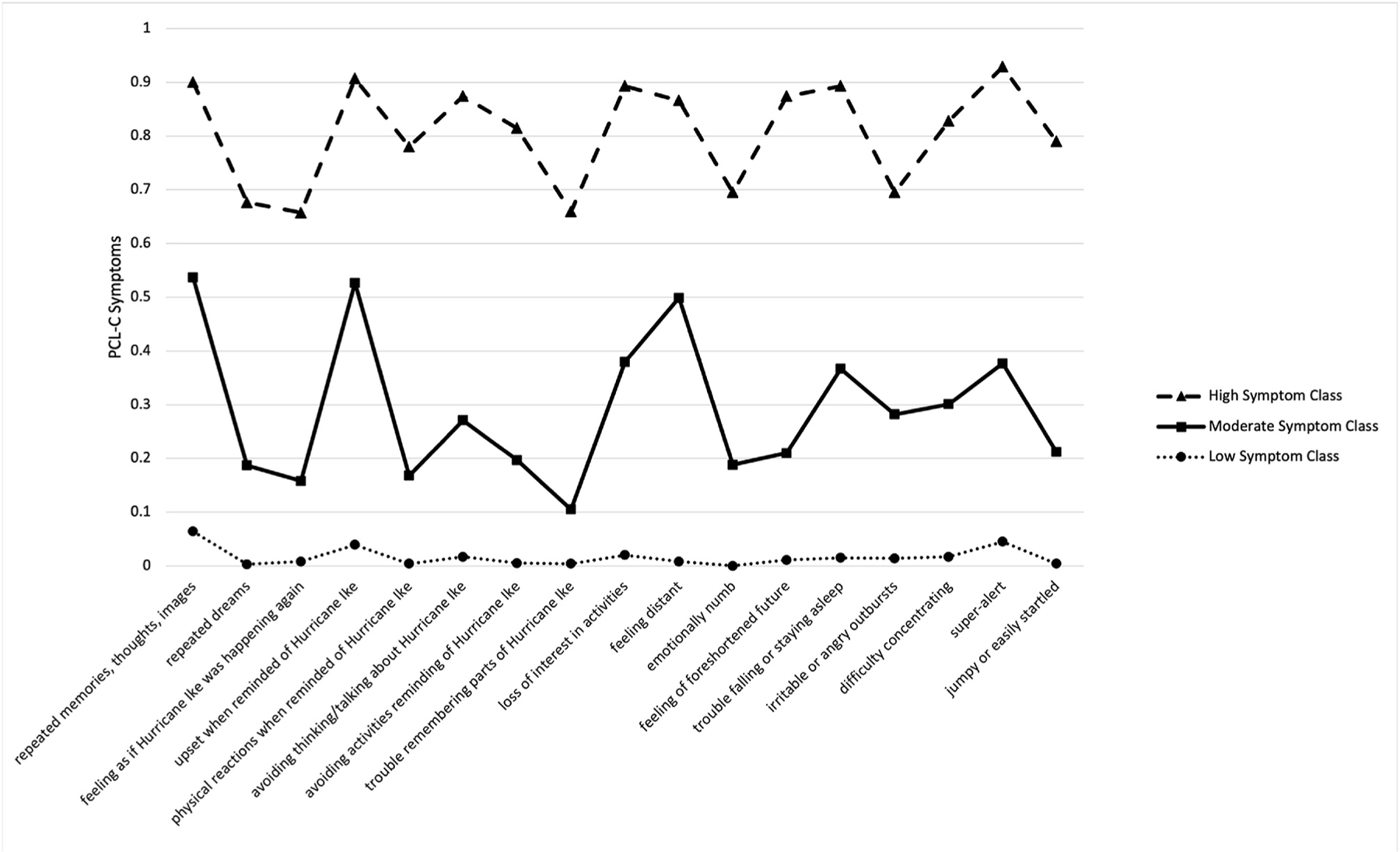
Probabilities of PTSD Symptom Endorsement across Latent Classes
Note. The x-axis shows each PTSD symptom assessed; The y-axis depicts probabilities of endorsing each symptom; PCL-C = PTSD Checklist-Civilian Version. PTSD symptoms were assessed 2–5 months after Hurricane Ike.
2.3. Class differences
Table 2 shows class differences for gender, age, racial and ethnicity minority status, depression, anxiety, perceived need for services, quality of life, and disaster exposure across latent classes. In addition, it shows chi-square values for class comparisons based on these variables.
Table 2.
Class characteristics and class comparisons.
| Variable | High Symptom Class (n=60) |
High vs. Moderate | Moderate Symptom Class (n=191) |
Moderate vs. Low | Low Symptom Class (n=407) |
|---|---|---|---|---|---|
|
| |||||
| M (SE) | χ2 | M (SE) | χ2 | M (SE) | |
| Gendera | 0.245 (0.059) | 1.910 | 0.343 (0.036) | 5.879* | 0.453 (0.025) |
| Age | 3.912 (0.215) | 0.125 | 4.001 (0.120) | 1.051 | 3.845 (0.085) |
| Racial or ethnic minorityb | 0.251 (0.065) | 18.332*** | 0.581 (0.038) | 3.240 | 0.665 (0.024) |
| Depression | 7.440 (1.087) | 14.936*** | 2.959 (0.360) | 27.908*** | 0.881 (0.125) |
| Anxiety | 5.312 (0.785) | 11.562** | 2.373 (0.331) | 21.351*** | 0.701 (0.119) |
| Perceived need: info about stress reactions | 0.446 (0.074) | 10.696** | 0.183 (0.030) | 23.630*** | 0.028 (0.009) |
| Perceived need: medicine for emotional problems | 0.468 (0.074) | 15.492*** | 0.154 (0.028) | 11.406** | 0.049 (0.011) |
| Perceived need: discuss causes of distress | 0.219 (0.061) | 0.694 | 0.162 (0.028) | 19.216*** | 0.028 (0.009) |
| Perceived need: change thoughts or feelings | 0.502 (0.074) | 6.867** | 0.284 (0.035) | 24.985*** | 0.089 (0.015) |
| Perceived need: talk through problems | 0.536 (0.074) | 1.734 | 0.424 (0.038) | 60.250*** | 0.095 (0.016) |
| Perceived need: get help with housing, employment | 0.641 (0.072) | 8.285** | 0.403 (0.038) | 53.899*** | 0.093 (0.016) |
| Quality of life | 35.278 (1.419) | 17.723*** | 42.083 (0.715) | 77.860*** | 49.964 (0.489) |
| Disaster Exposure Severityc | 4.681 (0.249) | 5.116* | 4.048 (0.117) | 57.427*** | 2.957 (0.076) |
Note.
p < .05
p < .01
p < .001; age: 18–24 years = 1, 25–34 years = 2, 35–44 years = 3, 45–54 years = 4, 55–64 years = 5, 65+ years = 6; anxiety = GAD-7; depression = PHQ-9; M = mean; perceived need = PNCQ Item endorsement; quality of life = Q-LES-Q-SF Scores; SE = standard error; χ2 = chi-square tests with one degree of freedom are reported.
Coded as Male = 1.
Coded as White Non-Hispanic = 1.
Coded as 1 = low severity to 8 = high severity.
Two out of the three demographic factors demonstrated significant class differences. In terms of gender, there was a significant difference between the moderate and low symptom classes, such that there was a higher percentage of female participants in the moderate symptom class as compared to the low symptom class. There was no significant gender difference between the moderate and the high symptom classes. There were no significant differences across classes in terms of age. In terms of racial and ethnic minority status, there was a significant difference between the moderate and high symptom classes, such that there was a higher percentage of participants belonging to racial or ethnic minority groups in the high symptom class as compared to the moderate and low symptom classes. There was no significant difference between the moderate and the low symptom classes. Overall, female participants appeared most at-risk for a moderate-severity PTSD presentation as opposed to a low-severity PTSD presentation, and participants belonging to racial or ethnic minority groups appeared most at-risk for high-severity PTSD presentation as opposed to moderate- or low-severity PTSD presentation.
The two measures of psychopathology (i.e., depression and anxiety severity) demonstrated a consistent pattern of differences across classes. For both variables, there was a significant difference between the moderate and low symptom classes, as well as between the moderate and high symptom classes. Specifically, the low symptom class reported lower levels of depression and anxiety compared to the moderate symptom class. Additionally, the moderate symptom class had lower levels of depression and anxiety compared to the high symptom class. Relatedly, quality of life also demonstrated a consistent pattern of differences across classes. There was a significant difference between the moderate and low symptom classes, as well as between the moderate and high symptom classes. Specifically, the low symptom class reported higher levels of quality of life as compared to the moderate symptom class. Additionally, the moderate symptom class reported higher levels of quality of life as compared to the high symptom class. Thus, with increasing severity of PTSD presentation, there was increasing severity of anxiety and depression symptoms and decreasing quality of life.
In alignment with the psychopathology and quality of life variables, the perceived need for service items also demonstrated a consistent pattern of differences across classes. For all perceived service needs, we found significant differences between the moderate and low symptom classes, as well as between the moderate and high symptom classes, with the exception that moderate and high symptom classes did not differ from each other in their perceived need to discuss causes of distress since Hurricane Ike and perceived need to talk through problems since Hurricane Ike. Specifically, the high symptom class reported greater need for information about common stress reactions since Hurricane Ike, medicine to help with emotional problems since Hurricane Ike, help to change thoughts, feelings, or behaviors since Hurricane Ike, and help sorting out housing, employment since Hurricane Ike, as compared to the moderate symptom class. Therefore, belonging to a higher severity PTSD symptom class was associated with reporting a higher need for a range of services to support adjustment after the Hurricane.
Lastly, in examination of disaster exposure severity, results demonstrated that the high symptom class consisted of participants with the highest levels of Hurricane Ike exposure, followed by the moderate symptom class, and finally the low symptom class. Furthermore, differences between the high and moderate symptom classes as well as the moderate and low symptom classes were significant.
3. Discussion
The aim of this study was to understand heterogeneity of PTSD symptoms using LCA in a large sample of adults from areas affected by Hurricane Ike. Overall, we found that individuals exposed to Hurricane Ike could be classified into subgroups based on differing PTSD symptom severity. Moreover, these subgroups were distinct from one another based on various demographic factors, levels of concurrent psychological symptoms (depression and anxiety), quality of life, perceived need for services, and disaster exposure. These results provide evidence for heterogeneous responses to disaster with distinct profiles across demographic, psychological, and contextual factors.
When examining number of classes, LCA suggested a three-class solution: a low symptom class (61.4%), a moderate symptom class (31.2%), and a severe symptom class (7.4%). This is consistent with a previous natural disaster LCA study that found four PTSD symptom classes differing in overall symptom severity (Rosellini et al., 2014). However, the pattern differs somewhat from what has been reported in other LCA studies of participants experiencing various types of PTEs. Such previous studies have identified classes that differed substantially in terms of specific types of PTSD symptoms (e.g., avoidance symptoms vs. re-experiencing symptoms), rather than overall symptom severity (Barbieri et al., 2021; Byrne et al., 2019; Horn et al., 2016). Interestingly, although classes did not differ substantially in the current analyses based on symptom types, we found spikes in avoidance and arousal symptoms for the high symptom class, namely anhedonia, detachment, sleep problems, and hypervigilance, as well as spikes in a few of the re-experiencing symptoms for the moderate symptom class, namely, intrusive memories and distress due to reminders. Thus, although classes were differentiated primarily by their overall severity, certain distinct symptoms were especially elevated relative to other symptoms in each of these classes. Elevation in these specific symptoms may help inform levels of severity. Assessing these symptoms in particular could be important in screening, observation, and triage settings with limited time for assessing PTSD symptoms. In addition, therapists with limited resources may want to target re-experiencing, avoidance, and arousal symptoms in particular.
The current investigation further explored demographic differences among PTSD symptom classes. We found that the moderate symptom class included a significantly higher proportion of female participants compared to the low symptom class. This finding is consistent with substantial evidence suggesting that women are at greater risk than men for internalizing disorders including PTSD (e.g., Ditlevsen and Elklit, 2010; Eaton et al., 2012; Hyde and Mezulis, 2020). There may be various reasons why women possessed greater risk for belonging to the moderate (versus low) symptom class, such as insufficient social support and more severe trauma appraisals (Olff et al., 2007). Identifying intervention methods to prevent this gender disparity in PTSD presentation following natural disaster is important for public mental health following population-wide PTEs.
In addition, the high symptom class had a significantly larger proportion of participants that identified as racial and/or ethnic minorities compared to the moderate symptom class. This finding adds to the growing literature surrounding risk factors for those belonging to minority groups. Hispanic participants or participants identifying with a race other than White (e.g., African American participants) may have been at a higher risk of adverse outcomes following the hurricane due to various structural reasons such as poorer housing conditions or lack of access to resources that may aid in disaster recovery (e.g., Dancy, 2018; Farfel et al., 2008; Rodriguez-Díaz and Lewellen-Williams, 2020; Sharpe and Wolkin, 2021). For example, a report found that Hurricane Ike-affected areas with the greatest hurricane vulnerability also had the highest concentration of individuals belonging to racial or ethnic minority groups (Dancy, 2018). Further, a study of adverse effects of natural disasters and extreme weather found that the mortality rate among non-Hispanic African Americans was twice as high as non-Hispanic White participants (Sharpe and Wolkin, 2021). Such structural disparities could have made Hispanic and African American persons more vulnerable to adverse impact of Hurricane Ike. Overall, these findings suggest that different demographic groups may be at risk for differential and clinically important PTSD symptom presentations following natural disasters. It will be important for future research and applied efforts to identify and remediate causes for these differences.
There were significant class differences when exploring depression and anxiety symptoms, quality of life, perceived need for services, and disaster exposure. The finding of more severe PTSD classes having poorer overall mental health is consistent with prior LCA results (Rosellini et al., 2014). Fewer studies, however, have examined services needed within latent classes of PTSD symptoms. Interestingly, 76.2% of participants in the high severity class reported a perceived need for employment or housing support; this was the highest reported need within this group, though need for mental health services was also high. Of note, the high symptom class reported greater perceived need than the moderate symptom class for several kinds of psychological services: gaining information about stress reactions, changing thoughts and feelings, and taking medication for emotional problems. These kinds of services represent the psychoeducation and exposure-focused interventions that are typical of cognitive-behavioral therapies, as well as pharmacological treatment, both of which are evidence-based methods of treating PTSD symptoms (Bryant and Friedman, 2001). At the same time, the moderate symptom class did not report significantly lower perceived needs than the high symptom class for discussing causes of distress or talking through problems. Needing to talk through problems was also the most commonly reported perceived need in the moderate symptom class. This may suggest that talk therapy involving psychoeducation, problem-solving skills, and processing of the trauma may be useful for this group. Ultimately, treatment delivery decisions for a given individual are based on a number of factors such as available treatment options, degree of need, understanding of the empirical literature on efficacy, and individual readiness for specific interventions. Providers should take care to incorporate each of these sources of information, though it is possible that future latent class analysis studies on PTSD symptoms and service needs will pave the way for empirically derived methods of indicated service delivery (e.g., Lanza and Rhoades, 2013).
We also found that degree of exposure to Hurricane Ike related danger and loss was the worst for the high symptom class. This was closely followed by the moderate symptom class and was the lowest for the low symptom class. Thus, higher degrees of exposure to a natural disaster could be a risk factor for a more severe PTSD presentation. This converges with results from a recent study suggesting that youths with high exposure to a flood had higher levels of depression, anxiety, and PTSD symptom severity as compared to those with lower exposure (Felix et al., 2019). Future research should continue to explore the relationship between PTSD severity and degree of disaster-related exposure.
Findings from this study add to the existing literature on natural disasters with specific focus on PTSD symptomatology. Although classes were generally differentiated by overall severity of PTSD symptoms, within each class, there were certain symptoms that were especially common. Thus, the latent classes carried information beyond a person’s overall PCL-C sum score. An additional contribution from the present study was the examination of perceived service needs within latent PTSD symptom classes and exposure severity. Perceived need for a range of psychological and social welfare services was high in the high severity class, as well as (to a lesser extent) the moderate severity class. Thus, a possible application of this work is the delivery of targeted intervention strategies to members of classes that report specific service needs (Lanza and Rhoades, 2013). We are aware of no intervention study to date that has used empirically derived latent class membership as a basis for determining treatment delivery, but this represents a promising direction for personalized care. Such efforts will require replication of the present findings to ensure that the latent class solution and associated treatment preferences are generalizable across diverse contexts and related to optimal treatment outcome.
Despite the strengths of this study, various limitations warrant mention. Firstly, this study used cross-sectional data and could not provide information on changes over time compared to pre-hurricane data. A prospective study could clarify whether belonging to a given latent class may predict later mental health and comorbid symptoms. Additionally, this study focused on residents of a single disaster-affected area after one event. Generalizability would be enhanced by examining latent classes of PTSD symptoms across multiple disaster-affected samples. Furthermore, PTSD symptoms were collected in 2008 using a version of the PCL-C based on DSM-IV. Therefore, findings may not be representative of DSM-5 PTSD symptoms or specific symptom clusters within DSM-5. Of note, the primary difference between DSM-IV and DSM-5 PTSD symptoms is the division of DSM-IV avoidance symptoms into DSM-5 avoidance and negative cognitive/mood symptoms. Although many PTSD symptoms overlap substantially between DSM-IV and DSM-5, using an updated assessment in future research would ensure that latent classes could be understood in terms of current nosology. Another limitation was that the current dataset did not include assessment of pre-Hurricane Ike PTSD or related psychopathology symptoms. Also, PTSD symptoms were not measured solely in reference to Hurricane Ike. Instead, the study only assessed PTSD symptoms two to five months after Hurricane Ike with reference to the time since Ike. Therefore, we cannot rule out the possibility that previous PTSD or other psychopathology contributed to PTSD symptom severity as opposed to being due solely to exposure to Hurricane Ike. Future research should measure history of prior psychopathology and trauma as well as disaster-specific PTSD symptoms. Finally, although this study used probability sampling methods and achieved a fairly high response rate (40%), there is not information available about participants who did not respond which could help gauge the representativeness of the sample. Gathering such information in future studies of natural disaster impact (e.g., through follow-up phone calls with non-responders) would be valuable. Addressing these limitations in future research would provide a deeper understanding of the nature and implications of PTSD symptom subpopulations.
4. Conclusion
The current study examined heterogeneity of PTSD symptoms in a large community sample from Galveston Bay area following Hurricane Ike. There were three latent classes which were characterized by low, moderate, or high PTSD symptoms. Relative to men, women were more likely to be part of the moderate symptom class compared to the low symptom class. Furthermore, relative to White non-Hispanic participants, participants belonging to racial or ethnic minority groups were more likely to be part of the high symptom class versus the moderate symptom class. Latent class membership was related to depression, anxiety, quality of life, perceived need for services, and disaster exposure, suggesting that latent classes of PTSD severity could have important implications for mental health and well-being. Further, combined with other investigations of PTSD symptom heterogeneity, the present study can inform the development of treatments and interventions with a special focus on at-risk groups.
Acknowledgments
The data used in this publication were made publicly available on the Resource Center for Minority Data and theInter-university Consortium for Political and Social Research. Data were collected and shared by the National Center for Disaster Mental Health Research, Sandro Galea, and Fran Norris. Further, the data collection was supported by National Institute of Mental Health (NIMH 5 P60 MH082598). The original authors and organizations involved in collecting, funding, and distributing the data are not responsible for any analyses, writing, or interpretation in this manuscript.
Funding source declaration
Data collection for this study was funded by the National Institute of Mental Health (5P60MH082598). Additionally, the authors were supported by a grant from the National Institute of Mental Health (5R01MH115128-03). The funding agencies, and the researchers who originally collected and disseminated the data, are not responsible for any data analysis or interpretation in this manuscript. No author is being paid to write this article by a pharmaceutical company or other agency.
Abbreviations:
- PTE
potentially traumatic event
- PTSD
post-traumatic stress disorder
- LCA
latent class analysis
- MDD
major depressive disorder
- GAD
generalized anxiety disorder
- GBRS
Galveston Bay Recovery Study
- FEMA
Federal Emergency Management Agency
- PCL-C
PTSD Checklist-Civilian Version
- PHQ-9
Patient Health Questionnaire-9
- GAD-7
General Anxiety Disorder-7
- PNCQ
Perceived Need for Care Questionnaire
- Q-LES-Q-SF
Quality of Life Enjoyment and Satisfaction Questionnaire
- AIC
Akaike Information Criterion
- BIC
Bayesian Information Criterion
- LMR-LRT
Lo-Mendell-Rubin Likelihood Ratio Test
- LL
log-likelihood
- DSM-IV
Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition
- DSM-5
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
Footnotes
Credit author statement
DrishtiE.Sanghvi: Conceptualization, Methodology, Software, Validation, Formal analysis, Data Curation, Writing - Original Draft, Writing - Review & Editing, Visualization. GavinN.Rackoff: Methodology, Validation, Data Curation, Writing - Review & Editing, Visualization, Supervision. Michelle G. Newman: Validation, Writing - Review & Editing, Supervision.
Declaration of competing interest
The authors declare that they have no conflicts of interest regarding this article’s authorship, research, and publication, or any financial disclosures.
IRB statement
In the Galveston Bay Recovery Study (GBRS), participants were contacted based on their location within the study area (Galveston County and Chambers County, Texas) and eligibility. Additional information about the terms of use for the GBRS dataset can be found at: http://www.icpsr.umich.edu/icpsrweb/ICPSR/studies/34801/terms. This study used publicly accessible data from the GBRS dataset, which was collected with institutional review board approval.
Handling Editor: Susan J. Elliott
We chose to use the BCH method to model associations between latent classes and other variables in the study because this method accounts for classification error. That is, each participant has non-zero probability of belonging to each class, and we cannot be entirely certain about someone’s class. Using other variables to predict class membership, such as through logistic regression, would ignore uncertainty in class membership and increase risk for type I error. Ultimately, this is a cross-sectional study, and the goal was to identify correlates of class membership, rather than to delineate precursors or consequences of class membership. Thus, we chose the BCH method because it was the most principled way to model associations with class membership. For more information, see Asparouhov and Muthén (2014).
Data availability
Data will be made available on request.
References
- American Psychiatric Association, 1994. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). American Psychiatry Press. [Google Scholar]
- American Psychiatric Association, 2013. Diagnostic And Statistical Manual of Mental Disorders (DSM-5). 10.1176/appi.books.9780890425596. [DOI] [PubMed]
- Asparouhov T, Muthén BO, 2014. Auxiliary variables in mixture modeling: Three-step approaches using Mplus. Structural Equation Modeling: A Multidisciplinary Journal, 21 (3), 329–341. 10.1080/10705511.2014.915181. [DOI] [Google Scholar]
- Bámaca-Colbert MY, Gayles JG, 2010. Variable-centered and person-centered approaches to studying Mexican-origin mother-daughter cultural orientation dissonance. Journal of Youth and Adolescence, 39 (11), 1274–1292. 10.1007/s10964-009-9447-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barbieri A, Visco-Comandini F, Alunni Fegatelli D, Dessì A, Cannella G, Stellacci A, Pirchio S, 2021. Patterns and predictors of PTSD in treatment-seeking African refugees and asylum seekers: A latent class analysis. International Journal of Social Psychiatry, 67 (4), 386–396. 10.1177/0020764020959095. [DOI] [PubMed] [Google Scholar]
- Beaglehole B, Mulder RT, Frampton CM, Boden JM, Newton-Howes G, Bell CJ, 2018. Psychological distress and psychiatric disorder after natural disasters: Systematic review and meta-analysis. The British Journal of Psychiatry, 213 (6), 716–722. 10.1192/bjp.2018.210. [DOI] [PubMed] [Google Scholar]
- Bonanno GA, Westphal M, Mancini AD, 2011. Resilience to loss and potential trauma. Annual Review of Clinical Psychology, 7, 511–535. 10.1146/annurev-clinpsy-032210-104526. [DOI] [PubMed] [Google Scholar]
- Bryant RA, Friedman M, 2001. Medication and non-medication treatments of post-traumatic stress disorder. Current Opinion in Psychiatry, 14 (2), 119–123. 10.1097/00001504-200103000-00004. [DOI] [Google Scholar]
- Burstein M, Georgiades K, Lamers F, Swanson SA, Cui L, He JP, Merikangas KR, 2012. Empirically derived subtypes of lifetime anxiety disorders: Developmental and clinical correlates in U.S. adolescents. Journal of Consulting and Clinical Psychology, 80 (1), 102–115. 10.1037/a0026069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Byrne SP, Harpaz-Rotem I, Tsai J, Southwick SM, Pietrzak RH, 2019. Latent typologies of DSM-5 PTSD symptoms in U.S. military Veterans. Psychiatry Research, 273, 266–273. 10.1016/j.psychres.2018.12.094. [DOI] [PubMed] [Google Scholar]
- Conybeare D, Behar E, Solomon A, Newman MG, Borkovec T, 2012. The PTSD checklist—civilian version: Reliability, validity, and factor structure in a nonclinical sample. Journal of Clinical Psychology, 68 (6), 699–713. 10.1002/jclp.21845. [DOI] [PubMed] [Google Scholar]
- Dancy K, 2018. Seizing the opportunity for equitable and inclusive redevelopment: Galveston’s trials after Hurricane Ike offer lessons for other communities https://www.dallasfed.org/-/media/Documents/cd/pubs/galveston.pdf?la=en.
- DiMauro J, Carter S, Folk JB, Kashdan TB, 2014. A historical review of trauma-related diagnoses to reconsider the heterogeneity of PTSD. Journal of Anxiety Disorders, 28 (8), 774–786. 10.1016/j.janxdis.2014.09.002. [DOI] [PubMed] [Google Scholar]
- Ditlevsen DN, Elklit A, 2010. The combined effect of gender and age on post traumatic stress disorder: Do men and women show differences in the lifespan distribution of the disorder? Annals of General Psychiatry, 9, 32. 10.1186/1744-859x-9-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eaton NR, Keyes KM, Krueger RF, Balsis S, Skodol AE, Markon KE, Hasin DS, 2012. An invariant dimensional liability model of gender differences in mental disorder prevalence: Evidence from a national sample. Journal of Psychopathology and Clinical Science, 121 (1), 282–288. 10.1037/a0024780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisma MC, Lenferink LI, Chow AY, Chan CL, Li J, 2019. Complicated grief and post-traumatic stress symptom profiles in bereaved earthquake survivors: A latent class analysis. European Journal of Psychotraumatology, 10 (1), 1558707. 10.1080/20008198.2018.1558707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Endicott J, Nee J, Harrison W, Blumenthal R, 1993. Quality of life enjoyment and satisfaction questionnaire: A new measure. Psychopharmacology Bulletin, 29 (2), 321–326. 10.1111/j.1365-2850.2011.01735.x. [DOI] [PubMed] [Google Scholar]
- Farfel M, DiGrande L, Brackbill R, Prann A, Cone J, Friedman S, Thorpe L, 2008. An overview of 9/11 experiences and respiratory and mental health conditions among World Trade Center Health Registry enrollees. Journal of Urban Health, 85 (6), 880–909. 10.1007/s11524-008-9317-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Felix ED, Binmoeller C, Nylund-Gibson K, Benight CC, Benner AD, Terzieva A, 2019. Addressing disaster exposure measurement issues with latent class analysis. Journal of Traumatic Stress, 32 (1), 56–66. 10.1002/jts.22368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galatzer-Levy IR, Bryant RA, 2013. 636,120 ways to have posttraumatic stress disorder. Perspectives on Psychological Science, 8 (6), 651–662. 10.1177/1745691613504115. [DOI] [PubMed] [Google Scholar]
- Galatzer-Levy IR, Huang SH, Bonanno GA, 2018. Trajectories of resilience and dysfunction following potential trauma: A review and statistical evaluation. Clinical Psychology Review, 63, 41–55. 10.1016/j.cpr.2018.05.008. [DOI] [PubMed] [Google Scholar]
- Hagenaars JA, McCutcheon AL (Eds.), 2002. Applied latent class analysis. Cambridge University Press. [Google Scholar]
- Horn SR, Pietrzak RH, Schechter C, Bromet EJ, Katz CL, Reissman DB, Feder A, 2016. Latent typologies of posttraumatic stress disorder in World Trade Center responders. Journal of Psychiatric Research, 83, 151–159. 10.1016/j.jpsychires.2016.08.018. [DOI] [PubMed] [Google Scholar]
- Howard MC, Hoffman ME, 2018. Variable-centered, person-centered, and person-specific approaches: Where theory meets the method. Organizational Research Methods, 21 (4), 846–876. 10.1177/1094428117744021. [DOI] [Google Scholar]
- Hyde JS, Mezulis AH, 2020. Gender differences in depression: Biological, affective, cognitive, and sociocultural factors. Harvard Review of Psychiatry, 28 (1), 4–13. 10.1097/hrp.0000000000000230. [DOI] [PubMed] [Google Scholar]
- Kaltman S, Green BL, Mete M, Shara N, Miranda J, 2010. Trauma, depression, and comorbid PTSD/depression in a community sample of Latina immigrants. Psychological Trauma: Theory, Research, Practice, and Policy, 2 (1), 31. 10.1037/a0018952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keane TM, Kaloupek DG, 1997. Comorbid psychiatric disorders in PTSD: Implications for research. Annals of the New York Academy of Sciences, 821 (1), 24–34. 10.1111/j.1749-6632.1997.tb48266.x. [DOI] [PubMed] [Google Scholar]
- Kilpatrick DG, Resnick HS, Milanak ME, Miller MW, Keyes KM, Friedman MJ, 2013. National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. Journal of Traumatic Stress, 26 (5), 537–547. 10.1002/jts.21848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline RB, 2015. Principles and practice of structural equation modeling. Guilford Publications. [Google Scholar]
- Kroenke K, Spitzer RL, 2002. The PHQ-9: A new depression diagnostic and severity measure. Psychiatric Annals, 32 (9), 509–515. 10.3928/0048-5713-20020901-06. [DOI] [Google Scholar]
- Kroenke K, Spitzer RL, Williams JBW, 2001. The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16 (9), 606–613. 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lanza ST, Rhoades BL, 2013. Latent class analysis: An alternative perspective on subgroup analysis in prevention and treatment. Prevention Science, 14 (2), 157–168. 10.1007/s11121-011-0201-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lenferink LIM, de Keijser J, Smid GE, Djelantik A, Boelen PA, 2017. Prolonged grief, depression, and posttraumatic stress in disaster-bereaved individuals: Latent class analysis. European Journal of Psychotraumatology, 8 (1), 1298311. 10.1080/20008198.2017.1298311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzog W, Herzberg PY, 2008. Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Medical Care, 46 (3), 266–274. 10.1097/MLR.0b013e318160d093. [DOI] [PubMed] [Google Scholar]
- Macdonald A, Danielson CK, Resnick HS, Saunders BE, Kilpatrick DG, 2010. PTSD and comorbid disorders in a representative sample of adolescents: The risk associated with multiple exposures to potentially traumatic events. Child Abuse and Neglect, 34 (10), 773–783. 10.1016/j.chiabu.2010.03.006. [DOI] [PubMed] [Google Scholar]
- Meadows G, Burgess P, Bobevski I, Fossey E, Harvey C, Liaw S-T, 2002. Perceived need for mental health care: Influences of diagnosis, demography and disability. Psychological Medicine, 32 (2), 299–309. 10.1017/s0033291701004913. [DOI] [PubMed] [Google Scholar]
- Meadows G, Harvey C, Fossey E, Burgess P, 2000. Assessing perceived need for mental health care in a community survey: Development of the perceived need for care questionnaire (PNCQ). Social Psychiatry and Psychiatric Epidemiology, 35 (9), 427–435. 10.1007/s001270050260. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO, 1998–2017. Mplus user’s guide, Eighth Edition.
- National Center for Disaster Mental Health Research, Galea S, Norris F, 2016. Galveston Bay Recovery Study, pp. 2008–2010. 10.3886/ICPSR34801.v1. [DOI]
- Nylund KL, Asparouhov T, Muthén BO, 2007. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling: A Multidisciplinary Journal, 14 (4), 535–569. 10.1080/10705510701575396. [DOI] [Google Scholar]
- Nylund-Gibson K, Choi AY, 2018. Ten frequently asked questions about latent class analysis. Translational Issues in Psychological Science, 4 (4), 440–461. 10.1037/tps0000176. [DOI] [Google Scholar]
- O’Donnell ML, Schaefer I, Varker T, Kartal D, Forbes D, Bryant RAA, Steel Z, 2017. A systematic review of person-centered approaches to investigating patterns of trauma exposure. Clinical Psychology Review 57, 208–225. 10.1016/j.cpr.2017.08.009. [DOI] [PubMed] [Google Scholar]
- Olff M, Langeland W, Draijer N, Gersons BP, 2007. Gender differences in posttraumatic stress disorder. Psychological Bulletin, 133 (2), 183–204. 10.1037/0033-2909.133.2.183. [DOI] [PubMed] [Google Scholar]
- Rodriguez-Díaz CE, Lewellen-Williams C, 2020. Race and racism as structural determinants for emergency and recovery response in the aftermath of hurricanes Irma and Maria in Puerto Rico. Health Equity, 4 (1), 232–238. 10.1089/heq.2019.0103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosellini AJ, Coffey SF, Tracy M, Galea S, 2014. A person-centered analysis of posttraumatic stress disorder symptoms following a natural disaster: Predictors of latent class membership. Journal of Anxiety Disorders, 28 (1), 16–24. 10.1016/j.janxdis.2013.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sautter FJ, Brailey K, Uddo MM, Hamilton MF, Beard MG, Borges AH, 1999. PTSD and comorbid psychotic disorder: Comparison with veterans diagnosed with PTSD or psychotic disorder. Journal of Traumatic Stress, 12 (1), 73–88. 10.1023/A:1024794232175. [DOI] [PubMed] [Google Scholar]
- Sharpe JD, Wolkin AF, 2021. The epidemiology and geographic patterns of natural disaster and extreme weather mortality by race and ethnicity, United States, 1999–2018. Public Health Reports,. 10.1177/00333549211047235, 333549211047235. [DOI] [PMC free article] [PubMed]
- Smith TW (Ed.), 2016. Standard definitions: Final dispositions of case codes and outcome rates for surveys, ninth ed. https://www.aapor.org/Publications-Media/AAPOR-Journals/Standard-Definitions.aspx
- Spitzer RL, Kroenke K, Williams JB, Löwe B, 2006. A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166 (10), 1092–1097. 10.1001/archinte.166.10.1092. [DOI] [PubMed] [Google Scholar]
- Stevanovic D, 2011. Quality of Life Enjoyment and Satisfaction Questionnaire – short form for quality of life assessments in clinical practice: A psychometric study. Journal of Psychiatric and Mental Health Nursing, 18 (8), 744–750. 10.1111/j.1365-2850.2011.01735.x. [DOI] [PubMed] [Google Scholar]
- Tracy M, Norris FH, Galea S, 2011. Differences in the determinants of posttraumatic stress disorder and depression after a mass traumatic event. Depression and Anxiety, 28 (8), 666–675. 10.1002/da.20838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van de Schoot R, Sijbrandij M, Winter SD, Depaoli S, Vermunt JK, 2017. The GRoLTS-Checklist: Guidelines for reporting on latent trajectory studies. Structural Equation Modeling: A Multidisciplinary Journal, 24 (3), 451–467. 10.1080/10705511.2016.1247646. [DOI] [Google Scholar]
- Vermunt JK, 2010. Latent class modeling with covariates: Two improved three-step approaches. Political Analysis, 18 (4), 450–469. 10.1093/pan/mpq025. [DOI] [Google Scholar]
- Weathers FW, Litz BT, Herman DS, Huska JA, Keane TM, 1993. The PTSD checklist (PCL): Reliability, validity and diagnostic utility Proceedings of the 9th Annual Meeting of the International Society for Traumatic Stress Studies, San Antonio TX. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data will be made available on request.