

Abstract
Background
Nursing home residents (NHR) show high rates of polypharmacy. The HIOPP-3-iTBX study is the first cRCT on medication optimization in nursing homes (NH) in Germany. The intervention did not result in a reduction of PIM and/or antipsychotics. This analysis looks at structure quality in the HIOPP-3-iTBX study participants.
Aims
Evaluation of structure quality as part of a cluster-randomized controlled intervention study.
Methods
Structure quality in multiprofessional teams from n = 44 NH (n = 44 NH directors, n = 91 family doctors (FD), and n = 52 pharmacies with n = 62 pharmacists) was assessed using self-designed questionnaires at baseline. Main aspects of the questionnaires related to the qualification of participants, quality management, the medication process and size of the facilities. All completed questionnaires were included. number of PIM/antipsychotics was drawn from the baseline medication analysis in 692 NHR. Data were analyzed by descriptive statistics and mixed model logistic regression.
Results
The presence of a nurse with one of the additional qualifications pain nurse or Zertifiziertes Curriculum (Zercur) Geriatrie in the participating NH was associated with a lower risk for the prescription of PIM/antipsychotics. No association between any characteristic in the other participants at baseline was observed.
Conclusions and discussion
The results support the known role of nursing qualification in the quality and safety of care. Further studies need to look more closely at how use is made of the additional qualifications within the multiprofessional teams. Perspectively, the results can contribute to the development of quality standards in NH in Germany.
Supplementary Information
The online version contains supplementary material available at 10.1007/s40520-023-02513-9.
Keywords: Medication safety, Interprofessional care, Nursing home, Quality management, Antipsychotics, Potentially inappropriate medication
Background
Aging societies worldwide are associated with an increase in the rate of polypharmacy, which is frequently characterized by the concurrent use of five or more medications [1]. The rate of polypharmacy greatly varies from 4% to about 96.5% depending on the age group, definition, healthcare setting, and region studied [2]. Nursing home residents (NHR) show particularly high rates of polypharmacy when compared to older people living at home in international studies, as well as in Germany [3–6]. Polypharmacy is associated with numerous clinical consequences such as higher mortality and an increased risk for adverse drug events (ADEs), falls, and hospitalization [2, 7]. Among the elderly, polypharmacy also increases the risk of receiving potentially inappropriate medications (PIM). PIMs are described as medications which should be avoided in older adults, as detailed on the Beers list of the American Geriatric Society [8] and adapted to the drug markets and prescribing preferences of other countries, e.g., Japan [9], France [10] and Germany [11]. The use of drugs on PIM-lists is associated with a higher risk of ADEs [12, 13] and also mortality [14].
The risk of receiving PIM is also higher in NHR compared to older people living in the community [12]. In addition, PIM are associated with a higher risk of ADEs [15, 16]. Furthermore, approximately 50% of NHR receive antipsychotics which have been associated with cardiovascular events, hip-fractures, and increased all-cause mortality in that group [17–19].
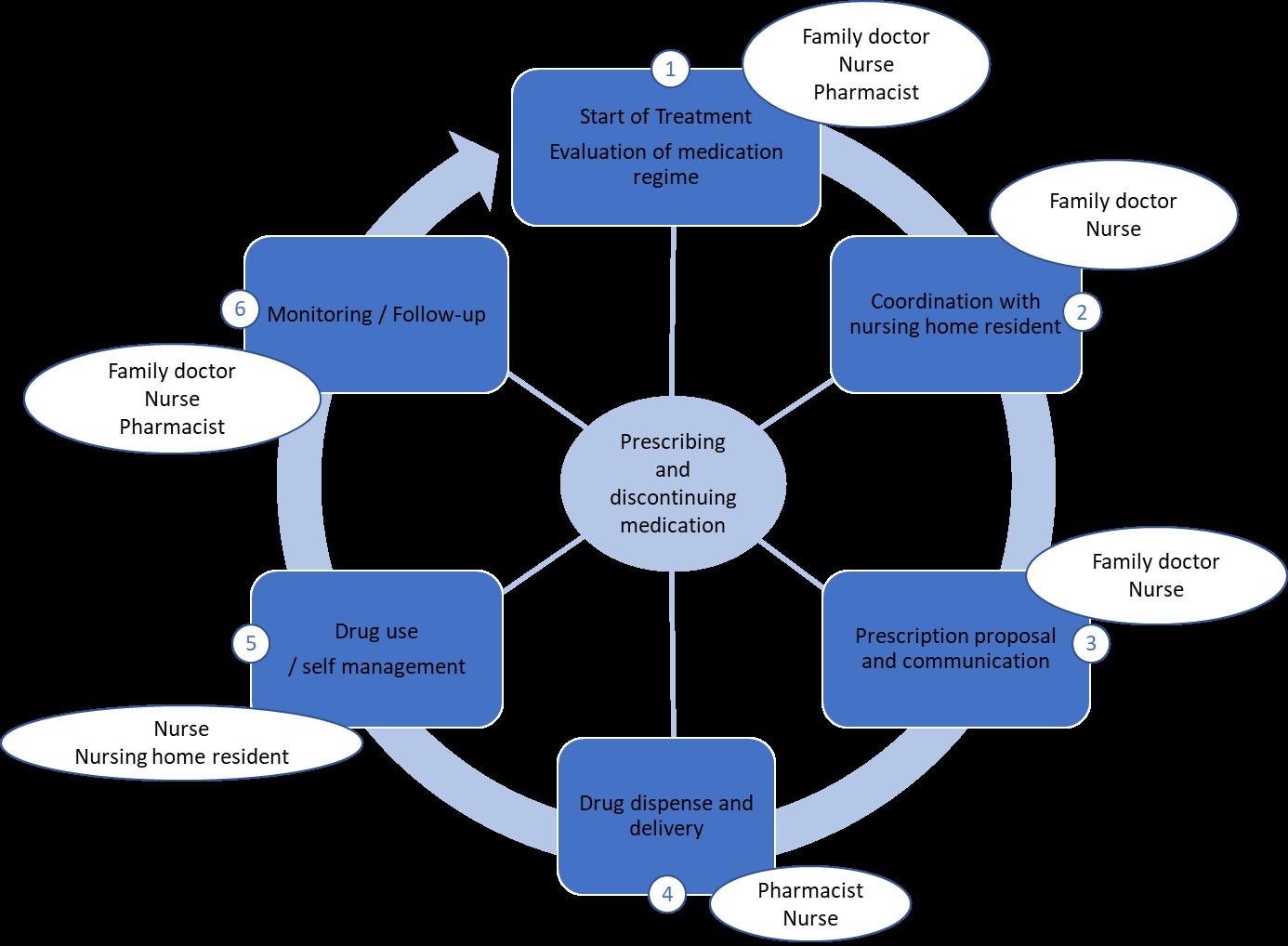
Drug management in NHR is a complex interprofessional six-step process that involves the collaboration of NHR (or their relatives/representatives), physicians (mostly family doctors), nurses, and pharmacists [20]. The six steps of prescribing and discontinuing medication are: evaluation of medication regime, coordination with NHR, prescription proposal, and communication, drug dispense and delivery, drug use, and monitoring/follow-up (see also Fig. 1).
NHR are more likely to get a PIM prescription when collaboration is unstructured [3, 21]. It is known that quality standards such as implemented concepts for person-centered care in nursing homes (NH), concepts for dealing with behavior experienced as challenging and valid standards for pain management influence the number of antipsychotics prescribed [22, 23]. In Germany, there are no interprofessional standards implemented regarding the medication process in NHR. However, according to the German Pharmacy Practice Legislation (§12a ApoG), the delivery of drugs to a NH has to be regulated by a contract between the pharmacy and the NH, and the owner of the pharmacy is obliged to inform nurses and patients about appropriate drug use and risks. In addition, many family doctors (FD) apply quality management standards in their practices. In general, it is known that structured medication management is associated with medication safety in primary care [24]. The German clinical guideline on multimedication in family medicine recommends a structured, planned, and, as far as possible, committing communication between FD, pharmacist, and NH [20] in the care for NHR. Previous studies in German nursing homes show that this recommendation is not implemented in all nursing homes and everyday practice [3, 4]. Since October 2019, an indicator-based quality and audit system for NH has been introduced in Germany. The system includes nursing-sensitive outcome-based indicators of six quality areas, one of which contains the topics of drug therapy and pain management [25]. Nursing-sensitive indicators are defined as criteria for changes in health status that can be affected by nurses directly [26]. In the United States, the percentage of NHR receiving antipsychotic medication is an implemented quality criteria in NH already [27]. A systematic review by Oner et al. showed that there is an inverse relationship between medication administration errors and the proportion of registered nurses in NH, the working environment, and work during night shifts [26]. No significant relationship was shown between ADEs and other nursing-sensitive variables. So far, there are no data available on the relationship between the association of nursing qualification and medication safety and the prescription of PIM/ antipsychotics in particular in German NH.
According to Donabedian, quality of care comprises two main aspects: 1. technical care—meaning the extent to which the provided care maximizes the health benefits of an individual without increasing risk (a valuation that is to be shared between the caregivers and the patient), and 2. the psychosocial interaction between caregiver and receiver [28]. In this concept, it is important to consider three domains of quality: 1. structure quality (comprising quality of the structural factors that affect the performance of care), 2. process quality or the quality of the direct care that the staff provides, and 3. outcome quality including the impact for the individual patient or the health care service outcome of a population.
The HIOPP-3-iTBX study (HIOPP, primary care initiative to optimize patient safety in polypharmacy; iTBX, interprofessional toolbox) is the first cRCT on medication optimization in NH in Germany [29]. In contrast to previous open observational studies, the complex intervention in the HIOPP-3-iTBX study did not lead to a reduction of PIM and/or antipsychotic drugs, nor any improvement in the overall health status of the NHR studied [3, 4]. In line with the model of Donabedian and the new audit guideline for NH in Germany, the analysis of HIOPP-3-iTBX so far has focused on outcome quality [29, 30]. In the present work, the focus of the analysis focuses on aspects of structure quality. The aim of this study, therefore, is to 1. describe structures in the participating professions and institutions, 2. analyze the potential relationship between structures identified and the number of PIM and/or antipsychotic drugs taken by the participating patients in the baseline data of the HIOPP-3-iTBX study.
Methods
HIOPP-3-iTBX study
Between May 2018 and July 2019, a cRCT was conducted in 44 German NH at four study centers (the Institutes for General Practice in Düsseldorf, Hannover, Rostock, and Tübingen; Germany) [29]. Each nursing home formed a cluster in which a multiprofessional team was formed including nurses, pharmacists, and FD serving NHR in that particular NH. The inclusion criterion for the NHR was age ≥ 65 years. The complex intervention addressed all involved professions and comprised a medication review, training of the participants, the implementation of a toolbox, and change management measures. The primary endpoint of the study was the proportion of NHR with at least one PIM and/or at least two antipsychotic drugs 6 months after the intervention [29, 31].
Analyzed data
As a part of the project evaluation, questionnaires addressing structural aspects in HIOPP-3-iTBX study participating FD (n = 91), pharmacists (n = 62), and NH (n = 44) were distributed at baseline. The questionnaires were self-developed within the study team in a consensus process, then pre-tested using cognitive interviews in the analyzed population and subsequently adapted. Main aspects of the questionnaires related to the qualification of participants, work experience, quality management, regulations on the medication process, number of employees in participating facilities, and size of NH/NHR. The number of PIM/antipsychotics taken by participating patients was drawn from the current medication plan of NHR at baseline. The relevant nursing qualifications for the present analysis were: 1. Zercur Geriatrie: developed by the German Geriatrics Association, is an advanced training course that aims to impart interdisciplinary knowledge in the field of geriatrics to nursing professionals, with aspects, such as ethics, palliative care, medication, dementia/depression, and pain. The curriculum comprises up to 180 h (basic qualification) and a total of 520 h of training to become a “Zercur Geriatrics Nursing Specialist”; 2. Pain nurses: nursing professionals with certified advanced training on pain and its management that comprises up to 200 h of training. The curriculum is based on the Pain Therapy Curriculum for Integrated Training and Continuing Education in Nursing of the German Pain Society (DGSS)—Section of the International Association for the Study of Pain (IASP); 3. Geriatric psychiatry: an additional qualification offered in varying amounts of training hours (from about 100 h (basic qualification) up to about 1000 h (advanced specialized training), most curricula include approx. 600 h).
In the present analysis, all completed questionnaires by participating nursing home directors, FDs, and pharmacists at baseline were included.
Statistical methods
Descriptive results are presented as absolute frequencies and percentages or as mean ± standard deviation (SD). To evaluate the association of different factors with the proportion of NHR receiving a PIM/antipsychotic at baseline, a mixed model logistic regression was applied. In the logistic regression model data from n = 786 of the n = 787 NHR in the baseline examination (99.8%) were included. Accounting for the cluster effect of the NH, their identification code was included as a random effect in the model. The fixed factors in the model were: additional qualifications in nurses (gerontopsychiatry, pain nurse, palliative care, wound expert, Zertifiziertes Curriculum (Zercur) Geriatrie and others), the presence of a concept for dealing with challenging behavior in NHR (yes/no), the presence of a concept for avoiding measures that deprive patients of their freedom (yes/no), number of drugs and number of comorbidities. Age, gender, and dementia status of the NHR were included as adjusting factors. All analyses were performed with SPSS® Version 27 and StataSE Version 16.
Results
In the HIOPP-3 iTBX study, n = 44 NH directors, n = 91 FDs, and n = 52 pharmacies with n = 62 pharmacists participated. Structure quality data from all FDs and NHs provided by their directors, and n = 50 (95%) pharmacies and n = 59 pharmacists (95%) was analyzed. Descriptive data of NHR and NH can be found in Tables 1 and 2, data of FDs and pharmacists in Tables 4 and 5 in the supplement. Association of potential influencing variables of NHR, NH structures, and the prescription of PIM/antipsychotics can be found in Table 3. Additional qualifications of nursing staff were asked about as characteristics of the NH (see Table 2). On average, between 2 and 3 of the five additional qualifications surveyed were available in the 44 participating NH. Most often were palliative care (n = 31), gerontopsychiatry (n = 26), and wound management (n = 25). Pain nurse qualification was available in 7 NH and Zercur Geriatrie in 2 NH.
Table 1.
Sociodemographic characteristics of nursing home residents (NHR, n = 787) at baseline (T0)
| Ø Age in years (SD) | 84.3 (± 7.9) |
| Sex (female, %) | 73.8 (n = 581) |
| NHR with legal guardianship, % | 35.5 (n = 254)1 |
| NHR educational statusa, % | |
| Low | 45.4 (n = 357) |
| Medium | 30.5 (n = 240) |
| High | 7.5 (n = 59) |
| Not specified | 16.6 (n = 131) |
| Nursing home stay in months (median, IQA) | 29 (13–53) |
| NHR care level, % | |
| None | 0.4 (n = 3) |
| 1 and 2 | 22.0 (n = 173) |
| 3 and 4 | 64.7 (n = 508) |
| 5 | 12.6 (n = 99) |
| Not specified | 0.3 (n = 2) |
| Ø Number of diagnoses (SD) | 7.4 (± 3.5) |
| Barthel Index NHR (ICD-Code U50.0–50), % | |
| None, mild (U50.0–10) | 17.5 (n = 137) |
| Moderate, moderately severe (U50.20–30) | 44.4 (n = 348) |
| Severe, very severe (U50.40–50) | 38.1 (n = 299) |
| NHR with sign of dementiab, % | 64.5 (n = 507) |
| Ø number of drugs prescribed (SD) | 11.1 (± 4.5) |
| NHR with ≥ 1 PIM and/or ≥ 2 antipsychotics, % | 41.3 (n = 325) |
NHR nursing home resident; PIM potentially inadequate medication; Ø average; SD standard deviation, % percentage NHR
aEducational status according to CASMIN[32]
bSign of dementia: identified by the nursing home or family physician
Table 2.
Characteristics of nursing homes (NH, n = 44)
| NH provider (%) | |
| Private | 29.5 (n = 13) |
| Public (e.g., Municipal sponsorship) | 6.8 (n = 3) |
| Non-profit (e.g., Red cross, welfare organization) | 63.6 (n = 28) |
| Qualification of NH director (%) | |
| Advanced training | 34.1 (n = 15) |
| Bachelor degree | 2.3 (n = 1) |
| Diploma degree | 36.4 (n = 16) |
| Master degree | 11.4 (n = 2) |
| Other | 4.5 (n = 2) |
| Not specified | 11.4 (n = 5) |
| Qualification head of nursing service (%) | |
| Advanced training | 88.6 (n = 39) |
| Bachelor degree | 2.3 8(n = 1) |
| Diploma degree | 4.5 (n = 2) |
| Master degree | 2.3 (n = 1) |
| Other | 2.3 (n = 1) |
| Type of record of care (%) | |
| Paper-based | 11.4 (n = 5) |
| Electronic | 63.6 (n = 28) |
| Combination of paper-based and electronic | 25.0 (n = 11) |
| Number of pharmacies associated with NH (%) | |
| 1 | 75.0 (n = 33) |
| 2 | 20.5 (n = 9) |
| 3 | 4.5 (n = 2) |
| Ø Family doctors per NH (SD) | 9.76 (± 6.55). min/max 1/35 |
| Ø Rate of specialized staff (%, SD) | 53.02 (± 6.02). min/max 33/70 |
| Additional qualification of nursing staff (%) | |
| Geriatric psychiatry | 59.1 (n = 26) |
| Pain nurse | 15.9 (n = 7) |
| Palliative care | 70.5 (n = 31) |
| Wound management | 56.8 (n = 25) |
| Zercur Geriatrie | 4.5 (n = 2) |
| Other | 40.9 (n = 18) |
| Concept challenging behavior among NHR (%) | |
| None | 34.1 (n = 15) |
| Based on the framework recommendation on dementiaa | 36.4 (n = 16) |
| Other | 20.5 (n = 9) |
| Yes, not specified | 4.5 (n = 2) |
| Not specified | 4.5 (n = 2) |
| Concept avoidance of measures involving deprivation of liberty (%) | |
| None | 13.6 (n = 6) |
| Redufixb | 6.8 (n = 3) |
| Werdenfelser wayc | 50.0 (n = 22) |
| Other | 25.0 (n = 11) |
| Yes, not specified | 4.5 (n = 2) |
| Quality management representative (%) | 95.5 (n = 42) |
| Quality management system in use (%) | |
| None | 2.3 (n = 1) |
| DIN/ISO | 29.5 (n = 13) |
| Other | 38.6 (n = 17) |
| Yes, not specified | 20.5 (n = 9) |
| Not specified | 9.1 (n = 4) |
Table 3.
Association of potential influencing variables of NHR, NH structures, and the prescription of PIM/antipsychotics in n = 786 NHR, results of a mixed model logistic regression
| Variable (reference) | OR (95% CI) | P value |
|---|---|---|
| Sociodemographics of participating patients | ||
| Age | 0.99 (0.97–1.01) | 0,453 |
| Female sex | 1.20 (0.82–1.76 | 0,351 |
| Dementia diagnosed | 1.98 (1.40–2.80) | 0,000 |
| Additional qualification of nursing staff | ||
| Gerontopsychiatry | 1.35 (0.85–2.13) | 0,200 |
| Pain nurse | 0.55 (0.33–0.91) | 0,020 |
| Palliative care | 1.07 (0.70–1.65) | 0,752 |
| Wound manager | 1.28 (0.86–1.92) | 0,230 |
| Zercur geriatrics | 0.30 (0.12–0.71) | 0,006 |
| Other | 0.80 (0.52–1.23) | 0,302 |
| Nursing concepts regarding | ||
| Challenging behavior among nursing home residents | 0.83 (0.54–1.29) | 0,412 |
| Avoidance of measures involving deprivation of liberty | 1.21 (0.67–2.19) | 0,527 |
| Further aspects | ||
| Number of drugs | 1.15 (1.10–1.20) | 0,000 |
| Number of comorbidities | 0.98 (0.93–1.03) | 0,338 |
OR odds ratio; 95% CI 95% confidence interval
Regression analysis showed that at baseline a higher number of PIM/antipsychotics was associated with the presence of dementia in the NHR (OR: 1.70; 95% CI 1.23–2.34; p = 0.001). On the NHR level analysis the presence of a nurse with one of the additional qualifications pain nurse or Zertifiziertes Curriculum (Zercur) Geriatrie in the participating NH showed a statistically significant association to a lower risk for the prescription of PIM/antipsychotics (pain nurse OR: 0.59; 95% CI 0.35–0.96, p = 0.044 Zercur; OR 0.21; 95% CI 0.09–0.51; p = 0.001). No association between any characteristic in FDs and pharmacies/pharmacists and the number of PIM/antipsychotics prescribed at baseline was observed.
Discussion
To our knowledge, HIOPP-3-iTBX is the first randomized study to investigate structures, processes, and outcomes of an interprofessional medication management in NH in Germany. The complex intervention in HIOPP-3-iTBX did not lead to a reduction of PIM and/or antipsychotics in the participating NHR [29]. In this analysis, the focus is on aspects of structure quality and their possible effects on the prescription of PIM/antipsychotics in NHR at baseline of the HIOPP-3-iTBX study. In our study, the structural parameters collected from FD and pharmacists had no effects. We focused, therefore, on the qualification of nurses rather than the involvement of pharmacists, of which the latter has been shown as a success factor in other studies [36, 37].
The analysis showed that dementia in NHR and number of drugs were associated with a higher risk for the prescription of PIM/antipsychotics. Specific additional nursing qualifications regarding pain and geriatrics (ZERCUR GERIATRIE) were associated with a lower risk for the prescription of PIM/antipsychotics. No further associations to any of the study participant's characteristics (NHR, FD, and pharmacists) or their qualifications were found. The results show that the qualification of the nursing staff influences medication safety in the studied NH.
Previous work shows that higher qualification of nursing professionals is associated with improved patient outcomes [38, 39]. Regression analysis did not show a significant correlation between nurses' additional qualification in gerontopsychiatry and a higher risk for the prescription of PIM/antipsychotics to participating patients. Currently, it is not obligatory to have nurses with either one of the described advanced training in teams in NH in Germany. However, pain is a relevant issue in geriatrics. Inadequate pain management is known to be a frequent quality problem in NH leading to agitation and the prescription of antipsychotics as a consequence [40, 41]. Furthermore, the experience of pain is commonly associated with cognitive impairment [42–47]. Appropriate analgesia may reduce pain and its associated cognitive impairment. The lack of sensitivity of the medical staff in recognizing pain based on non-verbal cues/pain-related behavior in people suffering from cognitive impairment is a known cause of suboptimal pain management in this population [48, 49]. Untreated pain is considered to be one of the causes of challenging behavior, such as agitation or aggression in people with dementia [50]. On the other hand, in some cases, cognitive impairment may worsen under analgesic medication [51, 52]. Interprofessional collaboration in medication management, therefore, is necessary for the management of pain in NHR. Nurses can make a significant contribution here. Namely, the contribution comprises managing and monitoring patients’ medication and possible ADEs. Interprofessional medication management with the participation of FD (and possibly other specialized doctors), pharmacists, and nurses comprises the aspects named before. A model of an interprofessional medication process is shown in Fig. 1. Ideally, nurses are involved in all of the six steps. For example, nurses play an important role in tapering antipsychotics. The process of tapering, e.g., antipsychotics, should take place over a period of 2–8 weeks and requires good observation of the reaction of the NHR by nurses [53].
However, interprofessional cooperation means more than just the sum of tasks distributed among different disciplines. It is a model of collaboration between different healthcare providers in which the different professional groups have an awareness of the competencies and different roles of the other team members and are aware of a common goal for the patient (patient-centeredness) [54]. Both advanced trainings Zercur geriatrie and pain nurse were in our analysis found to be associated with a lower rate of PIM/antipsychotics in the NHR. Both trainings also comprise the knowledge and competencies named earlier, including aspects of interprofessional collaboration. Studies so far show that staff level and staff training have an impact on the reduction of inappropriate prescribing of antipsychotics in people with dementia [55]. One study showed that it is often nurses that initiate the prescription of antipsychotics in NHR [41]. Furthermore, it is known from the literature that applying this nursing-specific knowledge improves patient outcomes, including pain, and aggression. However, little is known about the exact relationships between certain skill levels, the nurse staffing ratio, and patient outcomes in NH [26]. Our results further support the initiatives to train nurses in their role in medication management specifically [56]. In Germany, a structured interprofessional study program on drug therapy safety needs analysis and design of a model curriculum (SINA) was developed [57]. It will be of interest to evaluate how this interprofessional training on drug therapy affects medication safety in nursing home care and the contribution of the different professions, as one focus of SINA is the role of pharmacists within interprofessional teams.
To summarize, our results emphasize the importance of nursing quality and qualifications for patient safety in NH.
Limitation
Only a few nurses in the HIOPP-3-iTBX study had one of the additional qualifications Pain Nurse (n = 7) or Zercur Geriatrie (n = 2); however, on the NHR-level analysis, these nursing qualifications and the rate of NHR with PIM/antipsychotics show a statistically significant association. As a limitation, it is to be mentioned that the exact number of hours of the advanced training course present in the different nurses was not asked for. Based on the present data, it is unclear why the additional qualification gerontopsychiatry is not associated with the rate of PIM/ antipsychotics. However, in four of the seven NH with pain nurses there was a nurse with additional qualification in gerontopsychiatry, just like in one of the two NH with a nurse qualified according to Zercur Geriatrics.
Data from the HIOPP-3-iTBX study does not allow for a description more detailed how the trained nursing professionals apply their knowledge in daily care. In addition, there is no data on whether the presence of nurses with additional qualifications changes the medication processes related to the prescription of PIM/ antipsychotics. Possible hypotheses are that the NH with specialized nurses are more innovative overall with possible side-effects such as more in-house training and case discussions or different attitudes towards interprofessional cooperation. This aspect needs to be investigated in further studies. Therefore, important information to undermine the findings is lacking. A further limitation could be an unintended selection bias: it is hard to rule out that NH, pharmacists, and FDs with a high interest in the topic participated in the study.
Conclusions
Medication management in NH is an interprofessional and complex task. The results of this analysis of the HIOPP-3-iTBX study support the known role of nursing qualification in the quality and safety of care. The analysis showed that advanced training in the field of pain and geriatrics in nursing professionals was associated with lower rates of PIM/antipsychotics in NHR at baseline of the HIOPP-3-iTBX study [20].
Based on the results, further studies should examine the effect of additional nursing qualifications in German NH more closely (e.g., number of qualified staff in NH, extent of qualification, collaboration/role within nursing team). Moreover, further studies are important to evaluate the role of advanced trained nurses in the medication process with a focus on the initiation of a prescription and its evaluation regarding PIMs and antipsychotics, especially in nursing teams in Germany. As quality standards for German NH are under development, the present and future studies can perspectively contribute to their development and introduction.
Supplementary Information
Below is the link to the electronic supplementary material.
{kind=link}
Acknowledgements
We would like to thank all participating NH as well as participating NHR and their careers. We would also like to thank all nursing staff in the homes, as well as all nursing services, FDs, medical assistants, and pharmacists for their participation.
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was funded by the Innovation Fund of the Joint Federal Committee (Grant No.: 01VSF16017). The study was registered in the German Register of Clinical Trials (DRKS00013588).
Declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
The Ethics Committee of the Hannover Medical University approved the Masters Ethics Application (No. 7655).
Statement of human and animal rights
This study was performed in line with the principles of the Declaration of Helsinki and results are reported in regard of the CONSORT Statement. The Medical Research Council (MRC) Guideline “Developing and evaluating complex interventions—new guidance” was applied in the intervention development.
Informed consent
Informed consent was obtained from all individual participants included in the study or their legal guardians.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Khezrian M, McNeil CJ, Murray AD, et al. An overview of prevalence, determinants and health outcomes of polypharmacy. Ther Adv Drug Saf. 2020;11:2042098620933741. doi: 10.1177/2042098620933741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pazan F, Wehling M. Polypharmacy in older adults: a narrative review of definitions, epidemiology and consequences. Eur Geriatr Med. 2021;12:443–452. doi: 10.1007/s41999-021-00479-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jaehde U, Thürmann PA. Medication safety in nursing homes. Z Evid Fortbild Qual Gesundhwes. 2012;106:712–716. doi: 10.1016/j.zefq.2012.10.021. [DOI] [PubMed] [Google Scholar]
- 4.Jaehde U, Thürmann P. Arzneimitteltherapiesicherheit bei Heimbewohnern. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2018;61:1111–1118. doi: 10.1007/s00103-018-2796-x. [DOI] [PubMed] [Google Scholar]
- 5.Onder G, Liperoti R, Fialova D, et al. Polypharmacy in nursing home in Europe: results from the SHELTER study. J Gerontol A Biol Sci Med Sci. 2012;67:698–704. doi: 10.1093/gerona/glr233. [DOI] [PubMed] [Google Scholar]
- 6.Hoffmann F, Schmiemann G, Dörks M. Untersuchungen zu Polypharmazie: Eine Frage der Definition und der verwendeten Daten. Z Evid Fortbild Qual Gesundhwes. 2016;113:27–35. doi: 10.1016/j.zefq.2016.03.004. [DOI] [PubMed] [Google Scholar]
- 7.Mosshammer D, Haumann H, Morike K, et al. Polypharmacy-an upward trend with unpredictable effects. Deutsch Arzteblatt Int. 2016;113:627–633. doi: 10.3238/arztebl.2016.0627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.By the American Geriatrics Society Beers Criteria Update Expert P American Geriatrics Society 2019 updated AGS Beers Criteria(R) for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67:674–694. doi: 10.1111/jgs.15767. [DOI] [PubMed] [Google Scholar]
- 9.Kojima T, Mizukami K, Tomita N, et al. Screening tool for older persons' appropriate prescriptions for Japanese: report of the Japan Geriatrics Society Working Group on “Guidelines for medical treatment and its safety in the elderly”. Geriatr Gerontol Int. 2016;16:983–1001. doi: 10.1111/ggi.12890. [DOI] [PubMed] [Google Scholar]
- 10.Roux B, Berthou-Contreras J, Beuscart JB, et al. Review of potentially inappropriate medication pr[e]scribing in seniors (remedi[e]s): French implicit and explicit criteria. Eur J Clin Pharmacol. 2021;77:1713–1724. doi: 10.1007/s00228-021-03145-6. [DOI] [PubMed] [Google Scholar]
- 11.Holt S, Schmiedl S, Thurmann PA. Potentially inappropriate medications in the elderly: the PRISCUS list. Deutsch Arzteblatt Int. 2010;107:543–551. doi: 10.3238/arztebl.2010.0543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Endres HG, Kaufmann-Kolle P, Steeb V, et al. Association between potentially inappropriate medication (PIM) use and risk of hospitalization in older adults: an observational study based on routine data comparing PIM use with use of PIM alternatives. PLoS ONE. 2016;11:e0146811. doi: 10.1371/journal.pone.0146811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Xing XX, Zhu C, Liang HY, et al. Associations between potentially inappropriate medications and adverse health outcomes in the elderly: a systematic review and meta-analysis. Ann Pharmacother. 2019;53:1005–1019. doi: 10.1177/1060028019853069. [DOI] [PubMed] [Google Scholar]
- 14.Heider D, Matschinger H, Meid AD, et al. Health service use, costs, and adverse events associated with potentially inappropriate medication in old age in Germany: retrospective matched cohort study. Drugs Aging. 2017;34:289–301. doi: 10.1007/s40266-017-0441-2. [DOI] [PubMed] [Google Scholar]
- 15.Hedna K, Hakkarainen KM, Gyllensten H, et al. Potentially inappropriate prescribing and adverse drug reactions in the elderly: a population-based study. Eur J Clin Pharmacol. 2015;71:1525–1533. doi: 10.1007/s00228-015-1950-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cullinan S, O'Mahony D, O'Sullivan D, et al. Use of a frailty index to identify potentially inappropriate prescribing and adverse drug reaction risks in older patients. Age Ageing. 2016;45:115–120. doi: 10.1093/ageing/afv166. [DOI] [PubMed] [Google Scholar]
- 17.Richter T, Mann E, Meyer G, et al. Prevalence of psychotropic medication use among German and Austrian nursing home residents: a comparison of 3 cohorts. J Am Med Dir Assoc. 2012;13:187e7–187e13. doi: 10.1016/j.jamda.2011.03.007. [DOI] [PubMed] [Google Scholar]
- 18.Bakken MS, Schjøtt J, Engeland A, et al. Antipsychotic drugs and risk of hip fracture in people aged 60 and older in Norway. J Am Geriatr Soc. 2016;64:1203–1209. doi: 10.1111/jgs.14162. [DOI] [PubMed] [Google Scholar]
- 19.Liperoti R, Sganga F, Landi F, et al. Antipsychotic drug interactions and mortality among nursing home residents with cognitive impairment. J Clin Psychiatry. 2017;78:e76–e82. doi: 10.4088/JCP.15m10303. [DOI] [PubMed] [Google Scholar]
- 20.Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF) e. V. (2021) Hausärztliche Leitlinie: Multimedikation. https://www.awmf.org/leitlinien/detail/ll/053-043.html. Accessed 20 Dec 2022
- 21.Fleischmann N, Geister C, Hoell A, et al. Interprofessional collaboration in nursing homes (interprof): a grounded theory study of nurse experiences of general practitioner visits. Appl Nurs Res. 2017;35:118–125. doi: 10.1016/j.apnr.2017.02.021. [DOI] [PubMed] [Google Scholar]
- 22.Deutsches Netzwerk für Qualitätsentwicklung in der Pflege (2020) Expertenstandard Schmerzmanagement in der Pflege. Aktualisierte Version. https://www.dnqp.de/fileadmin/HSOS/Homepages/DNQP/Dateien/Expertenstandards/Schmerzmanagement_2020/Schmerz-Akt2020_Auszug.pdf. Accessed 28 Nov 2022
- 23.Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde (DGPPN), Deutsche Gesellschaft für Neurologie (DGN) (2016) S3-Leitlinie „Demenz“. https://www.awmf.org/uploads/tx_szleitlinien/038-013l_S3-Demenzen-2016-07.pdf. Accessed 28 Nov 2022
- 24.Mahler C, Freund T, Baldauf A, et al. Structured medication management in primary care - a tool to promote medication safety. Z Evid Fortbild Qual Gesundhwes. 2014;108:258–269. doi: 10.1016/j.zefq.2013.07.011. [DOI] [PubMed] [Google Scholar]
- 25.Medizinischer Dienst Bund (2022) Qualitätsprüfungen von Pflegeeinrichtungen. https://md-bund.de/themen/pflegequalitaet/qualitaetspruefungen.html. Accessed 8 July 2022
- 26.Oner B, Zengul FD, Oner N, et al. Nursing-sensitive indicators for nursing care: a systematic review (1997–2017) Nurs Open. 2021;8:1005–1022. doi: 10.1002/nop2.654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Centers for Medicare & Medicaid Services (CMS) (2022) Quality measures. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/NHQIQualityMeasures. Accessed 30 July 2022
- 28.Donabedian A, Bashur R. An introduction to quality assurance in health care. New York: Oxford University Press; 2003. p. 2003. [Google Scholar]
- 29.Junius-Walker U, Krause O, Thürmann P, et al. Drug safety for nursing-home residents-findings of a pragmatic, cluster-randomized, controlled intervention Trialin 44 nursing homes. Deutsch Arzteblatt Int. 2021;118:705–712. doi: 10.3238/arztebl.m2021.0297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bund MDdS, (MDS) dKeV (2019) Richtlinien des GKV-Spitzenverbandes für die Qualitätsprüfung in Pflegeeinrichtungen nach § 114 SGB XI. Vollstationäre Pflege 2019. Available from https://md-bund.de/suchergebnis.html?tx_solr%5Bq%5D=Pr%C3%BCfbogen
- 31.Kirsch C, Doyle I-M, Krause O, et al. Lessons learned: challenges faced in the recruitment process for the cluster-randomized nursing home study HIOPP-3 iTBX. Z Evid Fortbild Qual Gesundhwes. 2020;156:24–32. doi: 10.1016/j.zefq.2020.07.002. [DOI] [PubMed] [Google Scholar]
- 32.Lüttinger P, König W. Die Entwicklung einer international vergleichbaren Klassifikation für Bildungssysteme. ZUMA Nachrichten. 1988;12:14. [Google Scholar]
- 33. Bundesministerium für Gesundheit (2006) Rahmenempfehlungen zum Umgang mit herausforderndem Verhalten bei Menschen mit Demenz in der stationären Altenhilfe. https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/Publikationen/Pflege/Berichte/Bericht_Rahmenempfehlungen_zum_Umgang_mit_herausforderndem_Verhalten_bei_Menschen_mit_Demenz_in_der_stationaeren_Altenhilfe.pdf. Accessed 15 Nov 2022
- 34.Branitzki S. Redu-Fix—a model for reducing physical restraint: protecting nursing home residence from mobility limitations. Pflege Z. 2007;60:84–87. [PubMed] [Google Scholar]
- 35.Wassermann J, Kirsch S (2022) Werdenfelser Weg [19.09.2022]. https://www.werdenfelser-weg-original.de
- 36.Gray SL, Hart LA, Perera S, et al. Meta-analysis of interventions to reduce adverse drug reactions in older adults. J Am Geriatr Soc. 2018;66:282–288. doi: 10.1111/jgs.15195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Mucherino S, Casula M, Galimberti F, et al. (2022) The effectiveness of interventions to evaluate and reduce healthcare costs of potentially inappropriate prescriptions among the older adults: a systematic review. Int J Environ Res Public Health. 2022;19:6724. doi: 10.3390/ijerph19116724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Ewers M, Lehmann Y. Hochschulisch qualifizierte Pflegende in der Langzeitversorgung?! In: Jacobs K, Kuhlmey A, Greß S, Klauber J, Schwinger A, editors. Pflege-Report 2019: Mehr Personal in der Langzeitpflege - aber woher? Berlin Heidelberg: Springer; 2020. pp. 167–177. [Google Scholar]
- 39.Basinska K, Wellens NIH, Simon M, et al. Registered nurses in expanded roles improve care in nursing homes: Swiss perspective based on the modified Delphi method. J Adv Nurs. 2021;77:742–754. doi: 10.1111/jan.14644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Toles M, Colón-Emeric C, Moreton E, et al. Quality improvement studies in nursing homes: a scoping review. BMC Health Serv Res. 2021;21:803. doi: 10.1186/s12913-021-06803-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Schwinger A, Behrendt S, Tsiasioti C, et al. Qualitätsmessungmit Routinedaten in deutschen Pflegeheimen: Eine erste Standortbestimmung. Pflege-Report 2018. Berlin: Springer; 2018. pp. 97–122. [Google Scholar]
- 42.Pergolizzi JV, Raffa RB, Paladini A, et al. Treating pain in patients with dementia and the possible concomitant relief of symptoms of agitation. Pain Manage. 2019;9:569–582. doi: 10.2217/pmt-2019-0024. [DOI] [PubMed] [Google Scholar]
- 43.Cravello L, Di Santo S, Varrassi G, et al. Chronic pain in the elderly with cognitive decline: a narrative review. Pain Ther. 2019;8:53–65. doi: 10.1007/s40122-019-0111-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Moreira SA, Novak P. Effects of pain on cognitive function and mobility. J Clin Trials. 2019;11:1–10. [Google Scholar]
- 45.Berryman C, Stanton TR, Jane Bowering K, et al. Evidence for working memory deficits in chronic pain: a systematic review and meta-analysis. Pain. 2013;154:1181–1196. doi: 10.1016/j.pain.2013.03.002. [DOI] [PubMed] [Google Scholar]
- 46.Landrø NI, Fors EA, Våpenstad LL, et al. The extent of neurocognitive dysfunction in a multidisciplinary pain centre population. Is there a relation between reported and tested neuropsychological functioning? Pain. 2013;154:972–977. doi: 10.1016/j.pain.2013.01.013. [DOI] [PubMed] [Google Scholar]
- 47.van der Leeuw G, Ayers E, Leveille SG, et al. The effect of pain on major cognitive impairment in older adults. J Pain. 2018;19:1435–1444. doi: 10.1016/j.jpain.2018.06.009. [DOI] [PubMed] [Google Scholar]
- 48.Rekatsina M, Paladini A, Viswanath O, et al. Opioids in the elderly patients with cognitive impairment: a narrative review. Pain Ther. 2022;11:381–394. doi: 10.1007/s40122-022-00376-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Liu JYW, Leung DYP. Pain treatments for nursing home residents with advanced dementia and substantial impaired communication: a cross-sectional analysis at baseline of a cluster randomized controlled trial. Pain Med. 2016;18:1649–1657. doi: 10.1093/pm/pnw242. [DOI] [PubMed] [Google Scholar]
- 50.Manietta C, Labonté V, Thiesemann R, et al. Algorithm-based pain management for people with dementia in nursing homes. Cochrane Database System Rev. 2022 doi: 10.1002/14651858.CD013339.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Wegier P, Varenbut J, Bernstein M, et al. “No thanks, I don’t want to see snakes again”: a qualitative study of pain management versus preservation of cognition in palliative care patients. BMC Palliat Care. 2020;19:182. doi: 10.1186/s12904-020-00683-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Wong G. Pharmacological management of chronic non-cancer pain in frail older people. Aust Prescr. 2022;45:2–7. doi: 10.18773/austprescr.2022.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Hager K, Krause O. Neuroleptika bei Demenzpatienten? Absetzversuch lohnt sich! Der Allgemeinarzt. 2017;17:24–28. [Google Scholar]
- 54.Tsakitzidis G, Anthierens S, Timmermans O, et al. Do not confuse multidisciplinary task management in nursing homes with interprofessional care! Prim Health Care Res Dev. 2017;18:591–602. doi: 10.1017/S146342361700024X. [DOI] [PubMed] [Google Scholar]
- 55.Thompson Coon J, Abbott R, Rogers M, et al. Interventions to reduce inappropriate prescribing of antipsychotic medications in people with dementia resident in care homes: a systematic review. J Am Med Dir Assoc. 2014;15:706–718. doi: 10.1016/j.jamda.2014.06.012. [DOI] [PubMed] [Google Scholar]
- 56.Dijkstra NE, De Baetselier E, Dilles T, et al. Developing a competence framework for nurses in pharmaceutical care: a Delphi study. Nurse Educ Today. 2021;104:104926. doi: 10.1016/j.nedt.2021.104926. [DOI] [PubMed] [Google Scholar]
- 57.Jaehde U (2020) Strukturiertes interprofessionelles Studienangebot zur Arzneimitteltherapiesicherheit: Bedarfsanalyse und Konzeption eines Mustercurriculums (SINA): Abschlussbericht zum BMG-geförderten Forschungsvorhaben: Pharmazeutisches Insitut, Rheinische Friedrich-Wilhelms-Universität Bonn [20.12.2022]. https://www.zem.uni-bonn.de/news/abschlussbericht-201estrukturiertes-interprofessionelles-studienangebot-zur-arzneimitteltherapiesicherheit-sina-201c
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.