

Abstract
Education is protective against cognitive impairment. We used nationally representative data from Mexico and Brazil to assess the association between education and cognitive function. The sample included adults ≥ 50 years from the Brazilian Longitudinal Study of Aging (ELSI) and the Mexican Health and Aging Study (MHAS). Participants were classified as cognitively impaired or not impaired. We used logistic regression models to estimate the association between education and cognitive function. Education level was higher in MHAS than in ELSI. Participants with at least 1 year of education were less likely to have cognitive impairment than those with no formal education in both cohorts. Men in ELSI had higher odds for cognitive impairment compared to men in MHAS. In both cohorts, higher educational level was associated with lower odds of cognitive impairment compared to no formal education. Sex was an effect modifier in MHAS but not in ELSI.
HIGHLIGHTS
Cognitive test batteries were harmonized using a regression‐based approach.
Even very low levels of education were associated with reduced odds of cognitive impairment compared to no formal education.
Brazilians were more likely to have cognitive impairment than Mexicans given the same education level.
The differences in the association of education with cognition between Brazil and Mexico were only observed among men.
Keywords: cognition, ELSI, harmonization, MHAS, sex differences
1. INTRODUCTION
The estimated number of people living with dementia will triple by 2050, increasing from 57.4 million to 153 million. 1 Currently, 58.0% of people living with dementia live in low‐ to middle‐income countries (LMIC), and this prevalence is expected to reach 68.0% in 2050. 2 Latin America (LA) is the region with the highest burden of dementia worldwide, with a prevalence of 8.5%. 3 Currently, there is no available treatment for dementia. 4 However, it is estimated that 40% of dementia cases could be prevented or delayed by controlling 12 modifiable risk factors. 4 Low education was the most important risk factor for dementia in LA, with 7.7% of dementia cases attributable to lower education in Brazil and 13.5% in Mexico. 5 , 6
Cognitive reserve refers to the ability of the cognitive processes to withstand brain insult with little or no loss in performance. 7 Cognitive reserve is built over the life course through dynamic processes as a consequence of exposure to education, occupation, and leisure‐time activities. 7 Education is an early surrogate marker of cognitive reserve and is a predictor of better cognitive performance both in early and middle ages, and higher educational attainment is a protective factor against cognitive decline and dementia. 8 , 9 In a previous study that included several LMICs, low educational attainment was associated with higher incidence of dementia. 10 Additionally, results from Mexico have shown that there is a sex gap in education, with women achieving lower educational attainment than men. 11 However, few studies on this topic were conducted in LA. Most research on education and cognitive function has been conducted in high‐income countries, where the average years of education are higher (≥12 years) and the education quality is more homogeneous than in LMIC. 12 , 13 In 2019, the average years of education for adults aged ≥ 25 years was 8.0 in Brazil and 8.8 in Mexico. 14 In 1970, 33.7% of people ≥ 15 years in Brazil and 25.8% in Mexico were illiterate. 15 , 16 In 2000, following the world trend, these numbers had lowered to 13.6% in Brazil and 9.5% in Mexico. 15 , 16 , 17 While in Brazil the percentage of illiteracy is similar in both sexes (12.3% for women and 12.4% for men), in Mexico illiteracy is higher in women (11.3%) than in men (7.4%). 15 , 16 Education quality is also a relevant issue for older adults in LA. For example, Brazilian older adults that report higher education (for example, those completing middle and high school), may have a literacy return below the expected for that level of education. Brazilian national data indicate that 49.0% of adults ≥ 50 years are likely to be functionally illiterate and 35.0% have an elementary school literacy level. 18 The same is true for Mexico, where 50.0% of adults aged 16 to 65 years have functional illiteracy, with similar levels in other Latin American countries, such as Chile, Ecuador, and Peru. 19
RESEARCH IN CONTEXT
Systematic review: Education is a predictor of better cognitive performance and is protective against dementia according to studies from high‐income countries.
Interpretation: Using nationally representative samples from Brazil and Mexico, we found that even low levels of education (1–4 years) were associated with lower odds of cognitive impairment. Brazilian men had higher odds of cognitive impairment than Mexican men, in all education levels.
Future directions: Other studies from low‐ and middle‐income countries focusing on education quality and sex differences are needed to understand the benefits of education on cognitive function in these settings.
Given the lower levels of education in LA and the heterogeneous quality of education for older adults, the protective effect of education on cognition may differ in these countries. Thus, it is important to investigate the association of education in LA to extend the findings of previous studies. Brazil and Mexico are the largest countries of LA and, despite differences in language and cultural heritage, they have faced similar societal challenges, such as high prevalence of illiteracy, historical sex inequality in access to education, and low quality of education. 15 , 16 , 17 Furthermore, there is a 200% expected increase in dementia cases in Brazil and Mexico from 2019 to 2050, which are the largest contributors to the dementia burden in LA. Although previous studies with convenience samples have investigated the association between education and cognitive performance in these countries, no study to date has investigated this association in a sample representative of older adults in Brazil and Mexico. 10 , 11 Therefore, we aimed to investigate the association between educational attainment and cognitive performance in older adults using two nationally representative LMIC samples, Brazil (n = 9412) and Mexico (n = 14,779).
2. METHODS
2.1. Study samples
We used data from two Health and Retirement Study (HRS) sister studies, the Brazilian Longitudinal Study of Aging (ELSI) and the Mexican Health and Aging Study (MHAS). The HRS sister studies were designed to be similar to the original HRS to facilitate cross‐national comparisons, while also having distinct characteristics that were developed to be culturally and linguistically appropriate, as well as tailored to their respective samples. 20 ELSI is an ongoing longitudinal survey of Brazilian adults aged ≥ 50 years and the baseline survey was conducted in 2015 and 2016 and included adults born in 1965 or earlier. 21 MHAS is an ongoing longitudinal survey of Mexican adults aged ≥ 50 years. Wave 1 was collected in 2001 and included adults born in 1951 or earlier. Four follow‐up waves were conducted in 2003, 2012, 2015, and 2018, with refresher cohorts added to the 2012 (born 1952–1961) and 2018 (born 1962–1968) waves. 22 Data 2015 was used for this study, which represents Wave 1 of the ELSI and Wave 4 of the MHAS. The analytical sample included adults aged ≥ 50 years, who participated in the proxy or direct interviews (details about the interviews are in supporting information).
2.2. Education
The independent variable was education, measured as total years of formal education in the MHAS and as categories describing the highest grade completed in the ELSI. We transformed the ELSI education categories into total years of education to harmonize with the MHAS variable (Table S1 in supporting information). Education had a non‐linear association with cognitive impairment in both studies (Figure S1 in supporting information). Therefore, we report our results using four categories of education (0, 1–4, 5–8, > 8 years of education) based on the countries’ education levels (elementary, middle, and high school and above).
2.3. Cognitive function
The study outcome was cognitive function. The cognitive function module of the MHAS and ELSI studies for direct interviews was adapted from the Cross Cultural Cognitive Examination (CCCE). 23
The cognitive assessment in the 2015 ELSI wave included the 10‐word list immediate and delayed recall, temporal orientation (day, month, year, and day of the week), semantic verbal fluency (animal category), prospective memory (remember to write one's initials after finishing another test), and semantic memory questions (two questions about common items and two questions about current politics). The cognitive assessment in the 2015 MHAS wave included the 8‐word list immediate and delayed recall, visual scanning, immediate and delayed constructional praxis, temporal orientation (day, month, year), semantic verbal fluency (animal category), counting backward from 20 to 11, and serial 7s. The detailed descriptions of the tests used in both studies can be found in the supporting information. While the CCCE cognitive battery was translated and culturally adapted, some tests that evaluated the same cognitive domain in each study were applied differently. Additionally, translations of word recall lists may introduce heterogeneity. 23 Due to difficulties in harmonizing the cognitive battery in the ELSI and MHAS, we opted to categorize participants in each study as cognitively impaired or not impaired.
We created a global cognitive z score for each study using the available tests. First, we created a z score for the individual tests by subtracting the participant's score in each test from the mean test score and dividing this result by the standard deviation (SD) of the test. We then calculated the mean z score for all of the tests and standardized this mean to create the global cognitive score.
We selected a normative sample (MHAS, n = 4321; ELSI, n = 3074) to provide regression‐based norms for the cognitive assessment in each study. 24 The normative subsample included only participants without (1) history of stroke; (2) complaints about memory or instrumental activities of daily living; (3) depressive symptoms according to the Center for Epidemiological Scale‐Depression (CESD‐9, cut‐off of 5 points for MHAS, and CESD‐8, cut‐off of 4 points for ELSI); 25 , 26 (4) regression‐based classification of dementia in 2012 for MHAS, or self‐reported history of Alzheimer's disease for ELSI; (5) missing cognitive, age, education, or sex data (Figure S2 in supporting information).
We performed a linear regression for the global cognitive score adjusted for age, sex, and education, and used the coefficients to calculate the predicted global cognitive score for the entire sample. The predicted score was subtracted from the individual's actual score to calculate the residual score, which was then divided by the standard deviation of the residuals (root mean square error) from the normative sample regression. This final z score was used to classify the individual into two cognitive categories. 24
Participants were classified into cognitive impairment (yes vs. no) according to their cognitive status. Cognitive impairment for direct interviews was defined as a cognitive z score lower or equal to −1.5 SD from the z score of the normative sample. 24 The cognitive function was also assessed in an interview with a proxy when the participant was not able to answer the in‐person evaluation using the shortened version of the 16‐item Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) in both studies (details about the score in supporting information). 27 Cognitive impairment for proxy interviews was defined as an IQCODE score above or equal to the cut‐off of 3.4. 27 Next, we combined the results of the direct and proxy interviews to classify the participants’ cognitive function into cognitively impaired or not.
Missingness of cognitive test data can bias the analyses toward younger, more educated, and healthier participants. 28 Thus, we performed an imputation of the cognitive test data for both direct and proxy interviews using multiple imputations by chained equations (MICE). 29 Table S2 in supporting information shows the number of missing data that was imputed for each of the cognitive tests (details in supporting information).
2.4. Covariates
Sociodemographic covariates included age as a continuous variable and sex. Clinical covariates were self‐reported previous diagnosis of hypertension, cardiovascular disease, stroke, diabetes, and depression (measured with the CES‐D as previously described). Lifestyle variables included smoking (never, former, current), current alcohol consumption (yes or no), and body mass index (BMI) calculated as weight in kilograms divided by height in meters squared. Missing covariate values were imputed using MICE. 29
2.5. Statistical analyses
Descriptive analyses were presented as mean and SD for continuous variables and as percentages for categorical variables. The difference in covariates in the MHAS and ELSI studies were described using t tests for continuous variables and chi‐square for categorical ones.
We used logistic regression to evaluate the association between education and cognitive impairment separately for each cohort. Models were adjusted for sociodemographic, clinical, and lifestyle variables. We also investigated the modifying effect of sex and country separately on the association between education and cognitive impairment by adding an interaction term between education and each modifier in the fully adjusted model. To investigate the modifying effect of both cohort and sex on the association between education and cognitive impairment, we added a three‐way interaction term for education, sex, and country in the fully adjusted model. 30 , 31
We verified if the harmonization and subsequent analyses were affected by the different domains evaluated by each cohort's cognitive test battery by performing two sensitivity analyses. First, we used only the common cognitive tests in the direct interview for both studies (temporal orientation, immediate and delayed recall, and verbal fluency) to categorize participants as impaired or not and repeated the logistic regression to evaluate the association between education and cognitive impairment separately for each cohort. Second, we performed a linear regression using the continuous z scores from the common tests of the direct interview only as the outcome in the regression, and calculated a global cognitive z score by calculating the mean of the common tests’ z scores and standardizing this mean. We also performed an additional analysis using five education categories (0, 1–4, 5–8, 9–11, and ≥ 12 years of education) based on the countries’ education levels (elementary, middle, high school, and college education or more).
Descriptive analyses accounted for the sampling design of the ELSI and MHAS studies, and were weighted using the survey weights provided by each study, plus stratum and cluster for ELSI. Regression analyses were unweighted. The alpha level was set at 5%. All statistical analyses were performed using R version 3.6.3. 32
3. RESULTS
3.1. Sample characteristics
Data from 9412 participants from the ELSI and 14,779 participants from the MHAS were analyzed. The mean age for the ELSI participants was 62.5 (9.8) years, 53.9% were women, median (interquartile range [IQR]) years of education was 4 (2–10), with 13.3% having no formal education. The mean age (SD) of the MHAS participants was 64.8 (9.7) years, 55.3% were women, median (IQR) years of education was 6 (2–9), with 17.7% having no formal education. MHAS participants were more likely to be older, female, and have more years of education compared to ELSI participants (Table 1).
TABLE 1.
Characteristics of the Brazilian Longitudinal Study of Aging (ELSI) and the Mexican Health and Aging Study (MHAS).
| ELSI n = 9412 | MHAS n = 14,207 | P | |
|---|---|---|---|
| Age, mean (SD) | 62.5 (9.8) | 64.8 (9.7) | < 0.001 |
| Female, % | 53.9 | 55.3 | 0.208 |
| Education, median (IQR) | 4 (2–10) | 6 (2–9) | < 0.001 |
| Education categories, % | < 0.001 | ||
| 0 years | 13.3 | 17.7 | |
| 1–4 years | 38.3 | 25.5 | |
| 5–8 years | 21.5 | 27.7 | |
| > 8 years | 26.9 | 29.1 | |
| BMI, mean (SD) | 27.8 (5.3) | 27.3 (4.9) | < 0.001 |
| Hypertension, % | 52.2 | 43.8 | < 0.001 |
| Diabetes, % | 15.2 | 22.0 | < 0.001 |
| Cardiovascular disease, % | 5.5 | 3.2 | < 0.001 |
| Alcohol consumption, % | 18.8 | 25.2 | < 0.001 |
| Smoking, % | < 0.001 | ||
| Never | 45.6 | 76.2 | |
| Former | 37.3 | 4.5 | |
| Current | 17.0 | 19.3 | |
| Depression, % | 33.6 | 31.1 | < 0.001 |
Abbreviations: BMI, body mass index; IQR, interquartile range; SD, standard deviation.
A total of 6.0% of ELSI participants and 5.0% of MHAS participants were classified as cognitively impaired (Figure 1). Participants who were cognitively impaired were more likely to be older, women, and have depressive symptoms compared to participants who were not impaired in both studies (Table S3 in supporting information). ELSI and MHAS participants who were cognitively impaired were more likely to have no formal education compared to participants who were not impaired (Table S3). Women were more likely to have no formal education, higher BMI, hypertension, and depressive symptoms than men in both studies (Table S4 in supporting information).
FIGURE 1.
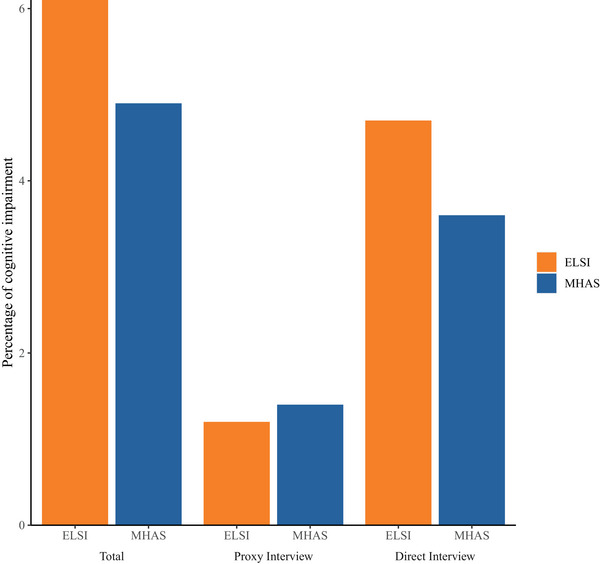
Percentage of cognitive impairment by cohort according to the type of interview. ELSI, Brazilian Longitudinal Study of Aging; MHAS, Mexican Health and Aging Study
3.2. Association between education and cognitive impairment
Compared to the group with no formal education, all education categories had lower odds of cognitive impairment in both studies (Table 2). Similar results were obtained using five categories for education (Table S5 in supporting information), using only the common cognitive tests in both cohorts (word list, temporal orientation, and semantic verbal fluency) for the regression‐based categorization (Table S6 in supporting information), or the continuous z scores of the common tests (Table S7 in supporting information).
TABLE 2.
Association between categories of years of education and cognitive impairment.
| ELSI | ||||||
|---|---|---|---|---|---|---|
| Unadjusted | Model 1 | Model 2 | ||||
| Education categories | OR (95% CI) | P | OR (95% CI) | P | OR (95% CI) | P |
| 0 | 1 (Reference) | 1 (Reference) | 1 (Reference) | |||
| 1–4 | 0.371 (0.304; 0.453) | < 0.001 | 0.450 (0.367; 0.551) | < 0.001 | 0.458 (0.396; 0.595) | < 0.001 |
| 5–8 | 0.252 (0.191; 0.329) | < 0.001 | 0.395 (0.296; 0.551) | < 0.001 | 0.438 (0.329; 0.579) | < 0.001 |
| >8 | 0.266 (0.206; 0.339) | < 0.001 | 0.428 (0.329; 0.555) | < 0.001 | 0.488 (0.372; 0.637) | < 0.001 |
| MHAS | ||||||
|---|---|---|---|---|---|---|
| Unadjusted | Model 1 | Model 2 | ||||
| Education categories | OR (95% CI) | P | OR (95% CI) | P | OR (95% CI) | P |
| 0 | 1 (Reference) | 1 (Reference) | 1 (Reference) | |||
| 1–4 | 0.300 (0.251; 0.359) | < 0.001 | 0.362 (0.301; 0.435) | < 0.001 | 0.357 (0.295; 0.430) | < 0.001 |
| 5–8 | 0.166 (0.134; 0.205) | < 0.001 | 0.266 (0.212; 0.329) | < 0.001 | 0.294 (0.236; 0.364) | < 0.001 |
| >8 | 0.126 (0.099; 0.159) | < 0.001 | 0.262 (0.203; 0.336) | < 0.001 | 0.308 (0.238; 0.395) | < 0.001 |
Abbreviations: CI, confidence interval; ELSI, Brazilian Longitudinal Study of Aging; MHAS, Mexican Health and Aging Study; OR, odds ratio.
Model 1: Unweighted logistics regression adjusted for age and sex.
Model 2: Unweighted logistics regression additionally adjusted for alcohol consumption, smoking, diabetes, hypertension, cardiovascular disease, body mass index, and depression.
There was a modifying effect of sex on the association between education and cognitive impairment in the MHAS (P for interaction = 0.048), but not in the ELSI (Figure 2 and Table S8 in supporting information). Women in the MHAS were more likely to have cognitive impairment than men with the same level of education (Figure 2 and Table S8). There was also a significant difference in the association between education and cognitive impairment by cohort (P for interaction < 0.001), where MHAS participants with more than 1 year of education had lower odds of cognitive impairment than the ELSI participants (Figure 3). The three‐way interaction of sex, cohort, and education was also significant (P for interaction < 0.001). Men in the MHAS had lower odds of cognitive impairment than the men in the ELSI at all levels of education but there was no difference for women (Figure S3 in supporting information).
FIGURE 2.
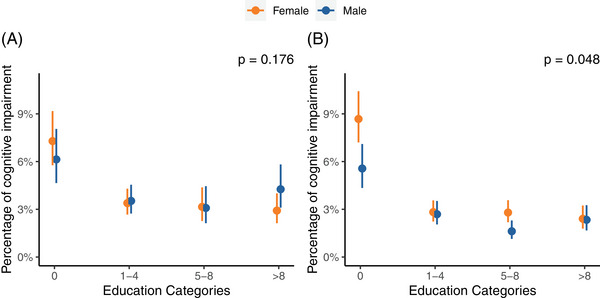
Associations between education categories and cognitive impairment in the (A) Brazilian Longitudinal Study of Aging (ELSI) and (B) Mexican Health and Aging Study (MHAS). P‐values represent the interaction between education and sex
FIGURE 3.
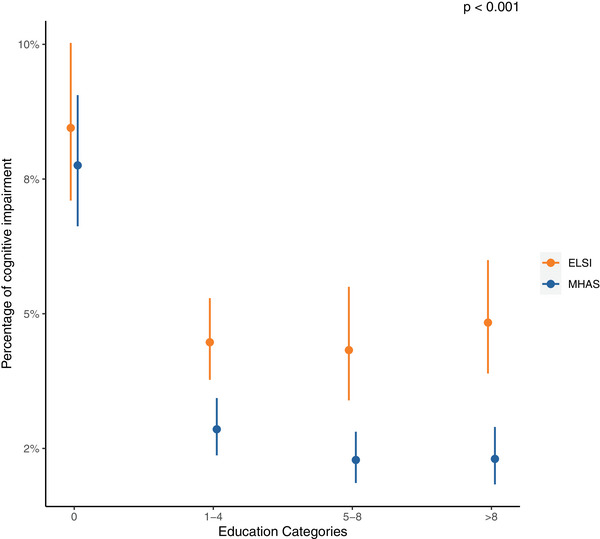
Association between education categories and cognitive impairment by cohort. ELSI, Brazilian Longitudinal Study of Aging. MHAS, Mexican Health and Aging Study. P‐values for the interaction between education and cohort
4. DISCUSSION
In a representative sample of 14,779 participants from the MHAS and 9,412 participants from the ELSI, more years of education were associated with lower odds of cognitive impairment in both cohorts. Compared to having no formal education, even very low levels of education (1–4 years) were associated with reduced odds of cognitive impairment. Sex and cohort were effect modifiers for the association between education and cognitive impairment. Those in the ELSI were more likely to have cognitive impairment than those in the MHAS even at higher levels of education, but this difference was only observed among men.
Our findings are in line with several studies showing that low educational achievement is associated with cognitive impairment. 33 , 34 Nevertheless, 68.8% of older adults in LA have low education (less than 4 years). 5 Moreover, it is estimated that 11.0% of dementia cases in LA are attributable to low education, with this estimate reaching 13.5% in Mexico and 7.7% in Brazil. 5 , 6 Our study shows that even at low levels, having more education is associated with reduced odds of cognitive impairment. Most studies evaluating the association between years of education and cognitive performance have focused on high‐income countries with relatively high educational attainment (≥ 12 years). 35 Other evidence using non‐nationally representative data from LMICs, where the average years of education is lower than 8 years and the prevalence of illiteracy is high, also shows that very low levels of education were associated with higher cognitive performance compared to no formal education. 10 Therefore, our study adds to the evidence that even at low levels, additional years of education are beneficial to cognitive function.
We found an interaction of sex on the association between education and cognitive impairment in the MHAS, but not in the ELSI. Women had higher odds of cognitive impairment compared to men with the same education level in the MHAS. Women in Mexico suffer socioeconomic disadvantages that may impact their cognition in later life, such as less access to health care and overall lower socioeconomic level compared to men. 36 Additionally, women in LA suffer persistent expectations of traditional gender roles, with low incentives to achieve higher education and work outside of the home. 36 A recent study showed that sex differences in cognitive performance decreased over 19 years of follow‐up, as women achieved higher levels of education, 37 which suggests that higher cognitive reserve might lower dementia risk to a higher extent in women than men. 38 Therefore, the sex differences we found in this study may be due to differences in education level and quality between older men and women.
Our finding that the MHAS participants had lower odds of cognitive impairment than participants from the ELSI with the same level of education was surprising. The median years of education among older adults in our sample was 4 years for ELSI and 6 years for MHAS, which are close to the official national estimates but may not completely explain our findings. 39 , 40 Furthermore, years of education may not reflect education quality, and, consequently, may not reflect better cognitive outcomes. 41 Although Brazil and Mexico increased education investments during the early 1900s and particularly during the economic boom and rapid urbanization beginning in the 1950s, there are profound differences in the education systems in Brazil and Mexico. 17 In Mexico, secondary schooling was made compulsory only in 1992, whereas in Brazil basic education (from primary school to high school) was guaranteed as free for all since the 1946 Constitution, and regulated by law since 1971. 42 , 43 , 44 Although we do not have data for quality of education in our cohorts, recent data show that Brazil is among the worst performers in mathematics in LA. 45 Although the share of students reaching advanced learning outcomes is low in both countries, this number is higher in Mexico. 46 Finally, Brazil's education quality is lower than Mexico's as measured by different institutions. 47 These data suggest that although compulsory education in Brazil has been in place longer, quality of education may be higher in Mexico. Cultural and linguistic differences between Brazil and Mexico may also play a role in the observed country difference. Moreover, cognitive processes are universal, but they may be differently applied due to cultural differences. 48 Finally, although both cognitive test batteries are derived from the CCCE they may not be completely comparable and our cognitive impairment classification might not be equivalent in both samples. 23
Practice effects in the MHAS may also play a role in the different associations by cohort, as we used data from wave 4 in the MHAS and wave 1 in the ELSI. Previous studies have demonstrated that practice effect may introduce artificial differences in cognitive performance in different cohorts. 49 Finally, the difference between both studies seems to be driven by men. The men in the ELSI had a higher prevalence of hypertension and cardiovascular disease than the men in the MHAS, which may help explain the differences between studies. Evidence suggests that cardiovascular risk factors are associated with cognitive impairment and dementia. 4 However, we adjusted the models for these factors, suggesting that unmeasured confounding, including differences in diagnostic and disease control between both countries, may partially explain the higher odds of cognitive impairment in the ELSI compared to the MHAS.
Despite these caveats, this study has several strengths. First, it adds important evidence on the association of education and cognitive performance in the two countries. Thirteen and eighteen percent of the samples had no formal education, and even at low levels, having more years of education was associated with lower risk of cognitive impairment. This is also the first study comparing the association of educational attainment and cognitive impairment in nationally representative samples from the two largest countries in LA, Mexico and Brazil, which account for half of the population in the region. 50 We also used data that were collected in the same year in both countries, reducing cohort bias. Our study also has some limitations. First, the cognitive test batteries of the ELSI and the MHAS assess different cognitive domains, and our harmonization method may not identify cognitive impairment homogeneously in both samples. Nevertheless, we were able to include all tests from both studies in our cognitive impairment classification. Our methodology also allowed the inclusion of proxy responders because the IQCODE has an established cut‐off to categorize participants. Second, our classification of cognitively impaired and not impaired depended on several self‐reported variables, and we cannot exclude the possibility of undiagnosed conditions. Third, this study is cross‐sectional and therefore, we cannot determine causality. Finally, although we adjusted the models for several clinical and sociodemographic variables, we cannot exclude the possibility of bias from unmeasured confounders.
In conclusion, low levels of education were associated with lower odds of cognitive impairment compared to no formal education in ELSI and MHAS. Sex plays a critical role in the association between education and cognitive impairment. Men in ELSI have particularly high odds for cognitive impairment compared to men in MHAS, even at higher levels of education. Future longitudinal studies in LMICs are needed to confirm our findings, examine the trajectories of cognitive deterioration, and guide public policies to prevent cognitive impairment in these countries.
CONFLICT OF INTEREST STATEMENT
The authors report no conflicts of interest. Author disclosures are available in the supporting information.
ETHICS APPROVAL
This study was approved by the University of São Paulo Medical School Ethics Committee (CAAE: 54344721.5.0000.0068).
CONSENT STATEMENT
Participants gave informed written consent.
Supporting information
Supporting Information
Supporting Information
ACKNOWLEDGMENTS
NGG is the recipient of an AARF‐D fellowship from the Alzheimer's Association (grant 23AARFD‐1029257). The ELSI‐Brazil was supported by the Brazilian Ministry of Health: Department of Science and Technology from the Secretariat of Science, Technology and Strategic Inputs (DECIT/SCTIE; Grants: 404965/2012‐1 and TED 28/2017); Health Coordination of the Older Person in Primary Care, Department of Life Course from the Secretariat of Primary Health Care (COPID/DECIV/SAPS; Grants: 20836, 22566, 23700, 25560, 25552, and 27510). The MHAS is supported by the National Institutes of Health/National Institute on Aging (grant NIH R01AG018016) and the Instituto Nacional de Estadística y Geografía (INEGI).
Gonçalves NG, Avila JC, Bertola L, et al. Education and cognitive function among older adults in Brazil and Mexico. Alzheimer's Dement. 2023;15:1‐9. 10.1002/dad2.12470
DATA AVAILABILITY STATEMENT
Data from the ELSI is publicly available at https://elsi.cpqrr.fiocruz.br/en/home‐english/ and data from the MHAS is publicly available at https://www.mhasweb.org/Home/index.aspx
REFERENCES
- 1. Nichols E, Steinmetz JD, Vollset SE, et al. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Heal. 2022:7. doi: 10.1016/S2468-2667(21)00249-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Prince M, Wimo A, Guerchet M, Gemma‐Claire A, Wu Y‐T, Prina M. World Alzheimer Report 2015: the Global Impact of Dementia—An analysis of prevalence, incidence, cost and trends. Alzheimer's Dis Int. 2015. doi: 10.1111/j.0963-7214.2004.00293.x [DOI] [Google Scholar]
- 3. Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, Ferri CP. The global prevalence of dementia: a systematic review and metaanalysis. Alzheimer's. Dement. 2013:9. doi: 10.1016/j.jalz.2012.11.007 [DOI] [PubMed] [Google Scholar]
- 4. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020:396. doi: 10.1016/S0140-6736(20)30367-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Mukadam N, Sommerlad A, Huntley J, Livingston G. Population attributable fractions for risk factors for dementia in low‐income and middle‐income countries: an analysis using cross‐sectional survey data. Lancet Glob Heal. 2019:7. doi: 10.1016/S2214-109X(19)30074-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Suemoto CK, Mukadam N, Brucki S, et al. Risk factors for dementia in Brazil: Differences by region and race. Alzheimer's Dement 2022. doi: 10.1002/ALZ.12820 [DOI] [PubMed]
- 7. Stern Y, Arenaza‐Urquijo EM, Bartrés‐Faz D, Belleville S, Cantilon M, Chetelat G, et al. Whitepaper: defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimer's Dement 2020:16. doi: 10.1016/j.jalz.2018.07.219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Farmer ME, Kittner SJ, Rae DS, Bartko JJ, Regier DA. Education and change in cognitive function. Ann Epidemiol. 1995:5. doi: 10.1016/1047-2797(94)00047-w [DOI] [PubMed] [Google Scholar]
- 9. Lyketsos CG, Chen LS, Anthony JC. Cognitive decline in adulthood: an 11.5‐year follow‐up of the Baltimore Epidemiologic Catchment Area study. Am J Psychiatry. 1999:156. doi: 10.1176/ajp.156.1.58 [DOI] [PubMed] [Google Scholar]
- 10. Prince M, Acosta D, Ferri CP, et al. Dementia incidence and mortality in middle‐income countries, and associations with indicators of cognitive reserve: a 10/66 Dementia Research Group population‐based cohort study. Lancet. 2012:380. doi: 10.1016/S0140-6736(12)60399-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Díaz‐Venegas C, Samper‐Ternent R, Michaels‐Obregón A, Wong R. The effect of educational attainment on cognition of older adults: results from the Mexican Health and Aging Study 2001 and 2012. Aging Ment Heal. 2019:23. doi: 10.1080/13607863.2018.1501663 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Seblova D, Berggren R, Lövdén M. Education and age‐related decline in cognitive performance: systematic review and meta‐analysis of longitudinal cohort studies. Ageing Res Rev. 2020:58. doi: 10.1016/J.ARR.2019.101005 [DOI] [PubMed] [Google Scholar]
- 13. Roser M, Ortiz‐Ospina E, Our World in Data: global education 2016. https://ourworldindata.org/global‐education (accessed June 15, 2022)
- 14. United Nations Development Programme . Human Development Report 2020 ‐ The next frontier. n.d.
- 15. Cuéntame de México . Analfabetismo n.d. https://cuentame.inegi.org.mx/poblacion/analfabeta.aspx?tema=P (accessed January 20, 2023)
- 16. Brasil—Ministério da Educação . Mapa do Analfabetismo no Brasil. n.d.
- 17. UNESCO . Education For All 2000‐2015: Achievements and Challenges. 2016.
- 18. Instituto Paulo Montenegro de Ação Educativa . INDICADOR DE ALFABETISMO FUNCIONAL—INAF. 2016.
- 19. Organization for Economic Co‐operation and Development (OECD) . Country note (Mexico). Skills Matter: Additional Results from the Survey of Adult Skills. 2019.
- 20. Gateway to Global Aging Data n.d. https://g2aging.org/
- 21. Lima‐Costa MF, De Andrade FB, Souza PRB De, et al. The Brazilian Longitudinal Study of Aging (ELSI‐Brazil): objectives and Design. Am J Epidemiol. 2018:187. doi: 10.1093/aje/kwx387 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Wong R, Michaels‐Obregon A, Palloni A. Cohort profile: the Mexican Health and aging study (MHAS). Int J Epidemiol. 2017:46. doi: 10.1093/ije/dyu263 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Kobayashi LC, Gross AL, Gibbons LE, et al. You Say Tomato, I Say Radish: can Brief Cognitive Assessments in the U.S. Health Retirement Study Be Harmonized With Its International Partner Studies? J Gerontol B Psychol Sci Soc Sci. 2021:76. doi: 10.1093/geronb/gbaa205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Manly JJ, Bell‐McGinty S, Tang MX, Schupf N, Stern Y, Mayeux R. Implementing diagnostic criteria and estimating frequency of mild cognitive impairment in an urban community. Arch Neurol. 2005:62. doi: 10.1001/archneur.62.11.1739 [DOI] [PubMed] [Google Scholar]
- 25. Aguilar‐Navarro SG, Fuentes‐Cantú A, Ávila‐Funes JA, García‐Mayo EJ. Validity and reliability of the screening questionnaire for geriatric depression used in the Mexican Health and Age Study. Salud Publica Mex. 2007:49. doi: 10.1590/s0036-36342007000400005 [DOI] [PubMed] [Google Scholar]
- 26. Steffick DE, Documentation of Affective Functioning Measures in the Health and Retirement Study (HRS/AHEAD). 2000.
- 27. Jorm AF. The informant questionnaire on cognitive decline in the elderly (IQCODE): a review. Int Psychogeriatrics. 2004:16. doi: 10.1017/S1041610204000390 [DOI] [PubMed] [Google Scholar]
- 28. Downer B, Avila J, Chen N‐W, Wong R. Imputation procedures for cognitive variables in the Mexican health and aging study: evaluating the bias from excluding participants with missing data. Real Datos y Espac Rev Int Estad y Geogr. 2021;12:90. [PMC free article] [PubMed] [Google Scholar]
- 29. van Buuren S, Groothuis‐Oudshoorn K. mice: multivariate imputation by chained equations in R. J Stat Softw. 2011:45. doi: 10.18637/jss.v045.i03 [DOI] [Google Scholar]
- 30. Robins M, James MAH, Hernán MA, Robins JM, Robins M, James MAH, Causal Inference: What If. Found Agnostic Stat 2020.
- 31. Nichols E, Ng DK, Hayat S, et al. Differences in the measurement of cognition for the assessment of dementia across geographic contexts: recommendations for cross‐national research. Alzheimer's Dement. 2022. doi: 10.1002/alz.12740 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. R Development Core Team . R Core Team (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing, URL https://www.R‐project.org/ R Found Stat Comput 2019;2:https://www.R‐project.org [Google Scholar]
- 33. Van Hooren SAH, Valentijn AM, Bosma H, Ponds RWHM, Van Boxtel MPJ, Jolles J. Cognitive functioning in healthy older adults aged 64‐81: a cohort study into the effects of age, sex, and education. Aging, Neuropsychol Cogn. 2007:14. doi: 10.1080/138255890969483 [DOI] [PubMed] [Google Scholar]
- 34. Wilson RS, Hebert LE, Scherr PA, Barnes LL, De Leon CFM, Evans DA. Educational attainment and cognitive decline in old age. Neurology. 2009:72. doi: 10.1212/01.wnl.0000341782.71418.6c [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Opdebeeck C, Martyr A, Clare L. Cognitive reserve and cognitive function in healthy older people: a meta‐analysis. Aging, Neuropsychol Cogn. 2016:23. doi: 10.1080/13825585.2015.1041450 [DOI] [PubMed] [Google Scholar]
- 36. SIGI 2020 Regional Report for Latin America and the Caribbean 2020. doi: 10.1787/CB7D45D1-EN [DOI]
- 37. Bloomberg M, Dugravot A, Dumurgier J, Kivimaki M, Fayosse A, Steptoe A, et al. Sex differences and the role of education in cognitive ageing: analysis of two UK‐based prospective cohort studies. Lancet Public Heal. 2021:6. doi: 10.1016/S2468-2667(20)30258-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Launer LJ, Andersen K, Dewey ME, et al. Rates and risk factors for dementia and Alzheimer's disease: results from EURODEM pooled analyses. Neurology. 1999:52. doi: 10.1212/wnl.52.1.78 [DOI] [PubMed] [Google Scholar]
- 39. Neumann LTV, Albert SM. Aging in Brazil. Gerontologist. 2018:58. doi: 10.1093/geront/gny019 [DOI] [PubMed] [Google Scholar]
- 40. INEGI . Encusta Intercensal 2015 n.d. https://www.inegi.org.mx/programas/intercensal/2015/?init=1#Tabulados (accessed January 20, 2023)
- 41. Mantri S, Nwadiogbu C, Fitts W, Dahodwala N. Quality of education impacts late‐life cognition. Int J Geriatr Psychiatry. 2019:34. doi: 10.1002/gps.5075 [DOI] [PubMed] [Google Scholar]
- 42. Santibañez L, Vernez G, Razquin P, Education in Mexico: Challenges and Opportunities. 2005.
- 43. Brasil . CONSTITUIÇÃO DOS ESTADOS UNIDOS DO BRASIL (DE 18 DE SETEMBRO DE 1946) 1946. http://www.planalto.gov.br/ccivil_03/Constituicao/Constituicao46.htm
- 44. Educação M da. Lei 5.962 de 11 de agosto de 1971. 1971.
- 45. Our World in Data . LLECE: Mean performance on the mathematics scale for 6th grade students n.d. https://ourworldindata.org/grapher/llece‐mean‐performance‐on‐the‐mathematics‐scale‐for‐6th‐grade‐students?time=2013
- 46. Our World in Data . Learning outcomes, minimum vs advanced achievement, 1990. n.d. https://ourworldindata.org/grapher/share‐of‐students‐achieving‐minimum‐vs‐advanced‐learning‐outcomes?time=1990&country=CAN~CUB~DOM~HND~MEX~USA~ARG~BOL~BRA~CHL~COL~PRY~PER~VEN
- 47. Roser M, Nagdy M, Ortiz‐Ospina E, Quality of Education n.d. https://ourworldindata.org/quality‐of‐education#the‐distribution‐of‐pisa‐outcomes‐within‐countries
- 48. Ardila A. Cross‐cultural differences in cognition and learning. SAGE Handb Evol Psychol. 2020. doi: 10.4135/9781529739442.n23 [DOI] [Google Scholar]
- 49. Bartels C, Wegrzyn M, Wiedl A, Ackermann V, Ehrenreich H. Practice effects in healthy adults: a longitudinal study on frequent repetitive cognitive testing. BMC Neurosci. 2010:11. doi: 10.1186/1471-2202-11-118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Countries in Latin America and the Caribbean by population (2023) n.d. https://www.worldometers.info/population/countries‐in‐latin‐america‐and‐the‐caribbean‐by‐population/(accessed January 20, 2023)
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information
Supporting Information
Data Availability Statement
Data from the ELSI is publicly available at https://elsi.cpqrr.fiocruz.br/en/home‐english/ and data from the MHAS is publicly available at https://www.mhasweb.org/Home/index.aspx