

Abstract
Objective:
Efficient pain management following arthroscopic shoulder surgery plays a crucial role in decreasing pain intensity, tramadol consumption, and related side effects. This study primarily aimed to examine the analgesic impact of intravenous (IV) ibuprofen and paracetamol on postoperative pain intensity. In addition, as secondary objectives, the study assesses tramadol consumption, determine the global satisfaction score (GSS), analyze hemodynamic parameters, and investigate tramadol-related side effects.
Methods:
In this study, we enrolled sixty-four patients who were scheduled to undergo arthroscopic shoulder surgery and met the inclusion criteria of having American Society of Anesthesiologists scores between 1 and 3 and falling within the age range of 18 to 85 years. All participants were managed using IV patient-controlled analgesia. These patients were then randomly assigned in a double-blind manner to two groups: one receiving paracetamol (n=32), and the other receiving ibuprofen (n=32). Demographic information, visual analog scale (VAS) and GSS data, hemodynamics, tramadol consumption, and tramadol-related side effects were recorded.
Results:
There were no significant differences between the two groups regarding demographics, hemodynamics, GSS scores, and tramadol side effects (respiratory depression, pruritus, urinary retention, and nausea and vomiting). VAS scores of the two groups were similar at postoperative 1st, 6th, and 12th hours. However, group ibuprofen significantly reduced the VAS scores at the postoperative 24th hour (p=0.039). On the other hand, the two groups showed no significant differences in GSS scores. Compared with total tramadol consumption during the postoperative 24-hour period, ibuprofen significantly reduced tramadol consumption (p=0.003).
Conclusions:
The findings of this study indicate a significant reduction in both pain intensity and tramadol consumption when IV ibuprofen was administered 24 hours following arthroscopic shoulder surgery, in comparison with the use of IV paracetamol.
Keywords: Anesthesiology, intravenous ibuprofen, intravenous paracetamol, postoperative pain, shoulder surgery
Abstract
Amaç:
Artroskopik omuz cerrahisi sonrası etkin ağrı yönetimi, ağrı yoğunluğunun, tramadol tüketiminin ve ilgili yan etkilerin azaltılmasında önemli bir rol oynamaktadır. Bu çalışmanın birincil amacı, intravenöz (İV) parasetamol ve ibuprofenin postoperatif ağrı şiddeti üzerindeki analjezik etkilerini karşılaştırmak, ikincil amacı ise tramadol tüketimi, global memnuniyet skoru (GMS), hemodinami ve tramadol ile ilgili yan etkileri incelemektir.
Yöntemler:
Bu çalışmaya artroskopik omuz cerrahisi planlanan, Amerikan Anestezistler Derneği skoru 1-3 olan, yaşları 18-85 arasında olan 64 hasta dahil edildi. Tüm hastalarda İV hasta kontrollü analjezi kullandı. Hastalar rastgele ve çift-kör olarak iki gruba ayrıldı: Parasetamol (n=32) ve ibuprofen (n=32). Demografik bilgiler, vizüel analog skala (VAS) ve GMS, hemodinami, tramadol tüketimi ve buna bağlı yan etkiler kaydedildi.
Bulgular:
İki grup arasında demografik özellikler, hemodinami, GMS skorları ve tramadole bağlı yan etkiler (solunum depresyonu, kaşıntı, idrar retansiyonu ve bulantı-kusma) açısından anlamlı fark yoktu. Postoperatif 1., 6. ve 12. saatlerde iki grubun VAS skorları benzerdi. Ancak ibuprofen grubu postoperatif 24. saatte VAS skorlarını anlamlı olarak düşürdü (p=0,039). Öte yandan, iki grubun GMS skorlarında anlamlı bir fark yoktu. Postoperatif 24 saatlik dönemde toplam tramadol tüketimi ile karşılaştırıldığında ibuprofen grubu, tramadol tüketimini anlamlı olarak azalttı (p=0,003).
Sonuçlar:
Bu çalışma, artroskopik omuz cerrahisi sonrası 24 saatlik periyotta, İV parasetamole kıyasla İV ibuprofen ile ağrı şiddetinin ve tramadol tüketiminin önemli ölçüde azaldığını göstermiştir.
Keywords: Anesteziyoloji, intravenöz ibuprofen, intravenöz parasetamol, ameliyat sonrası ağrı, omuz cerrahisi
INTRODUCTION
Arthroscopic shoulder surgery is a frequently performed orthopedic procedure that poses notable challenges for managing postoperative pain, both for orthopedic surgeons and anesthesiologists. Effective postoperative analgesia during shoulder surgery can reduce complications, expedite patient discharge and enhance postoperative care1,2.
Multimodal analgesia involves the use of multiple medications for postoperative pain management. Opioids play a prominent role in postoperative pain relief due to their effectiveness, although they are associated with limitations due to side effects such as respiratory depression, urinary retention, nausea, vomiting, and pruritus3. Combining supplemental analgesics may mitigate the side effects that often arise because of opioid use.
Supplementary agents, such as non-steroidal anti-inflammatory drugs (NSAIDs), can be integrated with opioids. These agents serve a dual purpose by not only mitigating pain but also targeting the inflammatory aspect of pain. Furthermore, the synergistic use of NSAIDs alongside opioids can mitigate adverse effects by reducing the overall opioid requirement4,5,6.
Previous research has established that intravenous (IV) paracetamol, renowned for its effective analgesic attributes and favorable safety profile, can effectively curtail opioid use and mitigate associated side effects when integrated into multimodal pain management strategies, particularly in the context of orthopedic surgeries7. Its analgesic efficacy is particularly notable when combined with opioids.
In the United States, IV ibuprofen is the first and sole NSAID designed for pain and fever management. Multicenter studies have validated the efficacy of IV ibuprofen for managing postoperative pain following orthopedic surgeries8.
Despite the proven efficacy of IV ibuprofen, the number of randomized controlled trials assessing its effectiveness and safety in orthopedic surgeries remains limited. Although previous studies have examined the use of IV ibuprofen in hip and knee surgeries, including replacements, reconstructions, and arthroplasties, no clinical trial has specifically addressed its role in pain management following arthroscopic shoulder surgery. Thus, we hypothesized that IV ibuprofen could be a valuable option in multimodal pain management after arthroscopic shoulder surgery. The primary objective of this study was to assess and compare the impact of acetaminophen and ibuprofen on postoperative pain intensity. As secondary objectives, this study evaluated tramadol consumption, global satisfaction scores (GSS), hemodynamic parameters, and the incidence of tramadol-related side effects in patients who underwent arthroscopic shoulder surgery.
MATERIALS and METHODS
Following approval from the Clinical Research Ethics Committee at Bezmialem Vakif University Clinical Research Ethics Committee (decision no: 15/1, date: 08.09.2021), this study was registered on ClinicalTrials.gov (#NCT05401916). We conducted a randomized, double-blind study involving 64 patients who underwent arthroscopic shoulder surgery under general anesthesia from June 2022 to April 2023 at a university hospital. This study was meticulously designed in compliance with the CONSORT guidelines9.
Inclusion criteria encompassed patients aged 18 to 85 years, with American Society of Anesthesiologists (ASA) physical status scores ranging from 1 to 3. Patients classified as having an ASA score of IV, those falling outside the specified age range, individuals with peptic ulcers, severe hepatic or renal failure, significant cardiovascular or pulmonary conditions, and a history of drug allergies (specifically, propofol, fentanyl, rocuronium, paracetamol, ibuprofen, and tramadol), as well as cases of emergency surgery and individuals who did not provide informed consent, were excluded from participation. All participants provided written informed consent before their scheduled arthroscopic shoulder surgery.
An independent investigator conducted randomization of this study to receive paracetamol or ibuprofen using MedCalc statistical software (medcalc.com.tr.), version 16. The patients were allocated into two groups: paracetamol (n=32) and ibuprofen (n=32) (Figure 1).
Figure 1.

Flow diagram.
On the day of surgery, the patients underwent standard premedidication consisting of midazolam administered intravenously at a dosage range of 0.01-0.02 mg/kg before their admission to the operating theater. Comprehensive monitoring protocols, which encompassed non-invasive blood pressure, heart rate (HR), peripheral oxygen saturation (SpO2), and electrocardiography, were uniformly implemented for all enrolled participants. Subsequently, all patients received standard general anesthesia, which was characterized by induction with propofol (2-2.5 mg/kg), ffentanyl (1 µg/kg), and rocuronium (0.6 mg/kg), and maintenance with sevoflurane (2-2.5%) in conjunction with a 40% oxygen mixture in oxygen-air. Fentanyl (0.1-0.2 µg/kg, IV) was titrated for intraoperative analgesia as required in cases where HR and/or mean arterial pressure (MAP) increased by 20% above baseline during surgery. Analgesic drugs, either 1 g paracetamol (IV, 10 mg/mL, PAROL®, Atabay Kimya, Istanbul, Turkey) for the paracetamol group or 800 mg ibuprofen (IV, 800 mg/8 mL, IBUPROFEN-PF®, Polifarma, Tekirdag, Turkey) administered in 250 mL saline for the ibuprofen group, were introduced into the patients’ treatment regimen approximately 30 minutes (min) before the end of the surgical procedure. Following their surgical procedures, patients who had fully recovered from neuromuscular blockade were transferred to the postanesthesia care unit. In the ensuing 24-hour postoperative period, all patients were administered tramadol (IV, 100 mg/2 mL, CONTRAMAL®, Abdi İbrahim, Istanbul, Turkey) via an IV patient-controlled analgesia (IV PCA) device [Abbott Provider, Pain Manager II (APMII) Single-Channel PCA, Chicago, USA]. It is noteworthy that the attending anesthesiologists maintained a blinded approach throughout the study, remaining uninvolved in anesthesia management and patient treatment. Local anesthetics were not used for any of the surgical procedures, and a uniform surgical protocol was adhered to for all patients. The PCA solution consisted of 500 mg tramadol dissolved in 100 mL of saline (5 mg/mL), with the PCA device settings configured as follows: infusion rate: 2 mL/h, bolus dose: 2 mL, lockout period: 15 min. The following observation in the postoperative care unit, the patients were subsequently transferred to the orthopedic ward.
Paracetamol (1 g/100 mL) and ibuprofen (800 mg/250 mL) administrations were administered via IV infusion7,10. The initial dose in both study groups was administered at the time of wound closure. Subsequently, paracetamol or ibuprofen was administered every 6 h in both groups throughout the follow-up period. Pain intensity was assessed using a visual analog scale (VAS), where 0 represented no pain and 10 indicated the worst imaginable pain. Postoperative evaluations were conducted at the 1st, 6th, 12th, and 24th hours, during which HR, MAP, VAS scores, total tramadol consumption, GSS, nausea-vomiting (graded on a scale of 0-4, with 0 indicating none, 1 for mild, 2 for moderate, 3 for severe nausea without vomiting, and 4 for very severe nausea-vomiting), and the presence of urine retention and pruritus were recorded. Antiemetic prophylaxis was not administered. If VAS scores exceeded 4 during the first postoperative hour, a 50 mg tramadol dose was administered via IV as rescue medication. If VAS scores remained above 4 in 30-minute intervals, tramadol dosages of 20-50 mg were repeated.
Based on the study of Korkmaz Dilmen et al.11 and the assumption that a difference of 2 units on the VAS scale (ranging from 0 to 10) in postoperative pain scores is of clinical significance, we determined an effect size of 2, with an estimated standard deviation of ±2. To achieve a study power (beta) of 0.9 and an alpha of 0.05, we planned for 22 patients in each group, with 64 patients included in the study to account for potential dropouts.
Statistical Analysis
Statistical analysis was conducted using the Statistical Package for Social Sciences Statistics for Windows, SPSS, and Version 22.0 software. Armonk, NY: IBM Corp. The data are presented as mean and standard deviation for quantitative data and as numbers and percentages for qualitative data. The Kolmogorov-Smirnov normality test was used to examine the quantitative data for a normal distribution. Group comparisons were made using the chi-square test, Student’s t-test, or Mann-Whitney U test, with statistical significance set at p<0.05.
RESULTS
This study comprised a total of sixty-four participants. No statistically significant differences were observed between the two groups concerning demographic data, ASA physical status, smoking or alcohol, comorbidities, duration of anesthesia, and total amount of fentanyl (p>0.05). Demographic data are shown in Table 1.
Table 1. Demographics.

VAS scores of the two groups were similar at postoperative 1st, 6th, and 12th hours. However, group ibuprofen significantly reduced the VAS scores at the postoperative 24th hour [VAS scores of group paracetamol: 2.50 (0-6), group ibuprofen: 2 (0-6), p=0.039] (Figure 2). On the other hand, there were no considerable differences between the groups regarding GSS scores during the postoperative 24-hour period. VAS and GSS of patients in two groups are presented in Table 2.
Figure 2.

VAS scores.
VAS: Visual analog scale
Table 2. Visual analog scales and global satisfaction scores of patients in two groups.

During the postoperative 24-hour period, tramadol consumption at PCA was 484.50 mg (244.00-600.00) for the paracetamol group and 363.00 mg (245.00-553.00) for the ibuprofen group. Rescue medications with tramadol were 80.00 mg (0-340.00) for group paracetamol 20.00 mg (0-200.00) for the ibuprofen group. The total tramadol consumption was 555.38 mg (244.00-940.00) for the paracetamol group and 419.63 mg (245.00-690.00) for group ibuprofen. In comparing tramadol consumption during the postoperative 24-hour period, group ibuprofen significantly reduced tramadol consumption (PCA-tramadol consumption; p=0.003, rescue medication of tramadol; p=0.011, total tramadol consumption; p=0.003). Tramadol consumption (mg) during the postoperative 24-hour period is presented in Table 3.
Table 3. Tramadol consumptions (mg) during the postoperative 24-hour period.

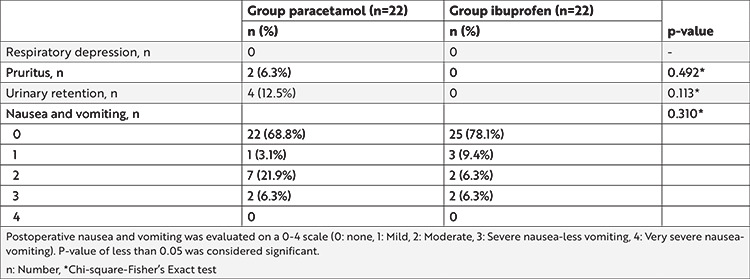
Throughout the postoperative 24-hour period, there were no significant alterations in vital signs, including HR, MAP, and SpO2, between the two groups. Furthermore, there were no noteworthy differences among the groups concerning adverse events related to tramadol, such as respiratory depression, pruritus, urinary retention, and nausea-vomiting. Adverse events related to tramadol are presented in Table 4.
Table 4. Side effects related to tramadol.
DISCUSSION
IV ibuprofen, administered in conjunction with IV PCA during the 24-hour post-arthroscopic shoulder surgery period, demonstrated a significant reduction in both pain intensity and tramadol consumption compared with IV paracetamol. On the other hand, the hemodynamics, GSS results, and tramadol-related side effects exhibited no substantial differences between the two groups.
The number of patients undergoing shoulder surgery continues to increase, underscoring the ongoing significance of postoperative pain management. Typically, patients report significant pain intensity during the initial 48 h following shoulder surgery12. Various approaches have been proposed to alleviate pain after arthroscopic shoulder surgery, including single local analgesic injections, continuous infusion of local analgesics, regional nerve blocks, and IV PCA13,14,15.
Multimodal analgesia has been advocated as a strategy for achieving effective pain control. Previous studies have highlighted the benefits of multimodal analgesia in postoperative care following shoulder surgery, primarily focusing on pain intensity, opioid consumption, and opioid-related side effects12,16. In line with these approaches, we conducted a clinical analysis using multimodal analgesia incorporating IV paracetamol and ibuprofen. Our results align with those of prior research, demonstrating reductions in pain scores and tramadol consumption. In addition, we extended our investigation to encompass hemodynamic parameters and GSS scores during the 24-hour postoperative period, revealing that the ibuprofen group yielded superior outcomes.
Numerous studies have examined the efficacy of different analgesics, consistently demonstrating that paracetamol exhibits potent analgesic effects and reduces opioid consumption across various surgical procedures (including gynecological surgeries, tonsillectomies, coronary artery bypass grafts, thyroidectomies, and laparoscopic cholecystectomy)17. IV ibuprofen has emerged as a crucial option for enhancing postoperative pain management and patient satisfaction18. However, the number of randomized controlled trials evaluating the efficacy and safety of IV ibuprofen remains limited, particularly in the context of orthopedic surgeries. While previous studies have investigated IV ibuprofen following hip and knee surgeries (replacement, reconstruction, or arthroplasty), there is a noticeable dearth of clinical trials examining its role in pain management following arthroscopic shoulder surgery19,20,21. Therefore, this study is one of the first studies on pain management using IV ibuprofen after arthroscopic shoulder surgery. Importantly, our findings indicate that IV ibuprofen significantly reduces pain intensity and tramadol consumption compared with IV paracetamol.
Consistent with prior research, this clinical trial aligns with previous studies concerning the side effects associated with tramadol consumption16,17. Although we observed no statistically significant differences between the groups, it is noteworthy that the ibuprofen group exhibited lower instances of pruritus, urinary retention, and nausea-vomiting, which were attributable to reduced tramadol consumption.
Several limitations were encountered in this study. First, the sample size was relatively small, which may have influenced the robustness of the findings. Second, it should be noted that pain medications and pain intensity experienced during the pre-operative period could impact the outcomes related to tramadol consumption and pain scores. Therefore, future research should consider a comprehensive evaluation of preoperative medications and pain intensity through thorough pain assessments. Third, regional techniques such as interscalene block of the arm were not implemented in this study, which could have influenced the results. Future investigations might explore comparisons between ibuprofen and regional methods in patients undergoing arthroscopic shoulder surgery to provide a more comprehensive understanding of optimal pain management strategies.
CONCLUSION
The results of this study indicate a significant reduction in both pain intensity and tramadol consumption when IV ibuprofen was administered 24 h following arthroscopic shoulder surgery, in comparison with the use of paracetamol. This suggests that IV ibuprofen could be a more favorable choice within a multimodal analgesic approach for managing post-arthroscopic shoulder surgery pain.
Footnotes
Ethics
Ethics Committee Approval: Following approval from the Clinical Research Ethics Committee at Bezmialem Vakif University Clinical Research Ethics Committee (decision no: 15/1, date: 08.09.2021), this study was registered on ClinicalTrials.gov (#NCT05401916).
Informed Consent: Written informed consent was obtained from the patients for publication of this clinical trial details.
Peer-review: Externally and internally peer-reviewed.
Author Contributions
Surgical and Medical Practices: M.C., S.Y., M.G., I.S., S.A., Concept: M.C., S.Y., S.A., Design: M.C., S.Y., S.A., Data Collection and/or Processing: M.C., S.Y., M.G., S.A., Analysis and/or Interpretation: M.C., M.G., I.S., S.A., Literature Search: M.C., S.Y., M.G., I.S., S.A., Writing: M.C., S.Y., S.A.
Conflict of Interest: The authors have no conflict of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.Metwalli Osama S, Abotaleb Usama I, Nasr Hatem M. Comparative study between intravenous ibuprofen, intravenous tramadol alone and in combination after arthroscopic reconstruction surgery. Ain-Shams Journal of Anesthesiology. 2013;6:171–4. [Google Scholar]
- 2.Lee SC, Jeong JH, Jeong SY, et al. Comparison between two different concentrations of a fixed dose of ropivacaine in interscalene brachial plexus block for pain management after arthroscopic shoulder surgery: a randomized clinical trial. Korean J Anesthesiol. 2021;74:226–33. doi: 10.4097/kja.20353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Joshi GP, Viscusi ER, Gan TJ, et al. Effective treatment of laparoscopic cholecystectomy pain with intravenous followed by oral COX-2 specific inhibitor. Anesth Analg. 2004;98:336–42. doi: 10.1213/01.ANE.0000093390.94921.4A. [DOI] [PubMed] [Google Scholar]
- 4.Akbas S, Ozkan AS, Durak MA, Yologlu S. Efficacy of Intravenous Paracetamol and Ibuprofen on Postoperative Pain and Morphine Consumption in Lumbar Disc Surgery: Prospective, Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Neurochirurgie. 2021;67:533–9. doi: 10.1016/j.neuchi.2021.04.019. [DOI] [PubMed] [Google Scholar]
- 5.Jebaraj B, Maitra S, Baidya DK, Khanna P. Intravenous paracetamol reduces postoperative opioid consumption after orthopedic surgery: a systematic review of clinical trials. Pain Res Treat. 2013;2013:402510. doi: 10.1155/2013/402510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ilyas AM, Miller AJ, Graham JG, Matzon JL. Pain Management After Carpal Tunnel Release Surgery: A Prospective Randomized Double-Blinded Trial Comparing Acetaminophen, Ibuprofen, and Oxycodone. J Hand Surg Am. 2018;43:913–9. doi: 10.1016/j.jhsa.2018.08.011. [DOI] [PubMed] [Google Scholar]
- 7.Lachiewicz PF. The role of intravenous acetaminophen in multimodal pain protocols for perioperative orthopedic patients. Orthopedics. 2013;36(2 Suppl):15–9. doi: 10.3928/01477447-20130122-52. [DOI] [PubMed] [Google Scholar]
- 8.Pitchon DN, Dayan AC, Schwenk ES, Baratta JL, Viscusi ER. Updates on Multimodal Analgesia for Orthopedic Surgery. Anesthesiol Clin. 2018;36:361–73. doi: 10.1016/j.anclin.2018.05.001. [DOI] [PubMed] [Google Scholar]
- 9.Schulz KF, Altman DG, Moher D; CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. doi: 10.1136/bmj.c332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Southworth S, Peters J, Rock A, Pavliv L. A multicenter, randomized, double-blind, placebo-controlled trial of intravenous ibuprofen 400 and 800 mg every 6 hours in the management of postoperative pain. Clin Ther. 2009;31:1922–35. doi: 10.1016/j.clinthera.2009.08.026. [DOI] [PubMed] [Google Scholar]
- 11.Korkmaz Dilmen O, Tunali Y, Cakmakkaya OS, et al. Efficacy of intravenous paracetamol, metamizol and lornoxicam on postoperative pain and morphine consumption after lumbar disc surgery. Eur J Anaesthesiol. 2010;27:428–32. doi: 10.1097/EJA.0b013e32833731a4. [DOI] [PubMed] [Google Scholar]
- 12.Cho CH, Song KS, Min BW, et al. Multimodal approach to postoperative pain control in patients undergoing rotator cuff repair. Knee Surg Sports Traumatol Arthrosc. 2011;19:1744–8. doi: 10.1007/s00167-010-1294-y. [DOI] [PubMed] [Google Scholar]
- 13.Boss AP, Maurer T, Seiler S, Aeschbach A, Hintermann B, Strebel S. Continuous subacromial bupivacaine infusion for postoperative analgesia after open acromioplasty and rotator cuff repair: preliminary results. J Shoulder Elbow Surg. 2004;13:630–4. doi: 10.1016/j.jse.2004.04.005. [DOI] [PubMed] [Google Scholar]
- 14.Cho NS, Ha JH, Rhee YG. Patient-controlled analgesia after arthroscopic rotator cuff repair: subacromial catheter versus intravenous injection. Am J Sports Med. 2007;35:75–9. doi: 10.1177/0363546506291632. [DOI] [PubMed] [Google Scholar]
- 15.Ruiz-Suarez M, Barber FA. Postoperative pain control after shoulder arthroscopy. Orthopedics. 2008;31:1130. doi: 10.3928/01477447-20081101-25. [DOI] [PubMed] [Google Scholar]
- 16.Jo CH, Shin JS, Huh J. Multimodal analgesia for arthroscopic rotator cuff repair: a randomized, placebo-controlled, double-blind trial. Eur J Orthop Surg Traumatol. 2014;24:315–22. doi: 10.1007/s00590-013-1208-z. [DOI] [PubMed] [Google Scholar]
- 17.Macario A, Royal MA. A literature review of randomized clinical trials of intravenous acetaminophen (paracetamol) for acute postoperative pain. Pain Pract. 2011;11:290–6. doi: 10.1111/j.1533-2500.2010.00426.x. [DOI] [PubMed] [Google Scholar]
- 18.Southworth SR, Woodward EJ, Peng A, Rock AD. An integrated safety analysis of intravenous ibuprofen (Caldolor(®)) in adults. J Pain Res. 2015;8:753–65. doi: 10.2147/JPR.S93547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dahl V, Dybvik T, Steen T, Aune AK, Rosenlund EK, Raeder JC. Ibuprofen vs. acetaminophen vs. ibuprofen and acetaminophen after arthroscopically assisted anterior cruciate ligament reconstruction. Eur J Anaesthesiol. 2004;21:471–5. doi: 10.1017/s026502150400609x. [DOI] [PubMed] [Google Scholar]
- 20.Singla N, Rock A, Pavliv L. A multi-center, randomized, double-blind placebo-controlled trial of intravenous-ibuprofen (IV-ibuprofen) for treatment of pain in post-operative orthopedic adult patients. Pain Med. 2010;11:1284–93. doi: 10.1111/j.1526-4637.2010.00896.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Steiness J, Hägi-Pedersen D, Lunn TH, et al. Paracetamol, ibuprofen and dexamethasone for pain treatment after total hip arthroplasty: protocol for the randomised, placebo-controlled, parallel 4-group, blinded, multicentre RECIPE trial. BMJ Open. 2022;12:e058965. doi: 10.1136/bmjopen-2021-058965. [DOI] [PMC free article] [PubMed] [Google Scholar]