

Gastroenterostomy using a lumen-apposing metal stent (LAMS) is an effective procedure to solve gastric outlet obstruction, but usually, an oroenteral catheter is necessary for filling the small bowel.[1] What to do in cases of complete obstruction when it is not possible even to advance a guidewire through?
The academic purpose of this work was to expose a useful approach that may be considered in this scenario. A 64-year-old woman was referred for a complete duodenal obstruction due to pancreatic adenocarcinoma: first, EUS–guided identification of the collapsed small bowel at the Treitz area, and second, EUS-guided puncture using a 22G needle (without stylet and flushed with saline to avoid air injection), filling contrast and saline into the lumen bowel. A submucosal injection of the enteral wall can be recognized as easy to perform and can help to access nicely the enteral lumen, without doubts and fluoroscopy assistance [Figure 1]. Once the lumen gains enough diameter, a second EUS-guided puncture with 19G needle is safely done. Then, a water-jet filling technique is possible, connecting a water pump directly to the 19G needle [Figure 2]. Lastly, once the small bowel is largely distended, the direct “free-hand” method using an electrocautery-enhanced LAMS (HotAxios; 20 × 10 mm) is used and then completely deployed. After intra-LAMS dilation (optional), spontaneous water drainage and visualization of the enteral lumen confirm successful gastroenterostomy [Figure 3, Video 1]. The patient started oral feeding correctly within 8 hours.
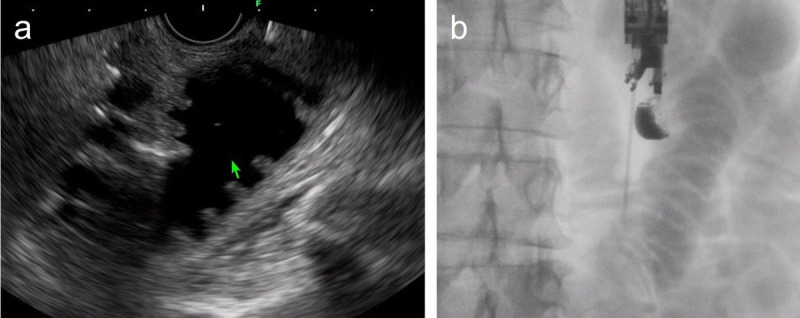
Figure 1.

a, Collapsed small bowel close to the gastric wall, at the Treitz area. b, EUS–guided puncture using a 22G needle (without stylet and flushed with saline), filling contrast and saline into the lumen bowel. A submucosal injection of the enteral wall can be recognized as easy to perform and can help to access nicely the enteral lumen, without doubts. c, Fluoroscopy confirmation.
Figure 2.
Once the enteral lumen gains enough diameter (a), a second EUS-guided puncture with 19G needle is performed b), EUS.
Figure 3.
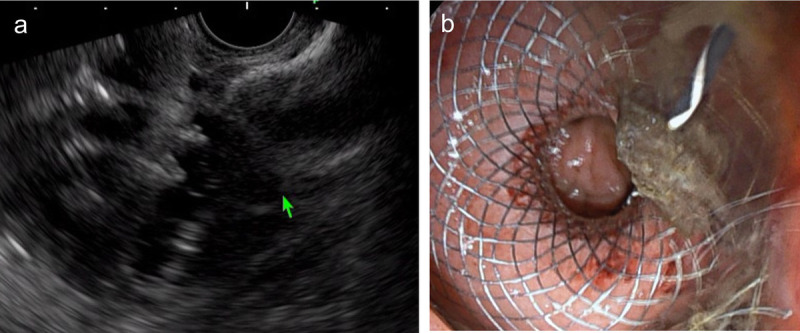
a, Direct free-hand method using an electrocautery-enhanced LAMS (HotAxios; 20 mm × 10 mm). b, After intra-LAMS dilation, visualization of the enteral lumen confirms successful gastroenterostomy. LAMS: lumen-apposing metal stent.
Video Legend.
Complete duodenal obstruction and EUS-guided gastroenterostomy: What to do?
Videos are only available at the official website of the journal (www.eusjournal.com).
Although the direct use of a 19G needle has been reported, given that, in most cases, the small bowel will be collapsed, the first attempt to access inside the enteral lumen may be easier using firstly a 22G needle (a 22G ➔ 19G ➔ free-hand LAMS, strategy).[2]
Informed Consent
Informed consent was obtained from the patient for the publication of their information and imaging. All authors have read and agreed on the content of this article.
Contributor Information
Maria Puigcerver-Mas, Email: jgornals@bellvitgehospital.cat.
Dani Luna-Rodriguez, Email: jgornals@bellvitgehospital.cat.
Albert Garcia-Sumalla, Email: jgornals@bellvitgehospital.cat.
Sergi Quintana-Carbo, Email: jgornals@bellvitgehospital.cat.
Sandra Maisterra, Email: jgornals@bellvitgehospital.cat.
Funding
The authors have no financial disclosures and no grant support to report.
Conflicts of Interest
Dr. Gornals is a consultant for BostonSc. The other authors have no conflicts of interest to disclose.
References
- 1.Consiglieri CF, Luna-Rodriguez D, Garcia-Sumalla A, Maisterra S, Velasquez-Rodriguez JG, Gornals JB. Direct endoscopic ultrasound–guided gastroenterostomy using a feeding-tube waterjet system: a teaching video to facilitate understanding of the technique. Endoscopy 2022;54:447–448. [DOI] [PubMed] [Google Scholar]
- 2.Collin A Brahmia S Rostain F, et al. Endoscopic ultrasound-guided gastroenterostomy with water-jet filling technique through a 19G needle to treat complete malignant duodenal obstruction. Endoscopy 2021;53:7–8. [DOI] [PubMed] [Google Scholar]