

Abstract
Background
Breastfeeding is known to be the biological norm. Despite this, many women wean their babies because of perceived insufficient breast milk production. Mothers are sometimes advised to increase their fluid intake in the hope that this could improve breast milk production. The effect of extra fluid on human breast milk production is not well established, however.
Objectives
To assess the effect of extra fluid for breastfeeding mothers on milk production/supply and infant growth.
Search methods
We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (27 April 2014), MEDLINE (1966 to 27 April 2014), African Journals Online (27 April 2014) and reference lists of retrieved studies.
Selection criteria
Randomised controlled trials and quasi‐randomised controlled trials on extra fluids for breastfeeding mothers.
Data collection and analysis
Two review authors independently assessed the potential studies for inclusion and assessed trial quality.
Main results
Five trial reports were retrieved using the search strategies. Four trials were excluded. We did not identify any randomised controlled trials for inclusion but we included one quasi‐randomised study (involving 210 women) that evaluated the effect of extra fluid for breastfeeding mothers on breastfeeding outcomes. The study was considered to be at a high risk of bias. Only one of this review's primary outcomes was reported (breast milk production (as defined by the trialist)) but data were not in a suitable format for analysis (no standard deviations or standard errors were reported). The trialist reported that advising women to drink extra fluids did not improve breast milk production. No data were reported for the review's other primary outcomes: satisfactory weight gain in the infant (as defined by the trialists) and duration of exclusive breastfeeding (months). Similarly, no data were reported for any of this review's secondary outcomes: duration of any breastfeeding; mother's satisfaction with breastfeeding; hydration in mother; dehydration in the infant; or episodes of gastrointestinal illness.
Authors' conclusions
This review only identified one small quasi‐randomised controlled trial of low quality and high risk of bias. The study provided limited data on only one of this review's primary outcomes, breast milk production, but the data were not reported in a format that permitted further analysis. The trialist reported that extra fluids did not improve breast milk production. However, this outcome was measured by using test feeds (also known as test weighing). In the 1950s, when the study was conducted, it was common for babies in developed countries to be weighed before and after a feed, known as test weighing or test feeding. However, this practice is not now routinely practiced for term infants due to concerns about lack of precision as a measure of breast milk production. The included study did not report on this review's other primary outcomes (satisfactory weight gain in the infant or duration of exclusive breastfeeding) nor any of the review's secondary outcomes.
The effect of additional fluids for breastfeeding mothers remains unknown, due to a lack of well‐conducted trials. However, because the physiological basis for any such improvement remains unclear, the conduct of further clinical trials may not be a priority. There is not enough evidence to support an increased fluid intake beyond what breastfeeding mothers are likely to require to meet their physiological needs.
Plain language summary
Extra fluids for breastfeeding mothers for increasing milk production
The World Health Organization recommends breastfeeding for infants during the first six months of life. Despite this, many women wean their babies because of their perceived insufficient breast milk production. In many cases where mothers are concerned about their milk production they are encouraged to increase their fluid intake. The mother also needs water to meet her own needs. Water and all the constituents of body fluid are continually being lost in urine, stool and sweat and, therefore need to be replaced.
This review aimed to assess whether increasing fluid intake of breastfeeding mothers has a beneficial effect on breast milk production and infant growth. However, the review only identified one small quasi‐randomised controlled trial (involving 210 women). The trial was of low quality and did not report on two of this review's important outcomes (satisfactory weight gain in the infant or duration of exclusive breastfeeding). The study did report on breast milk production (this review's other main outcome), but the data were not in a format that would permit further analysis in this review. The trial reported that advising women to consume extra fluids did not result in increased breast milk production, as measured by test feeds (also known as test weighing). In the 1950s, when the study was conducted, it was common for babies in developed countries to be weighed before and after a feed, known as test weighing or test feeding. However, this practice is not now routinely practiced for term infants due to concerns about lack of precision as a measure of breast milk production. The included study did not report any of this review's secondary outcomes: duration of any breastfeeding; mother's satisfaction with breastfeeding; hydration in mother; dehydration in the infant; or episodes of gastrointestinal illness.
The effect of additional fluids for breastfeeding mothers remains unknown, due to a lack of well‐conducted trials. However, because the physiological basis for any such improvement remains unclear, the conduct of further clinical trials may not be a priority. There is not enough evidence to support an increased fluid intake beyond what breastfeeding mothers are likely to require to meet their physiological needs.
Background
Description of the condition
Many studies have shown the benefits of breastfeeding to both mother and baby. To breastfeed is regarded as a biological norm (Brodribb 2007; Smith 2009; Wiessinger 1996); not breastfeeding carries short‐ and long‐term risks for infants and mothers in all countries. The World Health Organization (WHO) recommends exclusive breastfeeding up to six months of age, with continued breastfeeding along with appropriate complementary foods up to two years of age or beyond (WHO 2009).
It is estimated that worldwide only 35% of children between birth and their fifth month are breastfed exclusively (Peters 2005; WHO 2010). In order to achieve the Millennium Development Goal of reduction of child mortality, infant breastfeeding has been identified as one of the major intervention areas globally (Jones 2003).
Infants who have been breastfed optimally have a reduced risk of common childhood illnesses such as gastrointestinal and respiratory infections, otitis media, atopic eczema, and allergy during childhood (Foo 2005). Studies have also shown that exclusive breastfeeding for six months (versus three to four months) reduces rates of gastrointestinal infection, supports appropriate growth and can help the mother lose weight (Kramer 2002). Breastfeeding for at least three months is also associated with a reduction in episodes of gastrointestinal illness in the infant and rates of hospital admission (Howie 1990; Story 2008).
Breastfeeding is known to promote growth in children. In well‐nourished mothers, breast milk is generally sufficient in terms of energy, protein, nutrients, water, etc. for an infant's growth needs under six months of age (WHO 2002). Breastfeeding is associated with normal growth patterns in infants and confers protection against obesity (Kalies 2005; Nommsen‐Rivers 2009). The protection against obesity is duration dependent. Thus, infants breastfed exclusively for one month have double the risk of developing obesity compared with infants exclusively breastfed for six months (Kalies 2005).
Duration of breastfeeding is affected by many factors. The mother’s perception about her ability to breastfeed her infant successfully is very important. Approximately 25% to 35% of women reduce breastfeeding duration or level due to perceived breast milk insufficiency (Blyth 2002; Kirkland 2003; O'Brien 2007).
Many mothers are unable to establish and maintain breastfeeding despite wanting to do so (Dewey 2003). Their inability to establish breastfeeding could be a result of perceived lack of adequate milk supply. About one‐third of women wean their babies by eight weeks postpartum, and the most common reason they give for early weaning is lack of milk (Millar 2005; Sheehan 2001).
Women are sometimes advised to increase their water intake during lactation though this has not been proved to be beneficial (Anderson 2006; Filer 1975). Montgomery 2002 stated that pregnant and breastfeeding women should be encouraged to increase their intake of water and other fluids to meet their bodies' needs. This is based on the physiological need for more fluid to meet up the additional demand during pregnancy and lactation. A woman with perceived insufficient milk production should be encouraged to drink a glass of water every time she breastfeeds and when thirsty (National Health and Medical Research Council 2012). This recommendation derives from the theoretical expectation of an increased physiological requirement for water during lactation consequent upon weight gain and milk production (Food and Nutrition Board 1989; Montgomery 2002). However, empirical data describing fluid intakes of successfully lactating women is lacking (Stumbo 1985). Although lactating mothers tend to take much more water compared with their non‐pregnant, non‐lactating counterparts (Ershow 1991), they do not appear to consume enough to satisfy theoretical recommendations (Stumbo 1985). Current studies have not provided evidence to support this advice being given.
Some studies showed no positive benefit of extra maternal fluid intake. Dearlove 1981 demonstrated that giving lactating women extra fluids neither increased serum prolactin nor milk yield, and therefore cautioned against encouraging drinking to excess. Diuresis, depression and nausea may result from excess fluid intake (Anderson 2006).
Description of the intervention
The intervention is additional or extra fluid given beyond the mother's usual fluid intake. It is any fluid given to mothers deliberately to measure the effect on milk supply. It could be milk, water, non‐alcoholic beverages or fruit juice given in addition to the usual fluid intake over a period of time to mothers of babies from birth until six months in order to measure the expected outcomes.
How the intervention might work
Breast milk consists mainly of water and the infant depends on it for survival. The mother also needs water to meet her own needs. Water and all the constituents of body fluid are continually being lost in urine, stool and sweat, and, therefore, need to be replaced.
Presumably, extra water is needed during lactation to meet the additional physiological requirement for the production of breast milk (Food and Nutrition Board 1989). Maintenance of water balance is essential for normal tissue function. To ensure water balance, there is a continual movement of fluid from one area (body space) to another. Water tends to move to the area which has the highest concentration of electrolytes and protein (Woods 2005).
Animal studies have shown that renal physiology adapts to the body fluid challenges imposed by lactation through increased glomerular filtration rate, renal plasma flow and reabsorption of salt and water by the proximal convoluted tubule (Arthur 1986). Thus, normal milk secretion may continue in the presence of restricted intake in animals (Alamer 2009; Peng 2007). It is probable that these changes are mediated by prolactin.
In humans, Buckman 1973 reported significant correlation between osmolality and serum prolactin: serum prolactin fell following administration of hypotonic infusion but rose after infusion of hypertonic fluid. They proposed that prolactin may be involved in the physiologic regulation of osmolar balance and that the kidney may be an important target organ for prolactin. However, when this hypothesis was investigated by administering hypotonic fluid load to lactating women, there were no changes in serum prolactin, milk yield, serum or breast milk osmolality, suggesting that extra fluids during lactation had no effect on yield or composition of breast milk (Dearlove 1981).
Prentice 1984 observed that milk composition changed during fasting, probably reflecting changes in the permeability of the mammary cell. These authors showed that dehydration resulted in changes in milk osmolality, lactose, sodium and potassium concentrations indicative of a marked disturbance of milk synthesis.
An observational study undertaken by Horowitz 1980 to test the effects of physiological variations in fluid intake on prolactin secretion and milk yield in the puerperium among 21 multiparous women showed that milk yield was similar for both those on restricted fluid and excess fluid intake and the study concluded that there was no basis for prescribing changes in fluid intake for control of human lactation.
Why it is important to do this review
The issue of breast milk adequacy in satisfying babies on exclusive breastfeeding has been an issue for debate. It is important to determine whether extra fluids for breastfeeding mothers really improve lactation and health outcomes for their babies.
At the moment, some health professionals hold the belief that increased fluids would improve milk supply while the limited observational research available is in favour of mothers drinking to thirst as extra fluids do not increase milk supply. It is important to systematically review the evidence to bridge the gap between research evidence and some practices.
Objectives
To assess the effect of extra fluid for breastfeeding mothers on milk production/supply and infant growth.
Methods
Criteria for considering studies for this review
Types of studies
We planned to include randomised controlled trials and quasi‐experimental designs published in all languages. We also planned to include cluster‐randomised trials and studies that are published as abstracts. Cross‐over trials were not eligible for inclusion.
Types of participants
Healthy women who are feeding a baby at their breast or expressing/pumping their milk, and their infants aged from birth to six months. We included mothers who had delivered at any gestation.
Types of interventions
Extra fluids such as non‐alcoholic beverages, water and fruit juice compared with usual fluid intake or no advice to increase fluid intake in amount and over any length of time.
Adequate fluids: normal physiological fluid requirement
Extra fluids: additional fluid in excess of the normal requirement
Types of outcome measures
Primary outcomes
Satisfactory weight gain in the infant as defined by the trialists
Duration of exclusive breastfeeding (months)
Breast milk production as defined by trialists
Secondary outcomes
Duration of any breastfeeding
Mother's satisfaction with breastfeeding as measured by the trialists
Hydration in mother as measured by the trialists
Dehydration in the infant as measured by the trialists
Episodes of gastrointestinal illness
Search methods for identification of studies
Electronic searches
We searched the Cochrane Pregnancy and Childbirth Group’s Trials Register by contacting the Trials Search Co‐ordinator (27 April 2014).
The Cochrane Pregnancy and Childbirth Group’s Trials Register is maintained by the Trials Search Co‐ordinator and contains trials identified from:
monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
weekly searches of MEDLINE;
weekly searches of Embase;
handsearches of 30 journals and the proceedings of major conferences;
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Details of the search strategies for CENTRAL, MEDLINE and Embase, the list of handsearched journals and conference proceedings, and the list of journals reviewed via the current awareness service can be found in the ‘Specialized Register’ section within the editorial information about the Cochrane Pregnancy and Childbirth Group.
Trials identified through the searching activities described above are each assigned to a review topic (or topics). The Trials Search Co‐ordinator searches the register for each review using the topic list rather than keywords.
In addition, we carried out supplementary searches of MEDLINE (1966 to 27 April 2014) and African Journals Online (27 April 2014). See:Appendix 1.
Searching other resources
We checked reference lists of retrieved studies for suitable articles and contacted investigators where necessary.
We did not apply any language restrictions.
Data collection and analysis
Selection of studies
Two review authors (C Ndikom (CN) and R Ilesanmi (RI)) independently assessed for inclusion all the potential studies we identified as a result of the search strategy.
Data extraction and management
We designed a form to extract data. For the eligible study, data were not in a format to permit data extraction. In future updates of this review, CN and RI will extract data using the agreed form. We will resolve discrepancies through discussion or, if required, we will consult B Fawole (BF). Data were not in a suitable format for entry into Review Manager Data and Analysis tables. In future updates of this review, if more data are identified, we will enter them into Review Manager software (RevMan 2012) and check them for accuracy. Where information regarding any of the above is unclear, we will attempt to contact authors of the original reports to provide further details.
Assessment of risk of bias in included studies
CN and RI independently assessed risk of bias for the one included study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We resolved any disagreement by discussion or by involving BFas a third assessor.
(1) Random sequence generation (checking for possible selection bias)
We described for the one included study the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.
We assessed the method as:
low risk of bias (any truly random process, e.g. random number table; computer random number generator);
high risk of bias (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number);
unclear risk of bias.
(2) Allocation concealment (checking for possible selection bias)
We described for the one included study the method used to conceal allocation to interventions prior to assignment and will assess whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment.
We assessed the methods as:
low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
high risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
unclear risk of bias.
(3.1) Blinding of participants and personnel (checking for possible performance bias)
We described for the one included study the methods used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. We considered that the study was at low risk of bias if it was blinded, or if we judged that the lack of blinding would be unlikely to affect results. We planned to assess blinding separately for different outcomes or classes of outcomes.
We assessed the methods as:
low, high or unclear risk of bias for participants;
low, high or unclear risk of bias for personnel.
(3.2) Blinding of outcome assessment (checking for possible detection bias)
We described for the one included study the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed methods used to blind outcome assessment as:
low, high or unclear risk of bias.
(4) Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data)
We described for the one included study, and for each outcome or class of outcomes, the completeness of data including attrition and exclusions. We state whether attrition and exclusions were reported and we planned to report the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. In future updates, where sufficient information is reported, or can be supplied by the trial authors, we plan to re‐include missing data in the analyses which we undertake.
We assessed methods as:
low risk of bias (e.g. 20% or less of the data are missing; missing outcome data balanced across groups);
high risk of bias (e.g. where more than 20% of the data are missing; missing data imbalanced across groups; ‘as treated’ analysis done with substantial departure of intervention received from that assigned at randomisation);
unclear risk of bias.
(5) Selective reporting (checking for reporting bias)
We describe for the one included study how we investigated the possibility of selective outcome reporting bias and what we found.
We assessed the methods as:
low risk of bias (where it is clear that all of the study’s pre‐specified outcomes and all expected outcomes of interest to the review have been reported);
high risk of bias (where not all the study’s pre‐specified outcomes have been reported; one or more reported primary outcomes were not pre‐specified; outcomes of interest are reported incompletely and so cannot be used; study fails to include results of a key outcome that would have been expected to have been reported);
unclear risk of bias.
(6) Other bias (checking for bias due to problems not covered by (1) to (5) above)
We described for the included study any important concerns we have about other possible sources of bias.
We assessed whether the study was free of other problems that could put it at risk of bias:
low risk of other bias;
high risk of other bias;
unclear whether there is risk of other bias.
(7) Overall risk of bias
We make explicit judgements about whether the included study was at high risk of bias, according to the criteria given in the Handbook (Higgins 2011). With reference to (1) to (6) above, we assessed the likely magnitude and direction of the bias and whether we consider it is likely to impact on the findings. In future updates, we will explore the impact of the level of bias through undertaking sensitivity analyses ‐ seeSensitivity analysis.
Measures of treatment effect
This review contains one included study but data were not in a suitable format for analysis. The following measures of treatment effect will be used in future updates of this review.
Dichotomous data
For dichotomous data, we will present results as summary risk ratio with 95% confidence intervals.
Continuous data
For continuous data, we will use the mean difference if outcomes are measured in the same way between trials. We will use the standardised mean difference to combine trials that measure the same outcome, but use different methods.
Unit of analysis issues
Cluster‐randomised trials
We did not identify any cluster‐randomised trials for inclusions. If we identify any cluster‐randomised trials for inclusion in future updates of this review we will include them in the analyses along with individually‐randomised trials. We will adjust their sample sizes using the methods described in the Handbook using an estimate of the intracluster correlation co‐efficient (ICC) derived from the trial (if possible), from a similar trial or from a study of a similar population (Higgins 2011). If we use ICCs from other sources, we will report this and conduct sensitivity analyses to investigate the effect of variation in the ICC. If we identify both cluster‐randomised trials and individually‐randomised trials, we plan to synthesise the relevant information. We will consider it reasonable to combine the results from both if there is little heterogeneity between the study designs and the interaction between the effect of intervention and the choice of randomisation unit is considered to be unlikely.
We will also acknowledge heterogeneity in the randomisation unit and perform a subgroup analysis to investigate the effects of the randomisation unit.
Cross‐over trials
Cross‐over trials are not eligible for inclusion.
Dealing with missing data
For the included study, we noted levels of attrition. In future updates we will explore the impact of including studies with high levels of missing data in the overall assessment of treatment effect by using sensitivity analysis. For all outcomes, we will carry out analyses, as far as possible, on an intention‐to‐treat basis, i.e. we will attempt to include all participants randomised to each group in the analyses, and all participants will be analysed in the group to which they were allocated, regardless of whether or not they received the allocated intervention. The denominator for each outcome in each trial will be the number randomised minus any participants whose outcomes are known to be missing.
Assessment of heterogeneity
In future updates, we will assess statistical heterogeneity in each meta‐analysis using the T², I² and Chi² statistics. We will regard heterogeneity as substantial if the T² is greater than zero and either the I² is greater than 30% or there is a low P value (less than 0.10) in the Chi² test for heterogeneity.
Assessment of reporting biases
In future updates, if there are 10 or more studies in the meta‐analysis we will investigate reporting biases (such as publication bias) using funnel plots. We will assess funnel plot asymmetry visually. If asymmetry is suggested by a visual assessment, we will perform exploratory analyses to investigate it.
Data synthesis
We did not carry out statistical analysis using the Review Manager software (RevMan 2012) because data from the included study were not in a suitable format. In future updates of this review, we will use fixed‐effect meta‐analysis for combining data where it is reasonable to assume that studies are estimating the same underlying treatment effect: i.e. where trials are examining the same intervention, and the trials’ populations and methods are judged sufficiently similar. If there is clinical heterogeneity sufficient to expect that the underlying treatment effects differ between trials, or if substantial statistical heterogeneity is detected, we will use random‐effects meta‐analysis to produce an overall summary, if an average treatment effect across trials is considered clinically meaningful. We will treat the random‐effects summary as the average range of possible treatment effects and we will discuss the clinical implications of treatment effects differing between trials. If the average treatment effect is not clinically meaningful we will not combine trials.
If we use random‐effects analyses, we will present the results as the average treatment effect with its 95% confidence interval, and the estimates of T² and I².
Subgroup analysis and investigation of heterogeneity
In future updates of this review, if we identify substantial heterogeneity, we will investigate it using subgroup analyses and sensitivity analyses. We will consider whether an overall summary is meaningful, and if it is, use random‐effects analysis to produce it.
We did not plan to carry out any other prespecified subgroup analyses.
We will assess subgroup differences by interaction tests available within RevMan (RevMan 2012). We will report the results of subgroup analyses quoting the χ2 statistic and P value, and the interaction test I² value.
Sensitivity analysis
Planned sensitivity analyses were not performed due to insufficient data. In the future, we will carry out sensitivity analyses for aspects of the review that might affect the results, for example, where there is risk of bias associated with the quality of some of the included trials.
We will conduct the following sensitivity analyses:
excluding studies at high risk of bias, such as quasi‐randomised studies and studies with missing outcome data;
repeating analyses using a random‐effects model when substantial heterogeneity is found;
excluding studies published as abstracts or non‐peer reviewed publications.
Results
Description of studies
Results of the search
Five study reports were identified from the Pregnancy and Childbirth Group's Trials Register and four were excluded (Dusdieker 1985; Dusdieker 1986; Dusdieker 1990; Morse 1992) while one study (Illingworth 1953) was included in the review. We retrieved 272 reports from MEDLINE (two were duplicates and the rest were excluded at screening stage); and no reports from African Journals online.(SeeFigure 1).
1.
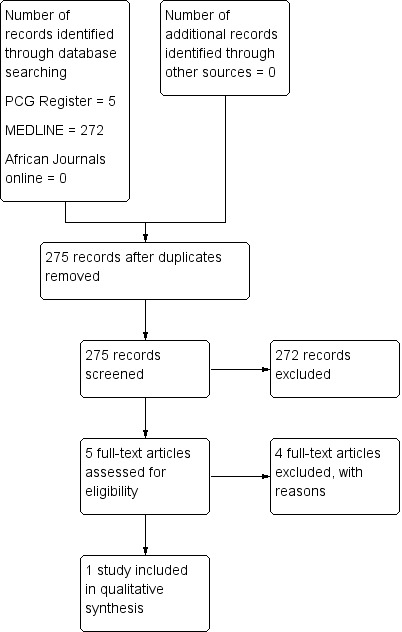
Study flow diagram.
Included studies
Only one study (Illingworth 1953) was included in this review. The trial was a quasi‐randomised trial (involving 210 women and their full term infants) and it evaluated the effect of extra fluid on milk production. This quasi‐randomised trial was carried out in a hospital in the UK during the 1950s. There were four maternity wards (two on the ground floor and two on the first floor). On each floor, all the women in one ward were advised to drink at least six pints of fluid per day and women in the other ward were not given any advice/instructions about how much fluid to drink (after 50 records had been obtained in each ward the ward changed to the other condition (i.e. the 'extra fluids' ward then gave no advice to women and the 'no advice' wards then advise women to drink extra fluid). Data were obtained from a total of 104 women in the 'extra fluid' condition and 106 women provided data in the 'usual fluids' control condition. To assess breast milk production the trialists reported on the results of 'test feeds' (the difference between the baby's weight pre‐ and post‐feed plus the volume of milk expressed after each feed) performed on the eighth day following the baby's birth.
Excluded studies
Four studies were excluded because they used a cross‐over design (Dusdieker 1985; Dusdieker 1986; Dusdieker 1990; Morse 1992).
Risk of bias in included studies
Allocation
The Illingworth 1953 study is a quasi‐randomised trial and as such is considered to be at 'high risk' of selection bias. The hospital wards (not the women themselves) were used for allocation and there appeared to be no allocation concealment.
Blinding
The study was considered to be at 'high risk' of bias. There appeared to be no form of blinding for participants or personnel. The women in the 'forced fluids' group knew they were required to drink extra fluids.
Incomplete outcome data
We assessed the Illingworth 1953 study as being at 'unclear' risk of attrition bias. Data collection continued until there at least 50 sets of data collected in each condition and the report does not mention whether there were any incomplete outcome data.
Selective reporting
The study design involved data collection until a set number of women had been included. Whilst unlikely, it is not clear from the trial report if any additional data items were collected and not reported, or if any results from participants were omitted from the analysis. We considered this study to be at 'unclear' risk of reporting bias.
Other potential sources of bias
The included study is considered to be at 'high risk' of bias due to the methods of data collection, which are laden with bias.
Effects of interventions
Primary outcomes
Satisfactory weight gain in the infant as defined by the trialists
This outcome was not reported in the included study.
Duration of exclusive breastfeeding (months)
This outcome was not reported in the included study.
Breast milk production as defined by trialists
The included study (Illingworth 1953) (involving 210 women and their full‐term infants) reported breast milk production but data were not in a suitable format for further analysis (no standard deviations or standard errors were reported). The babies were divided into three groups according to their weight: less that 6 lb 13 oz; between 6 lb 13 ¼ oz and 7 lb 13 oz; and more than 7 lb 13 oz. The trialist reported that, advising women to drink extra fluid did not result in increased breast milk production (as measured by test feeds throughout the baby's eighth day in hospital following birth) and in fact, for the heaviest group of babies, significantly more (P < 0.05) milk was produced by mothers who received no advice about fluid intake (mean 18 to 26 oz) compared to the mothers advised to drink extra fluids (mean 15 to 29 oz).
Secondary outcomes
The included study did not provide data relating to any of this review's secondary outcomes
Duration of any breastfeeding
Mother's satisfaction with breastfeeding as measured by the trialists
Hydration in mother as measured by the trialists
Dehydration in the infant as measured by the trialists
Episodes of gastrointestinal illness
Discussion
Summary of main results
We did not identify any randomised controlled trials for inclusion. We included one quasi‐randomised trial (involving 210 women and their full term infants) that examined the effect of extra fluids on breast milk production (Illingworth 1953). The study was considered to be at a high risk of bias. The report indicated that advising women to consume extra fluids did not translate to increased breast milk production, as measured by test feeds (also known as test weighing). At the time the study was conducted (the 1950s), it was common for babies in developed countries to be weighed before and after a feed, known as test weighing or test feeding. The practice is now not routinely practiced for term infants and is only sometimes practiced with ex‐premature infants as they develop their suck‐swallow skills over time. The concern with test weighing is the lack of precision: a comparison of infant weight change before and after milk intake, with the known amount of milk ingested, can range from ‐12.4 mL to 15 mL (Savenije 2006). Such imprecision could impact on care practices with premature infants, albeit unnecessarily. Therefore, although the trial reported by Illingworth 1953 did not demonstrate any effect of increased maternal fluid intake, it is possible that there may have been benefit, but that at most, it would have been a small amount (measured in mL) that would not impact on the overall care of a term infant.
The effect of additional fluids for breastfeeding mothers remains unknown, due to a lack of well‐conducted trials. However, because the physiological basis for any such improvement remains unclear, the conduct of further clinical trials may not be a priority.
Quality of the evidence
This review is based on one small quasi‐randomised controlled trial (Illingworth 1953) judged to be at a high risk of bias. Therefore, the overall quality of the evidence is considered to be low.
Potential biases in the review process
We attempted to minimise bias in the review process by following the review process as detailed in the Cochrane Handbook (Higgins 2011) and used the Cochrane Pregnancy and Childbirth Group's standard methods text. Two review authors independently assessed trial reports for eligibility and trial quality. We published a protocol to guide the development of this review (Ndikom 2010).
Agreements and disagreements with other studies or reviews
Other studies that have investigated the effect of extra fluids on milk production utilised a cross‐over design (a design which is not eligible for inclusion in this review). Dusdieker 1985, utilised a randomised cross‐over design to assess the effect of supplemental fluid intake on milk production. Milk production was not significantly affected by change in fluid intake. A similar study (Dusdieker 1990) evaluated the effect of prolonged supplemental fluid intake on human milk production. There was no significant relationship between milk production and prolonged supplemental fluid intake. Both studies showed that milk production was not significantly related to percentage increase in fluid intake.
Morse 1992 also studied the effect of altering fluid intake in lactating women using a cross‐over design. The trial assessed both milk yield in the mother and breast milk intake by the infant. The authors concluded that although milk supply decreased with decreased fluids and increased with increased fluids, this change however, was not statistically significant.
Authors' conclusions
Implications for practice.
There is no evidence from randomised controlled trials, and insufficient evidence from one low‐quality quasi‐randomised controlled trial to evaluate the practice of recommending extra fluids for breastfeeding mothers in order to increase milk production. There is not enough evidence to support advising breastfeeding mothers to increase fluid intake beyond what they are likely to require for comfort.
Implications for research.
The effect of additional fluids for breastfeeding mothers remains unknown, due to a lack of well‐conducted trials. However, because the physiological basis for any such improvement remains unclear, the conduct of further clinical trials may not be a priority.
Acknowledgements
We acknowledge the support provided by the Cochrane Pregnancy and Childbirth Group during the preparation of this review. Chizoma Ndikom (CN) received a fellowship award to attend the Reviews for Africa Programme (RAP, Nigeria) for the preparation of the protocol and review. We thank the RAP Nigeria branch of the South Africa Cochrane Centre for all the support given in the development of this review. CN acknowledges the College of Medicine, University of Ibadan for providing the enabling environment for staff development that enabled her to attend the RAP course.
As part of the pre‐publication editorial process, this review has been commented on by three peers (an editor and two referees who are external to the editorial team), a member of the Pregnancy and Childbirth Group's international panel of consumers and the Group's Statistical Adviser.
Appendices
Appendix 1. Search strategies
MEDLINE (1966 to 27 April 2014)
1. (additional or extra or supplement*).ti,ab.
2. exp Lactation/
3. exp Breast Feeding/
4. lactating.ti,ab.
5. ("breast feeding" or breastfeeding).ti,ab.
6. ("nursing mother" or "nursing mothers").ti,ab.
7. (fluid* or drink* or beverage*).ti,ab.
8. 1 and 7
9. 2 or 3 or 4 or 5 or 6
10. 8 and 9
African Journals Online (AJOL) (searched 27 April 2014)
We searched in all categories for:
(breastfeed* or "breast feed" or lactation or lactating or "nursing mothers" or "nursing mother" )
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Illingworth 1953.
| Methods | Quasi‐randomised design. | |
| Participants | 210 mothers of full term infants, all babies were included. | |
| Interventions | Forced fluids (104 women were advised to drink "at least six pints of fluid a day"). Control (106 women were not given any advice about fluid intake). |
|
| Outcomes | Breast milk production (measured by test feeds on day 8 combined with the volume of milk expressed after every feed throughout the day), gain in weight, duration of exclusive breastfeeding. | |
| Notes | There were 2 floors and 2 wards on each floor. On each floor, in 1 ward the women were advised to drink at least 6 pints of fluids a day and in the other ward the women were not given any advice about fluid intake. After 50 sets of data were obtained in each ward the wards swapped conditions (i.e. extra fluids switched to no advice and vice versa) until another 50 data sets were obtained (involving different women). "The birth weights of the babies studied were shown to be comparable," "Parity of the mothers, the incidence of breastfeeding and the mount of fluid taken were comparable in the two groups," Infants were divided into 3 groups according to birthweight: group A: birthweight less than 6 lb 13 oz; group B: birthweight from 6 lb 13¼ oz to 7lb 13 oz; group C: birthweight greater than 7 lb 13 oz. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Wards were used for allocation, the women were not randomised. |
| Allocation concealment (selection bias) | High risk | Women knew which group they belonged to so there was no allocation concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | There was no blinding as the personnel and women in intervention group knew they were to take additional fluids. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | There was no blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | The study design involved data collection until a set number of participants had been included. It is not clear from the report if any were missed. |
| Selective reporting (reporting bias) | Unclear risk | The study design involved data collection until a set number of participants had been included. Although unlikely, it is not clear from the report if any additional data items were collected and not reported, or if any results from participants were omitted from the analysis. |
| Other bias | High risk | The method of data collection is laden with bias. |
Characteristics of excluded studies [ordered by year of study]
| Study | Reason for exclusion |
|---|---|
| Dusdieker 1985 | The study utilised a cross‐over design. |
| Dusdieker 1986 | The study utilised a cross‐over design. |
| Dusdieker 1990 | The study utilised a cross‐over design. |
| Morse 1992 | The study utilised a cross‐over design. |
Differences between protocol and review
The title has been changed from 'Extra fluids for breastfeeding mothers' to 'Extra fluids for breastfeeding mothers for increasing milk production'.
The secondary outcome 'Dehydration in mother as measured by the trialists' has been changed to 'Hydration in the mother as measured by the trialists'.
The methods have been updated in accordance with the Cochrane Pregnancy and Childbirth Group's standard methods text and the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Contributions of authors
Chizoma Ndikom (CN) prepared the draft of the protocol and review. CN, Bukola Fawole (BF) and Roslyn Ilesanmi (RI) contributed to the development of the protocol and review. The review team worked on designing additional search strategies, with BF and CN and providing a methodological perspective. BF provided general advice on the protocol and review. All authors provided clinical, policy and consumer perspectives.
Sources of support
Internal sources
-
College of Medicine, University of Ibadan, Nigeria.
Permitted Chizoma Ndikom to attend the review for Africa programme
External sources
-
Review for Africa Programme (RAP) Nigeria Branch of Cochrane South Africa, Nigeria.
Chizoma Ndikom was awarded a Reviews for Africa Programme Fellowship (RAP, Nigeria), funded by a grant from the Nuffield Commonwealth Programme through the Nuffield Foundation
Declarations of interest
None known.
New
References
References to studies included in this review
Illingworth 1953 {published data only}
- Illingworth RS, Kilpatrick B. Lactation and fluid intake. Lancet 1953;2:1175‐7. [Google Scholar]
References to studies excluded from this review
Dusdieker 1985 {published data only}
- Dusdieker LB, Booth BM, Stumbo PJ, Eichenberger JM. Effect of supplemental fluids on human milk production. Journal of Pediatrics 1985;106:207‐11. [DOI] [PubMed] [Google Scholar]
Dusdieker 1986 {published data only}
- Dusdieker LB, Booth BM, Stumbo PJ, Eichenberger JM. Effect of supplemental fluids on human milk production. Breastfeeding Review 1986;9:18‐21. [DOI] [PubMed] [Google Scholar]
Dusdieker 1990 {published data only}
- Dusdieker LB, Stumbo PJ, Booth BM, Wilmoth RN. Prolonged maternal fluid supplementation in breast‐feeding. Pediatrics 1990;86:737‐40. [PubMed] [Google Scholar]
Morse 1992 {published data only}
- Morse JM, Ewing G, Gamble D, Donahue P. The effect of maternal fluid intake on breast milk supply: a pilot study. Canadian Journal of Public Health 1992;83(3):213‐6. [PubMed] [Google Scholar]
Additional references
Alamer 2009
- Alamer M. Effect of water restriction on lactation performance of Aardi goats under heat stress conditions. Small Ruminant Research 2009;84(1):76‐81. [Google Scholar]
Anderson 2006
- Anderson, A. Water intake during lactation. Journal of Human Lactation 2006;22:12‐3. [PubMed] [Google Scholar]
Arthur 1986
- Arthur SK, Green R. Fluid reabsorption by the proximal convoluted tubule of the kidney in lactating rats. Journal of Physiology 1986;371:267‐75. [DOI] [PMC free article] [PubMed] [Google Scholar]
Blyth 2002
- Blyth R, Creedy DK, Dennis CL, Moyle W, Pratt J, Vries SM. Effect of maternal confidence on breastfeeding duration: an application of breastfeeding self‐efficacy theory. Birth 2002;29(4):278–84. [DOI] [PubMed] [Google Scholar]
Brodribb 2007
- Brodribb W, Fallon AB, Hegney D, O'Brien M. Identifying predictors of the reasons women give for choosing to breastfeed. Journal of Human Lactation 2007;24(4):338‐44. [DOI] [PubMed] [Google Scholar]
Buckman 1973
- Buckman MT, Peake GT. Osmolar control of prolactin secretion in man. Science 1973;181:755‐7. [DOI] [PubMed] [Google Scholar]
Dearlove 1981
- Dearlove JC, Dearlove BM. Prolactin, fluid balance and lactation. British Journal of Obstetrics and Gynaecology 1981;88:652‐4. [DOI] [PubMed] [Google Scholar]
Dewey 2003
- Dewey KG, Nommsen‐Rivers LA, Heinig MJ, Cohen RJ. Risk factors for suboptimal infant breastfeeding behavior, delayed onset of lactation, and excess neonatal weight loss. Pediatrics 2003;112(3 Pt 1):607‐19. [DOI] [PubMed] [Google Scholar]
Ershow 1991
- Ershow AG, Brown LM, Cantor KP. Intake of tapwater and total water by pregnant and lactating women. American Journal of Public Health 1991;81(3):328‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Filer 1975
- Filer LJ. Maternal nutrition in lactation. Clinical Perinatology 1975;2:353. [PubMed] [Google Scholar]
Foo 2005
- Foo LL, Quek SJS, Ng SA, Lim MT, Deurenbergyap M. Breastfeeding prevalence and practices among Singaporean Chinese, Malay and Indian mothers. Health Promotion International 2005;20(3):229‐37. [DOI] [PubMed] [Google Scholar]
Food and Nutrition Board 1989
- Food, Nutrition Board. National Research Council: Recommended Dietary Allowances. Tenth. Washington, DC: National Academy of Sciences, 1989. [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Horowitz 1980
- Horowitz M, Higgins GD, Graham JJ, Berriman H, Harding PE. Effect of modification of fluid intake in the puerperium on serum prolactin levels and lactation. Medical Journal of Australia 1980;2(11):625‐6. [DOI] [PubMed] [Google Scholar]
Howie 1990
- Howie PW, Forsyth JS, Ogston SA, Clark A, Florey CV. Protective effect of breast feeding against infection. BMJ 1990;300:11‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Jones 2003
- Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS, for the Bellagio Child Survival Study Group. How many child deaths can we prevent this year?. Lancet 2003;362(9377):65‐71. [DOI] [PubMed] [Google Scholar]
Kalies 2005
- Kalies H, Heinrich J, Borte M, Schaaf B, Berg A, Kries R, et al. The effect of breastfeeding on weight gain in infants: results of a birth cohort study. European Journal of Medical Research 2005;10:36‐42. [PubMed] [Google Scholar]
Kirkland 2003
- Kirkland VL, Fein SB. Characterizing reasons for breastfeeding cessation throughout the first year postpartum using the construct of thriving. Journal of Human Lactation 2003;19(3):278–85. [DOI] [PubMed] [Google Scholar]
Kramer 2002
- Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database of Systematic Reviews 2002, Issue 1. [DOI: 10.1002/14651858.CD003517] [DOI] [PubMed] [Google Scholar]
Millar 2005
- Millar WJ, McLean H. Breastfeeding practices. Health Reports 2005;16(2):23‐31. [Google Scholar]
Montgomery 2002
- Montgomery KS. Nutrition Column an update on water needs during pregnancy and beyond. Journal of Perinatal Education 2002;11(2):40‐2. [DOI] [PMC free article] [PubMed] [Google Scholar]
National Health and Medical Research Council 2012
- National Health and Medical Research Council. Infant Feeding Guidelines. Canberra: Commonwealth of Australia, 2012. [Google Scholar]
Ndikom 2010
- Ndikom CM, Fawole B, Ilesanmi RE. Extra fluids for breastfeeding mothers. Cochrane Database of Systematic Reviews 2010, Issue 10. [DOI: 10.1002/14651858.CD008758] [DOI] [PMC free article] [PubMed] [Google Scholar]
Nommsen‐Rivers 2009
- Nommsen‐Rivers LA, Dewey KG. Growth of breastfed infants. Breastfeeding Medicine 2009;4(1):S45‐S49. [DOI] [PubMed] [Google Scholar]
O'Brien 2007
- OBrien M, Fallon A, Brodribb W, Hegney D. Reasons for stopping breastfeeding: what are they, what characteristics relate to them and are there underlying factors?. Birth Issues 2007;15(3‐4):105‐13. [Google Scholar]
Peng 2007
- Peng JJ, Somes SA, Rozeboom DW. Effect of system of feeding and watering on performance of lactating sows. Journal of Animal Science 2007;85(3):853‐60. [DOI] [PubMed] [Google Scholar]
Peters 2005
- Peters E, Wehkamp KH, Felberbaum RE, Krüger D, Linder R. Breastfeeding duration is determined by only a few factors. European Journal of Public Health 2005;16(2):162‐7. [DOI] [PubMed] [Google Scholar]
Prentice 1984
- Prentice AM, Lamb WH, Prentice A, Coward WA. The effect of water abstention on milk synthesis in lactating women. Clinical Science 1984;66(3):291‐8. [DOI] [PubMed] [Google Scholar]
RevMan 2012 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Savenije 2006
- Savenije OEM, Brand PLP. Accuracy and precision of test weighing to assess milk intake in newborn infants. Archives of Disease in Childhood: Fetal & Neonatal 2006;91(5):F330‐332. [DOI: 10.1136/adc.2005.091876] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sheehan 2001
- Sheehan D, Krueger P, Watt S, Sword W, Bridle B. The Ontario Mother and Infant Survey: breastfeeding outcomes. Journal of Human Lactation 2001;17:211‐9. [DOI] [PubMed] [Google Scholar]
Smith 2009
- Smith J, Dunstone M, Elliott‐Rudder M. Health professional knowledge of breastfeeding. Journal of Human Lactation 2009;25(3):350‐7. [DOI] [PubMed] [Google Scholar]
Story 2008
- Story L, Parish T. Breastfeeding helps prevent two major infant illnesses. Internet Journal of Allied Health Services and Practices 2008; Vol. 6, issue 3.
Stumbo 1985
- Stumbo PJ, Booth BM, Eichenberger JM, Dusdieker LB. Water intakes of lactating women. American Journal of Clinical Nutrition 1985;42(5):870‐6. [DOI] [PubMed] [Google Scholar]
WHO 2002
- WHO. Nutrient Adequacy of Exclusive Breastfeeding for the Term Infant During the First Six Months of Life. Geneva: WHO, 2002. [Google Scholar]
WHO 2009
- WHO. Breastfeeding. www.who.int/topic/breastfeeding/en/ (accessed 22 October 2009).
WHO 2010
- WHO. Infant and Young Child Feeding. WHO Data Base 2010 www.int/mediacentre/ factsheets accessed august,2012, issue 342.
Wiessinger 1996
- Wiessinger D. Watch your language!. Journal of Human Lactation 1996;12(1):1‐4. [DOI] [PubMed] [Google Scholar]
Woods 2005
- Woods DL (editor). Fluid requirement. Newborn Care Manual (http://www.gfmer.ch/PEP/pdf/UNIT‐21‐2005.pdf) (accessed 23 October 2009) 2005.