

Abstract
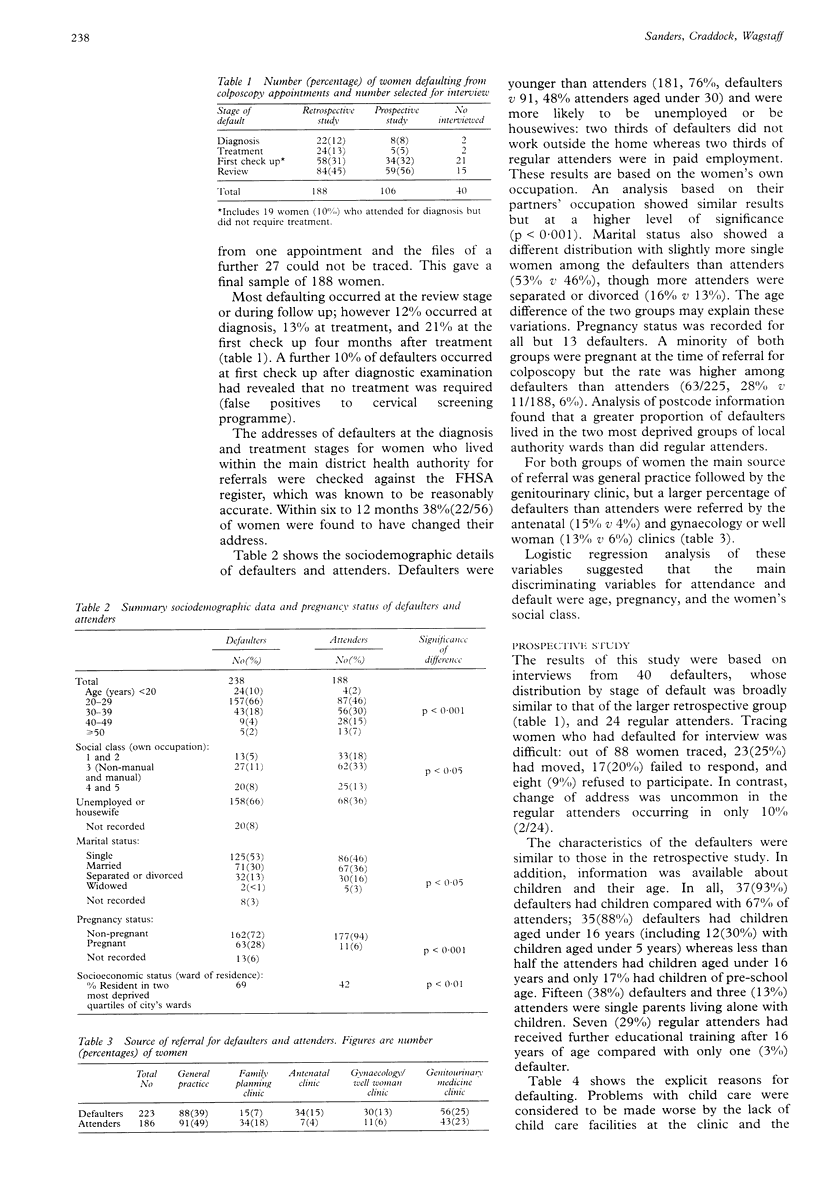
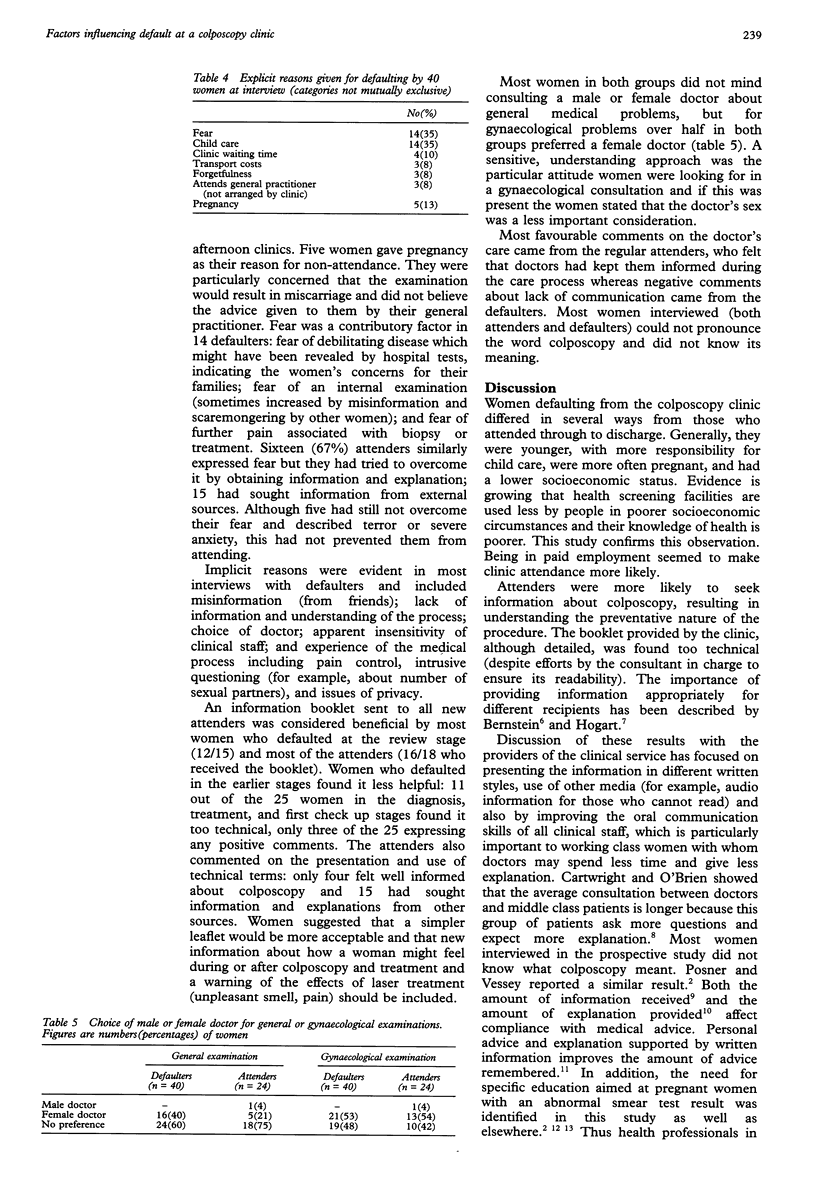
OBJECTIVE--To identify factors reducing compliance at diagnosis, treatment, and review stages among women referred with abnormal cervical smears to a hospital colposcopy clinic. DESIGN--Retrospective analysis of sociodemographic data from hospital notes of the attenders and defaulters during one year (1989-90) and prospective collection of information by structured interviews of a sample of defaulters and attenders during five months (May-September 1990). SETTING--One hospital colposcopy clinic. PATIENTS--238 women defaulting on two consecutive occasions and 188 attending regularly (retrospective analysis) and a subset of 40 defaulters and 24 attenders (interview sample). MAIN MEASURES--Sociodemographic data and interview responses about attitudes, behaviour, choice, accessibility cultural understanding, communications, and emotional response. RESULTS--22 (12%) women defaulted at diagnosis, 24(13%) at treatment, 39(21%) at the first check up after treatment, and 84(45%) at the review stage; 19(10%) defaulted from the first check up after diagnostic examination revealed no need for treatment. Age and social class differed between the two groups. 181(76%) defaulters were under 30 compared with 91(48%) attenders; 14(6%) compared with 41(23%) were over 40(p < 0.001). The proportion of women in social classes 4 and 5 was 33%(20/60) for defaulters and 21%(25/120) for attenders (p < 0.05) and unemployed was 66%(158/238) and 36%(68/188) respectively. 63(28%) defaulters were pregnant compared with 11(6%) attenders (p < 0.001). More defaulters came from gynaecology or antenatal clinics. Most defaulters (93%) had child care responsibilities and they knew and understood less about colposcopy. Their explicit reasons for defaulting included child care commitments and fear and their implicit reasons lack of understanding, inaccessibility of information, and staff attitudes. CONCLUSIONS--Compliance may be improved by promoting women's understanding of treatment and encouraging health professionals to develop a service more sensitive to the various needs of women in different socioeconomic groups.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- EGBERT L. D., BATTIT G. E., WELCH C. E., BARTLETT M. K. REDUCTION OF POSTOPERATIVE PAIN BY ENCOURAGEMENT AND INSTRUCTION OF PATIENTS. A STUDY OF DOCTOR-PATIENT RAPPORT. N Engl J Med. 1964 Apr 16;270:825–827. doi: 10.1056/NEJM196404162701606. [DOI] [PubMed] [Google Scholar]
- Skipper J. K., Jr, Leonard R. C. Children, stress, and hospitalization: a field experiment. J Health Soc Behav. 1968 Dec;9(4):275–287. [PubMed] [Google Scholar]