

Abstract
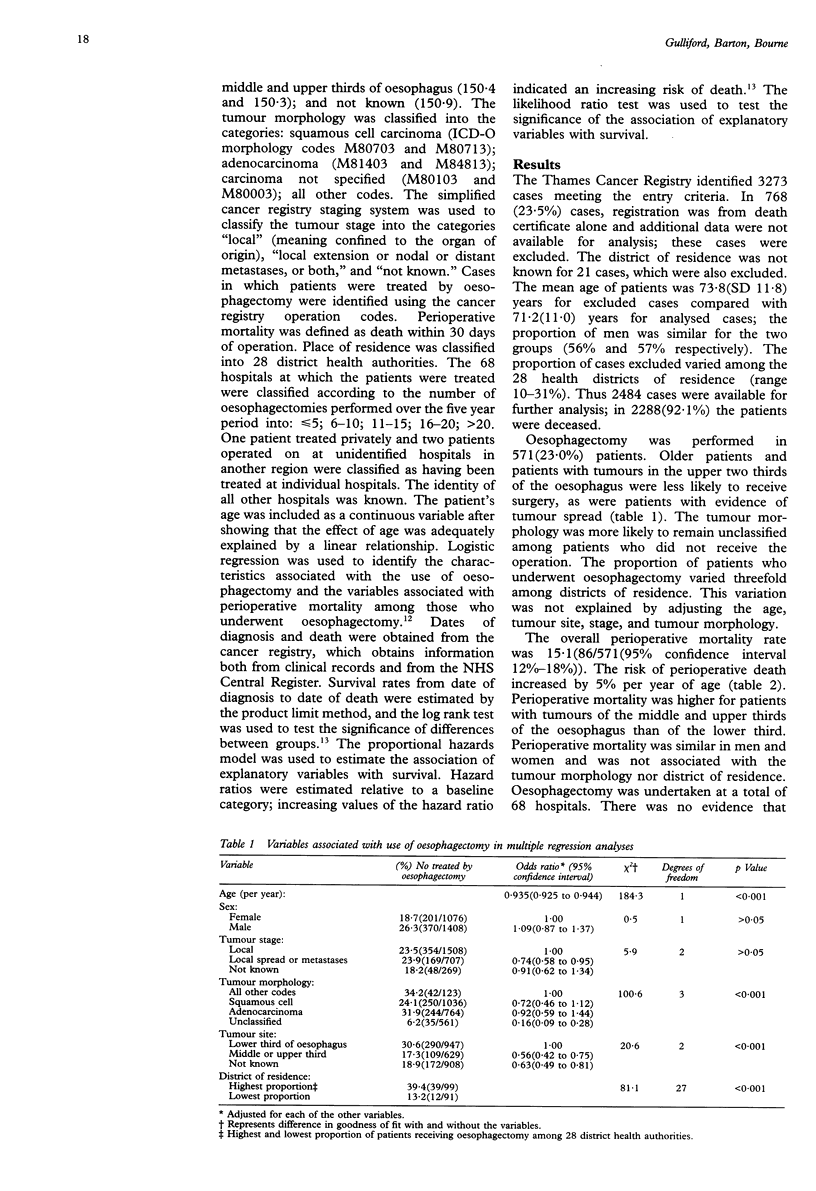
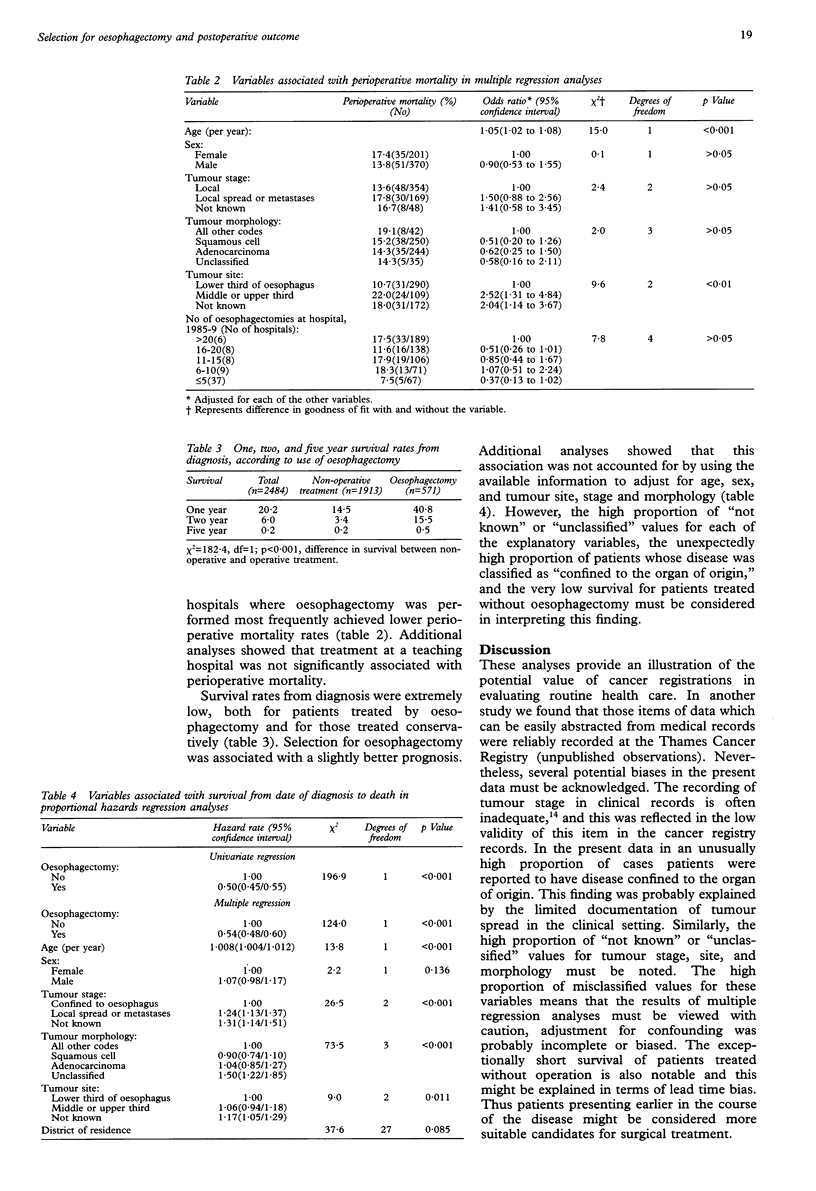
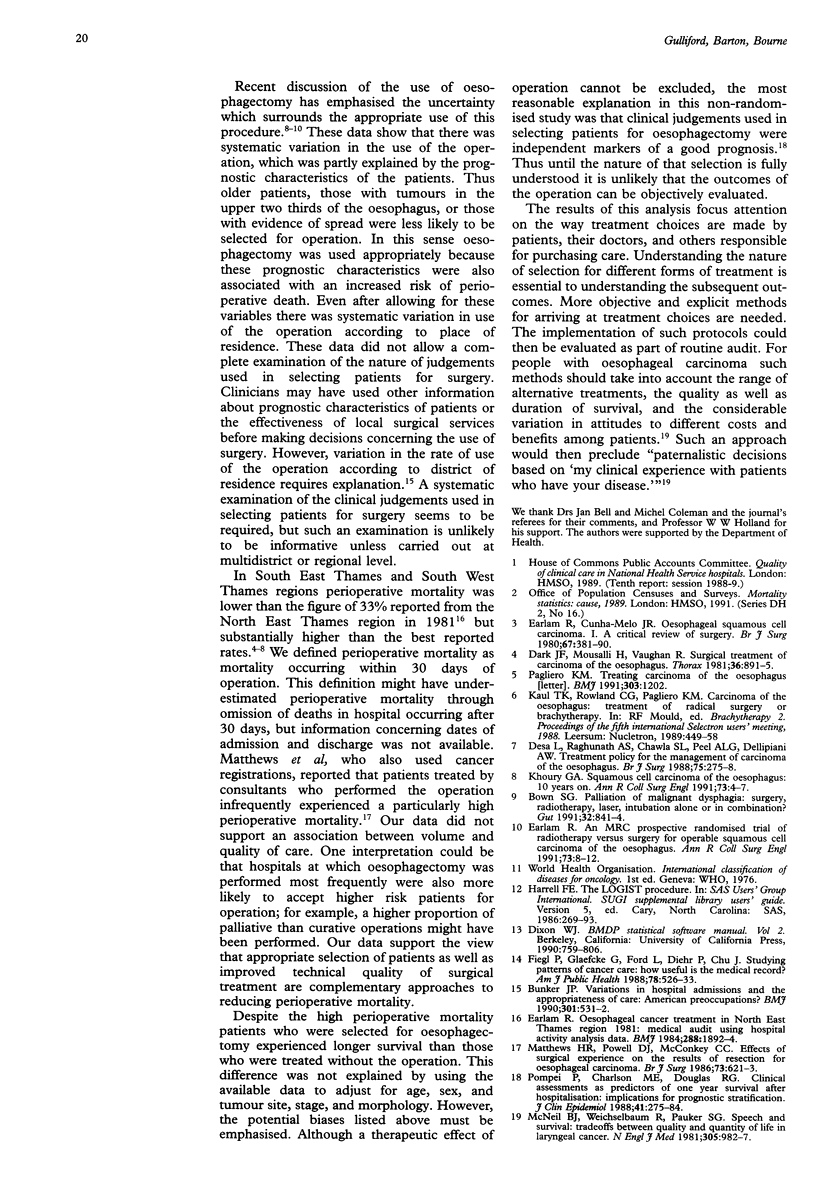
OBJECTIVE--To measure the extent of use of, and perioperative mortality from, oesophagectomy for carcinoma of the oesophagus, and to examine the association between oesophagectomy and long term survival. DESIGN--Retrospective cohort study of cases of oesophageal carcinoma notified to the Thames Cancer Registry. SETTING--South East Thames and South West Thames health regions. PATIENTS--3273 patients first registered with carcinoma of the oesophagus during 1985-9, 789 of whom were excluded because of incomplete data, leaving 2484 (75.9%) for further analysis. MAIN MEASURES--Treatment of oesophagectomy, mortality within 30 days of oesophagectomy, and duration of survival from date of diagnosis to death, according to patient and tumour characteristics. RESULTS--Oesophagectomy was performed in 571(23.0%) patients. Its use decreased with increasing age (odds ratio (95% confidence interval) 0.935(0.925 to 0.944) per year) and was less common for tumours of the middle or upper third of the oesophagus than the lower third (0.56(0.42 to 0.75)). The proportion of patients undergoing oesophagectomy varied threefold among the 28 districts of residence. The perioperative mortality rate was 15.1(86/571) (12% to 18%); it increased with age (odds ratio 1.05(1.02 to 1.08) per year) and for tumours of the middle or upper third of the oesophagus compared with the lower third (2.52(1.31 to 4.84)). Long term survival was slightly higher for patients undergoing oesophagectomy (0.5% v 0.2%). CONCLUSIONS--Despite a high perioperative mortality rate patients selected for oesophagectomy showed better long term survival than those who were not, suggesting that clinical judgements used in selection were independent markers of a better prognosis. The nature of this selection needs to be more completely characterised to permit a valid evaluation of outcome of oesophagectomy.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bown S. G. Palliation of malignant dysphagia: surgery, radiotherapy, laser, intubation alone or in combination? Gut. 1991 Aug;32(8):841–844. doi: 10.1136/gut.32.8.841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bunker J. P. Variations in hospital admissions and the appropriateness of care: American preoccupations? BMJ. 1990 Sep 15;301(6751):531–532. doi: 10.1136/bmj.301.6751.531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dark J. F., Mousalli H., Vaughan R. Surgical treatment of carcinoma of the oesophagus. Thorax. 1981 Dec;36(12):891–895. doi: 10.1136/thx.36.12.891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Desa L., Raghunath A. S., Chawla S. L., Peel A. L., Dellipiani A. W. Treatment policy for the management of carcinoma of the oesophagus. Br J Surg. 1988 Mar;75(3):275–278. doi: 10.1002/bjs.1800750329. [DOI] [PubMed] [Google Scholar]
- Earlam R. An MRC prospective randomised trial of radiotherapy versus surgery for operable squamous cell carcinoma of the oesophagus. Ann R Coll Surg Engl. 1991 Jan;73(1):8–12. [PMC free article] [PubMed] [Google Scholar]
- Earlam R., Cunha-Melo J. R. Oesophageal squamous cell carcinoma: I. A critical review of surgery. Br J Surg. 1980 Jun;67(6):381–390. doi: 10.1002/bjs.1800670602. [DOI] [PubMed] [Google Scholar]
- Earlam R. Oesophageal cancer treatment in North East Thames region, 1981: medical audit using Hospital Activity Analysis data. Br Med J (Clin Res Ed) 1984 Jun 23;288(6434):1892–1894. doi: 10.1136/bmj.288.6434.1892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feigl P., Glaefke G., Ford L., Diehr P., Chu J. Studying patterns of cancer care: how useful is the medical record? Am J Public Health. 1988 May;78(5):526–533. doi: 10.2105/ajph.78.5.526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khoury G. A. Squamous cell carcinoma of the oesophagus: 10 years on. Ann R Coll Surg Engl. 1991 Jan;73(1):4–7. [PMC free article] [PubMed] [Google Scholar]
- Matthews H. R., Powell D. J., McConkey C. C. Effect of surgical experience on the results of resection for oesophageal carcinoma. Br J Surg. 1986 Aug;73(8):621–623. doi: 10.1002/bjs.1800730811. [DOI] [PubMed] [Google Scholar]
- McNeil B. J., Weichselbaum R., Pauker S. G. Speech and survival: tradeoffs between quality and quantity of life in laryngeal cancer. N Engl J Med. 1981 Oct 22;305(17):982–987. doi: 10.1056/NEJM198110223051704. [DOI] [PubMed] [Google Scholar]
- Pagliero K. M. Treating carcinoma of the oesophagus. BMJ. 1991 Nov 9;303(6811):1202–1202. doi: 10.1136/bmj.303.6811.1202-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pompei P., Charlson M. E., Douglas R. G., Jr Clinical assessments as predictors of one year survival after hospitalization: implications for prognostic stratification. J Clin Epidemiol. 1988;41(3):275–284. doi: 10.1016/0895-4356(88)90132-1. [DOI] [PubMed] [Google Scholar]