

Abstract
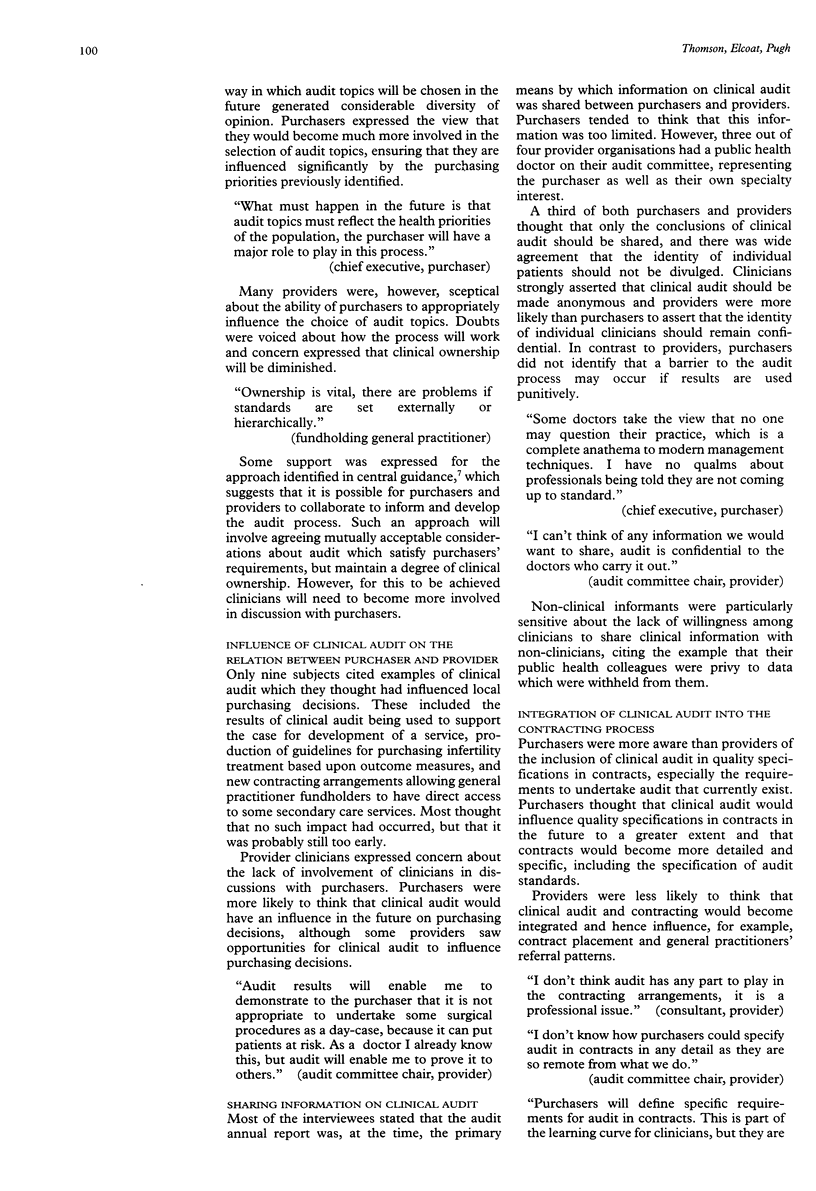
OBJECTIVES--To explore and describe the views on clinical audit of healthcare purchasers and providers, and in particular the interaction between them, and hence to help the future development of an appropriate interaction between purchasers and providers. DESIGN-- Semistructured interviews. SETTING--Four purchaser and provider pairings in the former Northern Region of the National Health Service (NHS) in England. SUBJECTS--Chief executives, contracts managers, quality and audit leaders, directors of public health, consultants, general practitioners, audit support staff, and practice managers (total 42). MAIN MEASURES--Attitudes on the present state and future development of clinical audit. RESULTS--Purchasers and providers shared common views on the purpose of clinical audit, but there were important differences in their views on the level and appropriateness of involvement of health care purchasers, integration with present NHS structures and processes (including contracting and the internal market), priority setting for clinical audit, the effects of clinical audit on service development and purchasing, change in behaviour, and the sharing of information on the outcomes of clinical audit. CONCLUSIONS--There are important differences in attitudes towards, and expectations of, clinical audit between health care purchasers and providers, at least in part due to the limited contact between them on audit to date. The nature of the relation and dialogue between purchasers and providers will be critical in determining whether clinical audit meets the differing aspirations of both groups, while achieving the ultimate goal of improving the quality of patient care.
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Black N., Thompson E. Obstacles to medical audit: British doctors speak. Soc Sci Med. 1993 Apr;36(7):849–856. doi: 10.1016/0277-9536(93)90077-h. [DOI] [PubMed] [Google Scholar]
- Grimshaw J. M., Russell I. T. Achieving health gain through clinical guidelines II: Ensuring guidelines change medical practice. Qual Health Care. 1994 Mar;3(1):45–52. doi: 10.1136/qshc.3.1.45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gumpert R., Lyons C. Setting up a district audit programme. BMJ. 1990 Jul 21;301(6744):162–165. doi: 10.1136/bmj.301.6744.162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hopkins A., Maxwell R. Contracts and quality of care. BMJ. 1990 Apr 7;300(6729):919–922. doi: 10.1136/bmj.300.6729.919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith H. E., Russell G. I., Frew A. J., Dawes P. T. Medical audit: the differing perspectives of managers and clinicians. J R Coll Physicians Lond. 1992 Apr;26(2):177–180. [PMC free article] [PubMed] [Google Scholar]
- Thomson R. G., Barton A. G. Is audit running out of steam? Qual Health Care. 1994 Dec;3(4):225–229. doi: 10.1136/qshc.3.4.225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomson R. The purchaser role in provider quality: lessons from the United States. Qual Health Care. 1994 Jun;3(2):65–66. doi: 10.1136/qshc.3.2.65. [DOI] [PMC free article] [PubMed] [Google Scholar]