

Abstract
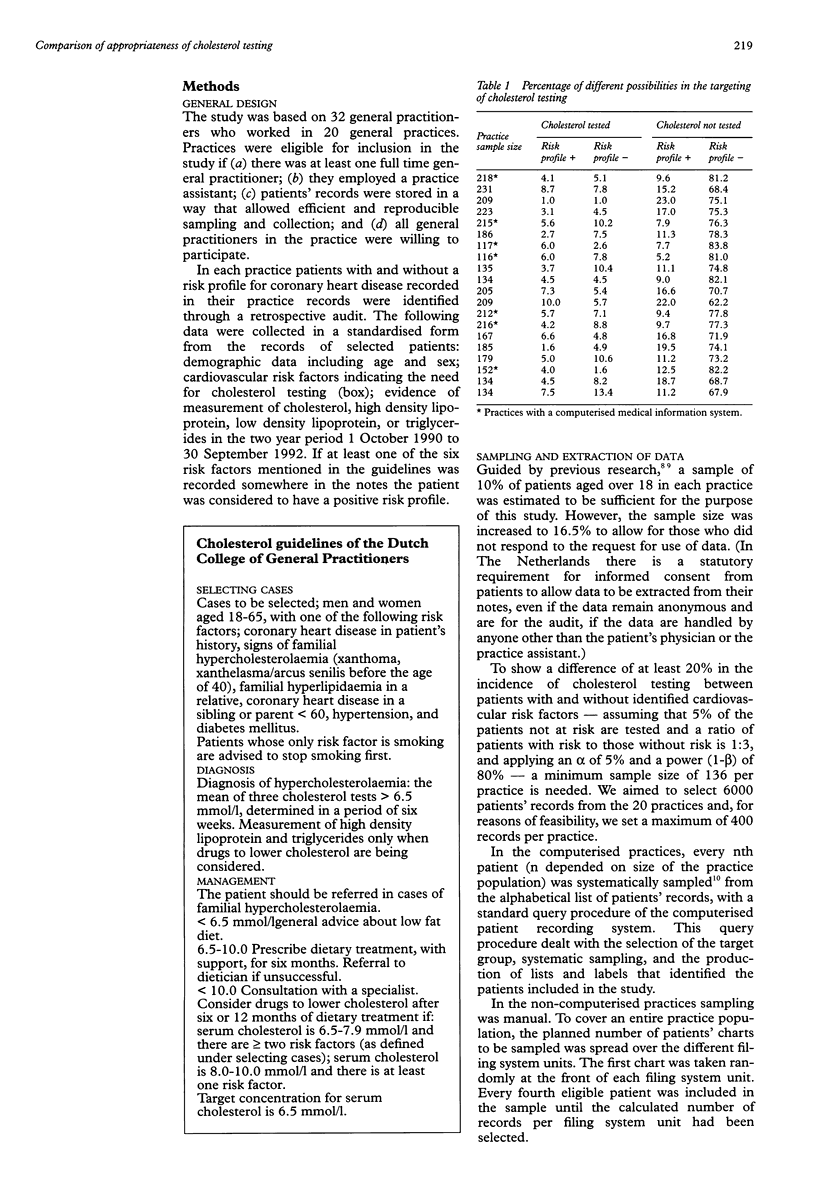
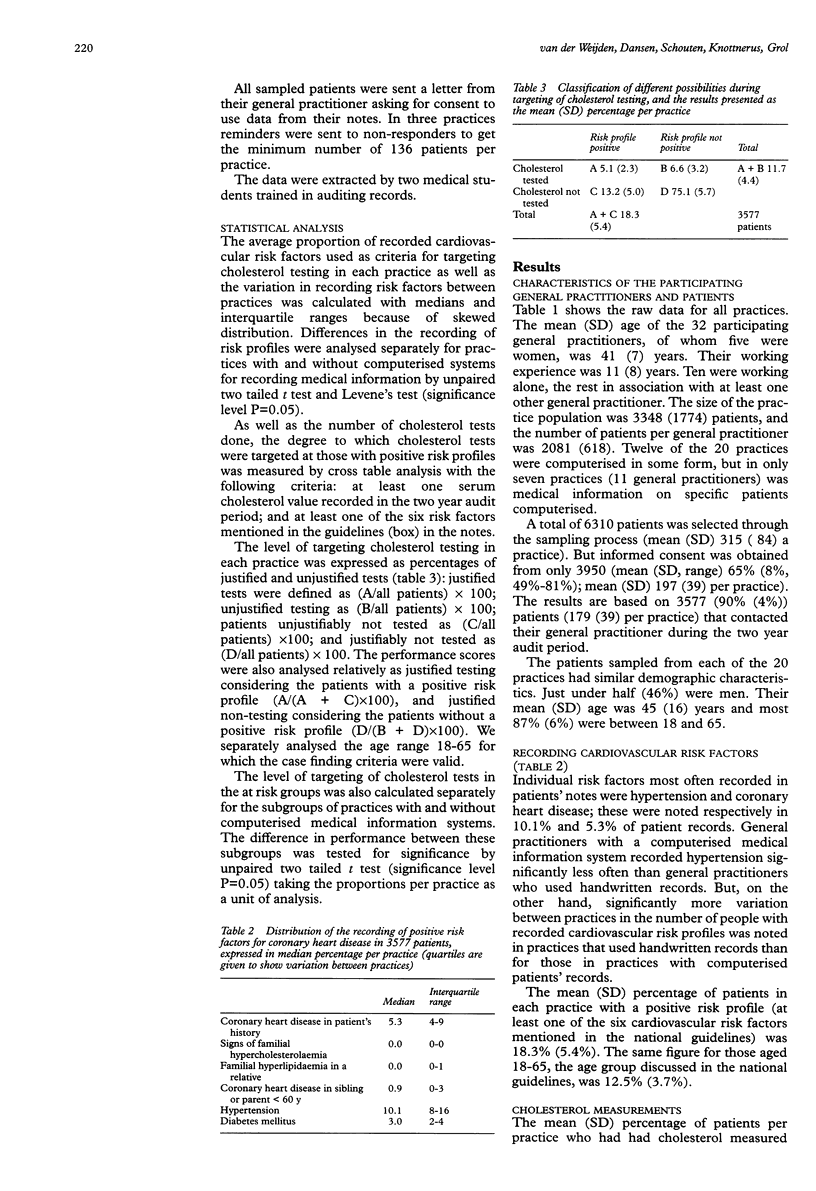
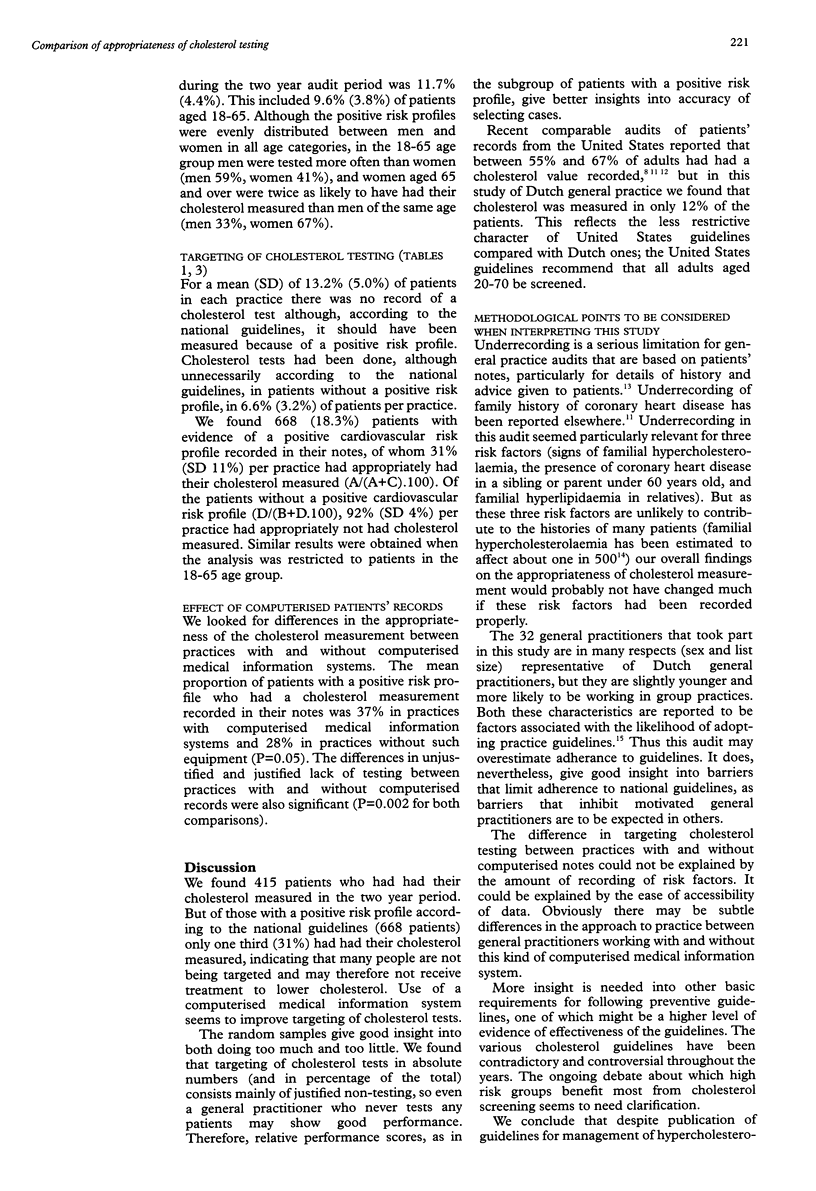
OBJECTIVE: To compare the profiles of those patients selected by general practitioners for measurement of serum cholesterol with the recommended profiles for opportunistic cholesterol testing described in the national practice guidelines published by the Dutch College of General Practitioners. DESIGN: Retrospective audit of general practitioners' records. MATERIALS: Practice records of 3577 adult patients systematically sampled from 20 general practices. MAIN MEASURES: With criteria set by the national guidelines, the proportion of patients per practice (a) for whom cholesterol testing would be considered justified, and (b) for whom cholesterol testing would be considered unjustified, and the proportion of patients within each of these groups who had had a cholesterol measurement recorded. RESULTS: Cholesterol tests were performed on 415 (11.7%) of the 3577 patients. National guidelines on the management of hypercholesterolaemia state that a positive cardiovascular risk profile is an indication for cholesterol measurement. Just under one fifth (668) of the patients in this study were recorded as having a positive cardiovascular risk profile, but only 31% of these had had their cholesterol measured. Of the patients without recorded evidence of a positive cardiovascular risk profile cholesterol had been measured in 8%. Restricting the analyses to the age group 18-65 (n = 3060) of whom 12.5% had a positive risk profile, did not improve the results. In practices with a computerised information system 37% of patients with recorded evidence of a positive cardiovascular risk profile had had their cholesterol measured. CONCLUSIONS: Cholesterol testing was not targeted as selectively as recommended by the national guidelines. The major problem was failure to test those likely to benefit. Improving the targeting of cholesterol measurements would undoubtedly increase the workload of general practitioners. If the national guidelines are to have an effect on health promotion the first step must be to increase the proportion of patients with positive cardiovascular risk profiles who get their cholesterol tested. A major factor in successfully selecting cases seems to be that practices are equipped with a computerised medical information system.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Davey Smith G., Pekkanen J. Should there be a moratorium on the use of cholesterol lowering drugs? BMJ. 1992 Feb 15;304(6824):431–434. doi: 10.1136/bmj.304.6824.431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunnigan M. G. The problem with cholesterol. BMJ. 1993 May 22;306(6889):1355–1356. doi: 10.1136/bmj.306.6889.1355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grol R. National standard setting for quality of care in general practice: attitudes of general practitioners and response to a set of standards. Br J Gen Pract. 1990 Sep;40(338):361–364. [PMC free article] [PubMed] [Google Scholar]
- Hudson J. W., Keefe C. W., Hogan A. J. Cholesterol measurement and treatment in community practices. J Fam Pract. 1990 Aug;31(2):139–144. [PubMed] [Google Scholar]
- Law M. R., Thompson S. G., Wald N. J. Assessing possible hazards of reducing serum cholesterol. BMJ. 1994 Feb 5;308(6925):373–379. doi: 10.1136/bmj.308.6925.373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Otradovec K., Blake R. L., Jr, Parker B. M. An assessment of the practice of preventive cardiology in an academic health center. J Fam Pract. 1985 Aug;21(2):125–129. [PubMed] [Google Scholar]
- Rethans J. J., Martin E., Metsemakers J. To what extent do clinical notes by general practitioners reflect actual medical performance? A study using simulated patients. Br J Gen Pract. 1994 Apr;44(381):153–156. [PMC free article] [PubMed] [Google Scholar]
- Robinson M. K., DeHaven M. J., Wallace J. B., Fost T. Hypercholesterolemia: case finding in family practice. South Med J. 1992 Nov;85(11):1091–1095. [PubMed] [Google Scholar]
- van der Weijden T., Hutten J. B., Brandenburg B. J., Grol R. P., van der Velden K. Cholesterol management in Dutch general practice. A comparison with national guidelines. Dutch College of General Practitioners. Scand J Prim Health Care. 1994 Dec;12(4):281–288. doi: 10.3109/02813439409029254. [DOI] [PubMed] [Google Scholar]
- van der Weijden T., Höppener P., Schouten B. Computerized sampling techniques. J Fam Pract. 1995 Feb;40(2):123–123. [PubMed] [Google Scholar]