

In recent years, endoscopic retrograde appendicitis therapy (ERAT) has been widely used in the treatment of acute uncomplex appendicitis 1 . However, the treatment of a periappendiceal abscess has always been a challenge. Early surgery may cause serious complications such as total peritonitis and postoperative anastomotic leakage 2 . We report a case of acute appendicitis with a giant periappendiceal abscess and intestinal obstruction. Through ERAT, full endoscopic drainage was achieved and the intestinal obstruction was quickly resolved.
A 34-year-old woman presented with abdominal pain, nausea, vomiting, and no anal exhaust defecation for 2 days. Computed tomography (CT) showed acute appendicitis with a giant periappendiceal abscess and intestinal obstruction ( Fig. 1 ). After informed consent was given, an ERAT procedure was performed ( Video 1 ) with the patient under general anesthesia. The intestine was prepared through colon dialysis. Colonoscopy showed significant protrusion of the mucosa around the appendix. The appendiceal cavity was successfully incised using a duodenal papillary incision knife ( Fig. 2 ). Then a guidewire was delivered to the giant periappendiceal abscess, which was clearly visualized by iohexol radiography ( Fig. 3 ). After that, a biliary plastic stent was successfully implanted. A large amount of pus flowed out of the stent ( Fig. 4 ). The procedure was performed successfully without any adverse events. Postoperative abdominal X-ray indicated no signs of intestinal obstruction. The patient recovered well.
Fig. 1.
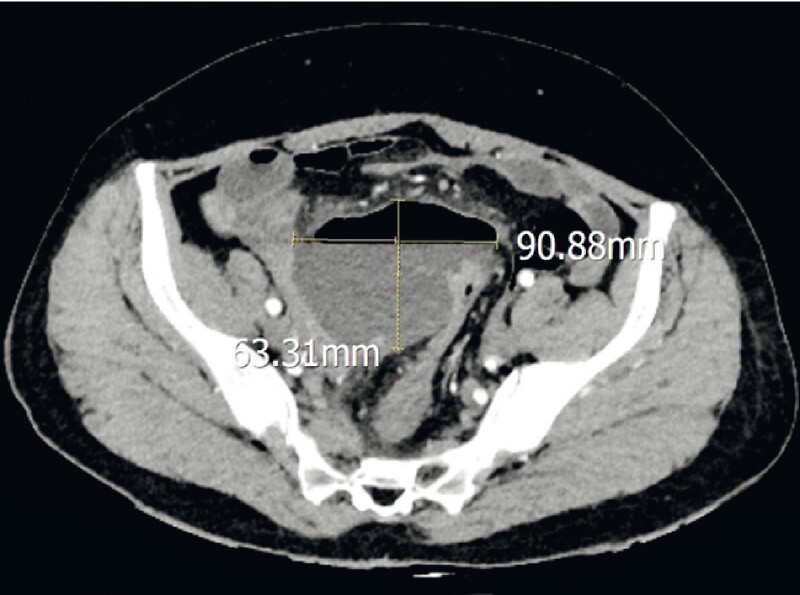
Before endoscopic retrograde appendicitis therapy, computed tomography (CT) showed acute appendicitis with a giant periappendiceal abscess (9.0 cm × 6.3 cm) and intestinal obstruction.
Fig. 2.
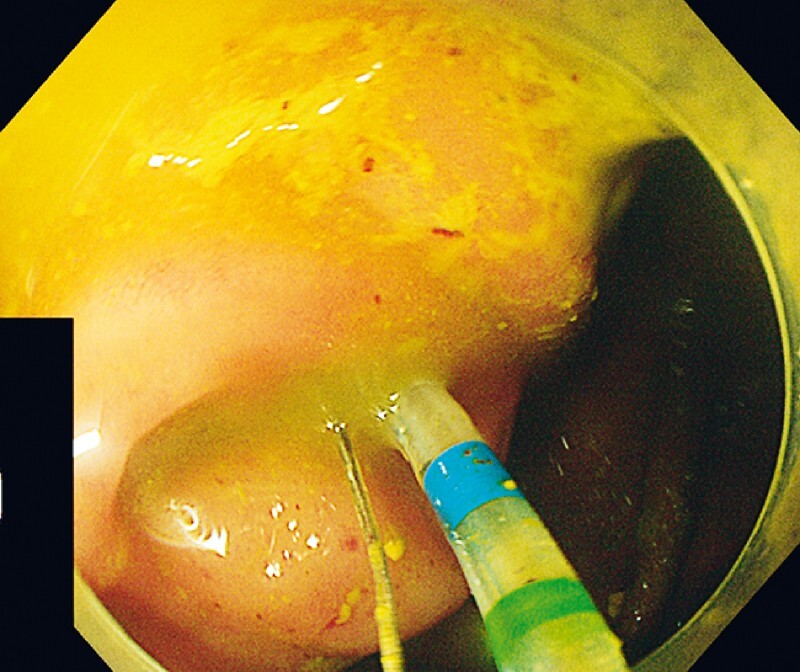
Colonoscopy showed protrusion of the mucosa around the appendix. The duodenal papillary incision was used for successful insertion into the appendix cavity.
Fig. 3.
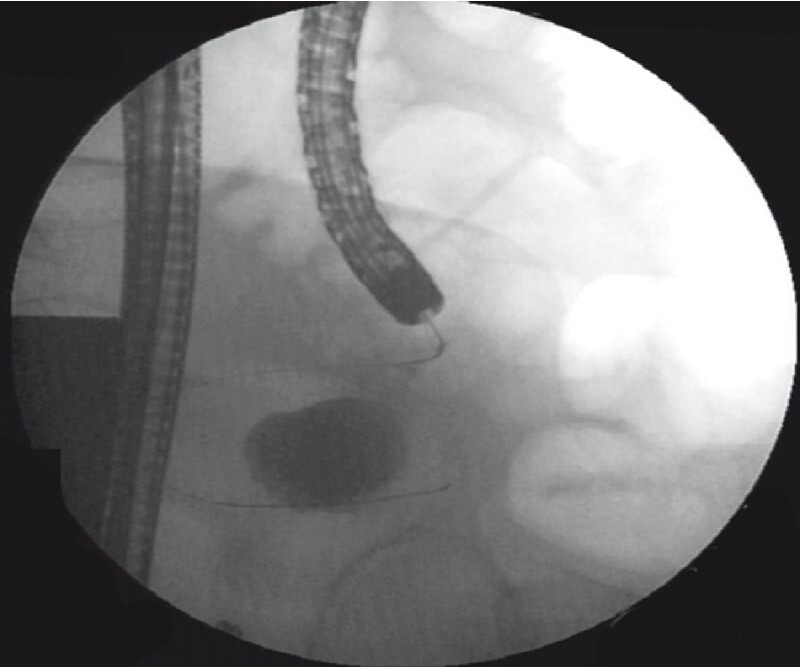
The guidewire was delivered to the appendix pus cavity, and then iohexol radiography clearly showed the giant periappendiceal abscess.
Fig. 4.
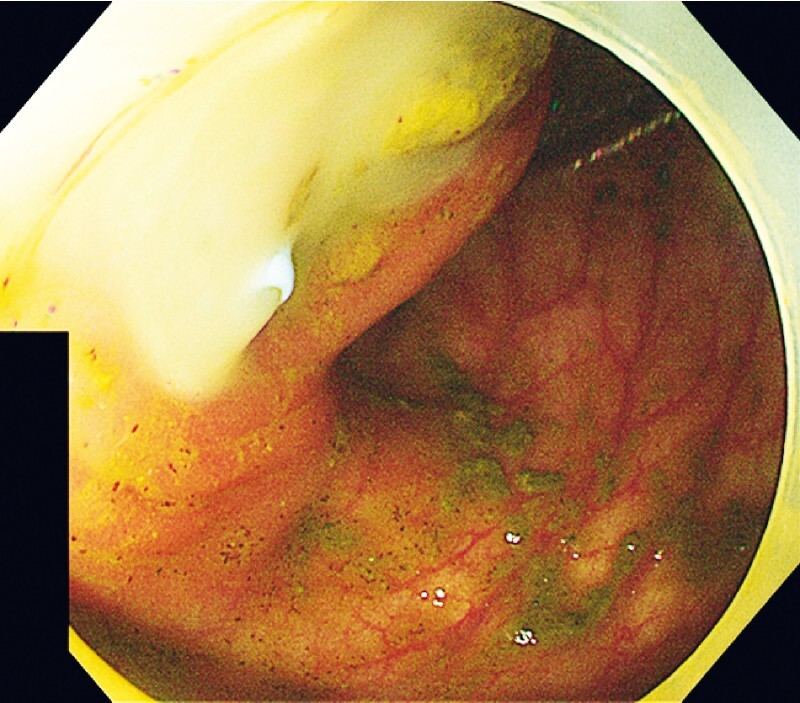
After a plastic biliary stent was implanted into the appendix pus cavity, a large amount of pus flowed out of the stent.
Video 1 Endoscopic retrograde appendicitis therapy for continuous drainage of giant periappendiceal abscess and the process of removing the stent under colonoscopy.
Follow-up CT after 2 months showed that the periappendiceal abscess had fully disappeared ( Fig. 5 ). The stent was removed under colonoscopy ( Video 1 ). ERAT may be a safe and effective method for adequate drainage of a periappendiceal abscess in the early stage. Further clinical studies with larger samples and long-term follow-up are needed to evaluate this.
Fig. 5.

Follow-up CT after 2 months showed that the periappendiceal abscess had fully disappeared and the stent was in place.
Endoscopy_UCTN_Code_CCL_1AD_2AG
Acknowledgments
The authors thank the patient involved for permitting the publication of the data regarding his case.
Footnotes
Competing interests The authors declare that they have no conflict of interest.
Endoscopy E-Videos : https://eref.thieme.de/e-videos .
E-Videos is an open access online section of the journal Endoscopy , reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high-quality video and are published with a Creative Commons CC-BY license. Endoscopy E-Videos qualify for HINARI discounts and waivers and eligibility is automatically checked during the submission process. We grant 100% waivers to articles whose corresponding authors are based in Group A countries and 50% waivers to those who are based in Group B countries as classified by Research4Life (see: https://www.research4life.org/access/eligibility/ ). This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
References
- 1.Ullah S, Ali F S, Shi M et al. Is it time for global adoption of endoscopic retrograde appendicitis therapy of acute appendicitis? Clin Res Hepatol Gastroenterol. 2022;46:102049. doi: 10.1016/j.clinre.2022.102049. [DOI] [PubMed] [Google Scholar]
- 2.Akingboye A A, Mahmood F, Zaman S et al. Early versus delayed (interval) appendicectomy for the management of appendicular abscess and phlegmon: a systematic review and meta-analysis. Langenbecks Arch Surg. 2021;406:1341–1351. doi: 10.1007/s00423-020-02042-3. [DOI] [PubMed] [Google Scholar]