

Abstract
Objective
Describe how people with lower limb spasticity present for treatment in routine clinical practice.
Methods
Prospective, observational study (Clinicaltrials.gov: NCT04050527) of ambulatory adult patients (≥ 18 years) with unilateral lower limb spasticity (able to take ≥ 5 steps with or without assistance) presenting for routine spasticity management, including treatment with abobotulinumtoxinA.
Results
The study population included 430 adults with lower limb spasticity. Despite their relatively young age (mean ± standard deviation 53.7 ± 13.9 years), only 20% of patients were employed. Most patients had an acquired brain injury due to cerebrovascular disease; 84.1% reported having concomitant upper limb spasticity. Using the Leg Activity Measure, most patients reported no or only mild difficulties in performing hygiene/positioning tasks, while 80.7% had at least mild difficulty with indoor ambulation and 90.5% had at least mild difficulty with walking outdoors. Sensory, communication and/or cognitive impairments were also common. At the first treatment cycle, 50.7% of patients set active function primary goals, including locomotion transferring or standing.
Conclusion
These observations highlight the complexity of presentation that must be considered when setting treatment goals for lower limb spasticity and emphasize the types of impairment and activity (functional) limitations that treating teams may expect to encounter in their patients and should cover in their initial and follow-up assessments.
LAY ABSTRACT
Stroke survivors with leg spasticity (an abnormal increase in muscle activity resulting in stiffness of muscle) are often treated with botulinum toxin to reduce the spasticity and enable physical therapy. This paper presents an overview of data from the start of the AboLiSh study, which explores how leg spasticity is managed with abobotulinumtoxinA (a type of botulinum toxin) in everyday practice. Findings from this study (including 384 patients with lower limb spasticity from 9 countries) show the complexity of problems that people with leg spasticity live with. Most stroke survivors were also treated for arm spasticity, and many patients also had significant motor, sensory, communication and cognitive impairments. For stroke survivors who are still able to walk at least 5 steps, the priority treatment goal was to improve their walking, followed by pain management and prevention of contractures (muscle and joint shortening or deformity). All these factors are important for clinicians to consider when agreeing treatment goals with stroke survivors who are living with leg spasticity so that the treatment meets their individual needs.
Key words: abobotulinumtoxinA, botulinum toxin A, goal attainment scaling, lower limb spasticity, LegA, rehabilitation,
Spasticity is one of the most frequent symptoms associated with a variety of conditions including stroke, cerebral palsy (CP), spinal cord or traumatic brain injury, and multiple sclerosis. Although a substantial proportion of people living with these long-term conditions have spasticity affecting the lower limbs (e.g. it is estimated to affect approximately one-third of stroke survivors (1)), there remains a surprising lack of global epidemiological data on its overall prevalence, severity, and presentation patterns, highlighting an overall lack of attention paid to this common and often disabling problem (1, 2). Importantly, there remains limited information regarding spasticity as a barrier to rehabilitation and its functional implications when occurring post-stroke (and other upper motor neurone lesions). The full socioeconomic burden of lower limb spasticity also remains largely uninvestigated. Clinically, it is known that slow walking speed and inability to ambulate safely in the community represent a significant ongoing health concern for patients with hemiparesis and is associated with accelerated health decline (3, 4). In addition, patients with lower limb spasticity often present secondary complications, such as static or dynamic postural instability, pain, limb deformity, and contractures (1, 5). Patients with lower limb spasticity are also at higher risk of falls and inactivity (6).
Current spasticity management is focused on physical rehabilitation, often facilitated by pharmacological interventions, with the aim of helping patients to achieve their goals. Evidence-based guidelines recommend botulinum toxin type A (BoNT-A) injections as an effective first-line treatment for focal lower limb spasticity (7–9). While well-conducted randomized controlled trials (RCTs) remain the scientific standard in assessing the efficacy of clinical interventions for regulatory compliance, they are often criticized as having limited generalizability as they do not typically consider the diversity of patient presentation, the need to combine other treatment interventions, nor the varied clinical treatment approaches used across the world. RCTs are also not the optimal or best design for addressing some questions, such as how best to apply evidence-based care in practice. Observational studies, conducted in routine treatment settings, preferably across multiple countries, are often the “gold standard” in addressing health-services research of this type and add to evidence-based data. In this context, they inform the current management of lower limb spasticity, allowing for different clinical practices. Such studies also provide important information on clinical presentation, effectiveness, and individualized treatment strategies.
Here, we present full baseline data from the international “AboBoNT-A injections for adult lower limb spasticity in a real-life cohort” (AboLiSh) study, which offers relevant and timely insights into how patients seeking treatment for lower limb spasticity present for treatment in routine clinical practice.
METHODS
This was a prospective, longitudinal (16-month), observational cohort study conducted at 46 specialist study centres across 9 countries (Australia, Brazil, Canada, France, Germany, Italy, Poland, Russia, and USA). Study centres were identified based on their current clinical practice (centres should be experienced with using BoNT-A for lower limb spasticity and should expect to recruit ≥ 3 patients within a reasonable timeframe), prior experience with lower limb studies, and familiarity with using go 10.2340/jrm.v55.4257 al attainment scaling (GAS).
The study was conducted in compliance with the International Society for Pharmacoepidemiology (ISPE) Guidelines for Good Pharmacoepidemiology Practices (GPP). Independent Ethics Committee/Institutional Review Board approval was obtained prior to each centre initiation with written informed consent obtained prior to participant enrolment. The study is registered at Clinicaltrials.gov (NCT04050527).
Population
The study enrolled adult patients (≥ 18 years old) with a documented diagnosis of unilateral lower limb spasticity who provided written informed consent. There was no minimal level of spasticity defined, other than the decision to inject abobotulinumtoxinA (aboBoNT-A) having been made prior to enrolment. The Modified Ashworth Scale (MAS) was, however, recorded in all cases. Participants were ambulatory (defined as being able to take ≥ 5 steps, with or without assistance) and could have previously received BoNT-A (with > 12-week interval since last injection), or be naïve to BoNT-A treatment. Key exclusion criteria included severe limitations in passive range of motion/contractures in the affected limb (defined as MAS (10) score of 4 in at ≥ 1 joint in the lower limb), limb surgery, intrathecal baclofen pump implantation for spasticity within 3 months, or history of a progressive neurological condition or cerebral palsy. Eligible patients were recruited consecutively (i.e. as they presented to the investigator’s clinic).
Assessments at baseline visit
Patients underwent a comprehensive clinical spasticity assessment at the baseline visit. Electronic case report forms were utilized for data collection, including data on medical history, treatment history, the neurological impairment scale (NIS) (11) and the GASleg tool to capture goals of treatment (12). In addition, quality of life was assessed using the EuroQoL 5 Dimensions, 5 Levels (EQ-5D-5L) scale (13).
Each patient had 1 primary treatment goal designated and had the option to identify up to 2 secondary goals that should be amenable to treatment of lower limb spasticity with aboBoNT-A. All goal statements were to be SMART (Specific, Measurable, Attainable, Realistic and Timely). The GASleg tool included categories for pain, involuntary movements, contracture prevention, locomotion, transfers/standing, passive function (caring for the affected limb), and facilitation of therapy/other. In principle, each chosen goal category was to be supported by a standardized outcome assessment that was determined at the time of goal setting. Standardized assessments included the Leg activity measure (LegA) (14), numerical pain rating scale (NPRS) (15), scale of pain intensity (SPIN) (16) and 10-metre walking speed test.
Statistical analyses
All statistical analyses presented in this report are descriptive. Mean and standard deviation (mean ± SD) or median (Q1, Q3) measures are used to summarize continuous variables, and absolute and relative frequencies expressed as a percentage (%) are presented for categorical information. The presence of neurological impairments was analysed as a score of 1–3 (non-normal) or missing. The EQ-5D-5L index values are derived using US standard value set.
RESULTS
Patient characteristics
A total of 430 patients were enrolled (8–137 patients per country). Of these, 46 patients were excluded from these analyses because they did not meet inclusion criteria (n = 18) and/or receive at least 1 BoNT-A injection (n = 14), and/or have a goal assessment (n = 43). Baseline demographics and relevant medical history for the 384 patients included in these analyses are summarized in Table I. Most patients were male (66.4%). Despite their relatively young mean age (53.9 ± 13.8 years), only 19.5% of patients were employed. Most patients had an acquired brain injury due to cerebrovascular disease. In general, enrolled patients had experienced lower limb spasticity for an extended period (median time since event 4.7 years), and a large majority (85.4%) also reported having upper limb spasticity. The median time from the event causing spasticity to the first BoNT injection was over 1 year, but a large majority (75%) of enrolled patients had already received prior BoNT injections.
Table I.
Patient characteristics
| Parameter | Baseline population N = 384 |
|---|---|
| Age, years, mean ± SD | 53.9 ± 13.8 |
| Sex; Male, n (%) | 255 (66.4) |
| Employment status, n (%) Employed (full-time, part-time, student, and sick-leave) Unemployed Retired |
75 (19.5) 162 (42.2) 147 (38.3) |
| Diagnosis of condition leading to upper limb spasticity, n (%) Acquired brain injury (stroke/trauma/other) Spinal cord injury Other |
374 (97.4) 8 (2.1) 2 (0.5) |
| Aetiology, n (%) Vascular (infarct or haemorrhage) Trauma Hypoxic Inflammatory Tumour Degenerative Other |
328 (85.4) 44 (11.5) 1 (0.3) 5 (1.3) 2 (0.5) 2 (0.5) 2 (0.5) |
| Affected leg, n (%) Left Right |
219 (57.0) 165 (43.0) |
| Affected by upper limb spasticity, n (%) Dominant arm Non-dominant arm Both No |
156 (47.6) 170 (51.8) 2 (0.6) 56 (14.6) |
| Time since onset of the event leading to lower limb spasticity, years Mean ± SD Median (IQR) |
6.9 ± 7.9 4.7 (1.7, 8.6) |
| Prior BoNT treatment; n (%) BoNT naïve Previously treated |
96 (24.0) 288 (76.0) |
| Time interval between onset of event and first BoNT injection, years Mean ± SD Median (IQR) |
N = 309 3.6 ± 6.9 1.3 (0.6, 3.3) |
SD: standard deviation; IQR: interquartile range; BoNT: botulinum toxin type A.
In those patients assessed using the NIS, distal motor impairment nearly was universal (99.1%), but other forms of motor impairment also were common (Table II). Almost three-quarters of patients with NIS data available had at least 1 form of sensory impairment, and approximately the same proportion had at least 1 type of communication impairment. The most common forms of cognitive impairment were memory (affecting 67.4% of those assessed) and attention (62.4%).
Table II.
Impairments as identified by the Neurological Impairment Scale (NIS)
| Impairment | Effectiveness population |
|---|---|
| Motor impairment; n/N (%) Impaired muscle power Impaired control of voluntary movement Proximal motor impairment Distal motor impairment Missing |
210/237 (88.6) 154/237 (65.0) 207/239* (86.6) 237/239* (99.1) 147/*145 |
| Sensory impairment; n/N (%) Somatic impairment Impaired proprioception Dysesthesia Missing |
157/219 (71.7) 131/219 (59.8) 72/219 (32.9) 165 |
| Communication impairment; n/N (%) Expressive Receptive Dysarthria Cognitive speech Missing |
161/223 (72.2) 102/223 (45.7) 134/223 (60.1) 99/223 (44.4) 161 |
| Cognitive impairment; n/N (%) Consciousness Memory Attention Executive function Orientation Initiation Missing |
114/218 (52.3) 147/218 (67.4) 136/218 (62.4) 111/218 (50.9) 89/218 (40.8) 89/218 (40.8) 166 |
The presence of neurological impairments was analysed as a score of 1–3 (non-normal) or missing.
Affected activities and quality of life
Overall, 284 patients (66.0%) utilized LegA assessments as part of their comprehensive baseline assessments. Part A of the LegA assesses the patient’s ability to care for the affected leg (i.e. passive function). Most patients reported no or only mild difficulties in performing hygiene or positioning tasks. However, approximately half of the patients (51.1%) had at least moderate difficulties in putting on trousers, and over half (57.4%) had at least moderate difficulty in putting on footwear (Fig. 1a).
Fig. 1.
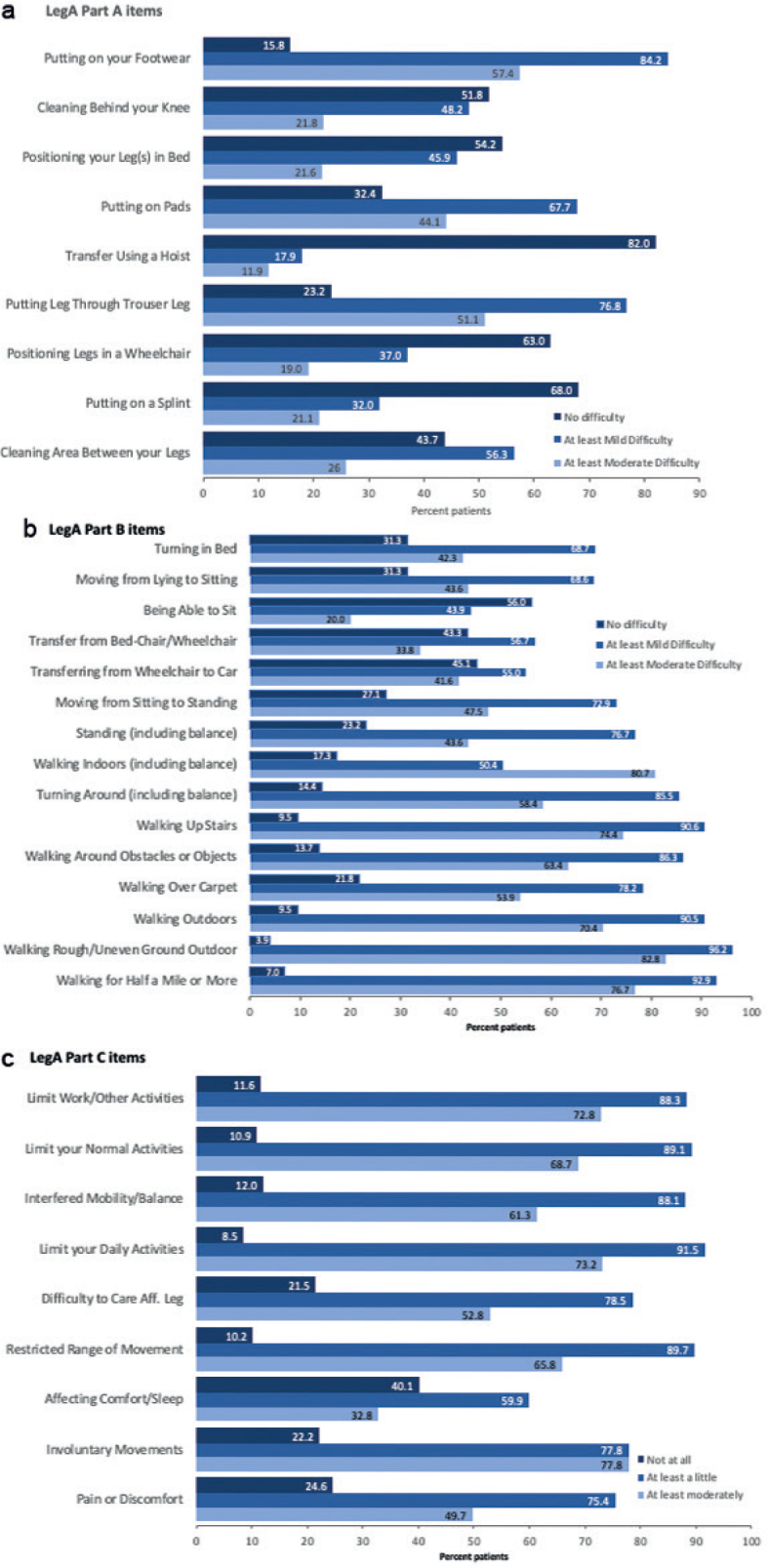
Affected activities as identified by the LegA scale. (a) Ability to care for the affected leg, (b) independently completing activities using the affected leg (c) impact on life, N = 284.
Most patients reported at least mild difficulties with ambulation as assessed by LegA part B, which assesses the patient’s ability to independently complete activities using the affected leg (i.e. active function). Most patients (≥ 70%) had at least moderate difficulty with outdoor ambulation and stairs, while 44–54% of patients had at least moderate difficulty with standing and walking indoors/on carpets (Fig. 1b). Finally, as assessed by part C of the scale, the presence of lower limb spasticity impacted most patients’ normal, daily, and work activities (88–92% reported at least a little impact and 69–73% reported at least moderate impact) (Fig. 1c). Overall, 75.4% of patients reported at least a little pain or discomfort, and 59.9% reported problems with comfort and sleep.
For patients whose walking speeds were recorded (n = 327), the mean ± SD 10m walking speed was 0.55 ± 0.39 m/s (median 0.49 m/s), indicating limited community ambulation. For patients whose pain scores were recorded to support a pain goal (n = 97), the mean ± SD pain score was 5.6 ± 1.9. For patients who completed EQ-5D-5L questionnaires (n = 286), the mean ± SD index score was 0.49 ± 0.26 and the visual analogue score was 59.3 ± 19.4, indicating a significant impact on quality of life.
Goal setting
During the first treatment cycle, 50.8% of patients selected active function primary goals, including locomotion, and transfer/standing (Fig. 2). In line with the LegA assessments, patients chose the impairment/symptoms domain less frequently as primary goals, including pain or discomfort, range of motion, and involuntary movements/spasms.
Fig. 2.

Primary goal setting by domain.
DISCUSSION
Baseline data from this observational study provide insight into the ambulatory patient population presenting at neurorehabilitation clinics for routine treatment of their lower limb spasticity with BoNT-A and start to fill an important gap in our understanding of disease burden. The observations of the current study serve to highlight the complexity of presentation that must be considered when setting treatment goals for lower limb spasticity and emphasize the overlap with other impairments. Three in 5 patients also were treated for upper limb spasticity, and many patients were living with significant motor, sensory, communication, and cognitive impairments alongside their lower limb spasticity. In this ambulatory population, the most common goals of lower limb spasticity treatment were related to locomotion, followed by pain and contracture prevention.
While this study included several aetiologies leading to lower limb spasticity, most patients were stroke survivors. This largely reflects the huge public health burden of stroke, which remains a leading cause of disability in people aged over 50 years (17). Although estimates vary widely (18), it is thought that approximately 2 in 5 patients will develop spasticity within the first year following a stroke (19). In addition, it is important to highlight that the distribution of a aetiologies recruited to this study also reflects the general consensus that BoNT-A is the preferred option for focal and multifocal spasticity (as often seen following traumatic brain injury which was the second most represented population), whereas other modalities, such as intrathecal baclofen may be used more frequently in patients with generalized leg spasticity (e.g. following spinal cord injury) (7, 8, 20–22). Patients with progressive neurological conditions, such as multiple sclerosis, were excluded from the study due to the unpredictable nature of the disease and the fact that they are seen less often in the neurorehabilitation clinics that participated in this study. Adults with cerebral palsy also were excluded due to the impact of spasticity on their normal musculoskeletal growth, contracture formation, and motor development.
Although the generalizability of our NIS findings to the wider population are limited by the large amount of missing data (which was to be expected in the context of an observational study (23)), the frequent observations of sensory, cognitive, behavioural, and emotional deficits still serve to highlight the complexity of patient presentation that can affect recovery and should be considered as part of rehabilitation programme design (24). For example, patients with brain injury often have executive dysfunction that can lead to goal neglect. In their consensus framework for person-centred spasticity management, Turner-Stokes and colleagues (21) stress the importance of the treating team identifying such problems during a comprehensive assessment, to ensure that the goals chosen are appropriate to the patient’s abilities and recommend strategies, such as goal management training for those with significant executive dysfunction (25). While study criteria required the patient to have sufficient capacity to sign written consent, expressive and receptive communication difficulties were also common and must be accounted for during goal-setting negotiations. To aid in this process, a focus group was held in collaboration with patient representatives to develop a goal-setting leaflet that explained the study design and GAS to patients and their caregivers using lay language (26). Patient representatives also provided input on the consent forms.
Scoping reviews have identified a lack of high-quality evidence for the burden of lower limb spasticity (1). Data from the LegA measure provide granularity on the daily burden of lower limb spasticity for ambulatory patients who are considered good candidates for BoNT-A therapy. Lower limb spasticity often involves equinovarus deformities that affect patients’ stance phase and other aspects of walking, including balance and symmetry of stride. Transfers (e.g. from sitting to standing or from wheelchair to car or toilet) are also essentially bipedal activities. Our observations highlight the fact that many ambulatory patients also experience difficulties with passive function, such as dressing and hygiene, albeit to a lesser extent. The presence of leg spasticity significantly impacts all aspects of daily and working life (LegA Part C results) as well as quality of life (EQ-5D-5L results). Therefore, despite the relatively young age of the study cohort, it is to be expected that only 20% of patients were employed. We also emphasize that the study included a relatively wide range of chronicity, with some patients early in their spasticity journey and others much further down the line. Thus, taken together, the LegA and EQ-5D-5L results support the idea that spasticity treatment with BoNT is warranted throughout the continuum of care. In addition, pain and problems with sleeping were common and should be considered in rehabilitation programmes.
These observations support the premise that improved walking is often the highest treatment priority for ambulatory patients with lower limb spasticity (27, 28). An inability to walk is associated with the loss of independence and likelihood of placement in a nursing home (29) and is a strong predictor of adverse health outcomes (30). Primary effectiveness analyses will inform how treatment goals change over time (for new and chronically treated patients) and will be reported separately. Finally, it is pertinent to note that many patients also have upper limb spasticity, and we intend to examine how lower limb spasticity goals (and aboBoNT-A injection patterns) were impacted longitudinally by the desire to manage both upper and lower limb spasticity. Given that the location and severity of spasticity may change over time or with treatment, goals selection and management strategies need to be reassessed periodically.
Strengths of this study lie in its prospective observational design and naturalistic setting. However, while the current study data are limited to those ambulatory patients whose lower limb spasticity is amenable to BoNT-A treatment, it should be emphasized that non-ambulatory patients may also benefit from chemodenervation with BoNT-A.
In summary, these baseline data provide granularity on the daily burden of lower limb spasticity for ambulatory patients who are considered good candidates for BoNT-A therapy and inform on the spectrum of impairments and limitations that treating teams should cover in their initial and follow-up assessments.
ACKNOWLEDGEMENTS
The authors thank all the investigators and patients who participated in this trial. We also thank Anita Chadha-Patel, PhD, of ACP Clinical Communications Ltd (Hertfordshire, UK) for providing medical writing support, which was funded by Ipsen (Paris, France) in accordance with Good Publication Practice guidelines.
This work was supported by Ipsen.
Competing interests
AE, RZ, SA and JJ all received honoraria from Ipsen for undertaking this research. AE reports research funding from Ipsen, Allergan/AbbVie, and Merz, and consultancy for Ipsen, Allergan/AbbVie and Shionogi. SA has a specific interest in outcomes evaluation and has published extensively on the use of GAS in this context, as well as a number of the other standardized measures. All of these tools are freely available, however, and he has no personal financial interest in any of the material mentioned in this article. SA has received honoraria for lecturing, scientific advisory, peer training from Ipsen, Allergan and Merz and research funding from Ipsen. FCG, PM, and SP are employed by Ipsen. JJ has received honoraria for lecturing, scientific advisory, peer training from Ipsen, Allergan, and Merz.
Data sharing
Qualified researchers may request access to patient-level study data that underlie the results reported in this publication. Additional relevant study documents, including the clinical study report, study protocol with any amendments, annotated case report form, statistical analysis plan and dataset specifications may also be made available. Patient level data will be anonymized, and study documents will be redacted to protect the privacy of study participants. Where applicable, data from eligible studies are available 6 months after the primary manuscript describing the results has been accepted for publication. Further details on Ipsen’s sharing criteria, eligible studies and process for sharing are available from https://vivli.org/members/ourmembers/. Any requests should be submitted to www.vivli.org for assessment by an independent scientific review board.
AboLiSh study group
Bozena Adamkiewicz, Arun Aggarwal, Etienne Allart, Claire Aymard, Ziyad Ayyoub, Tobias Bäumer, James Beegan, Francois Boyer, Yuxi Chen, Asare Christian, Regina Chueire, Edward Dabrowski, Claire Delleci, Ugo Dimanico, Ana Paula dos Santos, Steven Edgley, Philippe Gallien, Fatma Gul, Vadim Gusev, Denis Karpov, Nicholas Ketchum, Dina Khasanova, Svetlana Khatkova, Katja Kollewe, Alexey Korenko, Andrey Korolev, Dariusz Koziorowski, Iwona Jastrzebska Kurkowska, Ludovico Lispi, Giacomo Lus, Giorgio Maggioni, Katarzyna Marianska, Vladimir Mikhailov, Cornelia Möbius, Salvatore Napoli, Rachael Nunan, Colleen O’Connell, Atul Patel, Mitchell Paulin, Marcello Romano, Lalith Satkunam, Alexis Schnitzler, Agnieszka Slowik, Nicola Smania, Marsha Smith, Jessica Tate, Martin Todd Taylor, Ip Chi Wang.
REFERENCES
- 1.Martin A, Abogunrin S, Kurth H, Dinet J. Epidemiological, humanistic, and economic burden of illness of lower limb spasticity in adults: a systematic review. Neuropsychiatr Dis Treat 2014; 10: 111–122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Javed M, Ali MH. Epidemiological burden of lower limb spasticity in adults: a systematic review. J Med Res Innov 2020; 4: e000195. [Google Scholar]
- 3.Studenski S, Perera S, Wallace D, Chandler JM, Duncan PW, Rooney E, et al. Physical performance measures in the clinical setting. J Am Geriatr Soc 2003; 51: 314–322. [DOI] [PubMed] [Google Scholar]
- 4.Perera S, Patel KV, Rosano C, Rubin SM, Satterfield S, Harris T, et al. Gait speed predicts incident disability: a pooled analysis. J Gerontol A Biol Sci Med Sci 2016; 71: 63–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Esquenazi, A. Assessment of spasticity and other consequences of the upper motor neuron syndrome affecting the lower limb. In: Spasticity, diagnosis and management. 2nd edition. A. Brashear (editor). New York, NY: Demos Medical Publishing; 2016, Chapter 8, 91–100. [Google Scholar]
- 6.Soyuer F, Oztürk A. The effect of spasticity, sense and walking aids in falls of people after chronic stroke. Disabil Rehabil 2007; 29: 679–687. [DOI] [PubMed] [Google Scholar]
- 7.Royal College of Physicians (UK) Spasticity in adults: management using botulinum toxin. National guidelines; 2018. Available from: https://www.rcplondon.ac.uk/guidelines-policy/spasticity-adults-management-using-botulinum-toxin. [Google Scholar]
- 8.Simpson DM, Hallett M, Ashman EJ. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache. Neurology 2016; 86: 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Esquenazi A, Albanese A, Chancellor MB, Elovic E, Segal KR, Simpson DM, et al. Evidence-based review and assessment of botulinum neurotoxin for the treatment of adult spasticity in the upper motor neuron syndrome. Toxicon 2013; 67: 115–128. [DOI] [PubMed] [Google Scholar]
- 10.Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther 1987; 67: 206–207. [DOI] [PubMed] [Google Scholar]
- 11.Turner-Stokes L, Thu A, Williams H, Casey R, Rose H, Siegert RJ. The Neurological Impairment Scale: reliability and validity as a predictor of functional outcome in neurorehabilitation. Disabil Rehabil 2014; 36: 23–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ashford S, Williams H, Nair A, Orridge S, Turner-Stokes L. Categorisation of goals set using Goal Attainment Scaling for treatment of leg spasticity: a multicentre analysis. Disabil Rehabil 2019; 41: 1925–1930. [DOI] [PubMed] [Google Scholar]
- 13.Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 2011; 20: 1727–1736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ashford SA, Siegert RJ, Williams H, Nair A, Orridge S, Turner-Stokes L. Psychometric evaluation of the leg activity measure (LegA) for outcome measurement in people with brain injury and spasticity. Disabil Rehabil 2021; 43: 976–987. [DOI] [PubMed] [Google Scholar]
- 15.Turner-Stokes L, Disler R, Shaw A, Williams H. Screening for pain in patients with cognitive and communication difficulties: evaluation of the SPIN-screen. Clin Med (Lond) 2008; 8: 393–398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jackson D, Horn S, Kersten P, Turner-Stokes L. Development of a pictorial scale of pain intensity for patients with communication impairments: initial validation in a general population. Clin Med (Lond) 2006; 6: 580–585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1204–1222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Francisco GE, Wissel J, Platz T, Li S. Post-Stroke Spasticity. In: Clinical Pathways in stroke rehabilitation: evidence-based clinical practice recommendations, T. Platz, editor. Cham: Springer International Publishing; 2021, p. 149–173. [PubMed] [Google Scholar]
- 19.Watkins CL, Leathley MJ, Gregson JM, Moore AP, Smith TL, Sharma AK. Prevalence of spasticity post stroke. Clin Rehabil 2002; 16: 515–522. [DOI] [PubMed] [Google Scholar]
- 20.Biering-Soerensen B, Stevenson V, Bensmail D, Grabljevec K, Martínez Moreno M, Pucks-Faes E, et al. European expert consensus on improving patient selection for the management of disabling spasticity with intrathecal baclofen and/or botulinum toxin type A. J Rehabil Med 2022; 54: jrm00241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Turner-Stokes L, Ashford S, Esquenazi A, Wissel J, Ward AB, Francisco G, et al. A comprehensive person-centered approach to adult spastic paresis: a consensus-based framework. Eur J Phys Rehabil Med 2018; 54: 605–617. [DOI] [PubMed] [Google Scholar]
- 22.Williams G, Singer BJ, Ashford S, Hoare B, Hastings-Ison T, Fheodoroff K, et al. A synthesis and appraisal of clinical practice guidelines, consensus statements and Cochrane systematic reviews for the management of focal spasticity in adults and children. Disabil Rehabil 2022; 44: 509–519. [DOI] [PubMed] [Google Scholar]
- 23.Lee KJ, Tilling KM, Cornish RP, Little RJA, Bell ML, Goetghebeur E, et al. Framework for the treatment and reporting of missing data in observational studies: the treatment and reporting of missing data in observational studies framework. J Clin Epidemiol 2021; 134: 79–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Playford ED, Siegert R, Levack W, Freeman J. Areas of consensus and controversy about goal setting in rehabilitation: a conference report. Clin Rehabil 2009; 23: 334–344. [DOI] [PubMed] [Google Scholar]
- 25.Levine B, Schweizer TA, O’Connor C, Turner G, Gillingham S, Stuss DT, et al. Rehabilitation of executive functioning in patients with frontal lobe brain damage with goal management training. Front Hum Neurosci 2011; 5: 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Esquenazi A, Maisonobe P, Sánchez CD, Lysandropoulos A, Ashford S. Impact of patient input on the study execution of an observational study assessing the effectiveness of abobotulinumtoxinA treatment in leg spasticity management in adults (1376). Neurology 2021; 96: 1376. [Google Scholar]
- 27.Gupta AD, Chu WH, Howell S, Chakraborty S, Koblar S, Visvanathan R, et al. A systematic review: efficacy of botulinum toxin in walking and quality of life in post-stroke lower limb spasticity. Syst Rev 2018; 7: 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ward AB, Wissel J, Borg J, Ertzgaard P, Herrmann C, Kulkarni J, et al. Functional goal achievement in post-stroke spasticity patients: the BOTOX® Economic Spasticity Trial (BEST). J Rehabil Med 2014; 46: 504–513. [DOI] [PubMed] [Google Scholar]
- 29.Portelli R, Lowe D, Irwin P, Pearson M, Rudd AG. Institutionalization after stroke. Clin Rehabil 2005; 19: 97–108. [DOI] [PubMed] [Google Scholar]
- 30.Hardy SE, Kang Y, Studenski SA, Degenholtz HB. Ability to walk 1/4 mile predicts subsequent disability, mortality, and health care costs. J Gen Intern Med 2011; 26: 130–135. [DOI] [PMC free article] [PubMed] [Google Scholar]