

 This work is licensed under a
This work is licensed under a Abstract
Endometriosis is a chronic, debilitating disease characterized by the growth of endometrial tissues outside the endometrium. Its prevalence seems to differ across ethnicities, with the disease affecting and presenting with advanced stages in Asians more than any other race. Despite this, data on endometriosis in Asians is limited, and there seems to be a lack of support for endometriosis research in Asia. Hence, this review aims to consolidate the available literature on endometriosis in Asians to identify the gaps in knowledge regarding its occurrence in this population and emphasize the need to address the disease in this part of the world. Certain genetic, dietary, and environmental factors that predominate in Asians compared to other ethnicities may potentially impact endometriosis. Understanding these differences is essential in providing innovative strategies for reducing health disparities in endometriosis incidence and presentation across ethnic groups, thus improving disease management and health outcomes.
Key Words: endometrioma, endocrine-disrupting chemicals, food consumption, ethnic disparities
Introduction
Endometriosis is a debilitating, chronic, inflammatory, progressive, estrogen-dependent disease characterized by the presence of endometrial tissues outside the uterine cavity, presenting clinically as dysmenorrhea, dyspareunia, and dyschezia (1, 2). It has also been associated with an increased risk of asthma, autoimmune disorders, cardiovascular disease, and certain cancers (3). It is histologically characterized by the presence of functioning endometrial glands and stroma in extra-uterine sites, often resulting in a chronic, inflammatory reaction. The long-standing inflammation associated with the disease can cause extensive scarring, resulting in the distortion of the normal pelvic anatomy, which may cause severe life-impacting chronic pelvic pain during periods, sexual intercourse, bowel movements and/or urination, abdominal bloating, nausea, and fatigue, as well as depression, anxiety, and infertility (4). The chronic painful nature of pelvic endometriosis impacts various aspects of a woman’s life, including her school, work, social, and sexual and intimate relationships, leading to an overall decrease in quality of life (5, 6, 7, 8).
The delay in the diagnosis of endometriosis may take about a decade, as a definitive diagnosis is often established through surgery (9). Hence, affected women may live with the disease all throughout their reproductive years (10). Moreover, while several medications are available to manage the symptoms of endometriosis, laparoscopic excision surgery remains an important form of treatment, especially for improving fertility in women with endometriosis (4, 11). The difficulty in detection and the high cost of medications and treatments then become a strong financial burden to a woman with endometriosis. It is estimated that an affected woman would incur about an average of 9579 euros per year for the management of the disease (1). This further increases if the woman would miss work due to severe pain, as women with endometriosis tend to lose an average of 10.8 h of work per week due to the disease (12). Hence, the burden of the disease in women with endometriosis is likely heightened by their socioeconomic status, especially in low-income countries.
In Western populations, the prevalence of endometriosis can reach up to 10% of all reproductive-aged women, but estimates worldwide vary considerably, ranging from 2% to 45%, depending on the diagnostic criteria applied and the population examined (13). For example, the prevalence rates for endometriosis in fertile and infertile women are 0.5–5% and 25–40%, respectively (11). Low estimates may be due to studies that restrict inclusion criteria to patients with surgically confirmed endometriosis, and high prevalence estimates may be due to reports that include symptomatic women who were managed medically without tissue confirmation. While most studies do not report the type and stage of endometriosis, several studies describe a significantly higher overall prevalence of endometriosis in Asians than in other ethnicities (14, 15, 16), with estimates ranging from 6.8% to 15.7% (2, 17). Compared with Caucasian women, Asian women are more likely to be diagnosed with endometriosis (odds ratio (OR) 1.63, 95% CI 1.03–2.58) (14). Filipinos, Indians, Japanese, and Koreans are among the top Asian ethnicities who are more likely to have endometriosis than Caucasian women (17). In the annual census of the Department of Obstetrics and Gynecology of the Philippine General Hospital, endometriosis consistently comprises 15–20% of consults annually and 7.9% of surgeries for benign gynecologic diseases confirmed by histopathology. Despite the high rates of endometriosis in Asian women, data on endometriosis and funding support for endometriosis research in the region are still very limited.
Clinical presentation and severity of endometriosis in Asian women
Women with endometriosis often present with dysmenorrhea, severe chronic pelvic pain, and infertility. Other symptoms include dyspareunia, as well as extragenital symptoms such as dyschezia, dysuria, hematuria, and rectal bleeding (18). While East and Southeast Asian women with endometriosis have lesser pain and better quality of life than Caucasians (19, 20, 21), they are more likely to present with ovarian endometriomas and deep infiltrating lesions, or moderate-to-severe endometriosis at the time of surgery. Indeed, one study noted a 10.9 times higher rate of moderate-to-severe cases of endometriosis with revised American Fertility Society (rAFS) scores of III–IV at the time of surgery (adjusted odds ratio (aOR): 10.87, 95% CI: 4.34–27.21, P < 0.001, n = 368) and a 4.1 times higher presence of ovarian endometriomas on ultrasound (aOR: 4.10, 95% CI: 2.68–6.26, P < 0.001, n = 1521) among East and Southeast Asian women compared with their Caucasian counterparts after adjustments for age, BMI, infertility, previous surgery for endometriosis and ever usage of hormonal medications (22). This is speculated to be due in part to their poor health-seeking practices, as East and Southeast Asian women in their study experience less pain than Caucasians and tend to be diagnosed at an older age, allowing lesions to progress over time and develop into a more severe form of the disease. It is important to point out, however, that there are still many factors to consider when comparing incidences and clinical presentations across ethnic groups, as it is still unclear whether these associations are mere artifacts of diagnostic biases or actual heterogeneity in endometriosis phenotype. Hence, further research is still warranted to confirm ethnic disparities in endometriosis.
Progestins and gonadotropin-releasing hormone (GnRH) analogs are some of the most used medications for suppressing the growth of endometriotic tissues (23). Intake of oral progestins, such as dienogest, inhibits estrogen-induced mitosis and shrinks endometriotic lesions, while continuous administration of GnRH agonists downregulates GnRH receptors and prevents the release of follicle-stimulating hormone and luteinizing hormone from the pituitary gland, resulting in a reduced estradiol production from the ovaries. However, there may be ethnic disparities in terms of response to medication and predisposition to treatment side effects in Asian vs Caucasian women. For example, while dienogest and GnRH analogs have similar efficacy in reducing endometriosis in Japanese and European women, dienogest decreases the total bone mineral density in Japanese but not European women, and GnRH analogs significantly reduced bone mineral density in European more than the Japanese cohorts (24). Whether this difference in medical side effects is also evident in other ethnic groups in Asia remains uncertain.
Genetic polymorphisms in Asians implicated in endometriosis
The high concordance (75–87%) of the disease among identical twins suggests that genetic factors likely contribute to the development of endometriosis (25, 26). There are also reports showing a high incidence of endometriosis with certain family ties. Women with a first-degree relative diagnosed with endometriosis are highly likely to have the disease and highly likely to have severe endometriosis, possibly through a polygenic/multifactorial inheritance (27, 28, 29, 30). For example, in a larger cohort of women from Iceland, the familial clustering of endometriosis is evident even beyond first-degree relatives (31).
The key genes that contribute to the development of endometriosis remain elusive (32), but genetic polymorphisms of some genes have been described in women with endometriosis. One of the most studied genetic polymorphisms is that of estrogen receptors. In a study in Greece, women with endometriosis have a significantly higher frequency of a TC polymorphism recognized by the PvuII restriction enzyme and a fewer median number of microsatellite repeat polymorphisms in the estrogen receptor alpha (ESR1) gene than women without the disease (33). The same association with the PvuII polymorphism is observed in Taiwanese women (34) and Italian women (35). A meta-analysis suggests that this polymorphism in the ESR1 gene may be associated with stage I–III endometriosis (36). However, other studies such as those done in China (37), Japan (38), and Germany (39) did not find an association between the PvuII polymorphism of the ESR1 gene and endometriosis. In contrast, polymorphisms in the estrogen receptor beta (ESR2) but not ESR1 gene are associated with stage IV endometriosis in Japanese women (38). While the association of endometriosis with this polymorphism is found in women from Brazil (40), the link is not found in a group of Korean women (41). Hence, the contribution of these genetic polymorphisms to the pathogenesis of endometriosis remains controversial.
There are also other genetic polymorphisms that have been linked to a higher risk of endometriosis. An Arg399Gln mutation in the X-ray repair cross-complementing group 1 (XRCC1) is associated with endometriosis risk, with the A allele being a preventive factor for the disease in Asians but not among Middle Eastern women (42, 43). In addition, the pro-inflammatory cytokines TNF-α and interleukin-6 (IL-6) also contain polymorphisms that have been linked to endometriosis. The −1031T/C polymorphism in the TNF-α gene reduces the risk of endometriosis, while −238A/G and −174C/G gene polymorphisms in the TNF-α and IL-6, respectively, may increase the risk of endometriosis in Asians (44). However, these genetic polymorphisms were not detected in a more recent genome-wide association study of 60,674 European and East Asian women with endometriosis vs 701,926 controls (45). Instead, the extensive meta-analysis identified 42 genome-wide significant loci associated with endometriosis. Twelve of which were associated with pain sub-phenotypes (P < 0.05), including dysmenorrhea, dyspareunia, bladder pain, acyclical pelvic pain, and gastrointestinal pain. Two of the loci, namely 7p12.3/7p12.3 and VEZT/12q22, showed significant between-study heterogeneity due to ancestry after statistical adjustments (P < 0.05), with East Asian women having higher ORs for endometriosis on these two loci than European women, providing evidence that ethnicity can be a confounding factor for allelic effects on endometriosis. It is still unclear though if this is also true for endometriosis patients across different Asian countries. In addition, it is important to note that while the study described several genetic polymorphisms associated with endometriosis, a direct causal link between these mutations and the pathogenesis of endometriosis has not yet been demonstrated. More studies are then needed to show causal relationships.
Asian diet implicated in endometriosis
Women with endometriosis tend to have a lower BMI than women without the disease (46). This association is even more pronounced in women with deep infiltrating endometriosis (47). Interestingly, women born with low birth weight (<2.5 kg or <5.5 lb) were also likely to be diagnosed with endometriosis (48). Because Asian women have lower BMI than Caucasians, the contribution of BMI to the high rates of endometriosis in Asians has been suggested. But while the reason for the paradoxical association between BMI and endometriosis remains unclear and its implication in the development of endometriosis in Asians is uncertain, it is well recognized that Asians have different dietary patterns than Caucasians. Given the major role of diet in controlling BMI, it is possible that diet may contribute to the disparity in the risk of endometriosis across ethnic groups.
Asians generally consume rice and noodles as the main sources of carbohydrates and tend to eat more nuts, legumes, and fishes than other ethnicities (49). Asians also eat more vegetables and strong spices as part of their diet. Likewise, Asians in the United States have the highest intake of rice and fishes among the various ethnic groups (50, 51). However, consumption of these food products has not been associated with an increased risk of endometriosis. In fact, several studies point to the potential beneficial effects of natural compounds found in these food groups (52, 53). For example, intake of long-chain omega-3 fatty acids, commonly found in fish, seaweeds, vegetable oils, and nuts, is linked to a lower likelihood of being diagnosed with endometriosis (54), given its ability to inhibit endometriotic endometrial cell survival and modulating cytokine expression (55, 56). In vitro and in vivo experiments suggest that exposure to phytoestrogens found in legumes and other plants reduces the risk of endometriosis due to their anti-estrogenic, antiproliferative, antiinflammatory, and proapoptotic effects (57). Moreover, a higher intake of green vegetables but lower consumption of beef, red meat, and ham is associated with a lower incidence of endometriosis (58). This may be in part due to the ability of high fiber to decrease the level of bioavailable estrogen, thus, lowering the risk of endometriosis (59). Hence, there may be other food components or lack thereof that contribute to the development of the disease.
Women with endometriosis have lower consumption of food rich in vitamins A, C, and E, zinc, and copper than women without the disease (60). Women with endometriosis also have lower total dairy food intake and reduced plasma 25(OH)D (vitamin D) levels than women without the disease (61, 62). While the administration of vitamin D has not yet been proven to be effective in treating endometriosis in women (63), it can reduce endometriosis development in mice, in part, by inhibiting endometrial cells to adhere to collagen and reducing macrophage recruitment and inflammatory cytokine secretion (64, 65, 66). Consistent with the higher incidence of endometriosis in Asians, several Asian populations, especially from South Asia, have average serum levels of 25(OH)D below 25 nM (67). Moreover, among the various ethnic groups in the United States, Asians consume the least amount of dairy in their diet (68). Since dairy products, especially milk, are often fortified with vitamin D and become an excellent source of the vitamin, Asians who do not consume much dairy often rely on other sources for the vitamin. Hence, it is possible that the low consumption of these nutrients may be an important factor for endometriosis in Asian women.
Despite the low BMI in Asians, Asians tend to have higher percent body fat than Caucasians at the same BMI (69, 70). This may be attributed in part to the consequence of consuming higher amounts of sodium, saturated fat, and cholesterol by Asians vs Western individuals (71). While there are no reports on whether Asian food with high carbohydrates, sodium, and cholesterol contributes to the progression of endometriosis, eating fatty foods, especially a diet with high trans-unsaturated fat, is associated with an increased risk of endometriosis (54, 72). This is consistent in an animal model of endometriosis wherein feeding mice with a high-fat diet results in more ectopic lesions (73). Women with endometriosis also tend to have higher levels of total cholesterol and mean low-density lipoprotein to total cholesterol ratios than women without the disease (74, 75). These high levels were more pronounced in women with moderate-to-severe endometriosis than in women with minimal-to-mild endometriosis (76, 77). Moreover, while BMI is inversely proportional to the risk of endometriosis, obesity does not protect from endometriosis (78). In fact, obese individuals with endometriosis have higher rAFS scores than endometriosis patients with lower BMI (79). Hence, while Asians have lower BMI than Caucasians, Asians may be consuming more fatty food which increases their risk of endometriosis. More studies are still needed to show the connection between the Asian diet and endometriosis.
Environmental contaminants in Asia implicated in endometriosis
Many environmental contaminants, including heavy metals, are implicated in the pathophysiology of endometriosis. For example, high levels of lead are associated with an increased OR for endometriosis (80, 81), and co-exposure with cadmium further increases hospital admissions due to endometriosis (81). Notably, Asians have higher blood and urine concentrations of these heavy metals than other ethnicities living in the United States (51), with the high levels being more pronounced in Asians born outside the country (82). Hence, heavy metal exposure may be a potential contributor to endometriosis in Asians.
One possible reason for the disparity in heavy metal exposure in Asians vs other ethnicities may be due to their lifestyle differences. Rice, the staple food of most Asians, is a major source of inorganic arsenic (51, 82), while certain spices, particularly turmeric, used by many South Asians may be a potential source of lead exposure (83). Fish, an important protein source of many Asian cuisines, is the most common source of total arsenic exposure in Asians (82). Vegetables, cereal grains, and fruits may also be contaminated with cadmium and may be a potential source of exposure for Asian women (51, 82). Hence, while some of these foods are protective against endometriosis, heavy metal contamination in some of these products may counter their beneficial effects.
Endocrine-disrupting chemicals (EDCs), which are ubiquitous in the environment and found in many consumer products, have also been implicated in endometriosis (84). EDCs, such as bisphenols, phthalates, and per- and polyfluorinated substances (PFAS) can leach out from food packages and canned beverages and enter humans through oral ingestion. They then bind to hormone receptors to activate and inhibit receptor function or interact with membrane proteins to alter hormone synthesis and secretion (85). As endometriosis is an estrogen-dependent disease, certain EDCs that mimic estrogen may exacerbate the development and progression of endometriotic lesions. For example, bisphenol A (BPA) is higher in urine and serum of women with endometriosis (86, 87). Exposure to PFAS, a persistent organic pollutant, is associated with an increased risk of endometriosis in the United States (88, 89) and China (90). A meta-analysis further reveals an overall OR of 1.41 (95% CO: 1.23–1.60) for endometriosis across all exposures to BPA, polychlorinated biphenyls, organochlorine pesticides, and phthalate ester (91). In mice, the association between EDCs and endometriosis is also evident, showing that oral consumption of BPA increases the growth of ectopic endometrial lesions (92), and in utero exposure to BPA yields ovarian lesions reminiscent of endometriosis (93).
Data showing the relationship of EDCs with endometriosis in many Asian countries are still limited, but human exposure to several EDCs is very evident in this part of the world and has been detected since the late 1900s (94). While EDC exposure is a worldwide issue and not restricted to one country or ethnic group, the level of exposure to these contaminants may vary across the globe. For example, the daily intake and urinary concentrations of BPA in Western countries are generally higher than in many Asian countries (95, 96), but BPA exposure appears to be rising in Asia while gradually declining in Western countries (96). In fact, one study showed that while urinary BPA concentrations in Los Angeles residents decreased from 2012 to 2017, BPA levels remained the same in Beijing residents during this period (97). The same study further demonstrated that individuals who traveled from Los Angeles to Beijing during the study period had a 2.91-fold increase in their urinary BPA levels, which fully returned to baseline after going back to Los Angeles. In addition, there is a concerning trend of escalating PFAS levels in women from China (98, 99) and Korea (100, 101) and a persistent PFAS exposure documented in women from Vietnam and Japan (101, 102). In the Philippines, the level of BPA in Filipinos is about twice as much and the level of PFAS can reach up to ten times as high as in women from the United States (103). While the main sources of human exposure remain unclear, some studies suggest that manufacturing sites and food contamination may be important sources of human exposure to EDCs in Asia (104, 105).
The disparity in EDC exposure may be due in part to differences in local production, uses, and regulatory policies related to EDCs. For instance, there has been an increased production of EDC-containing goods in Asian countries like China, coincidental with the rise of EDC exposures in their population (99, 105). Moreover, as Western countries continue to implement effective restrictions on EDCs (106), some EDC-containing products may end up in many Asian countries, especially Southeast Asian countries with poor regulations (99, 107). Hence, it is imperative to have a concerted global effort to manage EDCs worldwide and to monitor the levels of EDCs and other emerging contaminants in each country, especially in vulnerable countries, to create relevant local policies and help lower the risk of diseases, such as endometriosis.
Conclusion
The higher prevalence of endometriosis in Asians yet limited data on this population emphasizes the need for further investigation. Potential factors that predispose Asian women to a more advanced course of the disease should be explored further. Overall, the role of genetics, food consumption, and environment are important in influencing the pathogenesis of endometriosis in Asians (Fig. 1). Several modifiable factors that influence the development of endometriosis should then be explored in this region. Dietary therapy through a combination of vitamins, minerals, salts, lactic ferments, and fish oil may offer protective roles against the disease, as it seems to be as equally effective as hormonal therapy in reducing non-menstrual pelvic pain in endometriosis patients after surgery (108). Strategies to reduce environmental contaminants from important food sources, such as fish, would provide a universal benefit to society. Other emerging contaminants of concern, including microplastics (109), should also be investigated. Determining the impact of genetics, food consumption, and environmental factors will be essential to attaining a more comprehensive understanding of endometriosis and providing new approaches to prevent and treat the disease not only in Asians but also in other ethnic groups.
Figure 1.
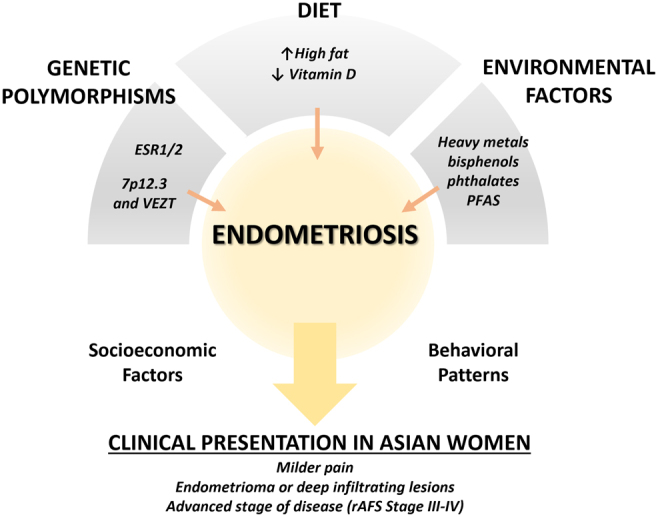
Endometriosis in Asian women. Genetic polymorphisms, dietary patterns, and environmental exposures that are characteristic of the region potentially influence the pathogenesis of endometriosis in Asian women. These elements, coupled with socioeconomic factors and behavioral patterns, result in a more advanced clinical presentation of the disease at the time of diagnosis. PFAS, per- and polyfluorinated substances.
Declaration of interest
The authors declare no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Funding
This paper was funded in part by the University of the Philippines Office of the Vice President for Academic Affairs (OVPAA) Emerging Interdisciplinary Research Program (EIDR-C08-006, MCV).
References
- 1.Simoens S, Dunselman G, Dirksen C, Hummelshoj L, Bokor A, Brandes I, Brodszky V, Canis M, Colombo GL, DeLeire T, et al. The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres. Human Reproduction 2012271292–1299. ( 10.1093/humrep/des073) [DOI] [PubMed] [Google Scholar]
- 2.Yen CF Kim MR & Lee CL. Epidemiologic factors associated with endometriosis in East Asia. Gynecology and Minimally Invasive Therapy 201984–11. ( 10.4103/GMIT.GMIT_83_18) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kvaskoff M Mu F Terry KL Harris HR Poole EM Farland L & Missmer SA. Endometriosis: a high-risk population for major chronic diseases? Human Reproduction Update 201521500–516. ( 10.1093/humupd/dmv013) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Khine YM Taniguchi F & Harada T. Clinical management of endometriosis-associated infertility. Reproductive Medicine and Biology 201615217–225. ( 10.1007/s12522-016-0237-9) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jia SZ Leng JH Shi JH Sun PR & Lang JH. Health-related quality of life in women with endometriosis: a systematic review. Journal of Ovarian Research 2012529. ( 10.1186/1757-2215-5-29) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Marinho MCP Magalhaes TF Fernandes LFC Augusto KL Brilhante AVM & Bezerra LRPS. Quality of life in women with endometriosis: an integrative review. Journal of Women’s Health 201827399–408. ( 10.1089/jwh.2017.6397) [DOI] [PubMed] [Google Scholar]
- 7.Bień A Rzońca E Zarajczyk M Wilkosz K Wdowiak A & Iwanowicz-Palus G. Quality of life in women with endometriosis: a cross-sectional survey. Quality of Life Research 2020292669–2677. ( 10.1007/s11136-020-02515-4) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Soliman AM Coyne KS Zaiser E Castelli-Haley J & Fuldeore MJ. The burden of endometriosis symptoms on health-related quality of life in women in the United States: a cross-sectional study. Journal of Psychosomatic Obstetrics and Gynaecology 201738238–248. ( 10.1080/0167482X.2017.1289512) [DOI] [PubMed] [Google Scholar]
- 9.Pugsley Z & Ballard K. Management of endometriosis in general practice: the pathway to diagnosis. British Journal of General Practice 200757470–476. [PMC free article] [PubMed] [Google Scholar]
- 10.Moradi M Parker M Sneddon A Lopez V & Ellwood D. Impact of endometriosis on women’s lives: a qualitative study. BMC Women’s Health 201414123. ( 10.1186/1472-6874-14-123) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ozkan S Murk W & Arici A. Endometriosis and infertility: epidemiology and evidence-based treatments. Annals of the New York Academy of Sciences 2008112792–100. ( 10.1196/annals.1434.007) [DOI] [PubMed] [Google Scholar]
- 12.Nnoaham KE, Hummelshoj L, Webster P, d’Hooghe T, de Cicco Nardone F, de Cicco Nardone C, Jenkinson C, Kennedy SH, Zondervan KT. & World Endometriosis Research Foundation Global Study of Women ’ s Health consortium. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertility and Sterility 201196366–373.e8. ( 10.1016/j.fertnstert.2011.05.090) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Morassutto C Monasta L Ricci G Barbone F & Ronfani L. Incidence and estimated prevalence of endometriosis and adenomyosis in Northeast Italy: a data linkage study. PLoS One 201611e0154227. ( 10.1371/journal.pone.0154227) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Farland LV & Horne AW. Disparity in endometriosis diagnoses between racial/ethnic groups. BJOG 20191261115–1116. ( 10.1111/1471-0528.15805) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bougie O Yap MI Sikora L Flaxman T & Singh S. Influence of race/ethnicity on prevalence and presentation of endometriosis: a systematic review and meta-analysis. BJOG 20191261104–1115. ( 10.1111/1471-0528.15692) [DOI] [PubMed] [Google Scholar]
- 16.Sangi-Haghpeykar H & Poindexter AN. Epidemiology of endometriosis among parous women. Obstetrics and Gynecology 199585983–992. ( 10.1016/0029-7844(9500074-2) [DOI] [PubMed] [Google Scholar]
- 17.Yamamoto A Johnstone EB Bloom MS Huddleston HG & Fujimoto VY. A higher prevalence of endometriosis among Asian women does not contribute to poorer IVF outcomes. Journal of Assisted Reproduction and Genetics 201734765–774. ( 10.1007/s10815-017-0919-1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dai Y Li X Shi J & Leng J. A review of the risk factors, genetics and treatment of endometriosis in Chinese women: a comparative update. Reproductive Health 20181582. ( 10.1186/s12978-018-0506-7) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chen H Vannuccini S Capezzuoli T Ceccaroni M Mubiao L Shuting H Wu Y Huang H & Petraglia F. Comorbidities and quality of life in women undergoing first surgery for endometriosis: differences between Chinese and Italian population. Reproductive Sciences 2021282359–2366. ( 10.1007/s43032-021-00487-5) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Campbell CM & Edwards RR. Ethnic differences in pain and pain management. Pain Management 20122219–230. ( 10.2217/pmt.12.7) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chapron C Lang JH Leng JH Zhou Y Zhang X Xue M Popov A Romanov V Maisonobe P & Cabri P. Factors and regional differences associated with endometriosis: a multi-country, case-control study. Advances in Therapy 2016331385–1407. ( 10.1007/s12325-016-0366-x) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Williams C Long AJ Noga H Allaire C Bedaiwy MA Lisonkova S & Yong PJ. East and South East Asian ethnicity and moderate-to-severe endometriosis. Journal of Minimally Invasive Gynecology 201926507–515. ( 10.1016/j.jmig.2018.06.009) [DOI] [PubMed] [Google Scholar]
- 23.Rafique S & Decherney AH. Medical management of endometriosis. Clinical Obstetrics and Gynecology 201760485–496. ( 10.1097/GRF.0000000000000292) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Gerlinger C Faustmann T Hassall JJ & Seitz C. Treatment of endometriosis in different ethnic populations: a meta-analysis of two clinical trials. BMC Women’s Health 2012129. ( 10.1186/1472-6874-12-9) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hadfield RM Mardon HJ Barlow DH & Kennedy SH. Endometriosis in monozygotic twins. Fertility and Sterility 199768941–942. ( 10.1016/s0015-0282(9700359-2) [DOI] [PubMed] [Google Scholar]
- 26.Moen MH. Endometriosis in monozygotic twins. Acta Obstetricia et Gynecologica Scandinavica 19947359–62. ( 10.3109/00016349409013396) [DOI] [PubMed] [Google Scholar]
- 27.Simpson JL Elias S Malinak LR & Buttram VC. Heritable aspects of endometriosis. I. Genetic studies. American Journal of Obstetrics and Gynecology 1980137327–331. ( 10.1016/0002-9378(8090917-5) [DOI] [PubMed] [Google Scholar]
- 28.Coxhead D & Thomas EJ. Familial inheritance of endometriosis in a British population. A case control study. Journal of Obstetrics and Gynaecology 19931342–44. ( 10.3109/01443619309151773) [DOI] [Google Scholar]
- 29.Nouri K Ott J Krupitz B Huber JC & Wenzl R. Family incidence of endometriosis in first-, second-, and third-degree relatives: case-control study. Reproductive Biology and Endocrinology 2010885. ( 10.1186/1477-7827-8-85) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Moen MH & Magnus P. The familial risk of endometriosis. Acta Obstetricia et Gynecologica Scandinavica 199372560–564. ( 10.3109/00016349309058164) [DOI] [PubMed] [Google Scholar]
- 31.Stefansson H Geirsson RT Steinthorsdottir V Jonsson H Manolescu A Kong A Ingadottir G Gulcher J & Stefansson K. Genetic factors contribute to the risk of developing endometriosis. Human Reproduction 200217555–559. ( 10.1093/humrep/17.3.555) [DOI] [PubMed] [Google Scholar]
- 32.Vigano P Somigliana E Vignali M Busacca M & Blasio AMD. Genetics of endometriosis: current status and prospects. Frontiers in Bioscience 2007123247–3255. ( 10.2741/2308) [DOI] [PubMed] [Google Scholar]
- 33.Georgiou I Syrrou M Bouba I Dalkalitsis N Paschopoulos M Navrozoglou I & Lolis D. Association of estrogen receptor gene polymorphisms with endometriosis. Fertility and Sterility 199972164–166. ( 10.1016/s0015-0282(9900198-3) [DOI] [PubMed] [Google Scholar]
- 34.Hsieh YY Wang YK Chang CC & Lin CS. Estrogen receptor alpha-351 XbaI*G and -397 PvuII*C-related genotypes and alleles are associated with higher susceptibilities of endometriosis and leiomyoma. Molecular Human Reproduction 200713117–122. ( 10.1093/molehr/gal099) [DOI] [PubMed] [Google Scholar]
- 35.Luisi S Galleri L Marini F Ambrosini G Brandi ML & Petraglia F. Estrogen receptor gene polymorphisms are associated with recurrence of endometriosis. Fertility and Sterility 200685764–766. ( 10.1016/j.fertnstert.2005.08.038) [DOI] [PubMed] [Google Scholar]
- 36.Wang J Hu R Wang J & He Q. PvuII and XbaI in estrogen receptor 1 (ESR1) polymorphisms and susceptibility to endometriosis risk. Clinical Laboratory 202066. ( 10.7754/Clin.Lab.2020.191209) [DOI] [PubMed] [Google Scholar]
- 37.Xie J Wang S He B Pan Y Li Y Zeng Q Jiang H & Chen J. Association of estrogen receptor alpha and interleukin-10 gene polymorphisms with endometriosis in a Chinese population. Fertility and Sterility 20099254–60. ( 10.1016/j.fertnstert.2008.04.069) [DOI] [PubMed] [Google Scholar]
- 38.Wang Z Yoshida S Negoro K Kennedy S Barlow D & Maruo T. Polymorphisms in the estrogen receptor beta gene but not estrogen receptor alpha gene affect the risk of developing endometriosis in a Japanese population. Fertility and Sterility 2004811650–1656. ( 10.1016/j.fertnstert.2004.02.094) [DOI] [PubMed] [Google Scholar]
- 39.Renner SP Strick R Oppelt P Fasching PA Engel S Baumann R Beckmann MW & Strissel PL. Evaluation of clinical parameters and estrogen receptor alpha gene polymorphisms for patients with endometriosis. Reproduction 2006131153–161. ( 10.1530/rep.1.00787) [DOI] [PubMed] [Google Scholar]
- 40.Zulli K Bianco B Mafra FA Teles JS Christofolini DM & Barbosa CP. Polymorphism of the estrogen receptor β gene is related to infertility and infertility-associated endometriosis. Arquivos Brasileiros de Endocrinologia e Metabologia 201054567–571. ( 10.1590/s0004-27302010000600010) [DOI] [PubMed] [Google Scholar]
- 41.Lee GH Kim SH Choi YM Suh CS Kim JG & Moon SY. Estrogen receptor β gene +1730 G/A polymorphism in women with endometriosis. Fertility and Sterility 200788785–788. ( 10.1016/j.fertnstert.2006.12.032) [DOI] [PubMed] [Google Scholar]
- 42.Lv MQ Wang J Yu XQ Hong HH Ren WJ Ge P & Zhou DX. Association between X-ray repair cross-complementing group 1(XRCC1) Arg399Gln polymorphism and endometriosis: a systematic review and meta-analysis. European Journal of Obstetrics, Gynecology, and Reproductive Biology 201721812–20. ( 10.1016/j.ejogrb.2017.09.011) [DOI] [PubMed] [Google Scholar]
- 43.Bau DT Hsieh YY Wan L Wang RF Liao CC Lee CC Lin CC Tsai CH & Tsai FJ. Polymorphism of XRCC1 codon arg 399 Gln is associated with higher susceptibility to endometriosis. Chinese Journal of Physiology 200750326–329. [PubMed] [Google Scholar]
- 44.Li J Chen Y Wei S Wu H Liu C Huang Q Li L & Hu Y. Tumor necrosis factor and interleukin-6 gene polymorphisms and endometriosis risk in Asians: a systematic review and meta-analysis. Annals of Human Genetics 201478104–116. ( 10.1111/ahg.12048) [DOI] [PubMed] [Google Scholar]
- 45.Rahmioglu N, Mortlock S, Ghiasi M, Møller PL, Stefansdottir L, Galarneau G, Turman C, Danning R, Law MH, Sapkota Y, et al. The genetic basis of endometriosis and comorbidity with other pain and inflammatory conditions. Nature Genetics 202355423–436. ( 10.1038/s41588-023-01323-z) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Liu Y & Zhang W. Association between body mass index and endometriosis risk: a meta-analysis. Oncotarget 2017846928–46936. ( 10.18632/oncotarget.14916) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Lafay Pillet MC Schneider A Borghese B Santulli P Souza C Streuli I de Ziegler D & Chapron C. Deep infiltrating endometriosis is associated with markedly lower body mass index: a 476 case-control study. Human Reproduction 201227265–272. ( 10.1093/humrep/der346) [DOI] [PubMed] [Google Scholar]
- 48.Olšarová K & Mishra GD. Early life factors for endometriosis: a systematic review. Human Reproduction Update 202026412–422. ( 10.1093/humupd/dmaa002) [DOI] [PubMed] [Google Scholar]
- 49.Zuñiga YLM Rebello SA Oi PL Zheng H Lee J Tai ES & Van Dam RM. Rice and noodle consumption is associated with insulin resistance and hyperglycaemia in an Asian population. British Journal of Nutrition 20141111118–1128. ( 10.1017/S0007114513003486) [DOI] [PubMed] [Google Scholar]
- 50.Awata H Linder S Mitchell LE & Delclos GL. Association of dietary intake and biomarker levels of arsenic, cadmium, lead, and mercury among Asian populations in the United States: NHANES 2011–2012. Environmental Health Perspectives 2017125314–323. ( 10.1289/EHP28) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Konkel L. The ‘typical’ Asian diet is anything but: differences in dietary exposure to metals among subgroups of U. Environmental Health Perspectives 2017125A58–A59. ( 10.1289/ehp.125-A58) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Saguyod SJU Kelley AS Velarde MC & Simmen RCM. Diet and endometriosis-revisiting the linkages to inflammation. Journal of Endometriosis and Pelvic Pain Disorders 20181051–58. ( 10.1177/2284026518769022) [DOI] [Google Scholar]
- 53.Jurkiewicz-Przondziono J Lemm M Kwiatkowska-Pamuła A Ziółko E & Wójtowicz MK. Influence of diet on the risk of developing endometriosis. Ginekologia Polska 20178896–102. ( 10.5603/GP.a2017.0017) [DOI] [PubMed] [Google Scholar]
- 54.Missmer SA Chavarro JE Malspeis S Bertone-Johnson ER Hornstein MD Spiegelman D Barbieri RL Willett WC & Hankinson SE. A prospective study of dietary fat consumption and endometriosis risk. Human Reproduction 2010251528–1535. ( 10.1093/humrep/deq044) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gazvani MR Smith L Haggarty P Fowler PA & Templeton A. High omega-3:omega-6 fatty acid ratios in culture medium reduce endometrial-cell survival in combined endometrial gland and stromal cell cultures from women with and without endometriosis. Fertility and Sterility 200176717–722. ( 10.1016/s0015-0282(0101991-4) [DOI] [PubMed] [Google Scholar]
- 56.Tomio K, Kawana K, Taguchi A, Isobe Y, Iwamoto R, Yamashita A, Kojima S, Mori M, Nagamatsu T, Arimoto T, et al. Omega-3 polyunsaturated fatty acids suppress the cystic lesion formation of peritoneal endometriosis in transgenic mouse models. PLoS One 20138e73085. ( 10.1371/journal.pone.0073085) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Bartiromo L Schimberni M Villanacci R Ottolina J Dolci C Salmeri N Viganò P & Candiani M. Endometriosis and phytoestrogens: friends or foes? A systematic review. Nutrients 2021132532. ( 10.3390/nu13082532) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Parazzini F Chiaffarino F Surace M Chatenoud L Cipriani S Chiantera V Benzi G & Fedele L. Selected food intake and risk of endometriosis. Human Reproduction 2004191755–1759. ( 10.1093/humrep/deh395) [DOI] [PubMed] [Google Scholar]
- 59.Kaneda N Nagata C Kabuto M & Shimizu H. Fat and fiber intakes in relation to serum estrogen concentration in premenopausal Japanese women. Nutrition and Cancer 199727279–283. ( 10.1080/01635589709514538) [DOI] [PubMed] [Google Scholar]
- 60.Mier-Cabrera J Aburto-Soto T Burrola-Méndez S Jiménez-Zamudio L Tolentino MC Casanueva E & Hernández-Guerrero C. Women with endometriosis improved their peripheral antioxidant markers after the application of a high antioxidant diet. Reproductive Biology and Endocrinology: RB&E 2009754. ( 10.1186/1477-7827-7-54) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Harris HR Chavarro JE Malspeis S Willett WC & Missmer SA. Dairy-food, calcium, magnesium, and vitamin D intake and endometriosis: a prospective cohort study. American Journal of Epidemiology 2013177420–430. ( 10.1093/aje/kws247) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Trabert B Peters U De Roos AJ Scholes D & Holt VL. Diet and risk of endometriosis in a population-based case-control study. British Journal of Nutrition 2011105459–467. ( 10.1017/S0007114510003661) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Kalaitzopoulos DR Samartzis N Daniilidis A Leeners B Makieva S Nirgianakis K Dedes I Metzler JM Imesch P & Lempesis IG. Effects of vitamin D supplementation in endometriosis: a systematic review. Reproductive Biology and Endocrinology 202220176. ( 10.1186/s12958-022-01051-9) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Abbas MA Taha MO Disi AM & Shomaf M. Regression of endometrial implants treated with vitamin D3 in a rat model of endometriosis. European Journal of Pharmacology 201371572–75. ( 10.1016/j.ejphar.2013.06.016) [DOI] [PubMed] [Google Scholar]
- 65.Yildirim B Guler T Akbulut M Oztekin O & Sariiz G. 1-alpha,25-dihydroxyvitamin D3 regresses endometriotic implants in rats by inhibiting neovascularization and altering regulation of matrix metalloproteinase. Postgraduate Medicine 2014126104–110. ( 10.3810/pgm.2014.01.2730) [DOI] [PubMed] [Google Scholar]
- 66.Mariani M Viganò P Gentilini D Camisa B Caporizzo E Di Lucia P Monno A Candiani M Somigliana E & Panina-Bordignon P. The selective vitamin D receptor agonist, elocalcitol, reduces endometriosis development in a mouse model by inhibiting peritoneal inflammation. Human Reproduction 2012272010–2019. ( 10.1093/humrep/des150) [DOI] [PubMed] [Google Scholar]
- 68.Cifelli CJ Kristin Fulgoni VLF & Hess JM. Disparity in dairy servings intake by ethnicity and age in NHANES 2015–2018. Current Developments in Nutrition 20237100010. ( 10.1016/j.cdnut.2022.100010) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Deurenberg-Yap M Schmidt G Staveren van WA & Deurenberg P. The paradox of low body mass index and high body fat percentage among Chinese, Malays and Indians in Singapore. International Journal of Obesity and Related Metabolic Disorders 2000241011–1017. ( 10.1038/sj.ijo.0801353) [DOI] [PubMed] [Google Scholar]
- 70.Deurenberg P Deurenberg-Yap M & Guricci S. Asians are different from Caucasians and from each other in their body mass index/body fat per cent relationship. Obesity Reviews 20023141–146. ( 10.1046/j.1467-789x.2002.00065.x) [DOI] [PubMed] [Google Scholar]
- 71.Henry CJ Kaur B & Quek RYC. Are Asian foods as ‘fattening’ as western-styled fast foods? European Journal of Clinical Nutrition 202074348–350. ( 10.1038/s41430-019-0537-3) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Heilier JF Donnez J Nackers F Rousseau R Verougstraete V Rosenkranz K Donnez O Grandjean F Lison D & Tonglet R. Environmental and host-associated risk factors in endometriosis and deep endometriotic nodules: a matched case-control study. Environmental Research 2007103121–129. ( 10.1016/j.envres.2006.04.004) [DOI] [PubMed] [Google Scholar]
- 73.Heard ME Melnyk SB Simmen FA Yang Y Pabona JMP & Simmen RCM. High-fat diet promotion of endometriosis in an immunocompetent mouse model is associated with altered peripheral and ectopic lesion redox and inflammatory status. Endocrinology 20161572870–2882. ( 10.1210/en.2016-1092) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Melo AS Rosa-e-Silva JC Rosa-e-Silva ACJde S Poli-Neto OB Ferriani RA & Vieira CS. Unfavorable lipid profile in women with endometriosis. Fertility and Sterility 2010932433–2436. ( 10.1016/j.fertnstert.2009.08.043) [DOI] [PubMed] [Google Scholar]
- 75.Mu F Rich-Edwards J Rimm EB Spiegelman D Forman JP & Missmer SA. Association between endometriosis and hypercholesterolemia or hypertension. Hypertension 20177059–65. ( 10.1161/HYPERTENSIONAHA.117.09056) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Verit FF Erel O & Celik N. Serum paraoxonase-1 activity in women with endometriosis and its relationship with the stage of the disease. Human Reproduction 200823100–104. ( 10.1093/humrep/dem340) [DOI] [PubMed] [Google Scholar]
- 77.Turgut A Özler A Görük NY Tunc SY Evliyaoglu O & Gül T. Copper, ceruloplasmin and oxidative stress in patients with advanced-stage endometriosis. European Review for Medical and Pharmacological Sciences 2013171472–1478. [PubMed] [Google Scholar]
- 78.Pantelis A Machairiotis N & Lapatsanis DP. The formidable yet unresolved interplay between endometriosis and obesity. Scientific World Journal 202120216653677. ( 10.1155/2021/6653677) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Holdsworth-Carson SJ Dior UP Colgrave EM Healey M Montgomery GW Rogers PAW & Girling JE. The association of body mass index with endometriosis and disease severity in women with pain. Journal of Endometriosis and Pelvic Pain Disorders 20181079–87. ( 10.1177/2284026518773939) [DOI] [Google Scholar]
- 80.Lai GL Yeh CC Yeh CY Chen RY Fu CL Chen CH & Tzeng CR. Decreased zinc and increased lead blood levels are associated with endometriosis in Asian Women. Reproductive Toxicology 20177477–84. ( 10.1016/j.reprotox.2017.09.001) [DOI] [PubMed] [Google Scholar]
- 81.Kim MG Min YS & Ahn YS. Does exposure of lead and cadmium affect the endometriosis? International Journal of Environmental Research and Public Health 2021189077. ( 10.3390/ijerph18179077) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Awata H Linder S Mitchell LE & Delclos GL. Biomarker levels of toxic metals among Asian populations in the United States: NHANES 2011–2012. Environmental Health Perspectives 2017125306–313. ( 10.1289/EHP27) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Gleason K, Shine JP, Shobnam N, Rokoff LB, Suchanda HS, Ibne Hasan MOS, Mostofa G, Amarasiriwardena C, Quamruzzaman Q, Rahman M, et al. Contaminated turmeric is a potential source of lead exposure for children in rural Bangladesh. Journal of Environmental and Public Health 20142014730636. ( 10.1155/2014/730636) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Interdonato L Siracusa R Fusco R Cuzzocrea S & Di Paola R. Endocrine disruptor compounds in environment: focus on women’s reproductive health and endometriosis. International Journal of Molecular Sciences 2023245682. ( 10.3390/ijms24065682) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Diamanti-Kandarakis E Bourguignon JP Giudice LC Hauser R Prins GS Soto AM Zoeller RT & Gore AC. Endocrine-disrupting chemicals: an Endocrine Society scientific statement. Endocrine Reviews 200930293–342. ( 10.1210/er.2009-0002) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Upson K Sathyanarayana S De Roos AJ Koch HM Scholes D & Holt VL. A population-based case-control study of urinary bisphenol A concentrations and risk of endometriosis. Human Reproduction 2014292457–2464. ( 10.1093/humrep/deu227) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Cobellis L Colacurci N Trabucco E Carpentiero C & Grumetto L. Measurement of bisphenol A and bisphenol B levels in human blood sera from healthy and endometriotic women. Biomedical Chromatography 2009231186–1190. ( 10.1002/bmc.1241) [DOI] [PubMed] [Google Scholar]
- 88.Louis GMB, Peterson CM, Chen Z, Hediger ML, Croughan MS, Sundaram R, Stanford JB, Fujimoto VY, Varner MW, Giudice LC, et al. Perfluorochemicals and endometriosis: the endo study. Epidemiology 201223799–805. ( 10.1097/EDE.0b013e31826cc0cf) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Campbell S Raza M & Pollack AZ. Perfluoroalkyl substances and endometriosis in US women in NHANES 2003–2006. Reproductive Toxicology 201665230–235. ( 10.1016/j.reprotox.2016.08.009) [DOI] [PubMed] [Google Scholar]
- 90.Wang B Zhang R Jin F Lou H Mao Y Zhu W Zhou W Zhang P & Zhang J. Perfluoroalkyl substances and endometriosis-related infertility in Chinese women. Environment International 2017102207–212. ( 10.1016/j.envint.2017.03.003) [DOI] [PubMed] [Google Scholar]
- 91.Wen X Xiong Y Qu X Jin L Zhou C Zhang M & Zhang Y. The risk of endometriosis after exposure to endocrine-disrupting chemicals: a meta-analysis of 30 epidemiology studies. Gynecological Endocrinology 201935645–650. ( 10.1080/09513590.2019.1590546) [DOI] [PubMed] [Google Scholar]
- 92.Jones RL Lang SA Kendziorski JA Greene AD & Burns KA. Use of a mouse model of experimentally induced endometriosis to evaluate and compare the effects of bisphenol A and bisphenol AF exposure. Environmental Health Perspectives 2018126127004. ( 10.1289/EHP3802) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Signorile PG Spugnini EP Citro G Viceconte R Vincenzi B Baldi F & Baldi A. Endocrine disruptors in utero cause ovarian damages linked to endometriosis. Frontiers in Bioscience 201241724–1730. ( 10.2741/493) [DOI] [PubMed] [Google Scholar]
- 94.Matsumoto A Kunugita N Kitagawa K Isse T Oyama T Foureman GL Morita M & Kawamoto T. Bisphenol A levels in human urine. Environmental Health Perspectives 2003111101–104. ( 10.1289/ehp.5512) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Zhang Z Alomirah H Cho HS Li YF Liao C Minh TB Mohd MA Nakata H Ren N & Kannan K. Urinary bisphenol A concentrations and their implications for human exposure in several Asian countries. Environmental Science and Technology 2011457044–7050. ( 10.1021/es200976k) [DOI] [PubMed] [Google Scholar]
- 96.Huang RP Liu ZH Yin H Dang Z Wu PX Zhu NW & Lin Z. Bisphenol A concentrations in human urine, human intakes across six continents, and annual trends of average intakes in adult and child populations worldwide: a thorough literature review. Science of the Total Environment 2018626971–981. ( 10.1016/j.scitotenv.2018.01.144) [DOI] [PubMed] [Google Scholar]
- 97.Lin Y Qiu X Liu J Tseng CH Allard P Araujo JA & Zhu Y. Different temporal trends of exposure to bisphenol A among international travelers between los Angeles and Beijing. Environment International 2020141105758. ( 10.1016/j.envint.2020.105758) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Liu Y Li A Buchanan S & Liu W. Exposure characteristics for congeners, isomers, and enantiomers of perfluoroalkyl substances in mothers and infants. Environment International 2020144106012. ( 10.1016/j.envint.2020.106012) [DOI] [PubMed] [Google Scholar]
- 99.Baluyot JC Reyes EM & Velarde MC. Per- and polyfluoroalkyl substances (PFAS) as contaminants of emerging concern in Asia’s freshwater resources. Environmental Research 2021197111122. ( 10.1016/j.envres.2021.111122) [DOI] [PubMed] [Google Scholar]
- 100.Seo SH Son MH Choi SD Lee DH & Chang YS. Influence of exposure to perfluoroalkyl substances (PFASs) on the Korean general population: 10-year trend and health effects. Environment International 2018113149–161. ( 10.1016/j.envint.2018.01.025) [DOI] [PubMed] [Google Scholar]
- 101.Harada KH, Yang HR, Moon CS, Hung NN, Hitomi T, Inoue K, Niisoe T, Watanabe T, Kamiyama S, Takenaka K, et al. Levels of perfluorooctane sulfonate and perfluorooctanoic acid in female serum samples from Japan in 2008, Korea in 1994–2008 and Vietnam in 2007–2008. Chemosphere 201079314–319. ( 10.1016/j.chemosphere.2010.01.027) [DOI] [PubMed] [Google Scholar]
- 102.Okada E, Kashino I, Matsuura H, Sasaki S, Miyashita C, Yamamoto J, Ikeno T, Ito YM, Matsumura T, Tamakoshi A, et al. Temporal trends of perfluoroalkyl acids in plasma samples of pregnant women in Hokkaido, Japan, 2003–2011. Environment International 20136089–96. ( 10.1016/j.envint.2013.07.013) [DOI] [PubMed] [Google Scholar]
- 103.Velarde MC, Chan AFO, Sajo MEJV, Zakharevich I, Melamed J, Uy GLB, Teves JMY, Corachea AJM, Valparaiso AP, Macalindong SS, et al. Elevated levels of perfluoroalkyl substances in breast cancer patients within the Greater Manila Area. Chemosphere 2022286131545. ( 10.1016/j.chemosphere.2021.131545) [DOI] [PubMed] [Google Scholar]
- 104.Yamaguchi M, Arisawa K, Uemura H, Katsuura-Kamano S, Takami H, Sawachika F, Nakamoto M, Juta T, Toda E, Mori K, et al. Consumption of seafood, serum liver enzymes, and blood levels of PFOS and PFOA in the Japanese population. Journal of Occupational Health 201355184–194. ( 10.1539/joh.12-0264-oa) [DOI] [PubMed] [Google Scholar]
- 105.Huang YQ Wong CKC Zheng JS Bouwman H Barra R Wahlström B Neretin L Wong MH & Bisphenol A. Bisphenol A (BPA) in China: a review of sources, environmental levels, and potential human health impacts. Environment International 20124291–99. ( 10.1016/j.envint.2011.04.010) [DOI] [PubMed] [Google Scholar]
- 106.Kassotis CD Vandenberg LN Demeneix BA Porta M Slama R & Trasande L. Endocrine-disrupting chemicals: economic, regulatory, and policy implications. Lancet. Diabetes and Endocrinology 20208719–730. ( 10.1016/S2213-8587(2030128-5) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Gifford R Siribaddana S Forbes S & Eddleston M. Endocrine-disrupting chemicals and the diabetes epidemic in countries in the WHO South-East Asia region. Lancet. Diabetes and Endocrinology 20153925–927. ( 10.1016/S2213-8587(1500423-4) [DOI] [PubMed] [Google Scholar]
- 108.Sesti F Pietropolli A Capozzolo T Broccoli P Pierangeli S Bollea MR & Piccione E. Hormonal suppression treatment or dietary therapy versus placebo in the control of painful symptoms after conservative surgery for endometriosis stage III–IV. A randomized comparative trial. Fertility and Sterility 2007881541–1547. ( 10.1016/j.fertnstert.2007.01.053) [DOI] [PubMed] [Google Scholar]
- 109.Smith M Love DC Rochman CM & Neff RA. Microplastics in seafood and the implications for human health. Current Environmental Health Reports 20185375–386. ( 10.1007/s40572-018-0206-z) [DOI] [PMC free article] [PubMed] [Google Scholar]