

Abstract
Dissolved ozone is generally used for sanitization, but it has not been used for thoracic cavity sanitization because of its short half-life (< 20 min) and possible toxicity. We developed a novel solution containing ultrafine ozone bubbles (ozone-UFB) with a fivefold longer half-life than non-UFB ozone. Using an in vitro model, Staphylococcus aureus colonies were counted after exposure to ozone-UFB or non-UFB ozone at the same ozone concentration (0.4 mg/L). The colony count was significantly lower in the ozone-UFB group than in the non-UFB ozone group (p = 0.034). The effect of repeated pleural irrigation using ozone-UFB and saline was compared in a rat empyema model of S. aureus infection. The bacterial count in the pleural effusion was decreased by at least fivefold following intrathoracic lavage with ozone-UFB (3 mg/L). To examine the safety of ozone-UFB for intrathoracic use, ozone-UFB with a higher ozone concentration (10 mg/L) was injected into the thoracic cavities of normal rats. The treatment did not result in any specific pleural damage or elevated serum interleukin-6 concentrations. The findings highlighted the efficacy and safety of ozone-UFB for intrathoracic sanitization, but further studies are needed to determine the optimal therapeutic ozone concentration with appropriate safety margins.
Subject terms: Microbiology, Diseases, Materials science
Introduction
Empyema is generally defined as a pathological condition in which pus accumulates in the thoracic cavity. Empyema is associated with pneumonia, chest surgery, trauma, and esophageal perforation. In the USA, 1 × 106 people are hospitalized for pneumonia each year. Of these, 20%–40% have pleural effusion and 5%–10% of those with pleural effusion develop empyema1. In Japan, pleural effusion occurs in 30%–40% of people with bacterial pneumonia and 0.5%–2% of people with pleural effusion develop empyema2.
Local treatment, such as drainage, is useful because antibacterial agents that are administered usually reach low concentrations in the thoracic cavity. However, the effects of intrathoracic irrigation are not well investigated. One reason for this is that normal saline is the only safe liquid available for intrathoracic irrigation. Reports of human clinical studies show that povidone-iodine is effective for empyema and pleural infection3,4. Moreover, pleurodesis using povidone-iodine against air leaks following lung surgery, malignant pleural effusion, and chylothorax has been successful, with the occurrence of only non-serious adverse events such as chest pain5–7. However, in Japan, it is currently not approved for use in body cavities because of concerns about tissue damage and residues8. Additionally, chlorhexidine is only approved as a skin sanitizer in Japan9.
Here, we focused on using ozone dissolved in water to clean the thoracic cavity. Ozone dissolved in water has well-known bactericidal effects, and the effects on various microorganisms have been reported10,11. Ozone dissolved in water has been safely used to sterilize the surfaces of foods such as vegetables and fruits12. However, ozone dissolved in water has a high deactivation rate at 20 °C and has a half-life of 20–30 min, so an ozone solution needs to be prepared immediately before clinical use10,13,14. Ozone dissolved in water is readily deactivated by organic matter10. A technique for preparing a liquid containing bubbles with diameters of 100–200 nm, called ultrafine bubbles (UFBs), has recently been developed. Ozone UFBs can remain dissolved and stable for longer than non-UFB ozone13. Solutions containing ozone-UFBs have been used in the medical field, and there have been several publications about the efficacy and safety of using ozone-UFBs to treat periodontal disease15,16. However, no studies of the efficacy and safety of using ozone-UFBs within the body cavity have been performed. Furthermore, the effects of solutions containing ozone-UFB in the presence of organic matter are unclear.
We assessed the bactericidal effects of a solution containing ozone-UFBs in the presence of organic matter in vitro, the bactericidal effects of a solution containing ozone-UFBs in a rat empyema model, and the effects of a solution containing ozone-UFBs injected into the thoracic cavities of rats on tissue damage.
Materials and methods
Preparing a solution containing ozone-UFBs and determining the ozone concentration
An ozone-UFB solution was prepared using a two-step procedure. First, oxygen was separated from air and ozone was created from the oxygen using a silent electric discharge system in a PZH-12N ozone production device (KOFLOC, Kyoto, Japan). Second, ozone-UFBs were created in a normal saline solution (NSS; Otsuka Pharmaceutical, Tokyo, Japan) by dissolving the ozone by applying power and causing cavitations to form using a UFB creation device (LIVING ENERGIES & Co., Shizuoka, Japan). There were ~ 3 × 108 UFB particles per milliliter of solution, and the UFB diameters were 100–200 nm. The number of UFBs remained sufficient for the tests for > 3 days. The number of UFBs was determined using a NanoSight system (Malvern Panalytical, Malvern, UK). The UFB size distributions are shown in Supplemental Fig. 1. The dissolved ozone concentration in the ozone-UFB NSS decreased more slowly than the dissolved ozone concentration in NSS containing non-UFB ozone at room temperature (22 °C), as shown in Supplemental Fig. 2. Supersaturated ozone rapidly volatilized in the first 10 min after the ozone-UFB NSS was produced, but the ozone concentration then decreased slowly and remained ~ 1 mg/L for > 1 h. In contrast, almost no ozone was detected in the NSS containing non-UFB ozone after another 10 min.
Time to achieve disinfection
Microorganisms
Several microorganisms cause empyema17. Staphylococcus aureus ATCC 29213 (S. aureusATCC) and Pseudomonas aeruginosa ATCC 27853 (P. aeruginosaATCC) used in this study were obtained from the American Type Culture Collection (ATCC). Methicillin-resistant S. aureus (MRSA) was obtained from a clinical sample from Kyoto University Hospital (MRSA-Kyoto). Peptostreptococcus anaerobius GTC 0201 (P. anaerobiusGTC) was obtained from Gifu University Center for Conservation of Microbial Genetic Resourcethrough the National BioResource Project (Pathogenic Bacteria) run by MEXT/AMED (Japan). S. aureusATCC, P. aeruginosaATCC, and MRSA-Kyoto were grown on trypticase soy agar (BD, Franklin Lakes, NJ, USA) at 35 °C for 1 day. P. anaerobiusGTC was grown anaerobically on GAM agar (Nissui Pharmaceutical, Tokyo, Japan) at 36 °C for 3 days.
Sample preparation
A 0.1 mL aliquot of culture medium containing ~ 1 × 107 colony forming units (CFUs)/mL of test bacteria was added to 0.9 mL of ozone-UFB NSS at one of several concentrations (prepared from a solution with an initial ozone concentration of 0.4 mg/L) at 25 °C. The bactericidal effect of the ozone-UFB NSS was compared with the bactericidal effect of 0.5% chlorhexidine gluconate (CHX) (0.5% Hexizac Water W; Yoshida Pharmaceutical, Saitama, Japan).
The mixture was then incubated at 25 °C for 1 min. In tests to compare the bactericidal effects of ozone-UFB NSS and CHX, the bacterial suspensions were incubated for either 1 or 10 min because the duration of the bactericidal effect of each solution was different. CHX did not become deactivated in the mixed solution but ozone-UFB NSS rapidly became deactivated. The bactericidal effects of ozone-UFB NSS on P. anaerobiusGTC and air-UFB NSS were also compared.
Counting bacterial colonies after exposure to a test solution
After incubation, a 0.1 mL aliquot of a mixture was aseptically transferred to a Petri dish and mixed with ~ 20 mL of trypticase soy agar medium, then the mixture was incubated at 35 °C for 1 day (for S. aureusATCC, P. aeruginosaATCC, and MRSA-Kyoto) or mixed with 20 mL of GAM agar medium and incubated at 36 °C for 3 days under anaerobic conditions (for P. anaerobiusGTC). In the tests performed to compare the ozone-UFB and CHX solutions, a 0.1 mL aliquot of a mixture was aseptically transferred to a Petri dish and mixed with 20 mL of tryptic soy agar containing polysorbate 80 and lecithin (Nissui Pharmaceutical) to deactivate the test solution, then the mixture was incubated at 35 °C for 2 days. The colonies that formed were then counted. The minimum bactericidal concentration (MBC) was calculated. The MBCs for S. aureusATCC and P. aeruginosaATCC for non-UFB ozone solutions and ozone-UFB solutions were compared.
Bactericidal effects of ozone-UFB solutions for solutions containing bacteria and albumin
Dissolved ozone is readily deactivated by organic matter, so we assessed the bactericidal effects of ozone-UFB solutions in solutions containing S. aureusATCC and albumin in in vitro tests imitating the intrathoracic environment of empyema.
Bactericidal effects of ozone-UFB solutions at different albumin concentrations
A 50 µL aliquot of culture medium containing ~ 107 CFUs/mL of S. aureusATCC was mixed with NSS containing bovine albumin (Serologicals Corporation, Norcross, GA, USA) at a concentration of 10%, 5%, 1%, or 0.1%. A 0.1 mL aliquot of the mixture was then added to 0.9 mL of ozone-UFB solution (ozone concentration 0.5 mg/L), then the mixture was incubated at 25 °C for 10 min. A 0.1 mL aliquot of the mixture was then aseptically transferred to a Petri dish and mixed with 20 mL of trypticase soy agar medium, then the mixture was incubated at 35 °C for 1 day and the colonies were counted.
Bactericidal effects of ozone-UFB solutions added several times to a solution containing S. aureus and albumin
A 50 µL aliquot of culture medium containing ~ 108 CFUs/mL of S. aureusATCC was mixed with NSS containing bovine albumin at a concentration of 10%. A 0.1 mL aliquot of the mixture was then added to 0.9 mL of ozone-UFB solution (ozone concentration 0.7–1.0 mg/L). A 0.1 mL aliquot of the mixture was then transferred to a tube containing 0.9 mL of ozone-UFB solution, and the same dilution was repeated two more times. For each mixture, a 0.1 mL aliquot was aseptically transferred to a Petri dish and mixed with 20 mL of trypticase soy agar medium, then the mixture was incubated at 35 °C for 1 day. The colonies were then counted.
Rat empyema model
Preparation
A controlled experiment was performed at the Institute of Laboratory Animals, Graduate School of Medicine, Kyoto University, Kyoto, Japan. The study protocol and all procedures were approved by the Kyoto University Ethics Committee (approval number Med Kyo 21306). The animals received humane care in compliance with the Principles of Laboratory Animal Care outlined in Federal Resolution 04/97. This study was carried out in compliance with the ARRIVE guidelines. Male Lewis rats each weighing 280–330 g were randomly selected. The rat supplier was Japan SLC (Hamamatsu, Japan). The effects of intrathoracic lavage using ozone-UFBs were compared with the effects of lavage using NSS using a rat empyema model using S. aureusATCC (one of the most common causes of empyema). The rat empyema model was created by performing intrathoracic injection of 1.0 mL of NSS containing bacteria (~ 108 CFUs of S. aureusATCC). The bacteria solution was injected into the right thoracic cavity through the diaphragm by performing a small laparotomy to avoid postoperative adhesion. All procedures were performed using aseptic techniques.
Treatment and assessment
Two days after S. aureusATCC had been injected, rats with sufficient pleural purulent effusion (≥ 0.5 mL) in which S. aureusATCC was detected after culturing the liquid were defined as having had empyema. Because further survival was not expected in this empyema model, all of the rats were sacrificed by causing them to inhale a lethal dose of isoflurane. The rats were placed in the lateral decubitus position. Skin disinfection was performed with 70% ethanol followed by 10% povidone-iodine. The following procedures were conducted in an aseptic manner using sterilized material. Right thoracotomy with resection of several ribs was performed to allow the entire thoracic space to be inspected. Pleural effusion occurred in both sides of the thoracic space, so the mediastinal pleura was removed to allow all of the pleural effusion to be collected from both sides.
After the effusion had been collected, lavage was performed twice, each time using 3 mL of urokinase (Mochida Pharmaceutical, Tokyo, Japan) diluted with NSS to give 6000 units/mL for 10 min, to remove suspended organic matter. The thoracic cavity was then filled for 2 min with ozone-UFB NSS or NSS. This was repeated 15 times. Ozone-UFB NSS with an ozone concentration of 3–4 mg/L was used for the lavage procedure. Once lavage had been performed 15 times, the thoracic cavity (of each rat in both groups) was filled for 2 min with NSS. The liquids from the first, fifth, 10th, and last NSS lavages were cultured. The pleural effusion and urokinase lavage liquids were each diluted by a factor of 100 and the immersion liquids were each diluted by a factor of 10 with NSS. A 0.1 mL aliquot of a sample was aseptically transferred to a Petri dish and mixed with 20 mL of trypticase soy agar medium, then the mixture was incubated at 35 °C for 1 day. The colonies were then counted. The decreases in the numbers of S. aureusATCC in the first, fifth, 10th, and last NSS immersion liquids were determined and compared with the total bacterial counts for the initial pleural effusion and urokinase lavage liquids.
In vivo toxicity study
Laparotomies were performed in the same manner as the empyema model using male Lewis rats weighing 280–330 g. A 1.0 mL aliquot of NSS containing ozone-UFBs at ozone concentrations of 9–10 mg/L or a 1.0 mL aliquot of NSS (the control) was injected intrathoracically through the diaphragm. The incision was closed without collecting the injected liquid, and the toxicity was evaluated 24 h later.
The rats were sacrificed 24 h after the liquid was injected, and a blood sample was obtained from the inferior vena cava of each rat. The interleukin-6 (IL-6) concentrations in the serum samples were determined and used to indicate inflammation. The IL-6 concentrations were determined by performing enzyme-linked immune sorbent assays using LEGEND MAX™ Rat IL-6 ELISA kits (Biolegend, San Diego, CA, USA). The lower right lung lobe, heart, liver, and right kidney were resected for histopathological examination to allow inflammatory changes to be evaluated. The tissue samples were fixed in 10% formalin and stained with hematoxylin–eosin. Each rat was weighed before the intervention and 24 h later.
Statistical analysis
Each result is presented as the median and interquartile range unless otherwise stated.
The results for pairs of groups were compared by performing Fisher’s exact tests for categorical data and Mann–Whitney U tests for nonparametric variables. Wilcoxon signed rank tests were used to compare the MBCs for S. aureusATCC and P. aeruginosaATCC for non-UFB ozone and ozone-UFB solutions. P < 0.05 was considered to indicate a statistically significant result. Statistical analyses were performed using EZR statistical software (Saitama Medical Center, Jichi Medical University, Saitama, Japan).
Results
Time to achieve disinfection
Enumeration of bacterial colonies following exposure to each solution
The median MBCs for S. aureusATCC and P. aeruginosaATCC for ozone-UFB NSS in 1 min were both 1/8 (range 1/4 to 1/16). The MBCs for S. aureusATCC and P. aeruginosaATCC for non-UFB ozone and ozone-UFB in NSS and the relative MBC distribution tables are shown in Fig. 1. The MBCs for S. aureusATCC and P. aeruginosaATCC were lower for ozone-UFB NSS than non-UFB ozone NSS (p = 0.034 for S. aureusATCC and p = 0.036 for P. aeruginosaATCC).
Figure 1.

Minimum bactericidal concentrations for Staphylococcus aureus (ATCC 29213) and Pseudomonas aeruginosa (ATCC 27853) for a normal saline solution (NSS) containing ozone and ultrafine bubbles of ozone (ozone-UFB) in NSS relative to the minimum bactericidal concentration distribution tables.
The median MBC (as a dilution rate from the solution containing ozone at a concentration of 0.4 mg/L) for MRSA-Kyoto for 1 min was 1/4 (range 1/2 to 1/4), and the median MBC for MRSA-Kyoto for 10 min was 1/24 (range 1/4 to 1/32). The median MBC (as an effective ozone concentration) for P. anaerobiusGTC (1.6 × 106 CFU/mL) for 1 min was 1.1 mg/L without dilution. The air-UFB NSS did not have any bactericidal effect.
The median MBCs for S. aureusATCC for 1 min were 1/4 (range 1/4 to 1/4) for ozone-UFB NSS and < 1 for CHX. The median MBCs for S. aureusATCC for 10 min were 1/8 for ozone-UFB NSS and > 1/16 for CHX.
Bactericidal effects of ozone-UFB solutions at different albumin concentration
The ozone-UFB NSS had a bactericidal effect on S. aureusATCC in a solution containing albumin at a concentration of < 1 g/dL (n = 3) (Fig. 2).
Figure 2.

Bactericidal effects of ultrafine bubbles of ozone in a normal saline solution (NSS) on a solution of Staphylococcus aureus (ATCC 29213) and albumin. The ultrafine bubbles of ozone in NSS had bactericidal effects on bacteria in a solution containing albumin at a concentration of < 1 g/dL (n = 3). BSA bovine serum albumin.
Bactericidal effects of ozone-UFB solutions added several times to a solution containing S. aureus and albumin
Irrigating a S. aureusATCC solution containing 10% albumin three times with ozone-UFB completely sterilized the solution, but irrigating with NSS only diluted the S. aureusATCC (n = 3) (Fig. 3).
Figure 3.

Bactericidal effects of repeated treatments with ultrafine bubbles of ozone (ozone-UFB) in normal saline solution (NSS) containing 10% albumin and Staphylococcus aureus (ATCC 29213). The ozone-UFB NSS had a bactericidal effect after three treatments (n = 3).
Rat empyema model
Solutions of S. aureusATCC (1.6 × 108–3.5 × 108 CFU/mL) were injected into 31 rats. Four rats died before treatment, two rats had no effusion, and eight rats had insufficient pleural effusion (< 0.5 mL). The results for 17 rats were therefore evaluated. These rats were divided into two groups, treatment with NSS (n = 10) and treatment with ozone-UFB NSS (n = 7). The appearances of the thoracic cavities 2 days after injection of S. aureusATCC are shown in Fig. 4. Purulent effusion and fibrin were observed in the right and left thoracic cavities. The volumes of pleural effusion were comparable between the NSS and ozone-UFB groups (1.3 mL [range 1.1–1.6] vs. 1.2 mL [range 1.1–1.5], p = 0.588). Thoracic lavage was therefore performed on both sides of the thoracic cavity through the left thoracic cavity.
Figure 4.
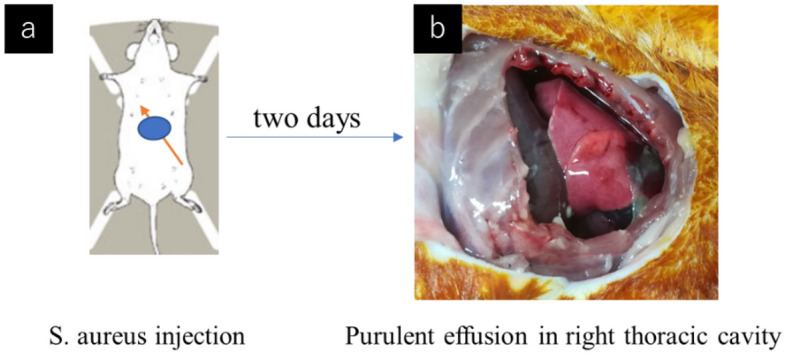
Empyema treatment in a sacrificed rat model. (a) Staphylococcus aureus (ATCC 29213) was injected into the right thoracic cavity via the diaphragm during a laparotomy. (b) Two days later, purulent effusion and fibrin were observed in the right and left parts of the thoracic cavity.
The decrease in the bacteria count after each lavage is shown in Fig. 5. The S. aureusATCC counts for the pleural effusion and the fluid collected after urokinase lavage were decreased by 11.8% (range 4.5%–21.1%) and 4.6% (range 3.2%–13.6%), respectively, (p = 0.417) by the first lavage, 4.2% (range 2.3%–9.0%) and 0.6% (range 0.6%–1.3%), respectively, (p = 0.007) by the fifth lavage, 6.7% (range 3.4%–20.6%) and 0.3% (range 0.2%–0.9%), respectively, (p = 0.019) by the 10th lavage, and 7.5% (range 2.4%–11.7%) and 0.5% (range 0.2%–1.6%), respectively, (p = 0.007) by the last NSS lavage.
Figure 5.

Decreases in the bacteria counts after lavage for empyema with Staphylococcus aureus (ATCC 29213) compared with the bacteria counts in the initial effusion. The decreases were larger in the rats treated with ultrafine bubbles of ozone (ozone-UFB) than in the rats treated with normal saline solution (NSS) after five lavages. IQR interquartile range.
In vivo toxicity study
Of the 16 rats that were used in the toxicity study, three were excluded because of technical damage. The 13 remaining rats were divided into two groups, NSS-treated rats (n = 6) and rats treated with ozone-UFBs (9–10 mg/L) (n = 7). All of these rats survived the evaluation period. The weights 24 h after treatment relative to the weights before treatment were 99.0% (range 98.2%–99.1%) for the NSS group and 96.0% (range 91.1%–98.1%) for the ozone-UFB group (p = 0.138). The serum IL-6 concentrations for all of the rats were < 5.3 pg/mL. The pathological examinations indicated that proliferation of type II alveolar epithelial cells around the airway occurred in one rat in the NSS group, focal proliferation of type II alveolar epithelial cells without infiltration of any inflammatory cells occurred in one rat in the ozone-UFB group, and aspiration pneumonia occurred in one rat in the ozone-UFB group. No inflammatory changes (e.g., pleuritis) or chemical pneumonitis, hepatitis, or nephritis was detected in any rat (Fig. 6).
Figure 6.

Pathological examinations of rat organs 24 h after injection of ultrafine bubbles of ozone (ozone-UFB) in normal saline solution (NSS) or NSS into the right part of the thoracic cavity (hematoxylin eosin stain, 10 × 10). There were no significant inflammatory changes in the right lower lung, heart, liver, or kidney in either the rats treated with ozone-UFBs or NSS.
Discussion
Ozone was discovered by Christian Friedrich Schonbein in 1840, and its use in medicine was reported in the early 1900s. Ozone is a powerful oxidizing substance that has both bactericidal and cytotoxic effects. The bioavailability of ozone is considered useful as long as its capacity is not exceeded18.
Ozone has high sterilization ability and low persistence, and therefore, it is also used for sterilization in wastewater and food materials12,19. Ozone has antimicrobial effects against various bacteria and fungi10,11 as well as viruses such as coronavirus20. In the medical field, ozonated water has been applied in dental treatment15,16. However, because the protective ability against ozone in the respiratory epithelium is low, inhalation of ozone gas at 0.1 ppm or more must be avoided when handling ozone18. A method of dissolving ozone in a liquid rather than in a gaseous state has been investigated, but this strategy is limited because ozone has a short half-life and becomes unstable in liquids10,13,14. We developed an ozone-UFB solution with a long half-life and found that it had an excellent bactericidal effect and was safe in both in vitro and in vivo tests. The effect of ozone (non-UFB) solutions decreases immediately because the half-life is short, and readily deactivated in an organic-matter-rich environment. When using an ozone solution (non-UFB) for sterilization purposes, there has been no choice but to use it at a high concentration of diluted ozone, so far. Therefore, ozone solutions cannot be safely used as antibacterial treatments in the thoracic cavity because of the possibility of the ozone being harmful. Although lavage through a drainage tube using ozonated water at a high ozone concentration (20 mg/L) and urokinase in humans has only been performed in one previous study14, we found that a sufficient bactericidal effect was achieved in a sacrificed rat model by repeated lavage using the ozone-UFB solution (3–4 mg/L) even when the ozone concentration was lower than the ozone concentration in a non-UFB ozone solution used in a previous study14.
In addition to existing treatments such as antibiotic therapy and drainage, intrathoracic lavage can be useful to promote clearance in the thoracic cavity. We observed that performing intrathoracic lavage more than five times did not result in a proportional decrease in the rate of reduction of bacteria. To further facilitate the bactericidal effect of ozone-UFB solution, it would be possible to lower the concentration of organic matter using fibrinolytic therapies such as urokinase. We are also considering other ways to improve the bactericidal effect of ozone-UFB such as intrathoracic lavage using ozone of a higher concentration but within the safety range, and intraoperative or postoperative use with surgical treatment.
We assessed the safety of injecting the ozone-UFB solution into the chest cavities of rats, and ozone at a concentration of 9–10 mg/L was acceptable because of the pathological exam results and the IL-6 concentrations. In a previous in vitro model study in the dental field16 it was found that cell viability in oral tissue exposed to ozone nanobubbles in water slightly decreased over 24 h. In contrast, cell viability in oral tissue exposed to 0.2% CHX halved by 8.4 h, suggesting that CHX can damage human oral tissues and ozone nanobubbles in water would be a safer oral antiseptic.
The evaluation of safety with the application of ozone-UFBs in therapy in humans is essential. There have been several reports regarding ozone nanobubble water therapy for periodontitis15,16, and the low toxicity of ozone nanobubble water in gingival tissue was reported16. In addition, Shichiri-Negoro et al. reported that ozonated water with a diluted ozone concentration of 11 ppm could suppress Candida albicans growth and biofilm formation on polymethyl methacrylate without impairing surface properties21. A systematic review on the effect of ozone therapy in root canal disinfection reported that the antimicrobial effect depended on the concentration of ozone, treatment period, and target microorganisms22. Further evaluation in terms of safe and effective ozone concentrations and conditions is needed until the ozone UFBs we created using our device can be applied in treatment.
There were some limitations to the study. First, empyema is usually treated using antibiotics and drainage with or without lavage. In this study, antibiotics were not used because the aim was to evaluate the bactericidal effects of local treatment using ozone-UFBs. Second, the bactericidal effect of intrathoracic lavage using ozone-UFBs in the empyema rat model were only evaluated for S. aureus, which is the most common cause of empyema. We evaluated the bactericidal effects of ozone-UFBs for several types of bacteria in vitro, but further evaluations for other bacteria (e.g., other kinds of anaerobic bacteria or multi-drug resistant bacteria) will be required. Third, we did not find concentration-dependent bactericidal effects in the rat empyema model. However, it may be necessary to determine the optimal ozone concentration by investigating the relationship between the ozone concentration and bactericidal effect. Finally, the bactericidal effects were evaluated only in sacrificed rats in this study. The extent to which intrathoracic lavage using ozone-UFB solution clinically promotes empyema healing has not been verified in a living animal model. We hope to develop a long-term empyema model combined with systemic treatment and evaluate the additional effect of intrathoracic lavage using ozone-UFB solution.
Conclusions
We found that ozone-UFBs in solution were bactericidal both in vitro and in a rat model. We also found that the effective ozone concentration was safe. This is the first paper to verify the efficacy and safety of ozone-UFBs in the body cavity.
Further studies using a living animal model to determine the therapeutic and adverse effects of ozone-UFB lavage are required before ozone-UFBs in solution can be applied to empyema in humans.
Supplementary Information
Acknowledgements
We thank Gareth Thomas, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Author contributions
All authors had full access to all of the data produced in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. M.T., M.Y., and M.N. contributed to the handling of the microorganisms. All authors contributed substantially to the study design, data analysis and interpretation, and writing the manuscript.
Funding
This work was supported by a grant from the Japan Agency for Medical Research and Development (Grant No. A161).
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Competing interests
MI, YY, and HD have a financial relationship with Yamato Scientific Co., Ltd., which is the company that developed the system used in this study to produce ultrafine ozone bubbles. The other authors have no conflicts of interest or financial ties to disclose. Technical and financial support for the work described in this manuscript was provided by Yamato Scientific Co., Ltd.
Footnotes
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
The online version contains supplementary material available at 10.1038/s41598-023-43787-3.
References
- 1.Shen KR, Bribriesco A, Crabtree T, Denlinger C, Eby J, Eiken P, et al. The American association for thoracic surgery consensus guidelines for the management of empyema. J. Thorac. Cardiovasc. Surg. 2017;153(6):e129–146. doi: 10.1016/j.jtcvs.2017.01.030. [DOI] [PubMed] [Google Scholar]
- 2.Aoki N, Arakawa S, Ouchi K, Ohnishi K, Kaneko A, Kiyota H, et al. The JAID/JSC Guide to Clinical Management of Infectious Diseases. 2019 JAID/JSC Infection Treatment Guide/Guideline Creation Committee. Life Science Publishing Corporation; 2019. [Google Scholar]
- 3.Gharagozloo F, Trachiotis G, Wolfe A, DuBree KJ, Cox JL. Pleural space irrigation and modified Clagett procedure for the treatment of early postpneumonectomy empyema. J. Thorac. Cardiovasc. Surg. 1998;116(6):943–948. doi: 10.1016/S0022-5223(98)70044-3. [DOI] [PubMed] [Google Scholar]
- 4.Hassan M, El-Shaarawy B, Elshazly A, Gadallah M, Sadaka A. Antiseptic pleural irrigation for adult pleural infection. Eur. Respir. J. 2022;60:330. doi: 10.1183/13993003.congress-2022.330. [DOI] [Google Scholar]
- 5.Chaari Z, Hentati A, Ben Ayed A, Abid W, Frikha I. Effectiveness and safety of povidone iodine for prolonged lung air-leak after lung surgery. Asian Cardiovasc. Thorac. Ann. 2022;30(3):314–320. doi: 10.1177/02184923211067637. [DOI] [PubMed] [Google Scholar]
- 6.Muthu V, Dhooria S, Sehgal IS, Prasad KT, Aggarwal AN, Agarwal R. Iodopovidone pleurodesis for malignant pleural effusions: An updated systematic review and meta-analysis. Support Care Cancer. 2021;29(8):4733–4742. doi: 10.1007/s00520-021-06004-3. [DOI] [PubMed] [Google Scholar]
- 7.Nahlovsky J, Matejek T. Chemical pleurodesis with povidone-iodine in congenital chylothorax. Indian J. Pediatr. 2023;90(6):634. doi: 10.1007/s12098-023-04526-8. [DOI] [PubMed] [Google Scholar]
- 8.Package insert for 10% povidone-iodine solution (Meiji Seika Pharma Co., Ltd., 2023). https://s3-ap-northeast-1.amazonaws.com/medleymedicine/prescriptionpdf/780009_2612701Q3466_2_01.pdf. (Japanese Article).
- 9.Package insert for 0.5% chlorhexidine-gluconate solution (Hexizac Water W, Yoshida Pharmaceutical Company, 2023). https://s3-ap-northeast-1.amazonaws.com/medley-medicine/prescriptionpdf/830039_2619702Q1175_1_11.pdf. (Japanese Article).
- 10.Broadwater WT, Hoehn RC, King PH. Sensitivity of three selected bacterial species to ozone. Appl. Microbiol. 1973;26(3):391–393. doi: 10.1128/am.26.3.391-393.1973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Arita M, Nagayoshi M, Fukuizumi T, Okinaga T, Masumi S, Morikawa M, et al. Microbicidal efficacy of ozonated water against Candida albicans adhering to acrylic denture plates. Oral Microbiol. Immunol. 2005;20:206–210. doi: 10.1111/j.1399-302X.2005.00213.x. [DOI] [PubMed] [Google Scholar]
- 12.Botondi R, Barone M, Grasso C. A review into the effectiveness of ozone technology for improving the safety and preserving the quality of fresh-cut fruits and vegetables. Foods. 2021;10:748. doi: 10.3390/foods10040748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Seki M, Ishikawa T, Terada H, Nashimoto M. Microbicidal effects of stored aqueous ozone solution generated by nano-bubble technology. In Vivo. 2017;31:579–583. doi: 10.21873/invivo.11097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Li B, Liu C, Li Y, Yang HF, Du Y, Zhang C, et al. Computed tomography-guided catheter drainage with urokinase and ozone in management of empyema. World J. Radiol. 2017;9(4):212–216. doi: 10.4329/wjr.v9.i4.212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hayakumo S, Arakawa S, Mano Y, Izumi Y. Clinical and microbiological effects of ozone nano-bubble water irrigation as an adjunct to mechanical subgingival debridement in periodontitis patients in a randomized controlled trial. Clin. Oral Invest. 2013;17:379–388. doi: 10.1007/s00784-012-0711-7. [DOI] [PubMed] [Google Scholar]
- 16.Hayakumo S, Arakawa S, Takahashi M, Kondo K, Mano Y, Izumi Y. Effects of ozone nano-bubble water on periodontopathic bacteria and oral cells -in vitro studies. Sci. Technol. Adv. Mater. 2014;15:055003. doi: 10.1088/1468-6996/15/5/055003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Iliopoulou M, Skouras V, Psaroudaki Z, Makarona M, Vogiatzakis E, Tsorlini E, et al. Bacteriology, antibiotic resistance and risk stratification of patients with culture-positive, community-acquired pleural infection. J. Thorac. Dis. 2021;13(2):521–532. doi: 10.21037/jtd-20-2786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bocci V. OZONE: A New Medical Drug. 2. Springer; 2011. [Google Scholar]
- 19.Azuma T, Usui M, Hayashi T. Inactivation of antibiotic-resistant bacteria in wastewater by ozone-based advanced water treatment processes. Antibiotics. 2022;11(2):210. doi: 10.3390/antibiotics11020210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Franke G, Knobling B, Brill FH, Becker B, Klupp EM, Campos CB, et al. An automated room disinfection system using ozone is highly active against surrogates for SARS-CoV-2. J. Hosp. Infect. 2021;112:108–113. doi: 10.1016/j.jhin.2021.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Shichiri-Negoro Y, Tsutsumi-Arai C, Arai Y, Satomura K, Arakawa S, Wakabayashi N. Ozone ultrafine bubble water inhibits the early formation of Candida albicans biofilms. PLoS ONE. 2021;16(12):e0261180. doi: 10.1371/journal.pone.0261180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Silva EJNL, Prado MC, Soares DN, Hecksher F, Martins JNR, Fidalgo TKS. The effect of ozone therapy in root canal disinfection: A systematic review. Int. Endod. J. 2020;53:317–332. doi: 10.1111/iej.13229. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.