

Abstract
Objective
To examine the incidence and characteristics of eyes with oblique astigmatism stratified by meridian, age, sex, and eye side (left to right).
Methods
One thousand eyes of 1000 patients with oblique corneal astigmatism underwent videokeratographic examination and was classified into 4 meridian categories: (1) 31°–45°, (2) 46°–59°, (3) 121°–135°, and (4) 136°–149°. Amounts of regular and irregular astigmatism, and the vertical/horizontal (Rx) and oblique astigmatism components (Ry) decomposed using vector analysis were compared among the 4 categories and age groups, and between sexes and eye sides.
Results
Incidences of the 4 meridian categories were similar and did not differ significantly among age groups or between sexes. The incidence was significantly greater in eyes in meridian categories 1 and 2 in the left eye and categories 3 and 4 in the right eye, and significantly greater in men in their 40 s and 50 s and in women in their 70 s and 80 s (P < 0.0001). The mean regular astigmatism, asymmetry and higher-order irregularity components, and Rx and absolute Ry significantly increased with age (P ≤ 0.0372). The mean regular and irregular astigmatism, and absolute Rx and Ry did not differ significantly among the 4 categories, or between sexes or left and right eyes.
Conclusions
The incidence of oblique astigmatism was significantly greater in the temporal side meridians, and the incidence in women increased with age. The degree of oblique astigmatism increased with age, with an increase in irregular astigmatism.
Subject terms: Corneal diseases, Refractive errors
Introduction
Oblique astigmatism may have specific features. The prevalence of eyes with oblique astigmatism is reported to be 10–20% as a whole [1–3]. Oblique astigmatism is divided into 2 astigmatism meridian ranges, 31°–59° and 121°–149°. With the centres of the meridian ranges at 45° and 135°, these 2 oblique astigmatism meridians can be further divided according to their clockwise and counterclockwise torque by Cartesian coordinate analysis [4], corresponding to against-the-rule (ATR) and with-the-rule (WTR) astigmatism, respectively. Thus, oblique astigmatism can be classified into 4 astigmatism meridian categories.
Corneal and refractive astigmatism shift from WTR astigmatism to ATR astigmatism with advancing age [5–8]. This ATR shift progresses earlier in men than in women [9], and occurs to a similar extent in ATR, WTR, and oblique astigmatism [10]. Thus, the prevalence of both WTR and ATR astigmatism changes with age. Many studies, however, report that the prevalence of eyes with oblique astigmatism does not change markedly with age [5–11]. Because no studies to date have focused on eyes with oblique astigmatism, the prevalence and characteristics of oblique astigmatism are unclear.
The present study evaluated the prevalence and characteristics of eyes with oblique astigmatism stratified by age decade, sex, and eye side (left to right). Because oblique astigmatism is classified into the 4 meridian categories mentioned above, we analysed the differences in the characteristics of eyes with oblique astigmatism among the 4 meridian categories.
Subjects and methods
Study design
This cross-sectional cohort study was conducted at the Hayashi Eye Hospital, Fukuoka, Japan between July 28, 2021 and March 14, 2022. The Institutional Review Board of the Hayashi Eye Hospital approved the study protocol on July 27, 2021 (ID number 2021-K-5). The study protocol adhered to the tenets of the Declaration of Helsinki, and informed consent was obtained from each patient before enrolment into the study.
Participants
All patients who underwent an examination using an autokeratometer (TONOREF II and III, NIDEK) at the outpatient clinic of the Hayashi Eye Hospital during the study period were screened. Patients with oblique astigmatism of the anterior cornea then underwent videokeratographic examination using the Topographic Modelling System, version 7 M (TMS-7; Tomey). Corneal astigmatism of the total cornea was evaluated using the TMS-7, and eyes that were confirmed to have oblique astigmatism and met the inclusion criteria were consecutively enrolled in the study. Exclusion criteria were: (1) pseudophakic or aphakic eyes, (2) corneal pathology, (3) severe dry eye, (4) blepharitis or Meibomian gland dysfunction, (5) pseudoexfoliation syndrome, (6) diabetes, (7) history of ocular surgery or inflammation, (8) difficulty undergoing examination, and (9) patient refusal. Eyes with a greater magnitude of oblique astigmatism were enrolled, and right eyes were included when the magnitude was the same between the left and right eyes. Patient enrolment was continued until 1000 eyes of 1000 patients were enrolled.
Meridian categories of oblique astigmatism
Oblique astigmatism is basically divided into 2 meridian ranges: 31°–59° and 121°–149°. With the range centres at 45° and 135°, these 2 meridians were further divided according to their clockwise and counterclockwise torque by Cartesian coordinate analysis [4], corresponding to ATR and WTR astigmatism, respectively. We thus classified oblique astigmatism into 4 astigmatism meridian categories: (1) 31°–45° (category 1), (2) 46°–59° (category 2), (3) 121°–135° (category 3), and (4) 136°–149° (category 4), as shown in Fig. 1.
Fig. 1. Schema of the 4 meridian categories of oblique astigmatism and comparison of the incidence of eyes with oblique astigmatism among the 4 meridian categories.
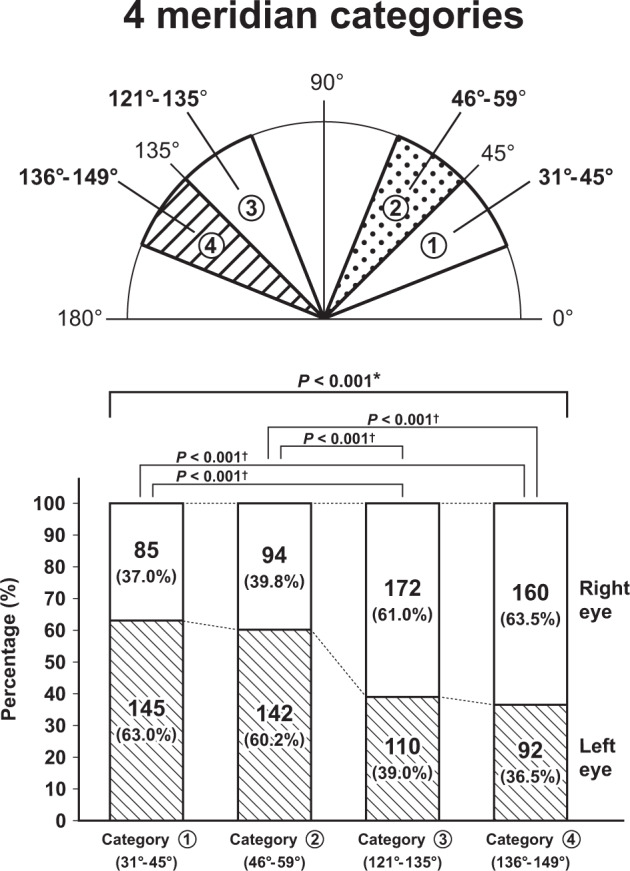
Oblique astigmatism is classified into 4 meridian categories: (1) 31°–45° (category 1); (2) 46°–59° (category 2); (3) 121°–135° (category 3); and (4) 136°–149° (category 4). The incidence of eyes with oblique astigmatism was significantly greater in meridian categories 1 and 2 in left eyes and in meridian categories 3 and 4 in right eyes. *Statistically significant difference among the 4 meridian categories, †Statistically significant difference between each meridian category pair.
Outcome measures
All patients underwent videokeratographic examination of the total cornea using the TMS, version 7 M. Details of the TMS are described elsewhere [12–14]. Briefly, the TMS includes a rotating Scheimpflug camera system and Placido ring topographer. This device obtains data by merging Placido-ring topography with the Scheimpflug camera system. This system initially obtains 4 measurements using Placido-ring topography (ring topo mode), with each measurement lasting less than 0.5 s. The examiner then activates the Scheimpflug system (slit mode), and Scheimpflug acquisition is performed.
Videokeratographs were obtained 3 times for each patient, and the highest-quality image was selected for each patient and stored in the TMS-7 computer. The data were used to determine regular and irregular astigmatism of the total cornea. The magnitude and meridian of regular astigmatism were calculated using the simulated keratometric values at the steeper and flatter meridians. The magnitude and meridian of regular astigmatism were decomposed to the vertical/horizontal astigmatism component (Rx) and oblique astigmatism component (Ry) using polar value analysis as described by Naeser [4]. A positive oblique astigmatism component indicates counterclockwise torque, and a negative component indicates clockwise torque. A positive vertical/horizontal astigmatism component indicates ATR astigmatism, and a negative component indicates WTR astigmatism.
The data were also used to determine irregular astigmatic components by Fourier analysis, as previously described [15]. Briefly, the dioptric powers on a mire ring i, Fi(É-) were transformed into trigonometric components as follows:
where a0 was the spherical equivalent power of the ring, c1 the asymmetry component, c2 the regular astigmatic component, and c3…n the third and higher-order irregularity components. Spherical equivalent power (a0) and the second order regular astigmatism component (c2) can be corrected by a spherocylindrical lens, while the first-order asymmetry component (c1) and third and higher-order irregularity (c3…n) components are regarded as irregular corneal astigmatism. These calculations were performed on rings 1 through 9 or 1 through 20, which correspond to the central corneal optical zone of 3.0 mm or 6.0 mm, respectively. The mean value of the 1 to 9 or 1 to 20 rings was determined and considered the representative value of each component. Because data from 3.0-mm optical zone are more closely related to the keratometric readings and visual function than data from the 6.0-mm optical zone, only the irregular astigmatism components of the central 3.0-mm optical zone are described in the present study.
The magnitude and meridian of oblique astigmatism of the total cornea were also plotted on double-angle plots utilizing the ASCRS Astigmatism Double Angle Plot Tool (available at http://ascrs.org) [16]. The centroid values of the astigmatism were revealed using this tool. All examinations were performed by experienced ophthalmic technicians who were unaware of the purpose of the study.
Statistical analysis
The normality of the data distribution was assessed by inspecting histograms. Because portions of the data regarding the magnitude of regular and irregular astigmatism, and the Rx and Ry values did not follow a normal distribution, non-parametric tests were used to evaluate the significance of differences. The mean magnitude of regular and irregular astigmatism, the Rx and Ry values, and other continuous variables were compared among the 4 meridian categories and among age groups using the Kruskal-Wallis test, as well as between sexes and left and right eyes using the Mann–Whitney U test. When a significant difference in these parameters was detected among the 4 meridian categories or age groups, each group pair was compared using the Mann–Whitney U test with Bonferroni’s correction. The incidences were compared among the 4 meridian categories, and age decades, and between the sexes, and left and right eyes were compared among the 4 categories and age and between sexes and left to right eyes using the chi-square test or Fisher’s exact test. Any difference with a P value less than 0.05 was considered statistically significant.
Results
All data of the 1000 eyes of 1000 patients were collected. Mean patient age (± standard deviation) was 67.5 ± 10.4 years (range 32–89 years), and there were 443 men and 557 women. The incidence of eyes with oblique astigmatism differed significantly among age groups (P < 0.001; Supplementary Table 1); the incidence was significantly smaller in eyes of patients in their 40 s or 50 s than in those in their 60 s or 70 s (P < 0.001).
Comparison of oblique astigmatism parameters among the 4 meridian categories
The incidence of the 4 meridian categories differed significantly between the left and right eyes (P < 0.001; Fig. 1). Comparison of each pair of meridian categories revealed a significantly greater incidence in categories 1 and 2 in left eyes and in categories 3 and 4 in right eyes (P < 0.001). The incidence of the 4 meridian categories did not differ significantly among age groups or between sexes (Supplementary Table 2). The mean magnitude of regular astigmatism, asymmetry and higher-order irregularity components, and the absolute Rx and Ry values did not differ significantly among the 4 meridian categories (Supplementary Table 3).
Comparison of oblique astigmatism parameters among age groups and double-angle plots stratified by age
The mean magnitude of regular astigmatism significantly increased with age (P = 0.005; Fig. 2), with a significant difference between patients in their 40 s and those in their 80 s (P = 0.001). The mean asymmetry components significantly increased with age (P < 0.001; Fig. 2), with significant differences between patients in their 40 s, 50 s, or 60 s and those in their 70 s or 80 s (P ≤ 0.004), and between patients in their 70 s and those in their 80 s (P = 0.003). The higher-order irregularity components significantly increased with age (P < 0.001; Fig. 2), with significant differences between patients in their 40 s, 50 s, or 60 s and those in their 70 s or 80 s (P ≤ 0.001), and between patients in their 70 s and those in their 80 s (P = 0.002).
Fig. 2. Comparison of magnitude of regular astigmatism, and asymmetry and higher-order irregularity astigmatism components among the 5 age groups.

Both the mean amounts of asymmetry and higher-order irregularity components significantly increased with advancing age. *Statistically significant difference among age groups, †Statistically significant difference between age group pairs.
The mean Rx significantly increased from a negative to a positive value with age (P = 0.037), with no significant difference between each age group pair (Fig. 3A), indicating a slight amount of ATR shift. The mean absolute Ry increased with age (P = 0.003; Fig. 3B), with significant differences between patients in their 40 s or 50 s and those in their 80 s (P ≤ 0.004), indicating an increase in oblique astigmatism. Double-angle plots also illustrated that oblique astigmatism increased with age, with a slight amount of change toward ATR astigmatism (Fig. 4).
Fig. 3. Comparison of vertical/horizontal astigmatism components (Rx; A) and absolute value of oblique astigmatism components (Absolute Ry; B) among the 5 age groups.

A The mean Rx significantly increased from a negative to a positive value with age, with no significant difference between each age group pair. *Statistically significant difference/ among the 5 age groups. B The mean absolute Ry value increased with age, with significant differences between patients in their 40 s or 50 s and those in their 80 s. *Statistically significant difference among the 5 age groups, †Statistically significant difference between age group pairs.
Fig. 4. Double-angle plot analysis of the change in the oblique and vertical/horizontal astigmatism components with age.

The oblique astigmatism component markedly increased with advancing age, with only a slight change toward ATR astigmatism. The 95% confidence ellipse of the data is indicated by the dotted line.
Comparison of oblique astigmatism parameters between sexes
The ratio of men to women with oblique astigmatism significantly changed with age (P < 0.001; Fig. 5); the incidence was greater in men in their 40 s and 50 s and in women in their 70 s and 80 s. Comparisons between each age group pairs revealed that the ratio of men to women differed significantly different between 40 s and 60 s, 70 s, or 80 s (P ≤ 0.002), and between 50 s or 60 s and 70 s (P ≤ 0.002). The magnitude of regular astigmatism, asymmetry and higher-order irregularity components, and absolute Rx and Ry values did not differ significantly between the sexes (Supplementary Table 4).
Fig. 5. Comparison of the ratio of eyes with oblique astigmatism between men and women among the 5 age groups.
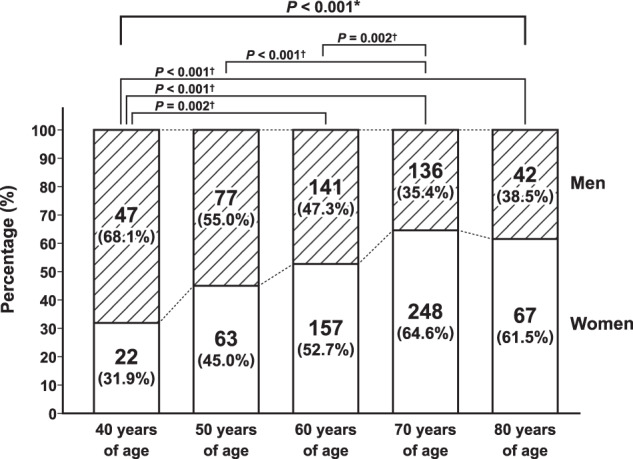
The ratio of eyes with oblique astigmatism between men and women significantly changed with age; the incidence was greater in men in their 40 s and 50 s and in women in their 70 s and 80 s. *Statistically significant difference among the 5 age groups, †Statistically significant difference between age group pairs.
Comparison of oblique astigmatism parameters between left and right eyes
The mean magnitude of regular astigmatism, asymmetry and higher-order irregularity components, and the absolute Rx and Ry values did not differ significantly between left and right eyes (Supplementary Table 4).
Discussion
The findings of the present study revealed that the incidence of oblique astigmatism was significantly greater in the temporal side meridian among the 4 meridian categories, but did not differ among age groups or between men and women. Additionally, the ratio of female eyes significantly increased according to advancing age with the transition occurring when patients were in their 60 s, although the incidence was similar between the left and right eyes. These findings suggest that eyes with oblique astigmatism have specific features that differ substantially from eyes with ATR and WTR astigmatism.
Regarding irregular astigmatism, the amounts of both asymmetry and higher-order irregularity components significantly increased with age in eyes having oblique astigmatism in the present study. Some studies revealed that the degree of irregular astigmatism increases with age [17–20], and that irregular astigmatism is greatest in eyes with oblique astigmatism, followed by ATR and WTR astigmatism [20]. Thus, the findings of the present study of only eyes with oblique astigmatism agree well with those of previous studies in eyes with ATR, WTR, and oblique astigmatism.
Previous studies demonstrated that regular corneal astigmatism continue to change from WTR to ATR astigmatism with advancing age [5–11], although controversy remains [21]. This ATR shift progresses faster in men than in women, and the transition from WTR to ATR astigmatism occurs in men in their 50 s and in women in their 60 s [9]. Accordingly, the magnitude of regular astigmatism decreases in men up to their 50 s and in women up to their 60 s, and thereafter increases again with age, indicating a biphasic change [9, 11]. Thus, regular astigmatism changes in a vertical direction with age, but the change in the oblique direction is generally not remarkable in eyes with ATR, WTR, and oblique astigmatism [8–11]. Whether or not a corneal shape changes in the oblique direction occurs in eyes with oblique astigmatism was an interesting question, but it was not examined to date. The present study revealed that the degree of the oblique astigmatism significantly increases with advancing age in eyes with oblique astigmatism.
A limitation of the present study is that it was conducted as a cross-sectional study. The longitudinal changes in oblique astigmatism in each patient were not examined. Further studies are necessary to examine the long-term changes in oblique astigmatism in each patient having oblique astigmatism.
In conclusion, the incidence of oblique astigmatism was significantly greater in the temporal side meridian among the 4 meridian categories. In addition, the ratio of female eyes significantly increased according to advancing age with the transition occurring when patients were in their 60 s. Furthermore, the amount of oblique astigmatism significantly increased with advancing age. These findings are clinically relevant when performing correction of preexisting oblique astigmatism at the time of cataract surgery, including the use of a toric intraocular lens or limbal relaxing incisions [22–25]. For example, on the basis of the findings of the present study, preexisting oblique astigmatism should be fully corrected or overcorrected because the oblique astigmatism may increase again after surgery. In the present study, however, longitudinal changes of oblique astigmatism in each patient were not examined. Further studies are necessary to examine the long-term changes in oblique astigmatism in individual patients.
Summary
What was known before
Studies reported that the prevalence of eyes with oblique astigmatism is 10% to 20% as a whole, but whether or not the prevalence of eyes with oblique astigmatism changes with age remains unclear.
Since no studies to date have focused on eyes with oblique astigmatism, the characteristics of oblique astigmatism are unclear.
What this paper adds
The present study revealed that the incidence of oblique astigmatism was significantly greater in the temporal side meridians among the 4 meridian ranges of oblique astigmatism, and the incidence of the 4 meridian ranges did not differ significantly among age groups or between sexes.
The ratio of female eyes significantly increased according to advancing age in eyes with oblique astigmatism, with the transition from male eyes to female eyes occurring when patients were in their 60 s.
The amount of oblique astigmatism increased with advancing age, with an against-the-rule shift of regular astigmatism and an increase in irregular astigmatism.
Supplementary information
Acknowledgements
We thank Koji Yonemoto, PhD (Ryukyu University) for statistical assistance.
Author contributions
KH; study conception, study design, data analysis/interpretation of data, and writing and revising of the manuscript. KU; data acquisition and final approval. SM; data acquisition and final approval. AH; study conception, study design, data analysis/interpretation of data, and final approval.
Data availability
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
The online version contains supplementary material available at 10.1038/s41433-023-02470-7.
References
- 1.Chen W, Zuo C, Chen C, Su J, Luo L, Congdon N, et al. Prevalence of corneal astigmatism before cataract surgery in Chinese patients. J Cataract Refract Surg. 2013;39:188–92. doi: 10.1016/j.jcrs.2012.08.060. [DOI] [PubMed] [Google Scholar]
- 2.Day AC, Dhariwal M, Keith MS, Ender F, Perez Vives C, Miglio C, et al. Distribution of preoperative and postoperative astigmatism in a large population of patients undergoing cataract surgery in the UK. Br J Ophthalmol. 2019;103:993–1000. doi: 10.1136/bjophthalmol-2018-312025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hoffmann PC, Hütz WW. Analysis of biometry and prevalence data for corneal astigmatism in 23,239 eyes. J Cataract Refract Surg. 2010;36:1479–85. doi: 10.1016/j.jcrs.2010.02.025. [DOI] [PubMed] [Google Scholar]
- 4.Næser K. Assessment and statistics of surgically induced astigmatism. Acta Ophthalmol. 2008;86(Suppl 1):5–28. doi: 10.1111/j.1755-3768.2008.01234.x. [DOI] [PubMed] [Google Scholar]
- 5.Ho JD, Liou SW, Tsai RJ, Tsai CY. Effects of aging on anterior and posterior corneal astigmatism. Cornea. 2010;29:632–7. doi: 10.1097/ICO.0b013e3181c2965f. [DOI] [PubMed] [Google Scholar]
- 6.Ueno Y, Hiraoka T, Beheregaray S, Miyazaki M, Ito M, Oshika T. Age-related changes in anterior, posterior, and total corneal astigmatism. J Refract Surg. 2014;30:192–7. doi: 10.3928/1081597X-20140218-01. [DOI] [PubMed] [Google Scholar]
- 7.Shao X, Zhou KJ, Pan AP, Cheng XY, Cai HX, Huang JH, et al. Age-related changes in corneal astigmatism. J Refract Surg. 2017;33:696–703. doi: 10.3928/1081597X-20170718-04. [DOI] [PubMed] [Google Scholar]
- 8.Hayashi K, Yoshida M, Manabe SI, Yoshimura K. Long-term changes in manifest refraction subsequent to cataract surgery. J Cataract Refract Surg. 2022;48:322–7. doi: 10.1097/j.jcrs.0000000000000767. [DOI] [PubMed] [Google Scholar]
- 9.Hayashi K, Sato T, Sasaki H, Hirata A, Yoshimura K. Sex-related differences in corneal astigmatism and shape with age. J Cataract Refract Surg. 2018;44:1130–9. doi: 10.1016/j.jcrs.2018.06.020. [DOI] [PubMed] [Google Scholar]
- 10.Hayashi K, Sasaki H, Hirata A, Yoshimura K Comparison of long-term astigmatic changes following cataract surgery among types of corneal astigmatism. Br J Ophthalmol. 2022; 10.1136/bjophthalmol-2021-321026. [DOI] [PubMed]
- 11.Hayashi K, Ogawa S, Manabe S, Hirata A. Influence of patient age at surgery on long-term corneal astigmatic change subsequent to cataract surgery. Am J Ophthalmol. 2015;160:171–8.e1. doi: 10.1016/j.ajo.2015.04.015. [DOI] [PubMed] [Google Scholar]
- 12.Guilbert E, Saad A, Grise-Dulac A, Gatinel D. Corneal thickness, curvature, and elevation readings in normal corneas: combined Placido-Scheimpflug system versus combined Placido-scanning-slit system. J Cataract Refract Surg. 2015;38:1198–206. doi: 10.1016/j.jcrs.2012.01.033. [DOI] [PubMed] [Google Scholar]
- 13.Chan TCY, Biswas S, Yu M, Jhanji V. Comparison of corneal measurements in keratoconus using swept-source optical coherence tomography and combined Placido-Scheimpflug imaging. Acta Ophthalmol. 2017;95:e486–e494. doi: 10.1111/aos.13298. [DOI] [PubMed] [Google Scholar]
- 14.Huang J, Savini G, Wang C, Lu W, Gao R, Li Y, et al. Precision of corneal thickness measurements obtained using the scheimpflug-placido imaging and agreement with ultrasound pachymetry. J Ophthalmol. 2015;2015:328798. doi: 10.1155/2015/328798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Oshika T, Tomidokoro A, Maruo K, Tokunaga T, Miyata N. Quantitative evaluation of irregular astigmatism by fourier series harmonic analysis of videokeratography data. Invest Ophthalmol Vis Sci. 1998;39:705–9. [PubMed] [Google Scholar]
- 16.Abulafia A, Koch DD, Holladay JT, Wang L, Hill W. Pursuing perfection in intraocular lens calculations: IV. Rethinking astigmatism analysis for intraocular lens-based surgery: Suggested terminology, analysis, and standards for outcome reports. J Cataract Refract Surg. 2018;44:1169–74. doi: 10.1016/j.jcrs.2018.07.027. [DOI] [PubMed] [Google Scholar]
- 17.Fujikado T, Kuroda T, Ninomiya S, Maeda N, Tano Y, Oshika T, et al. Age-related changes in ocular and corneal aberrations. Am J Ophthalmol. 2004;138:143–6. doi: 10.1016/j.ajo.2004.01.051. [DOI] [PubMed] [Google Scholar]
- 18.Amano S, Amano Y, Yamagami S, Miyai T, Miyata K, Samejima T, et al. Age-related changes in corneal and ocular higher-order wavefront aberrations. Am J Ophthalmol. 2004;137:988–92. doi: 10.1016/j.ajo.2004.01.005. [DOI] [PubMed] [Google Scholar]
- 19.Hayashi K, Kawahara S, Manabe S, Hirata A. Changes in irregular corneal astigmatism with age in eyes with and without cataract surgery. Invest Ophthalmol Vis Sci. 2015;56:7988–98. doi: 10.1167/iovs.15-18058. [DOI] [PubMed] [Google Scholar]
- 20.Ueno Y, Nomura R, Hiraoka T, Kinoshita K, Ohara M, Oshika T. Comparison of corneal irregular astigmatism by the type of corneal regular astigmatism. Sci Rep. 2021;11:15769. doi: 10.1038/s41598-021-95358-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Næser K, Savini G, Bregnhoj F. Age-related changes in with-the-rule and oblique astigmatism. Acta Ophthalmol. 2018;96:600–6. doi: 10.1111/aos.13683. [DOI] [PubMed] [Google Scholar]
- 22.Holland E, Lane S, Horn JD, Ernest P, Arleo R, Miller KM. The AcrySof Toric intraocular lens in subjects with cataracts and corneal astigmatism: a randomized, subject-masked, parallel-group, 1-year study. Ophthalmology. 2010;117:2104–11. doi: 10.1016/j.ophtha.2010.07.033. [DOI] [PubMed] [Google Scholar]
- 23.Nanavaty MA, Bedi KK, Ali S, Holmes M, Rajak S. Toric intraocular lenses versus peripheral corneal relaxing incisions for astigmatism between 0.75 and 2.5 diopters during cataract surgery. Am J Ophthalmol. 2017;180:165–77. doi: 10.1016/j.ajo.2017.06.007. [DOI] [PubMed] [Google Scholar]
- 24.Kaufmann C, Peter J, Ooi K, Phipps S, Cooper P, Goggin M, et al. Limbal relaxing incisions versus on-axis incisions to reduce corneal astigmatism at the time of cataract surgery. J Cataract Refract Surg. 2005;31:2261–5. doi: 10.1016/j.jcrs.2005.08.046. [DOI] [PubMed] [Google Scholar]
- 25.Mendicute J, Irigoyen C, Ruiz M, Illarramendi I, Ferrer-Blasco T, Montés-Micó R. Toric intraocular lens versus opposite clear corneal incisions to correct astigmatism in eyes having cataract surgery. J Cataract Refract Surg. 2009;35:451–8. doi: 10.1016/j.jcrs.2008.11.043. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.