
Figure 3. HFpEF patients with mutations in CH driver genes exhibit worse long-term prognosis.
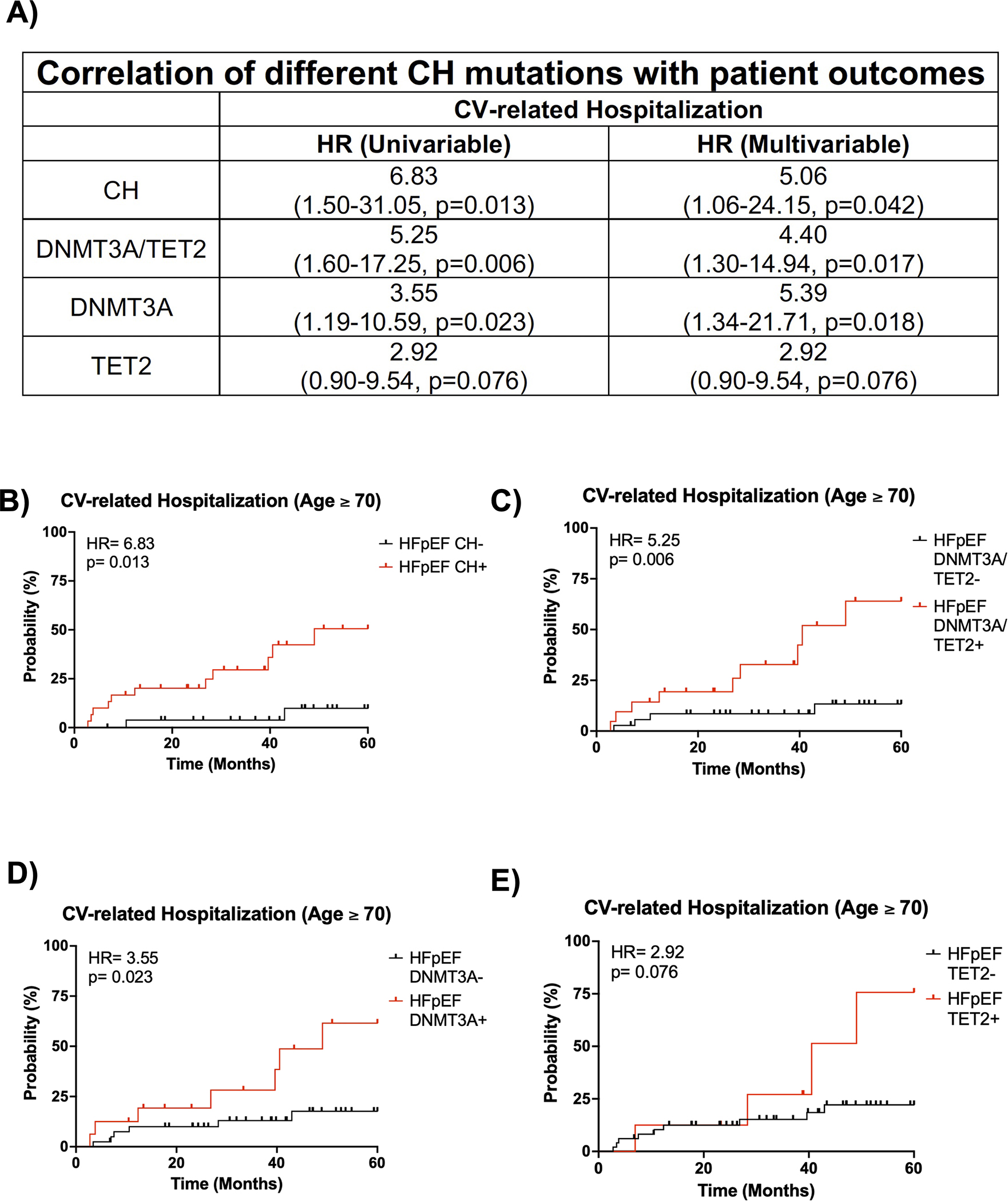
A. Univariate and multivariate analysis of CV-related hospitalization for HFpEF patients and an age ≥ 70 years old based on CH status, DNMT3A/TET2-driven CH status, DNMT3A-driven CH status, and TET2-driven CH status. Statistical significance and hazards ratio were determined by Cox proportional hazards model. B. 5-year CV-related hospitalization based on clonal hematopoiesis status for HFpEF patients with an age ≥ 70 years old. Statistical significance and hazards ratio were determined by Cox proportional hazards model (n= 27 HFpEF CH− patients and 30 HFpEF CH+ patients). C. 5-year CV-related hospitalization for HFpEF patients with and without DNMT3A/TET2-driven CH and an age ≥ 70 years old. Statistical significance and hazards ratio were determined by Cox proportional hazards model (n= 36 HFpEF DNMT3A/TET2- patients and 21 HFpEF DNMT3A/TET2+ patients). D. 5-year CV-related hospitalization for HFpEF patients with and without DNMT3A-driven CH and an age ≥ 70 years old. Statistical significance and hazards ratio were determined by Cox proportional hazards model (n= 41 HFpEF DNMT3A- patients and 16 HFpEF DNMT3A+ patients). E. 5-year CV-related hospitalization for HFpEF patients with and without TET2-driven CH and an age ≥ 70 years old. Statistical significance and hazards ratio were determined by Cox proportional hazards model (n= 49 HFpEF TET2- patients and 8 HFpEF TET2+ patients).