

ABSTRACT
Idiopathic pulmonary fibrosis (IPF) is a devastating chronic lung disease without a clear recognizable cause. IPF has been at the forefront of new diagnostic algorithms and treatment developments that led to a shift in patients’ care in the past decade, indeed influencing the management of fibrotic interstitial lung diseases other than IPF itself. Clinical presentation, pathophysiology, and diagnostic criteria are briefly addressed in this review article. Additionally, evidence regarding the use of antifibrotics beyond the settings of clinical trials, impact of comorbidities, and therapeutic approaches other than pharmacological treatments are discussed in further detail.
Keywords: Idiopathic pulmonary fibrosis/diagnosis, Idiopathic pulmonary fibrosis/physiopathology, Idiopathic pulmonary fibrosis/therapy, Idiopathic pulmonary fibrosis/rehabilitation
RESUMO
A fibrose pulmonar idiopática (FPI) é uma doença pulmonar crônica devastadora sem uma causa claramente reconhecida, que está na vanguarda de novos algoritmos de diagnóstico e do desenvolvimento de tratamentos que levaram a uma mudança no cuidado desses pacientes na última década, influenciando de fato o manejo de doenças pulmonares intersticiais fibróticas além da própria FPI. A apresentação clínica, a fisiopatologia e os critérios diagnósticos são brevemente abordados neste artigo de revisão. Além disso, as evidências sobre o uso de antifibróticos além dos cenários de ensaios clínicos, o impacto de comorbidades e abordagens terapêuticas, além dos tratamentos farmacológicos são discutidos detalhadamente.
Descritores: Fibrose pulmonar idiopática/diagnóstico, Fibrose pulmonar idiopática/fisiopatologia, Fibrose pulmonar idiopática//terapia, Fibrose pulmonar idiopática/reabilitação
INTRODUCTION
Interstitial lung diseases (ILDs) comprise a heterogeneous group of non-neoplastic diseases with various degrees of inflammation and/or fibrosis. Some have known causes; others have a set of recognizable risk factors and pathogenic pathways but not a single identifiable etiology, the so-called idiopathic interstitial pneumonias-among which figures idiopathic pulmonary fibrosis (IPF), its most prominent member, and regarded as the prototypical fibrotic disease. 1 , 2
IPF is a chronic progressive fibrotic disease restricted to the lungs that affects adult patients, mainly elderly individuals (> 50 years of age, but usually > 65 years), in a 2-3:1 male to female ratio, most commonly with a history of concurrent or previous smoking. 1 , 3
Epidemiological data are scarce, especially in low/medium-income countries, but its incidence and prevalence appear to be rising, reaching annual rates of more than 8 and 28 cases per 100,000 population per year, respectively. 4 In Brazil, Baddini-Martinez and Pereira 5 estimated, based on data from the USA, an annual incidence of 3.5-5.1/100,000 population and a prevalence of 7.1-9.4 per 100,000 population. Mortality is high, and most patients have an estimated survival of 3-5 years without treatment, which is comparable to cancers with poor prognosis. 1
Over the last decade, important advances regarding IPF physiopathology, consensus diagnostic criteria, and development of target medications have led to a new era of understanding and treatment of ILDs. 6
PATHOPHYSIOLOGY
Although not entirely known, IPF is believed to derive from recurrent epithelial injury in the lungs that are susceptible to cellular aging and aberrant repair, resulting in intense deposition of collagen through activated myofibroblasts. 7
Short telomeres, determinants of cellular senescence, associated with oxidative stress, mitochondrial dysfunction, and protein dysregulation, are also part of fibrosis initiation and progression, which occurs through several mediators, such as TGF-β, IL-1β, IL-6, and IL-8. 8 Up to one third of patients with IPF, either in its familial or sporadic presentation, have recognizable genes associated with pulmonary fibrosis (including, but not only, IPF), most notably those related to telomere length mutations (such as TERC, TERT, PARN, and RTEL1) and a single nucleotide polymorphism (rs35705950) of the promoter region of the MUC5B gene. 1 , 2
Although specific causes for IPF development are unknown, some risk factors have been widely recognized for their association with the disease, especially age, male sex, and smoking. Other risk factors include gastroesophageal reflux disease (GERD), obstructive sleep apnea, air pollution, occupational exposures throughout life (not leading to a specific pneumoconiosis), chronic viral infections (such as hepatitis C and Epstein-Bar virus), and a family history of ILD. 1
CLINICAL PRESENTATION AND NATURAL COURSE
IPF must be considered in adult patients (generally > 50 years of age) with an insidious course of progressive dyspnea on exertion, dry cough, and “Velcro” crackles on inspiration, sometimes with digital clubbing. Signs of pulmonary hypertension, such as limb edema and jugular vein distention, may be apparent in later stages of disease.
Constitutional symptoms should prompt the investigation of alternative etiologies or associated comorbidities, such as cancer. Additionally, a thorough history of exposures (both environmental and occupational), drugs, and infections as a cause of ILD must be ruled out before a diagnosis of IPF can be confidently made. 1 , 2
Pulmonary function tests should be performed in all patients, both for diagnostic purposes and especially for prognosis and follow-up. A restrictive pattern with low FVC, TLC, and DLCO is the rule. FVC is the most well studied parameter for mortality prediction, and a relative decline ≥ 10%, along with an absolute decline > 5%, is used as a surrogate for disease progression 9 and has been employed as an endpoint for randomized controlled trials.
Prognostication in IPF can be challenging since the disease course, although usually progressive, might be unpredictable. Classically, patients present with a slow and sustained loss of FVC over time, but some might present with an accelerated decline in functional capacity or even periods with stabilization. 2 , 6
The most widely validated prognostic tool was developed in 2012 by Ley et al, 10 the GAP index, which comprises Gender, Age, and Physiology (FVC and DLco). Field tests, such as the six-minute walk test (6MWT) and cardiopulmonary exercise testing, might also be employed as surrogates for severity. Hypoxemia on exertion occurs early in the disease course and can also reflect disease progression.
Rarely might patients also present with an acute exacerbation of IPF (AE-IPF), defined as a recent worsening of dyspnea (usually within the last 30 days or less), with new bilateral superposing consolidation or ground-glass opacities on chest X-ray or HRCT to previous fibrotic areas, excluding pulmonary edema as a sole cause. AE-IPF is either triggered by a known cause (such as infection, aspiration, or drugs) or idiopathic (untriggered). This condition is associated with poor prognosis and is responsible for most IPF-related hospitalizations. 11
DIAGNOSIS
Multidisciplinary meetings remain the gold standard for ILD diagnosis, including IPF. Ideally, patients should be evaluated at an ILD specialized center involving at least a group of clinicians, radiologists, and pathologists. Accurate early diagnosis remains suboptimal, delaying therapy initiation and frequently submitting patients to incorrect treatments for other conditions (such as COPD or congestive heart failure) or with the use of proven harmful drugs (such as corticosteroids and immunosuppressants).
A diagnosis of IPF requires definite exclusion of ILDs with known causes, such as drug-related ILD, fibrotic hypersensitivity pneumonitis (fHP), or connective tissue disease-associated ILD. Once other causes of ILD have been ruled out and/or IPF is suspected based on clinical suspicion, a combination of clinical and radiological features should be employed to determine the probability of IPF. Eventually, if lung biopsy is performed (usually after a first multidisciplinary meeting discussion), histopathological features are added to the probability estimation.
A morphological pattern of usual interstitial pneumonia (UIP), either a radiological or a histopathological one, is required to establish an IPF diagnosis. On the other hand, a UIP pattern has been associated with other conditions, such as asbestosis, fHP, and rheumatoid arthritis. Therefore, the exclusion of alternative diagnoses remains central, even with a typical UIP pattern on HRCT. 2
HRCT has become central to the diagnosis of IPF (Table 1). The radiological appearance of UIP (or typical UIP) has a strong correlation with histological UIP, precluding the need for invasive procedures (Figure 1). In other patterns, such as probable or indeterminate UIP, BAL or lung biopsy could be performed in order to improve diagnostic accuracy, although a probable UIP pattern in an appropriate clinical context of high suspicion of IPF is accepted by most thoracic/respiratory societies as diagnostic for IPF without biopsy (Figure 2), and some patients might be unsuitable for invasive procedures. 3 , 6
Table 1. HRCT findings in idiopathic pulmonary fibrosis (in relation to the usual interstitial pneumonia pattern).
| UIP | Probable UIP | Indeterminate for UIP | Alternative Diagnosis | |
|---|---|---|---|---|
| Distribution | • Subpleural inferior predominance • Might be asymmetrical and heterogeneous |
• Subpleural inferior predominance • Frequently heterogeneous |
• Diffuse (without subpleural predominance) | • Peribronchovascular • Perilymphatic • Upper or mid lung • Subpleural sparing |
| HRCT characteristics | • Honeycombing (with or without traction bronchiectasis) • Irregular thickening of interlobular septa • Superimposed to reticular pattern • Mild GGO • Might have pulmonary ossification |
• Reticular pattern with traction bronchiectasis • May have mild GGO (usually near areas of bronchiectasis) • Absence of subpleural sparing |
• HRCT features of lung fibrosis that do not suggest any diagnosis | • Lung findings: • Cysts • Mosaic attenuation • GGO predominance (might be found if diagnosed during an AE-IFP) • Centrilobular micronodules • Nodules • Consolidations • Mediastinal findings: • Pleural plaques • Dilated esophagus |
Based on Raghu et al. 3 ) UIP: usual interstitial pneumonia; GGO: ground-glass opacities; and AE-IPF: acute exacerbation of idiopathic pulmonary fibrosis.
Figure 1. HRCT patterns in relation to usual interstitial pneumonia (UIP). In A, UIP pattern, showing exuberant honeycombing. In B, probable UIP pattern, with traction bronchiectasis and typical subpleural inferior distribution. In C, indeterminate for UIP, showing mild reticular and ground-glass opacities.
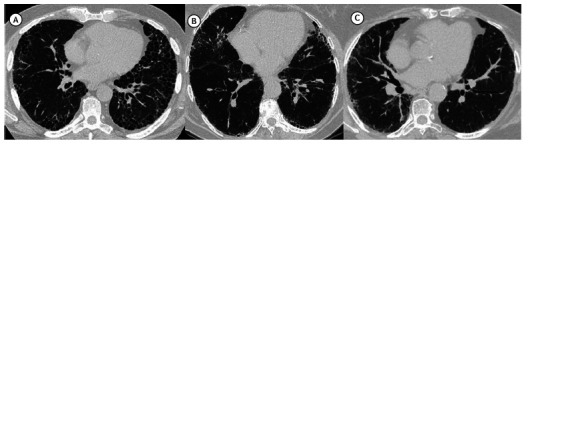
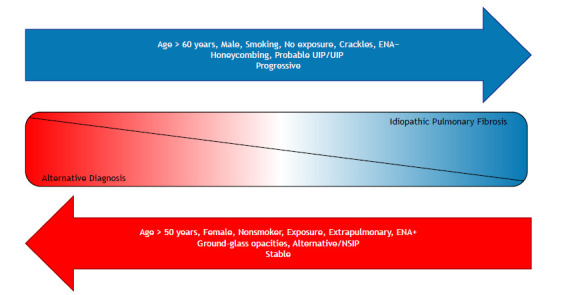
Figure 2. Probability of idiopathic pulmonary fibrosis based on clinical and radiological features. ENA: extractable nuclear antigen; UIP: usual interstitial pneumonia; NSIP: nonspecific interstitial pneumonia.
Differentiating IPF from other diseases has gained importance with current treatment approaches, but it is usually easier said than done, especially when dealing with diseases that might present with similar behavior and radiological appearance, such as fHP. Therefore, a provisional diagnosis with higher or lower confidence is acceptable in many practical clinical scenarios; however, the pursuit of alternative diagnosis should be restless. 12 , 13
When needed, lung sampling may be obtained either through open lung biopsy (preferably video-assisted thoracoscopy) or transbronchial cryobiopsy, which has become increasingly available. Choosing the best procedure should consider center expertise (both for the procedure and the pathological interpretation), individual contraindications, and preferences of patients. Some biomarkers for molecular diagnosis have shown promising results for a noninvasive diagnosis of a UIP pattern; however, they have not been incorporated into clinical practice and are not recommended as a standard of care yet. 3 , 14
In summary, the diagnostic criteria include the exclusion of alternative diagnosis of ILD (extensively investigated) and a UIP pattern on HRCT and/or lung biopsy or a combination of HRCT and/or histological patterns. 3
TREATMENT
Pharmacological treatment
The IPF treatment journey has been remarkable in terms of the number of failures in almost 25 years of clinical trials without positive results. 15 This has been motivated by an early (and, nowadays, abandoned) hypothesis that IPF could be the final pathway to persistent overt inflammation-most notably due to a changing practice clinical trial, the famously known PANTHER-IPF trial, that revealed an excessive death rate in the group of patients treated with a combination of prednisone, azathioprine, and N-acetylcysteine. 15 Anticoagulants and pulmonary circulation vasodilators have also been extensively studied with no convincing evidence of efficacy. 15
The understanding of IPF as a mostly fibrotic disease with minimal or no inflammation has inaugurated the antifibrotic era with two currently approved drugs: pirfenidone and nintedanib. Both have been FDA-approved in 2014, after concomitant publication of their phase III trials, although pirfenidone had already been used in Europe and Asia based on previous trials. 16 , 17 Recently, the “ILD world” has witnessed the growth of antifibrotic indications beyond IPF, the prototypical fibrotic disease, including their use for systemic sclerosis, unclassifiable ILD, and the progressive fibrotic phenotype.
Pirfenidone
The mechanism of action of pirfenidone is yet to be completely understood, but it is believed to reduce pro-fibrotic mediators, fibroblastic proliferation, and myofibroblast differentiation, mainly through TGF-β downregulation.
The recommended dosage is three 267-mg capsules thrice a day. The most common adverse reactions include cutaneous rash or photosensitivity and gastrointestinal effects (mainly nausea or vomiting). Hepatic function should be monitored after treatment initiation owing to the risk of toxicity. 18
Nintedanib
Nintedanib is a tyrosine kinase inhibitor that acts mainly through three receptors: fibroblast growth factor receptor (FGFR), platelet-derived growth factor receptor (PDFGR) and vascular endothelial growth receptor (VEGFR).
The suggested posology consists of 150 mg twice daily. The most common adverse reactions include gastrointestinal side effects, mainly diarrhea (about 60% of patients). Loperamide or dose reduction is usually effective in its management. Liver enzymes should also be monitored because of the increased risk of toxicity. It should also be administered with caution in patients with recent cardiovascular events or concomitant use of anticoagulants owing to its mechanism of action (including an exclusion criterion for these populations in pivotal trials). 18
The pivotal trials that culminated in the new paradigm of IPF treatment used a surrogate endpoint of FVC decline over 52 weeks, demonstrating an attenuation of functional loss by approximately 50% in a year. However, aggregated data from studies and, more recently, real-world cohort studies (mainly from world registries from different regions of the globe) have consistently shown mortality reduction, augmented progression-free survival, and reduced acute exacerbations, with sustained long-term effects. 19 , 20
Nathan et al. 21 evaluated aggregated data from three main pirfenidone randomized trials (CAPACITY 004, CAPACITY 006, and ASCEND trials) and found a 52-week mortality reduction. 20 - 22 Similarly, the combination of phase II (TOMORROW) and phase III (INPULSIS I and INPULSIS 2) trials of nintedanib have also shown mortality reduction in 52 weeks, when compared with placebo, as well as a delayed time to a first acute exacerbation and a borderline (not significant) reduction of mortality from all causes. 19 , 23 A further analysis that included the extended open-label trial (INPULSIS-ON) 24 and an exploratory phase IIIb trial (combined for more than 1,000 patients) suggested a 5-year extended survival in the treated group of patients (median survival of 3 years in the placebo group and of 8 years in the treated group).
Outside the clinical trial settings, evidence also supports the use of antifibrotics. Dempsey et al. 25 evaluated a large database of over 8,000 patients in the USA using propensity score matching and found a global mortality reduction and fewer hospitalizations in the treated group. No differences were found between both the available medications, suggesting a similar efficacy. A Korean group of researchers conducted a similar analysis with longer follow-up and found a similar reduction in mortality, respiratory hospitalizations, acute exacerbations, and annual mortality rates at 1, 3, and 5 years. 26
Several national or regional registries with real-world data have corroborated these findings. The Australian IPF Registry, which included patients with several comorbidities, a wide range of disease severity, and older age (i.e., patients usually left out of randomized trials), found better survival in the patients treated with antifibrotics regardless of disease severity at baseline. 27 Accordingly, the Finish IPF registry encompassed 28 centers and found a survival benefit in patients who received at least 6 months of treatment, even when taking account of between-group differences due to access to treatment (medication was reserved for patients with FVC between 50-90% of predicted values). 28 The Swedish IPF registry also found a survival benefit and longer transplant-free survival in patients with more severe disease (GAP index ≥ 2). 29
The 2-year follow-up analysis of the German IPF registry likewise found a significant reduction in mortality from 87% in the treated group against 46% in patients without treatment in 1 year, and from 62% against 21%, respectively, in the 2-year period. Curiously, these findings remained significant even after a multivariate analysis that failed to demonstrate any difference in lung function loss in the period between the two groups, suggesting that antifibrotic treatment benefits in mortality reduction might occur regardless of FVC and DLco trajectories. 30
More recently, a systematic review and meta-analysis of 26 studies 31 comprising almost 13,000 patients have shown a reduction in mortality from all causes, with a relative risk of 0.55 (95% CI, 0.45-0.66) favoring antifibrotics. The effect was consistent across a sensitivity analysis and in different subgroups, including study type (randomized trial or cohort study), risk of bias, duration of follow-up, and studied drug. The same study suggested a reduction in AE-IPF risk of the same magnitude (hazard ratio [HR] = 0.63; 95% CI, 0.53-0.76). 31
Given the rarity of the disease and the costs and restraints of conducting randomized controlled trials in this population of patients, although findings of aggregated populations and real-world data are largely subject to bias, 32 one might anticipate that the current evidence is almost definitive. Therefore, it should be regarded as enough to reassure a probable survival benefit and a significant reduction in mortality due to IPF, while further studies should assess the effects of new drugs currently under development or waiting for evidence-based analysis in combination with the current standard of care (Table 2). 16 , 17 , 19 - 28 , 30 , 31 , 33 - 41
Table 2. Main studies evaluating the impact of antifibrotics on idiopathic pulmonary fibrosis regarding mortality and acute exacerbation of idiopathic pulmonary fibrosis.
| Study | Study Type | Year | Antifibrotic | Outcome | Main Findings | Mortality Reduction | Effect on Acute Exacerbation |
|---|---|---|---|---|---|---|---|
| SHIONOGI Phase 2 - Research Group for Diffuse Lung Diseases Azuma et al. 17 | Randomized phase II trial | 2005 | Pirfenidone | Lowest oxygen saturation during 6MWT | Negative for the primary endpoint, but pirfenidone significantly reduced the decline in vital capacity at 9 months and reduced the incidence of acute exacerbations when compared with placebo. | No | Yes |
| SHIONOGI Phase 3 - Pirfenidone Clinical Study Group Taniguchi et al. 16 | Randomized trial | 2010 | Pirfenidone | FVC decline | Pirfenidone reduced the decline of lung function and improved progression-free survival. | No | No |
| CAPACITY-004 and CAPACITY-006 Noble et al. 22 | Randomized trial | 2011 | Pirfenidone | FVC decline | Pirfenidone reduced the rate of decline in FVC at 72 weeks in CAPACITY-004 (but not in CAPACITY-006) and reduced the mean change from baseline in 6MWD and improved progression-free survival in the pooled analysis. | No | N/A |
| TOMORROW Richeldi et al. 19 | Randomized phase II trial | 2011 | Nintedanib | FVC decline | Nintedanib reduced annual decline in FVC, incidence of acute exacerbations, and SGRQ score (improved quality of life) | No | Yes |
| INPULSIS-1 and INPULSIS-2 Richeldi et al. 23 | Randomized trial | 2014 | Nintedanib | FVC decline | Nintedanib reduced the annual rate of decline in FVC by 51% (p < 0.001) | No | Yesa |
| ASCEND King Jr. et al. 20 | Randomized trial | 2014 | Pirfenidone | FVC decline | Pirfenidone reduced change in FVC from baseline and improved progression-free survival (defined as death, decrease in FVC, or decrease in 6MWD). | No | N/A |
| Washington Group Canestaro et al. 33 | Systematic Review and Meta-analysis | 2016 | Pirfenidone + Nintedanib | All-cause and respiratory-specific death | Negative for primary endpoint, but pirfenidone and nintedanib had effects approaching significance under a fixed-effects model for all-cause mortality. | No | N/A |
| Combined CAPACITY and ASCEND trials Noble et al. 34 | Pooled analysis | 2016 | Pirfenidone | FVC decline or death | Pirfenidone reduced decline in lung function and improved other measures such as progression-free survival, 6MWD, and dyspnea. | Yes | N/A |
| Combined TOMORROW and INPULSIS Richeldi et al. 23 | Pooled analysis | 2016 | Nintedanib | FVC decline, acute exacerbation, SGRQ, and mortality in 52 weeks | Nintedanib reduced FVC decline, time to first acute exacerbation and on-treatment (but not all-cause) mortality | No | Yes |
| RECAP Costabel et al. 35 | Open-label extension study | 2016 | Pirfenidone | Long-term safety | Pirfenidone was deemed to be safe. Sustained effect on FVC decline and a median on-treatment survival of 77.2 months was observed. | N/A | N/A |
| Combined SHIONOGI, CAPACITY and ASCEND trials Nathan et al. 21 | Pooled analysis | 2017 | Pirfenidone | Long-term mortality (120 weeks) | Pirfenidone was associated with a reduced relative risk of death for patients for all mortality outcomes (all-cause mortality, treatment-emergent all-cause mortality, idiopathic-pulmonary-fibrosis-related mortality, and treatment-emergent idiopathic-pulmonary-fibrosis-related mortality). | Yes | N/A |
| AIPFR Jo et al. 27 | Real-life Registry from Australia | 2017 | Pirfenidone + Nintedanib | Baseline characteristics | Improved survival in patients taking antifibrotics even after multivariate analysis adjusted for age, gender, smoking, BMI, and baseline lung function. | Yes | N/A |
| INSTAGE Kolb et al. 36 | Randomized trial | 2018 | Nintedanib + sildenafil | Change in SGRQ | Addition of sildenafil to nintedanib did not improve dyspnea and similar percentages of patients had at least one acute exacerbation or died. | No | No |
| Post-hoc CAPACITY and ASCEND trials Nathan et al. 37 | Pooled data analysis | 2018 | Pirfenidone | Continued effect of pirfenidone after a disease progression event | Patients receiving pirfenidone who experienced an initial absolute or relative decline in percent predicted FVC were less likely to experience further decline in lung function or death in the subsequent 6 months compared with those receiving placebo. | Yes | Yesb |
| INPULSIS-ON Crestani et al. 24 | Open-label extension study | 2018 | Nintedanib | Safety and long-term efficacy | Nintedanib had a safety profile consistent with that observed in the INPULSIS trials and effect on slowing progression persisted beyond 4 years. | N/A | N/A |
| Post-hoc TOMORROW, INPULSIS, INPULSIS-ON and Phase IIIb trial Lancaster et al. 38 | Pooled data analysis | 2019 | Nintedanib | Safety and survival | Treatment with nintedanib was considered safe. Survival was estimated as 11.6 years in the treated group (versus 3.7 in the placebo group). | Yes | N/A |
| EMPIRE Zurkova et al. 39 | Real-life registry from Czech Republic | 2019 | Pirfenidone | Overall survival and FVC decline | Pirfenidone increased overall 5-year survival versus no-antifibrotics (55.9% vs. 31.5% alive, respectively, p = 0.002). | Yes | No |
| FinnishIPF Kaunisto et al. 28 | Real-life registry from Finland | 2019 | Pirfenidone + Nintedanib | Demographics and survival | Patients who received ≥ 6 months of treatment had better survival compared with those who did not receive treatment in the unadjusted analysis. | Yes | N/A |
| Insurance Database Dempsey et al. 25 | Retrospective cohort | 2019 | Pirfenidone + Nintedanib | Mortality and hospitalization | Lower risk of all-cause mortality and hospitalization compared with no treatment. | Yes | Yesb |
| IPF-PRO Snyder et al. 40 | Real-life registry | 2019 | Pirfenidone + Nintedanib | Predictors of death or lung transplant | The authors were unable to evaluate associations between the use of antifibrotic therapy at enrollment and death or lung transplant. | N/A | N/A |
| INSIGHTS-IPF Registry Behr et al. 30 | Real-life registry in Germany | 2020 | Pirfenidone + Nintedanib | Survival and FVC decline | Survival was significantly higher in IPF patients on antifibrotic therapy, but the course of lung function parameters was similar in patients on antifibrotic therapy or not. | Yes | N/A |
| Korean Cohort Kang et al. 26 | Retrospective cohort | 2020 | Pirfenidone + Nintedanib | Mortality, hospitalization, and acute exacerbation | Antifibrotic treatment significantly reduced the risks of mortality [hazard ratio (HR) = 0.59], all-cause hospitalization (HR = 0.71), respiratory-related hospitalization (HR = 0.67), acute exacerbation (HR = 0.69), and mortality after acute exacerbation (HR = 0.60). | Yes | Yes |
| Petnak et al. 31 | Systematic review and meta-analysis | 2021 | Pirfenidone + Nintedanib | Mortality and acute exacerbations | Antifibrotic treatment appears to reduce the risk of all-cause mortality and acute exacerbations. | Yes | Yes |
| REFIPI Caro et al. 41 | Real-life registry | 2022 | Pirfenidone + Nintedanib | Demographic, clinical, serological, functional, tomographic, histological, and treatment variables | Most patients in the REFIPI received antifibrotics, which were well tolerated and associated with a lower rate of adverse events than that reported in clinical trials. | N/A | N/A |
IPF: idiopathic pulmonary fibrosis; AE-IPF: acute exacerbation of IPF; 6MWT: six-minute walking test; SGRQ: Saint-George’s Respiratory Questionnaire; and 6MWD: six-minute walk distance. aOnly INPULSIS-1 showed a reduction in the incidence of AE-IPF. bRespiratory-related hospitalization was analyzed as a surrogate for AE-IPF.
GERD treatment
The latest IPF guidelines 3 have withdrawn an early conditional recommendation of universal GERD treatment for IPF patients (even without symptoms) with antacid therapy. The prevalence of GERD in IPF patients is high, but evidence for its treatment (regarding lung disease) is conflicting. A recent meta-analysis failed to demonstrate any effect on mortality, number of hospitalizations, or functional decline in patients treated with proton pump inhibitors. 42 Reflux surgery has also been proposed; however, although safe, the primary endpoint was not reached in a randomized controlled trial. 43 Therefore, GERD treatment in the IPF population should follow recommendations from GERD guidelines. 3
Special situations
Early or late disease
The efficacy of antifibrotic therapy (AFT) seems to be ubiquitous, working just as well in the subset of patients with early disease as in those with more advanced disease. 35 , 44 , 45 Early initiation of AFT is advocated due to its effect of attenuating functional loss (although not reversing any), but this decision should also consider diagnostic confidence, safety profile, life expectancy, and quality-of-life issues. However, the unpredictable course of the disease and the risk of AE-IPF warrant a prompt decision (without long watchful waiting periods). On the other hand, patients with more advanced disease (such as those with FVC < 50%) are still AFT candidates, since the effect of treatment is of the same magnitude, but greater mortality and increased risk of adverse effects should guide therapeutic decisions.
Elderly
IPF is an elderly disease, with rare exceptions (mostly in the context of familial IPF). However, patients > 75 years of age have an increased risk of adverse effects and higher discontinuation rates. Therefore, AFT should be used with more caution in this population. 46 Notwithstanding, frailty, as a measure of functional age, is very common in elderly IPF patients 47 and seems to have a greater impact on adverse events than biological age itself (even when adding measurement of telomere length to the analysis). 48 Hence, identifying patients with a critical state of frailty may be a better option than using age alone when selecting appropriate therapeutic strategies.
Switching
Although severe adverse events are rare and most side effects are manageable, some patients discontinue medication due to intolerance. Additionally, some patients may have their medication switched due to inefficacy (usually defined as a > 10% decline in FVC in 1 year or an acute exacerbation). Switching AFT appears to be safe, but evidence of its efficacy is scarce. In addition, AFT efficacy does not seem to disappear after an event of progression; therefore, continuity seems to be a reasonable option (and preferred over discontinuation alone). 49 - 51
Accessibility
AFT in some countries, including Brazil, is restricted and, sometimes, exacerbates social disparities in access to health care (for instance, due to its prohibitive costs or in situations where medication is obtained only through litigation). European registries show that treatment availability rates vary from 26% to 78% for patients at different sites. 28 , 52 The Latin-American IPF registry (REFIPI) showed that 72% of participants were on some antifibrotic medication; however, underrepresentation of most populated countries/regions and selection bias probably overestimated access. 41 Many international regulation agencies, including those in Canada (CADTH), Australia (PBS), Portugal (Infarrmed), and the United Kingdom (NICE), have incorporated access to antifibrotics in their standard of care.
Comorbidities
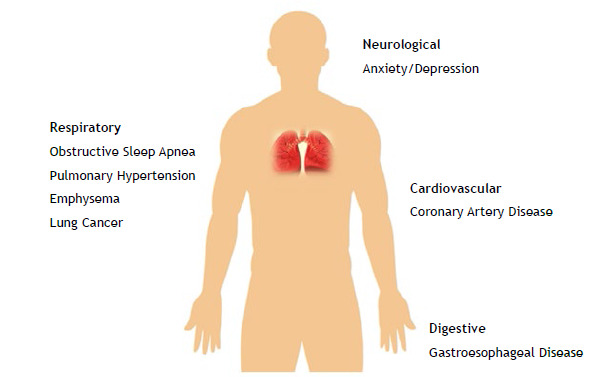
Comorbidity incidences surpass what would be expected for IPF patients even after taking into account shared risk factors (such as smoking and age) and have a negative impact on prognosis. 53 In addition to GERD (addressed above), some comorbidities deserve special attention (Figure 3).
Figure 3. Main comorbidities in idiopathic pulmonary fibrosis.
Lung cancer
The risk of lung cancer is increased in IPF patients, and this is one of the leading causes of mortality in this population. 28 The most frequent histology is squamous cell carcinoma, and most cancers are found in the lower lobes (as opposed to adenocarcinomas and upper lobe predominance in the general population). The concomitancy of diagnosis is associated with poor prognosis (worse than the sum of each isolated condition), even with potentially resectable nodules (i.e., early disease), and treatment can be very challenging, since all treatment modalities (chemotherapy, radiotherapy, or surgery) are associated with increased risks, especially that of AE-IPF. 6 , 54 Some experts recommend screening patients with HRCT annually, even if clinically stable, due to the augmented risk of lung cancer; however, the frequency of screening, concerns with unnecessary radiation exposure, and clear benefits of this strategy remain unknown.
Pulmonary hypertension
Pulmonary hypertension (PH) is a common IPF complication and has long been associated with increased mortality risk. 6 , 55 Several pulmonary circulation vasodilators have been studied for IPF treatment (even without concomitant PH); however, although these medications appear to be safe, they have not been demonstrated to benefit the disease course. Inhaled therapies (specifically treprostinil) have shown promising results, with increased walk distance on 6MWT, longer time to clinical worsening, and decrease in brain natriuretic peptide when compared with placebo in a clinical trial. 56 However, the short follow-up period and high discontinuation rates highlight the need for confirmation of these promising results in future trials.
Cardiovascular disease
ILDs in general, and IPF in particular, increase the risk of cardiovascular disease, mainly acute myocardial infarction (MI) and chronic coronary artery disease (CAD). A cohort study of over 68,000 patients suggested that IPF is an independent risk factor for CAD (even after taking into account other risk factors such as age and smoking), especially in the population of patients between 60 and 79 years of age. 57 Although chronic CAD was more common in men, women had a higher risk of acute MI. A particular challenge is the differential diagnosis of worsening dyspnea in IPF patients (since CAD can lead to dyspnea or fatigue as an anginal equivalent) and exercise-induced hypoxia that could lead to increased ischemic events; therefore, a high index of suspicion from doctors is needed to diagnose CAD and MI in this population. 57
Sleep disorders
Obstructive sleep apnea is extremely common in IPF patients, with a prevalence ranging from 50% to 90%. Some authors have suggested a common physiopathology of the two entities, with high-pressure swings, intermittent hypoxia, and association with GERD (and microaspirations) as possible etiologies for IPF due to recurrent injury. Most patients have less typical symptoms (such as excessive daytime sleepiness, snoring, and witnessed apnea). Likewise, lower BMI and higher desaturation indices, sometimes even in the absence of obstructive events, are found. Treatment with positive pressure (CPAP) seems challenging, with lower adherence and uncertainty regarding its efficacy. 58
Mood disorders
Patients with IPF are at an increased risk for anxiety and depression. Symptoms of both disorders may be present in up to two-thirds of patients, even without fulfilling criteria for a specific mental illness. These symptoms correlate with respiratory symptoms (i.e., cough and dyspnea) and with disease severity, GAP index, and walk distance on the 6MWT. 59
Emphysema
IPF and COPD share many risk factors, especially age and smoking; therefore, emphysema findings on HRCT are common (in up to 30% of IPF patients). However, the clinical impact of this finding will come down to the extension of both diseases-the upper predominance of emphysema and lower predominance of fibrosis constitutes a separate entity, frequently referred to as “combined pulmonary fibrosis and emphysema” or CPFE. The North-American IPF registry estimated the prevalence of CPFE in IPF patients to be approximately 13%. CPFE has some important distinct characteristics, such as pulmonary function pseudonormalization (with relative preservation of flows and volumes and accentuated loss of DLco), which impairs the use of FVC in the follow-up of this population. Besides that, PH seems to be more prevalent in this subgroup and has been associated with worse prognosis, although it can probably be explained by the sum of the extension of the two major components (emphysema and fibrosis). 6 , 60
Acute exacerbation
AE-IPF, as previously defined, is a rather frequent and life-threatening event in IPF patients, accounting for a number of IPF-related deaths. Prognosis is poor, with mortality rates as high as 50%. Baseline disease severity negatively impacts the risk of AE-IPF.
No treatment has been shown to be effective, and corticosteroids remain the treatment of choice; however, evidence for this suggestion relies mainly on retrospective data and expert opinion. Several immunomodulatory therapies have already been employed as well, with conflicting results and relying a lot on single-center experiences. 11 Prevention of AE-IPF with antifibrotics remains the sole best evidence-based treatment, although many patients may still experience an AE-IPF event while on AFT (although with a delayed time to the first event and decreased frequency).
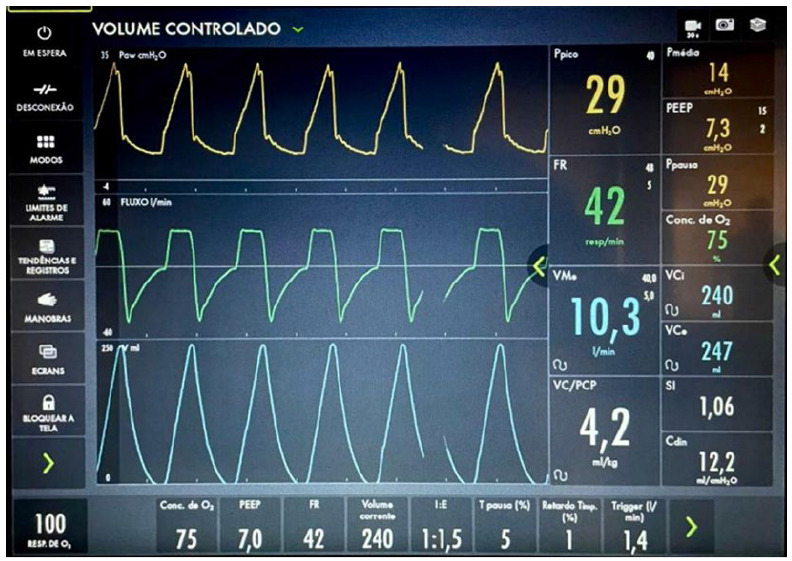
Acute or acute-on-chronic respiratory failure in these patients can be incredibly challenging. Mechanical ventilation (MV) in this population shares many features with ARDS, with greater lung heterogeneity but no lung recruitability, making protective ventilation strategies almost impossible in some cases (Figure 4). Employment of higher PEEP values has been associated with increased mortality, probably due to greater hyperinflation of healthy (with better compliance) lung portions, although no causality has been established. Owing to the high mortality rates, some authors have considered IPF a contraindication to MV, unless in the context of a bridge to lung transplant (LTx), but it might be employed in other situations, such as elective surgeries (e.g., surgical lung cancer treatment), when patients’ initial presentation of the disease is an AE-IPF, and even in some special conditions (such as COVID-19 in a patient with early or moderate disease, which is thought to be reversible in an expected time frame). Noninvasive ventilation seems to be an alternative, but with a greater risk of barotrauma. The use of high-flow nasal cannula is a feasible option, with decreased work of breathing and delivery of high Fio2 with better tolerability; however, evidence for its use (regarding clinical endpoints) is also lacking. 61
Figure 4. Mechanical ventilation parameters in a patient with acute exacerbation of idiopathic pulmonary fibrosis. Mechanical ventilation in this setting can be very challenging: note the high concentrations of oxygen (Fio2 = 75%) and low static lung compliance (estimated on 11 mL/cmH2O), with high driving pressure swings (22 cmH2O) even with high respiratory rates (42 breaths/min) to prevent severe respiratory acidosis.
Lung transplantation
Every patient with IPF should be considered for referral to a LTx center at diagnosis due to its poor prognosis, unless contraindications are readily identified, although inclusion in waiting lists must take account of the disease course (including hospitalizations) and the presence of comorbidities such as PH. ILD has surpassed COPD as the primary indication for LTx in the USA since an allocation score system has been adopted. Adequate selection of candidates is crucial, involving the impact of comorbidities, adherence to treatment, social and emotional aspects, and general risk profiling in order to achieve better outcomes, especially in settings of scarce supply of donors. Median survival is approximately 5 years, and many complications may arise after the procedure, particularly infection and chronic lung dysfunction; however, it has been demonstrated that LTx increases survival and improves symptoms in patients with advanced IPF. 3
Rehabilitation
A pulmonary rehabilitation program (PRP) appears to be safe and is associated with improvement in symptoms, exercise capacity, and general quality of life. Data regarding long-term effects and mortality are still lacking, but it may be considered for any symptomatic patient with IPF. PRPs are also frequently employed perioperatively in LTx to improve outcomes. 62
Symptom management and advanced disease
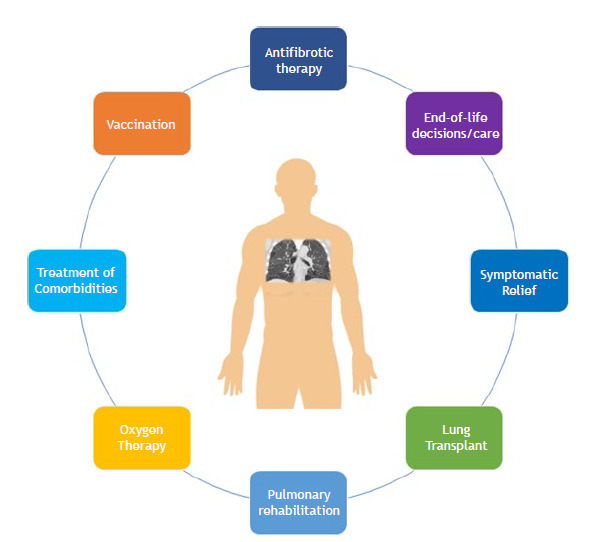
Disease course modifying drugs, such as AFT, have changed IPF treatment paradigms, but are not ideal, since disease course is still inexorable, besides having little or no impact on quality of life; therefore, caring for patients with IPF must include general measures, such as education about the disease course, smoking cessation strategies (when applicable), and immunization, along with palliative care (Figure 5). Palliative care is defined as symptom-based treatments aimed at improving quality of life and relief from suffering when indicated. It is often applied only to end-of-life care, but its use in early stages of diseases has been associated with extended survival and better quality of life in patients with lung cancer and refractory dyspnea from different causes. 63 Advanced care planning is key, preferably when patients are still able to make active decisions regarding their treatment strategies. 64
Figure 5. Management of patients with idiopathic pulmonary fibrosis.
Indications for ambulatory oxygen therapy generally follow those for COPD patients (Spo2 below 88% at room air or between 88% and 90% when associated with polycythemia and/or PH), although evidence is limited for IPF patients. Exercise-induced hypoxia starts earlier in the course of disease, and oxygen use may alleviate symptoms, increase walk distance, and even improve short-term quality of life; however, health care costs and the burden of oxygen delivery systems should be weighed against their potential benefits. 65
Dyspnea is usually the most debilitating symptom and can be effectively treated with opioids (e.g., morphine), alongside oxygen therapy, and PRP when indicated. Other nonpharmacological strategies such as breathing techniques, a hand-held fan, pacing guidance, and access to a breathlessness support service have been employed with great success in the treatment of refractory patients. 66 Cough is another important symptom and is sometimes very intense, and opioids are also first-line options, although codeine is usually preferred over morphine. Other strategies include treatment of comorbidities (such as GERD and rhinitis) and several options with lower quality evidence (such as gabapentin, corticosteroids, and even pirfenidone).
Perspectives
IPF remains the prototypical fibrotic ILD and, although AFT has been expanded to other ILDs, its long-standing history of trials, the validation of FVC as a surrogate endpoint, its presentation as an almost exclusively fibrotic disease, and its poor survival (which makes it suitable for shorter term studies) makes it an ideal candidate for trying out new therapies. In addition, current treatments, although effective, are far from perfect, since their effect on ameliorating lung function decline might be considered mere palliation, even if prolonged survival is indeed achieved.
Three recent drugs have shown promising results in phase II trials: pamrevlumab, a monoclonal antibody against connective-tissue growth factor, which reduced FVC decline in 48 weeks 67 ; recombinant human pentraxin-2 protein, which showed a sustained effect on attenuating functional and walking distance declines in 24 weeks, 68 although a phase III open-label trial evaluating its safety and efficacy was terminated early due to an interim analysis indicating futility 69 ; and a phosphodiesterase 4B inhibitor that prevented lung function decline at 12 weeks. 70 Currently, at least 15 randomized controlled trials are underway to evaluate the treatment of patients with chronic IPF or AE-IPF.
The future of IPF treatment, therefore, holds new perspectives of integrating early, less invasive diagnosis (with an essential role of biomarkers, which have been at the forefront of a great deal of research) and therapies aimed at restraining disease progression, most probably based on personalized or precision medicine (through targeting of genetic modification, for instance). 71
Footnotes
Financial support: None.
Study carried out in the Divisão de Pneumologia, Instituto do Coração - InCor - Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo (SP) Brasil.
REFERENCES
- 1.Lederer DJ, Martinez FJ. Idiopathic Pulmonary Fibrosis. N Engl J Med. 2018;378(19):1811–1823. doi: 10.1056/NEJMra1705751. [DOI] [PubMed] [Google Scholar]
- 2.Raghu G, Remy-Jardin M, Myers JL. Diagnosis of Idiopathic Pulmonary Fibrosis An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am J Respir Crit Care Med. 2018;198(5):e44–e68. doi: 10.1164/rccm.201807-1255ST. [DOI] [PubMed] [Google Scholar]
- 3.Raghu G, Remy-Jardin M, Richeldi L, Thomson CC, Antoniou KM, Bissell BD. Idiopathic Pulmonary Fibrosis (an Update) and Progressive Pulmonary Fibrosis in Adults An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am J Respir Crit Care Med. 2022;205(9):e18–e47. doi: 10.1164/rccm.202202-0399ST. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kaul B, Lee JS, Zhang N, Vittinghoff E, Sarmiento K, Collard HR. Epidemiology of Idiopathic Pulmonary Fibrosis among U S. Veterans, 2010-2019. Ann Am Thorac Soc. 2022;19(2):196–203. doi: 10.1513/AnnalsATS.202103-295OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Baddini-Martinez J, Pereira CA. How many patients with idiopathic pulmonary fibrosis are there in Brazil [published correction appears in J Bras Pneumol. 2016 Jan-Feb;42(1):78]. J Bras. Pneumol. 2015;41(6):560–561. doi: 10.1590/s1806-37562015000000165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Podolanczuk AJ, Thomson CC, Remy-Jardin M, Richeldi L, Martinez FJ, Kolb M. Idiopathic pulmonary fibrosis state of the art for 2023. Eur Respir J. 2023;61(4):2200957–2200957. doi: 10.1183/13993003.00957-2022. [DOI] [PubMed] [Google Scholar]
- 7.Selman M, Pardo A. When things go wrong exploring possible mechanisms driving the progressive fibrosis phenotype in interstitial lung diseases. Eur Respir J. 2021;58(3):2004507–2004507. doi: 10.1183/13993003.04507-2020. [DOI] [PubMed] [Google Scholar]
- 8.Phan THG, Paliogiannis P, Nasrallah GK, Giordo R, Eid AH, Fois AG. Emerging cellular and molecular determinants of idiopathic pulmonary fibrosis. Cell Mol Life Sci. 2021;78(5):2031–2057. doi: 10.1007/s00018-020-03693-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Richeldi L, Ryerson CJ, Lee JS, Wolters PJ, Koth LL, Ley B. Relative versus absolute change in forced vital capacity in idiopathic pulmonary fibrosis. Thorax. 2012;67(5):407–411. doi: 10.1136/thoraxjnl-2011-201184. [DOI] [PubMed] [Google Scholar]
- 10.Ley B, Collard HR, King TE., Jr Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183(4):431–440. doi: 10.1164/rccm.201006-0894CI. [DOI] [PubMed] [Google Scholar]
- 11.Collard HR, Ryerson CJ, Corte TJ, Jenkins G, Kondoh Y, Lederer DJ. Acute Exacerbation of Idiopathic Pulmonary Fibrosis An International Working Group Report. Am J Respir Crit Care Med. 2016;194(3):265–275. doi: 10.1164/rccm.201604-0801CI. [DOI] [PubMed] [Google Scholar]
- 12.Takei R, Yamano Y, Kataoka K, Yokoyama T, Matsuda T, Kimura T. New Guideline Diagnosis of Fibrotic Hypersensitivity Pneumonitis in Idiopathic Pulmonary Fibrosis. Am J Respir Crit Care Med. 2021;204(5):603–605. doi: 10.1164/rccm.202102-0407LE. [DOI] [PubMed] [Google Scholar]
- 13.O'Callaghan M, Bonella F, McCarthy C, O'Callaghan M, Bonella F, McCarthy C. Unclassifiable, or simply unclassified interstitial lung disease? Curr Opin Pulm Med. 2021;27(5):405–413. doi: 10.1097/MCP.0000000000000801. [DOI] [PubMed] [Google Scholar]
- 14.Richeldi L, Scholand MB, Lynch DA, Colby TV, Myers JL, Groshong SD. Utility of a Molecular Classifier as a Complement to High-Resolution Computed Tomography to Identify Usual Interstitial Pneumonia. Am J Respir Crit Care Med. 2021;203(2):211–220. doi: 10.1164/rccm.202003-0877OC. [DOI] [PubMed] [Google Scholar]
- 15.Raghu G. Idiopathic pulmonary fibrosis lessons from clinical trials over the past 25 years. Eur Respir J. 2017;50(4):1701209–1701209. doi: 10.1183/13993003.01209-2017. [DOI] [PubMed] [Google Scholar]
- 16.Taniguchi H, Ebina M, Kondoh Y, Ogura T, Azuma A, Suga M. Pirfenidone in idiopathic pulmonary fibrosis. Eur Respir J. 2010;35(4):821–829. doi: 10.1183/09031936.00005209. [DOI] [PubMed] [Google Scholar]
- 17.Azuma A, Nukiwa T, Tsuboi E, Suga M, Abe S, Nakata K. Double-blind, placebo-controlled trial of pirfenidone in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2005;171(9):1040–1047. doi: 10.1164/rccm.200404-571OC. [DOI] [PubMed] [Google Scholar]
- 18.Collins BF, Luppi F. Diagnosis and Management of Fibrotic Interstitial Lung Diseases. Clin Chest Med. 2021;42(2):321–335. doi: 10.1016/j.ccm.2021.03.008. [DOI] [PubMed] [Google Scholar]
- 19.Richeldi L, du Bois RM, Raghu G, Azuma A, Brown KK, Costabel U. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis [published correction appears in N Engl. J Med. 2015;373(8):782–782. doi: 10.1056/NEJMoa1402584. [DOI] [PubMed] [Google Scholar]
- 20.King TE, Jr, Bradford WZ, Castro-Bernardini S, Fagan EA, Glaspole I, Glassberg MK. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis [published correction appears in N Engl. J Med. 2014;371(12):1172–1172. doi: 10.1056/NEJMoa1402582. [DOI] [PubMed] [Google Scholar]
- 21.Nathan SD, Albera C, Bradford WZ, Costabel U, Glaspole I, Glassberg MK. Effect of pirfenidone on mortality pooled analyses and meta-analyses of clinical trials in idiopathic pulmonary fibrosis [published correction appears in Lancet Respir. Med. 2017;5(1):e7. doi: 10.1016/S2213-2600(16)30326-5. [DOI] [PubMed] [Google Scholar]
- 22.Noble PW, Albera C, Bradford WZ, Costabel U, Glassberg MK, Kardatzke D. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY) two randomised trials. Lancet. 2011;377(9779):1760–1769. doi: 10.1016/S0140-6736(11)60405-4. [DOI] [PubMed] [Google Scholar]
- 23.Richeldi L, Cottin V, du Bois RM, Selman M, Kimura T, Bailes Z. Nintedanib in patients with idiopathic pulmonary fibrosis Combined evidence from the TOMORROW and INPULSIS((r)) trials. Respir Med. 2016;113:74–79. doi: 10.1016/j.rmed.2016.02.001. [DOI] [PubMed] [Google Scholar]
- 24.Crestani B, Huggins JT, Kaye M, Costabel U, Glaspole I, Ogura T. Long-term safety and tolerability of nintedanib in patients with idiopathic pulmonary fibrosis results from the open-label extension study, INPULSIS-ON. Lancet Respir Med. 2019;7(1):60–68. doi: 10.1016/S2213-2600(18)30339-4. [DOI] [PubMed] [Google Scholar]
- 25.Dempsey TM, Sangaralingham LR, Yao X, Sanghavi D, Shah ND, Limper AH. Clinical Effectiveness of Antifibrotic Medications for Idiopathic Pulmonary Fibrosis. Am J Respir Crit Care Med. 2019;200(2):168–174. doi: 10.1164/rccm.201902-0456OC. [DOI] [PubMed] [Google Scholar]
- 26.Kang J, Han M, Song JW. Antifibrotic treatment improves clinical outcomes in patients with idiopathic pulmonary fibrosis a propensity score matching analysis. Sci Rep. 2020;10(1):15620–15620. doi: 10.1038/s41598-020-72607-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jo HE, Glaspole I, Grainge C, Goh N, Hopkins PM, Moodley Y. Baseline characteristics of idiopathic pulmonary fibrosis analysis from the Australian Idiopathic Pulmonary Fibrosis Registry [published correction appears in Eur Respir J. 2017 Mar 29;49(3):]. Eur Respir. 2017;49(2):1601592–1601592. doi: 10.1183/13993003.01592-2016. [DOI] [PubMed] [Google Scholar]
- 28.Kaunisto J, Salomaa ER, Hodgson U, Kaarteenaho R, Kankaanranta H, Koli K. Demographics and survival of patients with idiopathic pulmonary fibrosis in the FinnishIPF registry. ERJ Open Res. 2019;5(3):00170–02018. doi: 10.1183/23120541.00170-2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Gao J, Kalafatis D, Carlson L, Pesonen IHA, Li CX, Wheelock Å. Baseline characteristics and survival of patients of idiopathic pulmonary fibrosis a longitudinal analysis of the Swedish IPF Registry. Respir Res. 2021;22(1):40–40. doi: 10.1186/s12931-021-01634-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Behr J, Prasse A, Wirtz H, Koschel D, Pittrow D, Held M. Survival and course of lung function in the presence or absence of antifibrotic treatment in patients with idiopathic pulmonary fibrosis long-term results of the INSIGHTS-IPF registry. Eur Respir J. 2020;56(2):1902279–1902279. doi: 10.1183/13993003.02279-2019. [DOI] [PubMed] [Google Scholar]
- 31.Petnak T, Lertjitbanjong P, Thongprayoon C, Moua T. Impact of Antifibrotic Therapy on Mortality and Acute Exacerbation in Idiopathic Pulmonary Fibrosis A Systematic Review and Meta-Analysis. Chest. 2021;160(5):1751–1763. doi: 10.1016/j.chest.2021.06.049. [DOI] [PubMed] [Google Scholar]
- 32.Suissa S, Suissa K. Antifibrotics and Reduced Mortality in Idiopathic Pulmonary Fibrosis Immortal Time Bias. Am J Respir Crit Care Med. 2023;207(1):105–109. doi: 10.1164/rccm.202207-1301LE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Canestaro WJ, Forrester SH, Raghu G, Ho L, Devine BE. Drug Treatment of Idiopathic Pulmonary Fibrosis Systematic Review and Network Meta-Analysis. Chest. 2016;149(3):756–766. doi: 10.1016/j.chest.2015.11.013. [DOI] [PubMed] [Google Scholar]
- 34.Noble PW, Albera C, Bradford WZ, Costabel U, du Bois RM, Fagan EA. Pirfenidone for idiopathic pulmonary fibrosis analysis of pooled data from three multinational phase 3 trials. Eur Respir J. 2016;47(1):243–253. doi: 10.1183/13993003.00026-2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Costabel U, Albera C, Lancaster LH, Lin CY, Hormel P, Hulter HN. An Open-Label Study of the Long-Term Safety of Pirfenidone in Patients with Idiopathic Pulmonary Fibrosis (RECAP) Respiration. 2017;94(5):408–415. doi: 10.1159/000479976. [DOI] [PubMed] [Google Scholar]
- 36.Kolb M, Raghu G, Wells AU, Behr J, Richeldi L, Schinzel B. Nintedanib plus Sildenafil in Patients with Idiopathic Pulmonary Fibrosis. N Engl J Med. 2018;379(18):1722–1731. doi: 10.1056/NEJMoa1811737. [DOI] [PubMed] [Google Scholar]
- 37.Nathan SD, Costabel U, Glaspole I, Glassberg MK, Lancaster LH, Lederer DJ. Efficacy of Pirfenidone in the Context of Multiple Disease Progression Events in Patients With Idiopathic Pulmonary Fibrosis. Chest. 2019;155(4):712–719. doi: 10.1016/j.chest.2018.11.008. [DOI] [PubMed] [Google Scholar]
- 38.Lancaster L, Crestani B, Hernandez P, Inoue Y, Wachtlin D, Loaiza L. Safety and survival data in patients with idiopathic pulmonary fibrosis treated with nintedanib pooled data from six clinical trials. BMJ Open Respir Res. 2019;6(1):e000397. doi: 10.1136/bmjresp-2018-000397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Zurkova M, Kriegova E, Kolek V, Lostakova V, Sterclova M, Bartos V. Effect of pirfenidone on lung function decline and survival 5-yr experience from a real-life IPF cohort from the Czech EMPIRE registry. Respir Res. 2019;20(1):16–16. doi: 10.1186/s12931-019-0977-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Snyder L, Neely ML, Hellkamp AS, O'Brien E, De Andrade J, Conoscenti CS, et al. Predictors of death or lung transplant after a diagnosis of idiopathic pulmonary fibrosis insights from the IPF-PRO Registry. Respir Res. 2019;20(1):105–105. doi: 10.1186/s12931-019-1043-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Caro F, Buendía-Roldán I, Noriega-Aguirre L, Alberti ML, Amaral A, Arbo G. Latin American Registry of Idiopathic Pulmonary Fibrosis (REFIPI) Clinical Characteristics, Evolution and Treatment. Arch Bronconeumol. 2022;58(12):794–801. doi: 10.1016/j.arbres.2022.04.007. [DOI] [PubMed] [Google Scholar]
- 42.Khor YH, Bissell B, Ghazipura M, Herman D, Hon SM, Hossain T. Antacid Medication and Antireflux Surgery in Patients with Idiopathic Pulmonary Fibrosis A Systematic Review and Meta-Analysis. Ann Am Thorac Soc. 2022;19(5):833–844. doi: 10.1513/AnnalsATS.202102-172OC. [DOI] [PubMed] [Google Scholar]
- 43.Raghu G, Pellegrini CA, Yow E, Flaherty KR, Meyer K, Noth I. Laparoscopic anti-reflux surgery for the treatment of idiopathic pulmonary fibrosis (WRAP-IPF) a multicentre, randomised, controlled phase 2 trial. Lancet Respir Med. 2018;6(9):707–714. doi: 10.1016/S2213-2600(18)30301-1. [DOI] [PubMed] [Google Scholar]
- 44.Kolb M, Richeldi L, Behr J, Maher TM, Tang W, Stowasser S. Nintedanib in patients with idiopathic pulmonary fibrosis and preserved lung volume. Thorax. 2017;72(4):340–346. doi: 10.1136/thoraxjnl-2016-208710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Wuyts WA, Kolb M, Stowasser S, Stansen W, Huggins JT, Raghu G. First Data on Efficacy and Safety of Nintedanib in Patients with Idiopathic Pulmonary Fibrosis and Forced Vital Capacity of =50 % of Predicted Value. Lung. 2016;194(5):739–743. doi: 10.1007/s00408-016-9912-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Komatsu M, Yamamoto H, Ichiyama T, Kawakami S, Uehara T, Yoshikawa Y. Tolerability of nintedanib in the elderly with idiopathic pulmonary fibrosis A single-center retrospective study. PLoS One. 2022;17(2):e0262795. doi: 10.1371/journal.pone.0262795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Sheth JS, Xia M, Murray S, Martinez CH, Meldrum CA, Belloli EA. Frailty and geriatric conditions in older patients with idiopathic pulmonary fibrosis. Respir Med. 2019;148:6–12. doi: 10.1016/j.rmed.2019.01.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Guler SA, Kwan JM, Leung JM, Khalil N, Wilcox PG, Ryerson CJ. Functional ageing in fibrotic interstitial lung disease the impact of frailty on adverse health outcomes [published correction appears in Eur Respir J. 2020 Mar 26;55(3):]. Eur Respir. 2020;55(1):1900647–1900647. doi: 10.1183/13993003.00647-2019. [DOI] [PubMed] [Google Scholar]
- 49.Cilli A, Uzer F, Sevinç C, Coşkun F, Ursavaş A, Öner Ş, et al. Tolerability and efficacy of second-line antifibrotics in patients with idiopathic pulmonary fibrosis. Pulm Pharmacol Ther. 2021;71:102099–102099. doi: 10.1016/j.pupt.2021.102099. [DOI] [PubMed] [Google Scholar]
- 50.Suzuki Y, Mori K, Aono Y, Kono M, Hasegawa H, Yokomura K. Switching antifibrotics in patients with idiopathic pulmonary fibrosis a multi-center retrospective cohort study. BMC Pulm Med. 2021;21(1):221–221. doi: 10.1186/s12890-021-01587-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Adams CJ, Shapera S, Ryerson CJ, Assayag D, Johannson KA, Fell CD. Effect of continued antifibrotic therapy after forced vital capacity decline in patients with idiopathic pulmonary fibrosis; a real world multicenter cohort study. Respir Med. 2022;191:106722–106722. doi: 10.1016/j.rmed.2021.106722. [DOI] [PubMed] [Google Scholar]
- 52.Kolonics-Farkas AM, Šterclová M, Mogulkoc N, Lewandowska K, Müller V, Hájková M, et al. Differences in Baseline Characteristics and Access to Treatment of Newly Diagnosed Patients With IPF in the EMPIRE Countries. Front Med (Lausanne) 2021;8:729203–729203. doi: 10.3389/fmed.2021.729203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Tran T, Šterclová M, Mogulkoc N, Lewandowska K, Müller V, Hájková M, et al. The European MultiPartner IPF registry (EMPIRE) validating long-term prognostic factors in idiopathic pulmonary fibrosis. Respir Res. 2020;21(1):11–11. doi: 10.1186/s12931-019-1271-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Kim HC, Lee S, Song JW. Impact of idiopathic pulmonary fibrosis on clinical outcomes of lung cancer patients. Sci Rep. 2021;11(1):8312–8312. doi: 10.1038/s41598-021-87747-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Lacedonia D, Correale M, Tricarico L, Scioscia G, Stornelli SR, Simone F. Survival of patients with idiopathic pulmonary fibrosis and pulmonary hypertension under therapy with nintedanib or pirfenidone. Intern Emerg Med. 2022;17(3):815–822. doi: 10.1007/s11739-021-02883-w. [DOI] [PubMed] [Google Scholar]
- 56.Waxman A, Restrepo-Jaramillo R, Thenappan T, Ravichandran A, Engel P, Bajwa A. Inhaled Treprostinil in Pulmonary Hypertension Due to Interstitial Lung Disease. N Engl J Med. 2021;384(4):325–334. doi: 10.1056/NEJMoa2008470. [DOI] [PubMed] [Google Scholar]
- 57.Clarson LE, Bajpai R, Whittle R, Belcher J, Abdul Sultan A, Kwok CS. Interstitial lung disease is a risk factor for ischaemic heart disease and myocardial infarction. Heart. 2020;106(12):916–922. doi: 10.1136/heartjnl-2019-315511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Adegunsoye A, Neborak JM, Zhu D, Cantrill B, Garcia N, Oldham JM. CPAP Adherence, Mortality, and Progression-Free Survival in Interstitial Lung Disease and OSA. Chest. 2020;158(4):1701–1712. doi: 10.1016/j.chest.2020.04.067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Tzouvelekis A, Karampitsakos T, Kourtidou S, Bouros E, Tzilas V, Katsaras M. Impact of Depression on Patients With Idiopathic Pulmonary Fibrosis. Front Med (Lausanne) 2020;7:29–29. doi: 10.3389/fmed.2020.00029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Zhao A, Gudmundsson E, Mogulkoc N, Jones MG, van Moorsel C, Corte TJ. Mortality in combined pulmonary fibrosis and emphysema patients is determined by the sum of pulmonary fibrosis and emphysema. ERJ Open Res. 2021;7(3):00316–02021. doi: 10.1183/23120541.00316-2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Marchioni A, Tonelli R, Ball L, Fantini R, Castaniere I, Cerri S. Acute exacerbation of idiopathic pulmonary fibrosis lessons learned from acute respiratory distress syndrome?. Crit. Care. 2018;22(1):80–80. doi: 10.1186/s13054-018-2002-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Yu X, Li X, Wang L, Liu R, Xie Y, Li S. Pulmonary Rehabilitation for Exercise Tolerance and Quality of Life in IPF Patients A Systematic Review and Meta-Analysis. Biomed Res Int. 2019;2019:8498603–8498603. doi: 10.1155/2019/8498603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Sullivan DR, Chan B, Lapidus JA, Ganzini L, Hansen L, Carney PA. Association of Early Palliative Care Use With Survival and Place of Death Among Patients With Advanced Lung Cancer Receiving Care in the Veterans Health Administration. JAMA Oncol. 2019;5(12):1702–1709. doi: 10.1001/jamaoncol.2019.3105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Baddini-Martinez J, Baldi BG, Costa CH, Jezler S, Lima MS, Rufino R. Update on diagnosis and treatment of idiopathic pulmonary fibrosis. J Bras Pneumol. 2015;41(5):454–466. doi: 10.1590/S1806-37132015000000152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Visca D, Mori L, Tsipouri V, Fleming S, Firouzi A, Bonini M. Effect of ambulatory oxygen on quality of life for patients with fibrotic lung disease (AmbOx) a prospective, open-label, mixed-method, crossover randomised controlled trial. Lancet Respir Med. 2018;6(10):759–770. doi: 10.1016/S2213-2600(18)30289-3. [DOI] [PubMed] [Google Scholar]
- 66.Higginson IJ, Bausewein C, Reilly CC, Gao W, Gysels M, Dzingina M. An integrated palliative and respiratory care service for patients with advanced disease and refractory breathlessness a randomised controlled trial. Lancet Respir Med. 2014;2(12):979–987. doi: 10.1016/S2213-2600(14)70226-7. [DOI] [PubMed] [Google Scholar]
- 67.Richeldi L, Fernández Pérez ER, Costabel U, Albera C, Lederer DJ, Flaherty KR. Pamrevlumab, an anti-connective tissue growth factor therapy, for idiopathic pulmonary fibrosis (PRAISE) a phase 2, randomised, double-blind, placebo-controlled trial. Lancet Respir Med. 2020;8(1):25–33. doi: 10.1016/S2213-2600(19)30262-0. [DOI] [PubMed] [Google Scholar]
- 68.Raghu G, van den Blink B, Hamblin MJ, Brown AW, Golden JA, Ho LA, et al. Long-term treatment with recombinant human pentraxin 2 protein in patients with idiopathic pulmonary fibrosis an open-label extension study. Lancet Respir Med. 2019;7(8):657–664. doi: 10.1016/S2213-2600(19)30172-9. [DOI] [PubMed] [Google Scholar]
- 69.ClinicalTrials.gov [homepage on the Internet] A Study to Evaluate Long Term Safety and Efficacy of Recombinant Human Pentraxin-2 (rhPTX-2; PRM-151) in Participants With Idiopathic Pulmonary Fibrosis (STARSCAPE-OLE) Bethesda: National Institutes of Health; https://www.clinicaltrials.gov/ct2/show/NCT04594707 [Google Scholar]
- 70.Richeldi L, Azuma A, Cottin V, Hesslinger C, Stowasser S, Valenzuela C. Trial of a Preferential Phosphodiesterase 4B Inhibitor for Idiopathic Pulmonary Fibrosis. N Engl J Med. 2022;386(23):2178–2187. doi: 10.1056/NEJMoa2201737. [DOI] [PubMed] [Google Scholar]
- 71.Wu AC, Kiley JP, Noel PJ, Amur S, Burchard EG, Clancy JP. Current Status and Future Opportunities in Lung Precision Medicine Research with a Focus on Biomarkers An American Thoracic Society/National Heart, Lung, and Blood Institute Research Statement. Am J Respir Crit Care Med. 2018;198(12):e116–e136. doi: 10.1164/rccm.201810-1895ST. [DOI] [PMC free article] [PubMed] [Google Scholar]