

The final repair with a hemi-Commando aortic root enlargement and redo Bentall procedure.
Central Message.
A patient with 3 previous cardiac surgeries and recent Bentall procedure required reoperation with hemi-Commando root enlargement showing feasibility of this procedure even in redo aortic root surgery.
One challenging scenario in surgical aortic valve (AV) replacement is the small aortic root. A small aortic root limits the size of prosthetic valve that may be implanted and increases the risk of patient–prosthesis mismatch.1,2 Several valve options exist with larger effective orifice area or improved flow characteristics compared with a standard, stented, bioprosthetic valve, including supraannular, stentless, or mechanical valves.1,3 When these options are not suitable, an aortic root enlargement (ARE) allows for the implantation of a larger valve.
Whereas ARE techniques are widely utilized, an extensive ARE in the context of a previous Bentall procedure has not been described to the authors’ knowledge. Herein, we describe the case of a patient with a complex past surgical history presenting with recurrent aortic aneurysm requiring repeat surgical intervention and ARE.
Case Report
The patient provided written informed consent to publish their case; institutional review board approval was not required.
Past Medical History
A 49-year-old man with a complex past cardiac surgical history, including AV repair at age 10 years, homograft aortic root replacement at age 16 years, and modified bio-Bentall procedure at age 41 years.
Preoperative Investigations
Preoperative echocardiogram demonstrated moderate-severe aortic regurgitation (Figure 1). There were no other significant abnormalities. Preoperative angiogram identified no obstructive coronary disease.
Figure 1.

Preoperative transesophageal echocardiogram demonstrating severe aortic insufficiency (1) and trace mitral regurgitation (2), postoperative transesophageal echocardiogram showing mild mitral regurgitation (3), and the explanted aortic valve prosthesis with the noncoronary sinus leaflet partially detached at both posts (4).
Operative Details
Left axillary cannulation was performed, given previous right axillary cannulation, and repeat sternotomy was completed. The diaphragmatic surface of the heart, aorta, and superior vena cava were mobilized. Cardiopulmonary bypass was established.
An aortotomy was performed. On inspection of the aortic prosthesis, the noncoronary sinus leaflet was partially detached at both posts (Figure 1). The previously placed aortic root was explanted.
The aortic annulus would not accommodate a 21-mm valve sizer, so a Nick's ARE was performed. A 21-mm sizer would still not pass. It was clear that an extensive ARE would be required.
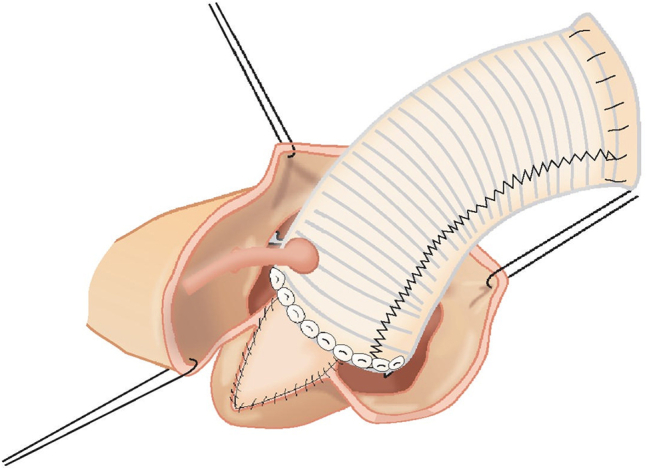
The previous root enlargement incision was extended onto the anterior leaflet of the mitral valve 7 mm from the free margin and extended through the dome of the left atrium. In a hemi-Commando fashion a piece of prepared bovine pericardium (20 mm maximal width) was placed (Figure 2).
Figure 2.

The steps of the case, including excision of the previous graft and valve (1-3), aortic root enlargement in a hemi-Commando fashion (4, 5), and replacement of the aortic valve and ascending aorta (6).
Sixteen pledgeted valve sutures were placed through the aortic annulus and pericardial patch, and through a 23-mm On-X valve conduit (On-X Life Technologies, Inc). The valve was secured using the Cor-Knot system (LSI Solutions).
The coronary buttons and distal anastomoses were performed. The patient was decannulated, hemostasis was achieved, and the chest was closed in standard fashion.
Follow-up
The patient developed third-degree heart block requiring permanent pacemaker on postoperative day 9 and was discharged on postoperative day 11 without further complication.
Discussion
The long-term surgical management of young patients with AV disease is of significant importance. Consideration of the long-term outcomes and required reoperations are crucial.4 As highlighted by this case, AV surgery at a young age carries significant risk of reoperation. The patient described required 4 AV surgeries to date, the most recent of which was complicated by restrictive aortic annular size.
Although AREs are commonly performed and have been demonstrated to be safe,1,2 the inability to accommodate an appropriately sized valve in a patient with a previous Bentall surgery is rarely encountered. In this case, a standard Nick's ARE did not provide sufficient expansion of the aortic root and so the incision was extended in a hemi-Commando ARE fashion to achieve adequate enlargement of the aortic root. Various root enlargement techniques have been described with varying degrees of enlargement of the aortic root. These include a Nick's ARE with an incision made in the noncoronary sinus, Nunez root enlargement, which is performed through the left noncommissure, Manougian ARE which is similar to a Nunez ARE but is extended onto the anterior leaflet of the mitral valve and allows for further upsizing, the Konno-Rastan ARE is performed from the right coronary sinus ending in the interventricular septum, and finally the Commando procedure is performed through an incision through the noncoronary sinus into the aortic root, through the anterior leaflet mitral valve, and onto the dome of the left atrium with patch reconstruction of the aorto-mitral curtain.3,5 The various ARE techniques allow for the selection of the optimal root enlargement based on the patient's anatomy and required valve size.3,5
Conclusions
This case highlights the importance of preoperative planning, both at the time of initial operation of the AV and for any subsequent interventions. A hemi-Commando ARE is feasible in a patient with a previous Bentall procedure and small aortic root requiring aortic valve replacement, and should be considered even in patients with prior aortic root surgery if prosthetic valve sizing is not adequate to prevent patient–prosthesis mismatch.
Footnotes
Disclosures: The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
IRB Number: N/A.
Informed Consent Statement: The patient provided written informed consent to publish their case.
References
- 1.Coutinho G.F., Correia P.M., Paupério G., de Oliveira F., Antunes M.J. Aortic root enlargement does not increase the surgical risk and short-term patient outcome? Eur J Cardio Thorac Surg. 2011;40:441–447. doi: 10.1016/j.ejcts.2010.11.064. [DOI] [PubMed] [Google Scholar]
- 2.Yu W., Tam D.Y., Rocha R.V., Makhdoum A., Ouzounian M., Fremes S.E. Aortic root enlargement is safe and reduces the incidence of patient-prosthesis mismatch: a meta-analysis of early and late outcomes. Can J Cardiol. 2019;35:782–790. doi: 10.1016/j.cjca.2019.02.004. [DOI] [PubMed] [Google Scholar]
- 3.Sankalp S., Yadav M., Kunwar S.S., Gupta A. Analysis of various techniques of aortic root enlargement. Asian Cardiovasc Thorac Ann. 2021;29:565–573. doi: 10.1177/0218492320988457. [DOI] [PubMed] [Google Scholar]
- 4.Deng J., Zhong Q. Clinical analysis of redo aortic root replacement after cardiac surgery. Int J Med Sci Clin Invent. 2021;8:5421–5427. doi: 10.1186/s13019-021-01587-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Massias S.A., Pittams A., Mohamed M., Ahmed S., Younas H., Harky A. Aortic root enlargement: when and how. J Card Surg. 2021;36:229–235. doi: 10.1111/jocs.15175. [DOI] [PubMed] [Google Scholar]