

Abstract
Overweight and obesity is a multifactorial, multisystem disease declared a global epidemic by the World Health Organization (WHO) as early as in 1997. At least 30% of the working-age population in Russia is overweight. Only the use of physical activity as an integral (basic) part of obesity treatment and maintenance of the body weight achieved in the course of treatment can achieve durable and long-lasting treatment results as well as significant changes in the body structure (fat/non-fat body weight ratio). Terrainkur (therapeutic walking) is a method of spa treatment that combines climatotherapy and physical therapy. One of the problems in physical activity in obese people is the difficulty they experience in exercising due to the impaired walking pattern caused by imbalances in the muscle chains, including pelvic region, cervical region, which reduces endurance and commitment to physical activity. The study found that the exposure group (Terrainkur) showed lower values of "total fat", "metabolic age", "basic caloric value" compared to initial results and the control group; the exposure group (Terrainkur) showed a decrease in the deviation of the centre of body axis projection from the proper axis, the percentage of non-compliance with the proper fluctuations of the foot underextension. These changes contributed to the elimination of terrainkur restrictions and, as a result, improved the patient compliance during the terrainkur exercises.
Key Words: overweight, сlimatotherapy, obesity, therapeutic walking
Ethical Publication Statement
We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Overweight is a multifactorial, multisystem disease, and the World Health Organization (WHO) declared obesity and overweight, a global epidemic as early as in 1997:1,2 "overweight and obesity are now so prevalent that they affect public health more than traditional health problems such as starvation and infectious diseases". In Russia, at least 30% of the Russian working-age population is overweight, with 25% of them obese,3 In EU countries, the direct monetary cost of obesity represents about 7% of all healthcare spendings, "which is comparable to that for some diseases, such as cancer.4
Only a combination of physical activity and diet therapy can achieve sustainable results, positively impacting on the psychogenic component of obesity.5 Terrainkur (therapeutic walking) is an effective method of losing weight.6 Walking improves coordination, balance and general mobility by strengthening the main muscle groups, increases overall performance, regulates the central nervous system,7,8 helps to restore a normal walking pattern and stabilizes the pelvic and cervical regions. Terrainkur training in sanatorium and spa conditions can be the first step towards a change in lifestyle and is an excellent motivator for patients.9 Outdoor physical activities are the most effective,10 with a wide range of weather and landscape-climatic factors: insolation that activates metabolism, wind loads that activate blood circulation in the subcutaneous tissue and stimulate thermogenesis, marine aerosols that increase gas exchange in the lungs and blood oxygenation.11
Materials and Methods
Between July and November 2021 a comparative clinical study was conducted in Medical and rehabilitation clinical centre "Yudino" in two parallel groups (group 1 - "control", group 2 - "gentle terrainkur") in which 36 healthy volunteers (14 men and 22 women, 61.1 % and 38.9 % respectively) were recruited.
Fig 1.
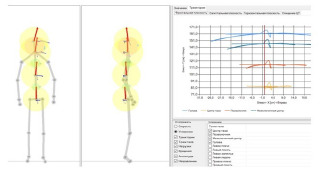
Schematic representation of measurement points, the size and deviation of the main directions (vectors) of movement (on the left), the trajectory of movement of the main body parts (on the right) [https://habilect.com/hmotionlab].
All the subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of National Medical Research Center (Project identification code # GZ 4, protocol # 4, 15 April 2021). The median age was 60.0 years and the range was 53.0 – 64.0. The median mean weight of the volunteers was 105.1 kg (86.9; 117.9 [UQ, LQ]). All the volunteers were overweight and some had a history of grade I-II arterial hypertension (corrected, at the time of the study) or other cardiovascular and/or endocrine risk factors, but all were on stable pharmacologic treatments. After obtaining prior consent to participate in the study from volunteers wich signed an informed consent form, the volunteers were divided into 2 groups - the exposure group (terrainkur) and the control group (daily physical activity). The exposure group included - 14 participants, the control group - 22 participants. The therapy consisted of a terrainkur course (7-10 sessions) using a constructed course of 1400 meters with an incline of no more than 12° every day at the same time for 30-40 minutes, 6 days a week except Sunday, in the afternoon from noon to 4:00 pm. The training was conducted at a pace which ensured medium-intensity exercise. The exercise intensity was calculated according to the formula 220 minus the age (in people without any cardiovascular diseases). A moderate-intensity exertion would correspond to 55-70% of the maximum heart rate.12 Exercise was performed no earlier than 2 hours after meals and volunteers were required to follow a drinking regime. Indications for stopping exercise included: overcoming the target distance or experiencing shortness of breath and discomfort in the upper torso (chest, neck, shoulder), an increased heart rate, and heaviness in the head. If nausea, dizziness, extreme fatigue, or insomnia occurred during or after exercise, the volunteer reduced the intensity of the next exercise session. Before and after the training course (terrainkur) - in the exposure group group, on day 1 and on day 8-11 - in the control group, the following tests were carried out: body composition using bioimpedance measurement (TANITA BC-1000 bio-analyzer, Japan), stabilometry examination (Habilect complex, Russia). Stabilometric examination was performed on Habilect complex. (РУ No. РЗН 2016/5213) that is a multifunctional medical system based on the Microsoft Kinect high-precision non-contact sensor. A camera (sensor) pointed at the patient, without the installation of additional sensors on the body, distinguishes 25 major points of the human body. Habilect records and analyses the movement of each such points (Figure 1). We used also the H.VrS (Virtual Balance Platform) system module, a virtual stability platform module, in our data analysis. With H.VrS it is possible to analyze the patient's gait changes, the trajectory of the centre of mass in the horizontal, vertical and sagittal planes.13,14 To perform the study, patients stood in a predetermined area on the floor and performed the "Walking in Place" test exercise. The test time was 30 seconds. To interpret the results of the study the following parameters were determined: X - coordinates of the position of the pressure centre in the frontal plane (anteroposterior) (mm); Y - coordinates of the position of the pressure centre in the horizontal plane (upper-lower) (mm); Z - coordinates of the position of the pressure centre in the sagittal plane (right-left) (mm); L - path length of the statokinesiogram (mm); V - speed of the statokinesiogram (mm/s). A total of 72 statokinesiograms were recorded and analyzed, while examining the patients before terrainkur and after. In addition to physical examination methods, a bioimpedance method was used for a non-invasive analysis of the patient's metabolism, which reflects quantitative and qualitative body composition (TANITA BC-1000 body composition monitor, Japan) and allows to estimate: body fat and water percentage (%), muscle mass (%), physical constitution (in points); basic metabolism (kcal), metabolic age (years), bone mass (kg), visceral fat level (points).
Fig 2.
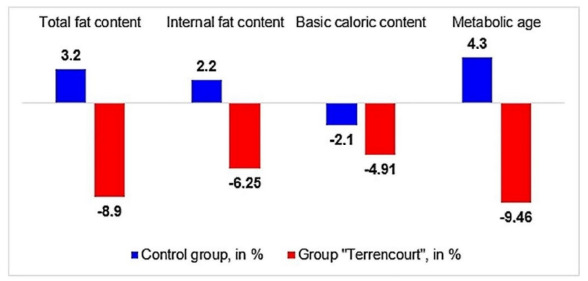
Evolution from the initial range of indicators (total and internal fat content, baseline calorie intake, metabolic age) in the control and intervention groups (Terrainkur).
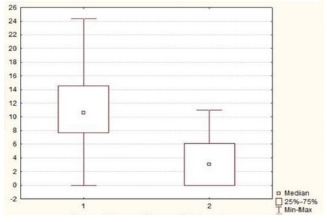
Fig 3.
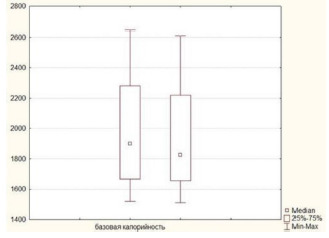
Comparison of the "baseline caloric value" in the intervention group before (1) and after the study (2), kcal.
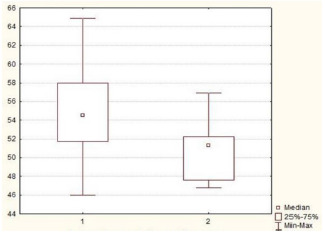
Fig 4.
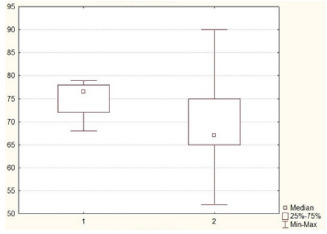
Comparison of the "metabolic age" indicator in the control group (1) and the intervention group (2), years.
Statistical processing of clinical data was performed using descriptive statistics, and taking into account small sample size and non-normal distribution, nonparametric methods were also used to test null hypothesis: χ2 criterion, the Mann-Whitney U test, Wilcoxon test.15 All obtained results were processed using Statistica for Windows, v. 8.0 (StatSoft Inc., USA) и Microsoft Excel (Microsoft, USA). The significance of differences was considered to be established at p<0.05.
Results
The terrainkur course achieved the following positive effects: reduction in total and internal fat, baseline caloric value and metabolic age (Figure 2). During bioimpedance measurement, the "baseline caloric value" value decreased significantly in the intervention group, at the end of the study (T – 4, 0; p<0.05) (Figure 3). The "metabolic age" indicator, in the group of patients over 60 years old, decreased significantly in the intervention group (U – 12,0; p<0.05) (Figure 4). The results of the stabilometry study are presented in Table 1 and Table 2. As can be seen from the tables, the indices of deviations along the main body axes of the head point and centre of mass of the body, as well as the direction of body motion vector after the terrainkur exercises decreased, which was subjectively noted as the disappearance of unsteadiness when walking. When calculating the increase in deviation (deviation of the main body axes from the initial value) using the Wilcoxon signed-rank test, statistically significant deviations of the body on the X axis (increase 300.5%, p=0.05), Y axis (increase 102.45%, p=0.02) were found. When calculating the increase in head axis deviation from the initial value using the Wilcoxon signed-rank test, statistically significant deviations were found in the X-axis (160.04% increase, p=0.02), Y-axis (83.7% increase, p=0.01). In addition, there was a significant decrease in displacement of the centre point in the Terrainkur group compared to the control group (U – 24.0; p=0.008) (Figure 5). There was a significant decrease in the percentage of non-compliance with the appropriate “Leg underextension” values in the “Terrainkur” group, compared with the control group (U – 29.0; p=0.02) (Figure 6).
Table 1.
Stabilometry results for the central body axes before and after the intervention.
| Parameter / Body axis | Body axis X, cm | Body axis Y, cm | |
|---|---|---|---|
| Before terrainkur | Median (Me) | 3.2 | -28.01 |
| Q25 | -90 | -28.01 | |
| Q75 | 90.5 | 14.76 | |
| After | Median (Me) | -8.96 | -29.59 |
| terrainkur | Q25 | -99.2 | -30.5 |
| Q75 | -80.6 | 30.09 | |
| % deviations from | the Median (Me) | 300.5%* | 102.45% |
| original value | Q25 | 100.98%* | 103.45% |
| Q75 | 85.28%* | 220. 95% |
* The data are presented as median and quartiles (Q25; Q75), analysis of differences was performed using the Wilcoxon signed-rank test (critical significance level of the criterion p<0.05).
Table 2.
Stabilometry results for the central axes of the head points before and after the intervention.
| Parameter / Body axis | Body axis X, cm | Body axis Y, cm | |
|---|---|---|---|
| Before terrainkur | Median (Me) | -0.82 | 120.33 |
| Q25 | -1.2 | 60.13 | |
| Q75 | -0.9 | 120.94 | |
| After | Median (Me) | 1.4 | 105.42 |
| terrainkur | Q25 | -10.0 | 50.49 |
| Q75 | 2.2 | 105.42 | |
| % deviations from | the Median (Me) | 160.04 %* | 83.7 %* |
| original value | Q25 | 821.77 %* | 83.7 %* |
| Q75 | 258.70 %* | 80.1 %* |
* The data are presented as median and quartiles (Q25; Q75). analysis of differences was performed using the Wilcoxon signed-rank test (critical significance level of the criterion p<0.05).
Discussion
Restoration of the physiological walking pattern and stabilization of the pelvic region require less resource input from the central nervous system, which manifests itself in a greater tolerance to physical exertion and, as a result, an increased compliance of patients when exercising terrainkur. The stabilometric study showed a decrease in the amplitude of body axis deviations in all 3 planes, indicating an improvement in all brain areas responsible for coordination of motor functions and their vegetative support, improved functional interaction within muscular chains. Improvement of the muscular chains of the upper half of the body consisted in normalisation of the spiral body chain, including the sternocleidomastoid muscle, which plays a major role in maintaining the "vertical" axis of the body, reduction of hypertonicity of the of the scalene muscles of the upper part of the trapezius muscle. Reducing the hypertonicity of these muscles reduces the hyperlordosis of the cervical spine. Consequently, it reduced the curvature of the vertebral arteries, which play an important role in blood supply to the brain. Hypertonicity of the scalene muscles and the upper part of the trapezium often leads to compression of the posterior scapular nerve and brachial plexus nerves, which can lead to hypofunction of the scapular muscles, which largely determine the support of the "upright body axis". Reducing the involvement of the head and neck muscles in compensatory balancing during walking and maintaining an upright body posture mainly at the expense of the lower limbs and pelvis muscles helps prevent arterial and venous circulatory disorders in the head and neck area and makes training not only more effective but safer as well. The increase in the angle of the bridge of the foot shown in Figure 6 indicates a change in the walking pattern, characterized by increased functional activity of the large gluteal muscles, quadriceps and lower leg muscles. This walking pattern ensures the involvement of the large muscles of the lower limbs, which improves venous blood flow, lymph flow, and accelerates metabolism in the large muscles.16,17 The decrease in the amplitude of movement in the pelvic and thoracic regions (Figure 5), suggests the recovery of the pelvic stabiliser muscles, pelvic diaphragm and abdominal muscles. Improvement of the work of these muscles contributes to the restoration of normal internal organ displacement trajectories during breathing and walking, which improves blood flow, lymph flow and metabolism in the visceral fat depot.
Fig 5.
Displacement parameters of the centre point in the control (1) and intervention (2) groups, %.
Fig 6.
The percentage of non-compliance with the appropriate “Leg underextension” values in the control (1) and intervention (2) groups, %.
In conclusion, we foud that: i) the patients in the intervention group ("Terrainkur") showed lower values of "total fat", "metabolic age", "baseline caloric value" compared with the initial results and the control group, indicating the positive effect of terrainkur on fat metabolism in patients with excessive body weight and obesity; ii) the patients in the intervention group ("Terrainkur") showed a decrease in the deviation of the centre of body axis projection from the proper axis, the percentage of non-compliance with the proper fluctuations of the foot underextension, indicating the restoration of the normal walking pattern and stabilization of the pelvic and cervical regions. These changes contributed to improvement of venous blood flow by terrainkur exercises.
Acknowledgments
The authors are grateful to the partecipants for their kind cooperation.
List of acronyms
- EU
European Union
- H.Vrs
Virtual Balance Platform
- Terrainkur
therapeutic walking
- WHO
World Health Organization
Funding Statement
Funding None.
Contributor Information
Anatoliy D. Fesyun, Email: fad68@yandex.ru.
Irina A. Grishechkina, Email: GrishechkinaIA@nmicrk.ru.
Andrey A. Lobanov, Email: alobanov89@gmail.com.
Sergei V. Andronov, Email: sergius198010@mail.ru.
Andrey I. Popov, Email: PopovAI@nmicrk.ru.
Michail A. Eremushkin, Email: medmassage@mail.ru.
Rinat R. Bogdanov, Email: rinatbo@rambler.ru.
Natalia P. Sanina, Email: nataliasanina2@yandex.ru.
Igor V. Reverchuk, Email: bios@reverchuk.com.
References
- 1.Guénard F, Houde A, Bouchard L, Tchernof A, Deshaies Y, Biron S, Lescelleur O, Biertho L, Marceau S, Pérusse L, Vohl MC. Association of LIPA gene polymorphisms with obesity-related metabolic complications among severely obese patients. Obesity (Silver Spring). 2012. Oct;20(10):2075-82. doi: 10.1038/oby.2012.52. Epub 2012 Mar 7. PMID: 22395809. [DOI] [PubMed] [Google Scholar]
- 2.WHO. Media centre. Obesity and overweight. Fact sheet: N°311, January 2015. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 11 Nov 2021) [Google Scholar]
- 3.Mel'nichenko GA. Romantsova TI Ozhirenie: epidemiologiya, klassifikatsiya, patogenez, klinicheskaya simptomatika i diagnostika [Obesity: epidemiology, classification, pathogenesis, clinical symptoms and diagnosis]. MIA, 2004. Russian. [Google Scholar]
- 4.Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i-xii, 1-253. PMID: 11234459. [PubMed] [Google Scholar]
- 5.Wimalawansa SJ. Controlling Obesity and Its Complications by Elimination of Causes and Adopting Healthy Habits: «Cause-Driven» Approach. Advances in Medical Sciences. 2014; 3(1): 1-15. Russian. [Google Scholar]
- 6.Salimgareeva IA, Ahmadullin RV, Gil'mutdinova LT, Gabdullin NT. Dietoterapiya ozhireniya v usloviyah sanatoriya [Diet therapy of obesity in a sanatorium]. Actual problems of restorative medicine, balneology and physiotherapy. Proceedings of the International Congress. "All-Russian forum "Zdravnitsa 2003". Moscow, Russian Federation. 2003: 172. Russian [Google Scholar]
- 7.Platonov VN. Sohranenie i ukreplenie zdorov'ya lyudej – prioritetnoe napravlenie sovremennogo zdravoohraneniya [Preservation and strengthening of people's health is a priority direction of modern health care]. Sportivnaya medicina. 2006; 2: 3–14. Russian. [Google Scholar]
- 8.Barieva YuB, Botvineva LA, Kajsinova AS, Samsonova NA. Rol' fizicheskih nagruzok i pit'evyh mineral'nyh vod v profilaktike i lechenii abdominal'nogo ozhireniya - osnovy metabolicheskogo sindroma [The role of physical activity and drinking mineral water in the prevention and treatment of abdominal obesity - the basis of the metabolic syndrome]. Fizioterapiya, bal'neologiya i reabilitaciya. 2017; 16(5): 228-233. Russian. [Google Scholar]
- 9.Khorkina NA, Filippova AV. Physical activity of elderly people as a public policy object. Voprosy gosudarstvennogo i munitsipal’nogo upravleniya. 2015; 2: 197-222. Russian. [Google Scholar]
- 10.American College of Cardiology/American Heart Association Task Force on Practice Guidelines Obesity Expert Panel, 2013. Expert Panel Report: Guidelines (2013) for the management of overweight and obesity in adults. Obesity (Silver Spring). 2014. Jul;22 Suppl 2:S41-410. doi: 10.1002/oby.20660. PMID: 24227637. [Google Scholar]
- 11.Sallis JF, Floyd MF, Rodríguez DA, Saelens BE. Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation. 2012. Feb 7;125(5):729-37. doi: 10.1161/CIRCULATIONAHA.110.969022. PMID: 22311885; PMCID: PMC3315587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner VA, Coke LA, Fleg JL, Forman DE, Gerber TC, Gulati M, Madan K, Rhodes J, Thompson PD, Williams MA; American Heart Association Exercise Cardiac Rehabilitation Prevention Committee of the Council on Clinical Cardiology, Council on Nutrition, Physical Activity and Metabolism, Council on Cardiovascular and Stroke Nursing, and Council on Epidemiology and Prevention. Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation. 2013. Aug 20;128(8):873-934. doi: 10.1161/CIR.0b013e31829b5b44. Epub 2013 Jul 22. PMID: 23877260. [DOI] [PubMed] [Google Scholar]
- 13.Ivanova GE, Isakova EV, Krivoshej IV, Kotov SV, Kubryak OV. Formirovanie konsensusa specialistov v primenenii stabilometrii i bioupravleniya po opornoj reakcii [Formation of a consensus of specialists in the application of stabilometry and biofeedback on the support reaction]. Vestnik vosstanovitel'noj mediciny. 2019; 89(1):16–21. Russian. [Google Scholar]
- 14.Guffanti D, Brunete A, Hernando M, Rueda J, Navarro Cabello E. The Accuracy of the Microsoft Kinect V2 Sensor for Human Gait Analysis. A Different Approach for Comparison with the Ground Truth. Sensors (Basel). 2020. Aug 7;20(16):4405. doi: 10.3390/s20164405. PMID: 32784586; PMCID: PMC7472493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Petrie A, Sabin C. Medical Statistics at a Glance, 4th ed. Wiley-Blackwell, 2019. [Google Scholar]
- 16.Ivanova EP, Lobanov AA, Andronov SV, Fesyun AD, Rachin AP, Barashkov GN, Bogdanova EN, Grishechkina IA, Popov AI, Lebedeva OD, Yakovlev MYu, Sidorov VV. Fresh Water Aquatic Training in Patients with Upright Posture Maintaining Disorders. Bulletin of Rehabilitation Medicine. 2021; 20(6): 58-66. doi: 10.38025/2078-1962-2021-20-6-58-66. [Google Scholar]
- 17.Lobanov AA, Irina A Grishechkina, Andronov SV, Gleb N Barashkov, Andrey I Popov, Anatoliy D Fesyun, Elena P Ivanova, Maccarone MC, Stefano Masiero. Can aquatic exercises contribute to the improvement of the gait stereotype function in patients with Long COVID outcomes? Eur J Transl Myol. 2022. Jul 14;32(3):10698. doi: 10.4081/ejtm.2022.10698. PMID: 35833897; PMCID: PMC9580543. [DOI] [PMC free article] [PubMed] [Google Scholar]