

Abstract
Background
Demographic data in North America, Europe, Asia, Australia and New Zealand suggest a rapid growth in the number of persons over the age of 65 years as the baby boomer generation passes retirement age. As older adults make up an increasing proportion of the population, they are an important consideration when designing future evidence‐based traffic safety policies, particularly those that lead to restrictions or cessation of driving. Research has shown that cessation of driving among older drivers can lead to negative emotional consequences such as depression and loss of independence. Older adults who continue to drive tend to do so less frequently than other demographic groups and are more likely to be involved in a road traffic crash, possibly due to what is termed the "low mileage bias". Available research suggests that older driver crash risk estimates based on traditional exposure measures are prone to bias. When annual driving distances are taken in to consideration, older drivers with low driving distances have an increased crash risk, while those with average or high driving distances tend to be safer drivers when compared to other age groups. In addition, older drivers with lower distance driving tend to drive in urban areas which, due to more complex and demanding traffic patterns, tend to be more accident‐prone. Failure to control for actual annual driving distances and driving locations among older drivers is referred to as "low mileage bias" in older driver mobility research. It is also important to note that older drivers are more vulnerable to serious injury and death in the event of a traffic crash due to changes in physiology associated with normal ageing. Vision, cognition, and motor functions or skills (e.g., strength, co‐ordination, and flexibility) are three key domains required for safe driving. To drive safely, an individual needs to be able to see road signs, road side objects, traffic lights, roadway markings, other vulnerable road users, and other vehicles on the road, among many other cues—all while moving, and under varying light and weather conditions. It is equally important that drivers must have appropriate peripheral vision to monitor objects and movement to identify possible threats in the driving environment. It is, therefore, not surprising that there is agreement among researchers that vision plays a significant role in driving performance. Several age‐related processes/conditions impair vision, thus it follows that vision testing of older drivers is an important road safety issue. The components of visual function essential for driving are acuity, static acuity, dynamic acuity, visual fields, visual attention, depth perception, and contrast sensitivity. These indices are typically not fully assessed by licensing agencies. Also, current vision screening regulations and cut‐off values required to pass a licensing test vary from country to country. Although there is a clear need to develop evidence‐based and validated tools for vision screening for driving, the effectiveness of existing vision screening tools remains unclear. This represents an important and highly warranted initiative to increase road safety worldwide.
Objectives
To assess the effects of vision screening interventions for older drivers to prevent road traffic injuries and fatalities.
Search methods
For the update of this review we searched the Cochrane Injuries Group's Specialised Register, the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library), MEDLINE (OvidSP), Embase (OvidSP), PsycINFO (OvidSP) and ISI Web of Science: (CPCI‐S & SSCI). The searches were conducted up to 26 September 2013.
Selection criteria
Randomised controlled trials (RCTs) and controlled before and after studies comparing vision screening to non‐screening of drivers aged 55 years and older, and which assessed the effect on road traffic crashes, injuries, fatalities and any involvement in traffic law violations.
Data collection and analysis
Two review authors independently screened the reference lists for eligible articles and independently assessed the articles for inclusion against the criteria. If suitable trials had been available, two review authors would have independently extracted data using a standardised extraction form.
Main results
No studies were found that met the inclusion criteria for this review.
Authors' conclusions
Most countries require a vision screening test for the renewal of an individual's driver's licence. There is, however, lack of methodologically sound studies to assess the effects of vision screening tests on subsequent motor vehicle crash reduction. There is a need to develop valid and reliable tools of vision screening that can predict driving performance.
Keywords: Aged; Humans; Automobile Driving; Vision Screening; Accidents, Traffic; Accidents, Traffic/prevention & control
Plain language summary
Vision screening of older drivers to prevent road traffic injuries and deaths
Good vision is critical for safe driving performance. Because vision declines with age, and the percentage of older adults in the population is increasing, it has become more important to consider the vision screening requirements for older adults when designing evidence‐based traffic safety policy. Mandatory vision screening for the issue or renewal of a driver's licence helps to ensure that older drivers are fit to safely operate vehicles.To date, there has been no trial to demonstrate the impact of vision screening on the prevention of older driver‐related crashes. However, given the importance of good vision for safe driving, vision testing remains a relevant issue for all licensed drivers.
Background
In the early 1990s, the "Global Burden of Disease Study" predicted that traffic‐related injuries would become the third largest contributor to global death and disability by the year 2020 (Murray 1996). Treatment of people with injuries from road traffic crashes has a substantial impact on the healthcare system and wider society. In low‐ and middle‐income countries, between 30% and 85% of trauma hospital admissions are road crash victims. According to a survey completed by the Transport Research Laboratory (TRL), between 40% and 75% of the motor vehicle crash victims in developing countries were the principal earners in a family group (Silcock 1997). This has a direct impact on the gross national product (GNP), to the extent that injuries due to crashes cost low‐ and middle‐income countries between 1% and 2% of their GNP; more than the total development aid received by these countries (Murray 1996; WHO 2005).
The number of older drivers has and will continue to increase dramatically as populations worldwide continue to age. In the next three decades it is expected that there will be a huge increase in both the number of older people and the proportion of the population that they represent in almost all European countries as well as North America, Asia and Australia (Rosenbloom 2001). Data from the USA, Australia, Germany, New Zealand, Norway, and the United Kingdom demonstrate that, in spite of cultural and policy differences, older people today are more likely to have a driver's licence and will take more trips than a comparable group 10 years ago (Rosenbloom 2001).
People over the age of 65 years have more fatal crashes per mile driven than any other demographic group, except teenage males (NCIPC 2002). Available research shows that fragility and frailty are commonly associated with old age. Fragility refers to increasing inability to withstand disease or injury. Frailty describes the ability to recover from a disease or injury (Kent 2009). Due to the fragility of older persons, crashes more often translate to severe injuries and fatalities (Li 2003).
Earlier research maintained that older drivers do not have a higher risk per capita or per driver's licence, but their increased crash proneness is reflected in higher crash rates per driven distance (Hakamies Blomqvist 2005). It has been argued that older drivers, a group that drive small annual distances, have a higher crash risk per kilometre than other population groups with larger annual driving distances. Available research also suggests that older drivers' crash risk based on traditional exposure measures are prone to bias (Hakamies Blomqvist 2005; Janke 2001). Recent studies also confirm that self‐estimates of driving mileage on which these estimates depend are often inaccurate (Rizzo 2011). In general, failure to control older drivers actual annual driving distances and the actual driving locations are referred in the older driver mobility research as the "low mileage bias" (Janke 2001). Finnish, French, and Dutch motor vehicle crash data have shown, when compared across age groups, that older drivers had higher crash rates per distance driven. However, the age effect disappeared when the comparison was made in groups matched for yearly driving distance (Fontaine 2003; Hakamies Blomqvist 2002; Langford 2006). Recently, this effect was termed the "low mileage bias". This bias has been empirically demonstrated and shows that increased crash rates are due to driving exposure rather than age.
Description of the condition
As most individuals age, they experience some level of functional decline in sensory, physical, and cognitive function (OECD 2001). Age‐related changes in vision make it more difficult for older drivers to adapt to low light conditions, recognise road and road side objects under low lighting conditions and recover from glare. It has been suggested that the deterioration in vision that results from the normal aging process, as well as from eye disease, is likely to be a major contributing factor to the increased crash rates of older people (Wood 2001).
Vision is the most important source of information during driving and many driving‐related injuries have been associated with visual problems (Johnson 2010; Owsley 2010). Therefore, visual assessment for driving is paramount to the reduction of crash‐related injuries. Vision, cognition and motor functions are the three key functions required for safe driving (Desapriya 2008). Visual and cognitive tasks that are involved in driving include selective and divided attention and cognition. Researchers also believe that colour vision and glare sensitivity are important in driving. In addition, research has indicated that poor depth perception and peripheral vision are also associated with poor driving performance (Javitt 2002; Shope 1998; West 2003). Poor depth perception and peripheral vision affect ability to judge distance and speed. Further, studies have shown that many eye diseases affect vision and driving, for example cataract, macular degeneration, diabetic retinopathy, glaucoma, retinitis pigmentosa, corneal scarring, and eye movement disorders (Fishman 1981; Gutierrez 1997; Mangione 1998; McCloskey 1994; Owsley 1999). These conditions affect many aspects of vision including acuity, contrast sensitivity, visual field sensitivity, and increased disability glare. Disability glare is a degradation of visual performance caused by a reduction of contrast (Smith 2002).
Description of the intervention
Many types of interventions have been proposed to decrease the risk of motor vehicle crashes among older drivers, targeted toward the vehicle, the roadway, and the driver. In many countries, the primary driver‐related intervention focuses on re‐licensing requirements for older drivers, which may involve reassessment. Government policy employs a variety of methods for increasing the stringency of the licensure process for older drivers, including the adoption of in‐person renewal requirements, road tests, implementation of a shorter renewal period, and vision screening tests (Grabowski 2004).
Vision screening is a complex issue. While licensing authorities in many jurisdictions throughout the world use simple strategies to measure driving fitness, utilising simple visual acuity tests, it is not clear that the vision tests used actually assess the visual functions required to drive safely (Sivak 1996). Indeed, research has shown that visual acuity alone is not an appropriate method for assessing full visual function, which includes other vision components such as visual field and contrast sensitivity among others. Current vision screening testes utilised for licensing purposes mainly rely on assessment of visual acuity, which research suggests is, at best, weakly associated with traffic crash involvement (Awardzi 2009; McGwin 2008a). Therefore, more comprehensive vision testing, together with an evaluation of continuing competency for driving, is essential (Christie 2000).
New vision screening methodologies and standards for fitness to drive are now urgently required in order to promote road safety (Desapriya 2008). Evidence shows that visual field, body co‐ordination, and reaction time influence fitness to drive. A recent prospective cohort study conducted by the Motor Vehicle Administration (MVA) in Maryland, USA demonstrated a relationship between performance‐based risk factors and subsequent at‐fault crashes among older drivers (Ball 2006). The study concluded that a driver had to be physically, mentally, medically, and functionally fit in order to operate an automobile. Currently, these factors are not evaluated by licensing authorities.
The common standard threshold used for visual acuity is 20/40 (0.50, 6/12) and this is an accepted requirement for driving in many countries. However, this criterion varies from country to country, although most agree that visual acuity in the better eye of 20/40 (0.50, 6/12) is acceptable. For example, USA jurisdictions differ on the required minimum visual acuity and minimum visual field necessary to pass a screening test. Furthermore, some states assess colour vision, depth perception, contrast sensitivity, and disability glare, while others do not. It is interesting to note that the way in which visual acuity itself is measured differs among countries. For example, in North America visual acuity is measured by a Snellen’s chart in the driving licence office, while UK authorities simply ask a driver to read a number plate for visual acuity.
With respect to the renewal of a driver’s licence, there is also considerable variation. For example, jurisdictions across the USA differ in requiring road tests, vision screening, renewal in person, by mail or by the Internet (McGwin 2008). In Florida, drivers must demonstrate visual acuity of 20/70 in either eye, with or without corrective lenses, whereas drivers in Connecticut must have 20/40 in the better eye, with or without corrective lenses.
In some states, drivers who do not meet the vision requirement may be eligible for a restricted driver’s licence (Levy 1995). There is also variation among states with respect to the field of vision required to operate a motor vehicle. For instance, in Arizona the field of vision must be 60°, plus 35° on the opposite side of the nose, in at least one eye. The field of vision for Connecticut drivers must be 140° for a person with two eyes and 100° for a person with one eye (Owsley 1999). The age at which a vision test is required at renewal ranges from 40 years (Maryland) to 80 years (Virginia). Illinois and New Hampshire require a road test at renewal for drivers age 75 and older (McGwin 2008). This evidence illustrates that practices in the USA and many other countries that govern required vision screening and licensing of older drivers vary significantly. Given the extent of this variation, it is understandable that evidence relating to the effectiveness of vision screening is inconclusive:
Two retrospective cohort studies conducted in USA have suggested that vision‐related older driver licence renewal policies are associated with lower vehicle fatality rates (Levy 1995; Shipp 1998). However, another study, found no traffic safety benefits of vision‐related older driver licence renewal policies in the USA. An in‐person driver licence renewal policy yielded significant traffic safety benefits (Grabowski 2004).
The McGwin 2008a study found that the Florida 2004 mandatory vision screening re‐licensure law reduced the number of elderly drivers involved in fatal crashes by 17 per cent. In addition, this study showed that 93 per cent of individuals who sought licence renewal passed the current Florida vision test. The study suggests that future age‐related vision screening re‐licensing laws should target high‐risk drivers and safeguard driving privileges of low‐risk drivers. The 2008 study by McGwin and colleagues suggests that the Florida 2004 mandatory vision screening re‐licensure law is not a deterrent to seeking licence renewal for the ≥ 80‐year‐old population (McGwin 2008).
One recent review found that the re‐licensing policies requiring in‐person renewal, vision testing and the restricted driver licence were yielding traffic safety benefits for older drivers (Stav 2008).
A recent US study found that the older drivers from states with age‐related licence renewal polices had lower injury prevalence rates compared with drivers with licences from states without any licence renewal policies (Awardzi 2009). Similar to Grabowski 2004, this study also confirmed that the states requiring in‐person renewal had lower injury rates compared to states without in‐person renewal. However, this study found no traffic safety benefits related to reduced renewal cycles and vision/medical tests (Awardzi 2009).
Agimi 2013 found that the vision testing conducted during in‐person renewals are associated with lower fatal crash rates and lower hospitalisation rates. Vision testing was especially predictive of a lower crash fatality rate among drivers aged 80 to 84 and lower dementia prevalence among hospitalised drivers aged 60 to 69. However, this study found that the physician reporting requirements (mandated or legally protected) and length of licensing renewal had no traffic safety benefits. The public health significance of this available traffic safety literature is that the more restrictions on driving do not translate to lower crash rates among older drivers (Agimi 2013).
How the intervention might work
Self‐regulation helps older drivers modify their driving habits to suit their limitations, such as avoiding rush hour, daytime driving only and driving for essential trips only (e.g., groceries, doctors appointments) (Ragland 2005). Driving cessation has been shown to induce depression (Azad 2002; Marottoli 1997; Ragland 2005; Siren 2002) through a loss of independence (Fonda 2001); therefore, self‐regulation may be a feasible option that enhances quality of life and to facilitate safe driving for a greater number of years. However, self‐regulation cannot occur if a person is unaware that their actions require regulating. The goal of vision screening is to identify high‐risk drivers accurately and help them limit their driving. If older drivers are not screened, they may not be aware of their functional limitations. Proper valid screening, therefore, targets both road safety injury prevention as well as self‐awareness.
Researchers agree that the assessment of the driver’s ability should be a fundamental part of the solution for maintaining safe, older driver mobility (Eby 2007; Shope 1998; Staplin 1999). However, the tools that are currently available for licensing authorities to assess fitness‐to‐drive tend not to be scientifically derived or validated and rely heavily on subjective rather than objective conclusions (Eby 2007; Molnar 2007). There is a need, therefore, for the development of valid, evidence‐based instruments to aid licensing authorities in determining fitness to drive (Desapriya 2008; Desapriya 2009; Desapriya 2012). Clinically sensible screening and assessment tools are needed in order that licensing agencies can assess fitness to drive, and promote and facilitate safe licensing of older drivers (Eby 2007; Molnar 2007).
New vision screening methodologies based on evidence‐based practice and standards for fitness to drive are now urgently required to predict visual impairment and promote road safety (Hales 1982). Promising strategies to improve older adults’ driving performance to acceptable levels include: education, training, remediation of physical or mental disabilities, self‐regulation, or regulation by licensing authorities (Adler 2003; Dobbs 1997; Fox 1997; Roenker 2003; Shope 1998; Tuokko 1995). In particular, self‐regulation of driving has been proposed as a viable means of balancing older adults’ autonomy against the competing demand of public safety (Ball 1998; Shope 1998).
Why it is important to do this review
The safety of older drivers and others with whom they share the road is an important global traffic safety issue.The aim of this review is to evaluate the effectiveness of vision screening tests for the prevention of motor vehicle crashes involving older drivers. While vision screening assessments have generally been tested against on‐road driving performance, their impact on traffic crashes, road traffic law violation, fatalities, or injury reduction has not been evaluated. The effectiveness of vision screening for older drivers has been evaluated in retrospective cohort studies (see 'Characteristics of excluded studies'); however, the results are inconclusive as retrospective cohort studies are prone to bias. We therefore propose a randomised controlled trial (RCT) to evaluate the efficacy of vision screening in reducing crashes among older drivers.
Objectives
To critically assess the effects of vision screening interventions on the prevention of older driver‐related motor vehicle crashes
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) comparing crash rates among older drivers before and after vision screening interventions. Studies must have included one or more of the primary outcomes of interest: traffic violations, motor vehicle crashes, injuries or fatalities. In the absence of RCTs evaluating the effects of vision screening, controlled before and after (CBA) studies were also eligible for inclusion.
Types of participants
Trials with older individuals (aged 55 years or over) of either sex, who were current drivers.
Types of interventions
Any screening method, including road and vision testing, compared with controls without screening. This included tests such as 'useful field of view' (UFOV), contrast sensitivity, visual fields (central or peripheral), visual acuity, and any other automated vision screening measures.
Types of outcome measures
Traffic violations.
Motor vehicle crashes.
Injuries sustained during motor vehicle crashes.
Fatalities due to motor vehicle crashes.
Search methods for identification of studies
We did not limit our search by language, date or publication status.
Electronic searches
The Cochrane Injuries Group Trials Search Co‐ordinator searched the following:
Cochrane Injuries Group's Specialised Register (26th September 2013);
Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library) (The Cochrane Library 2013, Issue 9 of 12);
MEDLINE (OvidSP) (1950 to Sept 27th 2013);
Embase (OvidSP) (1980 to 2013 week 39);
PsycINFO (1806 to October week 1 2013);
ISI Web of Science: Social Sciences Citation Index (SSCI) (1970 to Sept 2013);
ISI Web of Science: Conference Proceedings Citation Index‐ Science (CPCI‐S) (1990 to Sept13).
Search strategies are listed in Appendix 1. Search methods for previous versions of this review are in Appendix 2.
Searching other resources
No other sources were searched for this update. See Appendix 2 for details.
Data collection and analysis
Selection of studies
Two review authors (SH, RH) independently reviewed titles (and abstracts where available) from the search outputs to identify potentially relevant studies. The same two authors independently reviewed the full text of studies identified, using a standardised inclusion criteria form. We resolved discrepancies through discussions between the authors, with the involvement of a third party (ED) where necessary. A list of excluded studies, together with details regarding the reasons for exclusion, has been provided in the table 'Characteristics of excluded studies'. We obtained full copies of those articles identified by the search considered to have met the inclusion criteria based on title, abstract, and subject descriptors.
Assessment of risk of bias in included studies
We planned to assess the quality of individual components, such as randomisation, allocation, concealment methods, blinding, and patient follow‐up. Key definitions derived from the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) would have been used to assess the quality of selected studies. The elements inherent in a carefully designed and conducted RCT are intended to minimise bias, balance confounders, and produce the most reliable estimate of treatment effect. We planned to assess each included trial against a comprehensive checklist provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Four review authors (HC, ED, JB, SH) planned to perform quality assessment independently, with disagreements being resolved by further discussion.
In the event of an absence of RCTs, we planned to consider controlled before and after (CBA) studies for inclusion. The following methodological criteria would have been used to assess CBA studies:
study design;
data collection methods;
assessment of comparability of groups on potential confounders;
sound method of ascertaining exposure (should be valid, reproducible, and blinded);
sound case definition (should be valid, reproducible, and blinded);
sound outcome assessment (should be valid, reproducible, and blinded);
completeness of follow‐up.
Data synthesis
Where possible, we planned to calculate odds ratios (for categorical outcome data) or standardised mean differences (for continuous data) and their 95% confidence intervals (CI) from the data generated by each included RCT. If appropriate, and with available data, we planned to pool results from comparable groups of studies into a meta‐analysis using the RevMan 5.0 software provided by The Cochrane Collaboration (Review Manager). We intended to test heterogeneity between combined studies using the standard Chi2 test. Where statistical pooling was not appropriate or possible, we planned to provide a narrative summary of the findings.
Four review authors (HC, JB, SH, IP) planned to extract data independently using a standardised form. The following information was to be extracted:
Type of study: RCT or CBA study.
Study setting: road, time of year, and day when outcomes were measured.
Type of screening: useful field of view (UFOV), contrast sensitivity, visual fields (central or peripheral), visual acuity, and any other automated vision screening measures.
Follow‐up: duration of follow‐up from vision screening testing.
Outcomes: number and types of older drivers committing traffic violations; involved in motor vehicle crashes; and sustaining minor, severe, or fatal injury.
Cost: information about the cost of implementing vision screening.
Two review authors (HC, ED) planned to perform the applicable data analysis of the extracted data. The data would have been analysed as follows.
Meta‐analysis: a random‐effects meta‐analysis would have been performed.
Continuous data would have been analysed if means and standard deviations were available and there was no evidence of skew in the data (defined as mean > standard deviation). If scales measured the same outcome in different ways, standardised mean differences would have been combined across studies.
Binary data: for studies with binary outcome data, the association between intervention and outcome would have been quantified using the odds ratio along with the 95% CI.
Heterogeneity: investigation of the heterogeneity of the odds ratios across studies would have been assessed using a standard Chi2 test.
Funnel plots: odds ratios would have been determined and represented on a funnel plot, which describes the relationship between effect size and study precision. We intended to examine the reasons for any relationship identified (sample size, publication bias, diversity of interventions and populations).
Sensitivity analysis: the primary analysis would have involved all studies. We planned to assess the robustness of the findings by subgroup analysis based on sample size, study quality, and setting. Where possible, we planned to conduct high versus low‐ and middle‐income areas, and rural versus urban setting subgroup analyses, according to study context.
Results
Description of studies
In total we screened 5921 citations for eligibility: 4589 citations were screened in 2006; 756 citations in 2011; 576 citations were screened in 2013 (Figure 1). From the most recent search six relevant studies were identified but they did not meet the pre‐defined study design criteria.
1.
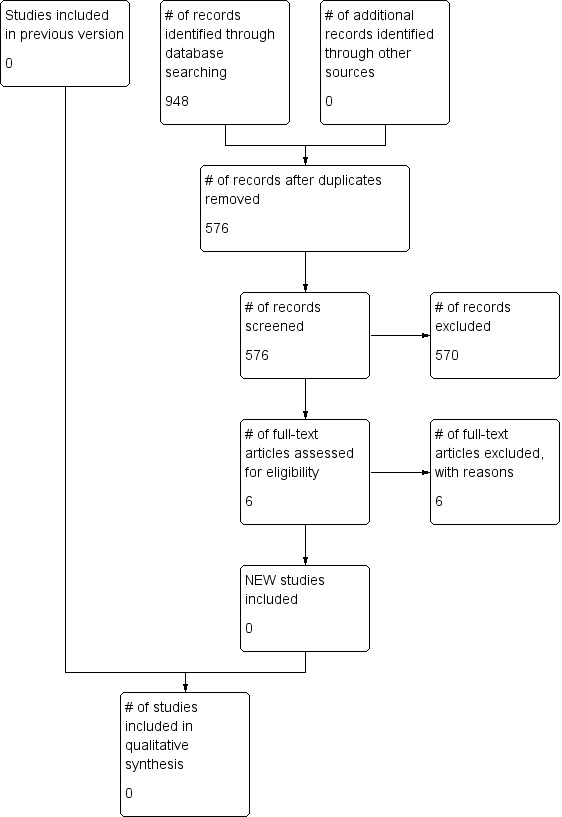
Study flow diagram.
Risk of bias in included studies
No studies met the inclusion criteria.
Effects of interventions
No studies were identified that satisfied the inclusion criteria.
Discussion
We found no studies that met the inclusion criteria, and no studies are included in the review.
The major limitation of this review is that we were unable to find any high quality studies, such as randomised controlled trials or controlled before and after studies, to include in the review. Therefore, there is no definitive evidence in support of, or against, the hypothesis that vision screening leads to a reduction in motor vehicle crashes involving older drivers. A strength of this review is that it has identified a gap in the literature by demonstrating a lack of trials studying older driver vision screening and motor vehicle crashes.
Authors' conclusions
Implications for practice.
At present, there is insufficient evidence to support or refute the efficacy of the vision screening test as a preventive strategy to reduce motor vehicle crashes among older drivers. In addition, the use of driving assessment tools, such as visual acuity, on road driving tests, simulator tests, and others vary among jurisdictions and their validity has been questioned in the research literature. Hence, further research is required to fully examine their reliability. In addition to licensing authorities, physicians also play a vital role in the safety of older drivers as they typically have the first encounter with older drivers experiencing vision problems. There is a serious need for research to develop a battery of tests with proven sensitivity and specificity for identifying high‐risk drivers so that physicians and ophthalmologists can provide guidance to their patients, and also to medical advisory boards working with licensing offices (Hales 1982). Not only does research have the challenge of developing tests of high sensitivity and specificity for identifying unsafe drivers, these tests must also be cost‐effective and acceptable to the public. In the interim, physicians should refer visually impaired drivers to driver training and re‐education programs that are designed to reinforce safe driving practices and caution on the road.
Implications for research.
There are no randomised controlled trials to demonstrate that vision screening for older drivers reduces the risk of motor vehicle crashes. Most countries require a vision screening test for driver licence renewal and this seems a reasonable and sensible approach. Good vision at all ages is important for safe driving. A case can be made, based on the existing literature, that more high quality trials are needed to evaluate the efficacy of vision screening in reducing motor vehicle crashes. Future trials would ideally utilise a randomised controlled trial design.
There is a need to develop effective vision screening tools that are valid predictors of fitness to drive. Vision standards established for driving licenses have been criticised for being arbitrary and not adequate to screen all potential visual components for safe driving (Ball 1988; Ball 1991; Levy 1995; Owsley 1998). Owsley 1991 and colleagues were the first to provide significant evidence that demonstrated a relationship between useful field of view (UFOV) and motor vehicle crashes. Performance‐based functional assessments, including the use of driving simulators and road tests, may facilitate this task by providing information that is useful for the evaluation and rehabilitation of possibly impaired older drivers (Boegner 2004; Shope 1998; Underwood 1992). The UFOV concept has been further developed and used for training programs to help older drivers to retain and regain their driving skills.
UFOV is the area over which a person can extract information in a single glance without moving his or her head or eyes. The UFOV is shown to adequately predict driving performance. It provides a rapid and effective measure of visual information processing speed in approximately five minutes. It identifies examinees whose performance is associated with a significant increase in collision risk. UFOV also measures skills in selective and divided attention (Rizzo 1997) and how rapidly one can process multiple stimuli in the visual field. This measure is economically valid in that it has been shown to be an excellent predictor of both motor vehicle crashes and mobility outcomes among older adults (Ball 1998). Rinalducci 2002 showed that UFOV adequately predicted driving performance on a low‐fidelity simulation task. Therefore, the UFOV may also serve as a useful method of identifying at‐risk drivers who may not be easily screened through other techniques. Recent prospective studies have confirmed a relationship between UFOV performance and future crashes, further supporting the use of this instrument as a potential screening measure for at‐risk older drivers (Rubin 2007). A recent meta‐analysis conducted with numerous studies that included various methodologies confirms the importance of the UFOV assessment as both valid and reliable for indicating driving performance and for ensuring road safety (Clay 2005). This meta‐analysis clearly demonstrated the association between poorer UFOV and poorer driving performance in older adults.
What's new
| Date | Event | Description |
|---|---|---|
| 26 September 2013 | New citation required but conclusions have not changed | The search for studies has been updated to 26 September 2013. No new studies have been included in the review. This review has no included studies. The authors of the review have changed. |
| 26 September 2013 | New search has been performed | The search for studies has been updated to 26 September 2013. |
History
Protocol first published: Issue 4, 2006 Review first published: Issue 1, 2009
| Date | Event | Description |
|---|---|---|
| 21 January 2011 | New citation required but conclusions have not changed | The search has been updated to 1 June 2010. No new studies were included; one study was excluded. There remain no studies included in this review. The authors have changed. |
Acknowledgements
We are grateful to the Cochrane Injuries Group's editorial base for their technical support. We especially want to thank Emma Sydenham and Deirdre Beecher for their on going support for review updates. We thank Shelina Babul, Kate Turcotte, Harshani Wijeratne, Fahra Rajabali and Jackie Kinney for their contribution to the original version of this review. We also thank the Cochrane Eyes and Vision Group for input on the manuscript.
Appendices
Appendix 1. Search strategies
Cochrane Injuries Group's Specialised Register
(((vision* or visual* or sight* or eyesight* or eye*)) AND ((exam* or test* or screen* or assessment*)) AND ((driver* or driving or crash* or accident* or motor* or vehicle* or automobile*)))
Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library) (The Cochrane Library)
#1MeSH descriptor: [Vision Screening] explode all trees #2MeSH descriptor: [Vision Tests] explode all trees #3MeSH descriptor: [Mass Screening] explode all trees #4MeSH descriptor: [Vision, Ocular] explode all trees #5(vision or visual or field of view or contrast sensitivity or visual field or driving capabilit*):ti,ab,kw (Word variations have been searched) #6#4 or #5 #7#3 and #6 #8((vision or visual or sight* or eyesight* or eye*) near/3 (exam* or test* or screen* or assessment*)):ti,ab,kw (Word variations have been searched) #9#1 or #2 or #7 or #8 #10MeSH descriptor: [Motor Vehicles] explode all trees #11MeSH descriptor: [Automobile Driving] explode all trees #12MeSH descriptor: [Accidents, Traffic] explode all trees #13(driver* or driving or crash* or accident* or motor* or vehicle* or automobile*):ti,ab,kw (Word variations have been searched) #14MeSH descriptor: [Geriatric Assessment] explode all trees #15MeSH descriptor: [Aged, 80 and over] explode all trees #16MeSH descriptor: [Aged] this term only #17MeSH descriptor: [Age Factors] explode all trees #18#10 or #11 or #12 or #13 #19#14 or #15 or #16 or #17 #20#18 and #19 #21(aged or senior* or elder* or older) near/3 (driver* or driving):ti,ab,kw (Word variations have been searched) #22(#20 or #21) and #9
MEDLINE (OvidSP)
1 exp Vision‐Screening/ 2 exp Vision‐Tests/ 3 exp Mass‐Screening/ 4 exp Vision/ 5 (vision or visual or field of view or contrast sensitivity or visual field or driving capabilit$).ab,ti. 6 4 or 5 7 3 and 6 8 ((vision or visual or sight$ or eyesight$ or eye$) adj3 (exam$ or test$ or screen$ or assessment$)).ab,ti. 9 1 or 2 or 7 or 8 10 exp Motor‐Vehicles/ 11 exp Automobile‐Driving/ 12 exp Accidents‐Traffic/ 13 (driver$ or driving or crash$ or accident$ or motor$ or vehicle$ or automobile$).ab,ti. 14 exp geriatric assessment/ 15 exp aged/ 16 exp "aged 80 and over"/ 17 exp age factors/ 18 10 or 11 or 12 or 13 19 14 or 15 or 16 or 17 20 18 and 19 21 ((aged or senior$ or elder$ or older) adj3 (driver$ or driving)).ab,ti. 22 20 or 21 23 9 and 22
Embase (OvidSP)
1 exp Vision‐Screening/ 2 exp Vision‐Tests/ 3 exp Mass‐Screening/ 4 exp Vision/ 5 (vision or visual or field of view or contrast sensitivity or visual field or driving capabilit$).ab,ti. 6 4 or 5 7 3 and 6 8 ((vision or visual or sight$ or eyesight$ or eye$) adj3 (exam$ or test$ or screen$ or assessment$)).ab,ti. 9 1 or 2 or 7 or 8 10 exp Motor‐Vehicles/ 11 exp Automobile‐Driving/ 12 exp Accidents‐Traffic/ 13 (driver$ or driving or crash$ or accident$ or motor$ or vehicle$ or automobile$).ab,ti. 14 exp geriatric assessment/ 15 exp aged/ 16 exp "aged 80 and over"/ 17 exp age factors/ 18 10 or 11 or 12 or 13 19 14 or 15 or 16 or 17 20 18 and 19 21 ((aged or senior$ or elder$ or older) adj3 (driver$ or driving)).ab,ti. 22 20 or 21 23 9 and 22
PsycINFO (OvidSP)
1 exp Screening/ 2 exp Vision/ 3 (vision or visual or field of view or contrast sensitivity or visual field or driving capabilit$).ab,ti. 4 2 or 3 5 1 and 4 6 ((vision or visual or sight$ or eyesight$ or eye$) adj3 (exam$ or test$ or screen$ or assessment$)).ab,ti. 7 5 or 6 8 exp Motor‐Vehicles/ 9 exp Motor Traffic Accidents/ 10 (driver$ or driving or crash$ or accident$ or motor$ or vehicle$ or automobile$).ab,ti. 11 exp geriatric assessment/ 12 exp aged/ 13 8 or 9 or 10 14 11 or 12 15 13 and 14 16 ((aged or senior$ or elder$ or older) adj3 (driver$ or driving)).ab,ti. 17 (15 or 16) and 7
ISI Web of Science ‐ CPCI‐S & SSCI
#1 TS=(((vision near/3 test*) or (sight near/3 test*) or (eyesight near/3 test*) or (eye near/3 test*) or (eye near/3 exam*) or (sight near/3 exam*) or (vision near/3 exam*) or (eyesight near/3 exam*) or (vision near/3 screen*))) #2 Topic=((driver* or driving or crash* or accident* or motor* or vehicle* or automobile*)) #3 #2 AND #1
Appendix 2. Search methods for previous versions
Previous searches for this review did not retrieve any relevant studies and therefore it was not deemed worthwhile to continue searching all of the sources listed here:
Electronic searches We searched the following electronic databases: Cochrane Injuries Group's Specialised Register (searched June 1, 2010); CENTRAL (The Cochrane Library Issue 2, 2010); MEDLINE (Ovid) 1950 to May (week 3) 2010); EMBASE (1980 to August 2006); TRANSPORT (Ovid) 1988 to June 2009); ASSIA: Applied Social Sciences Index and Abstracts (1987 to June 2010); AgeInfo (searched 6 September 2006); AgeLine (searched 6 September 2006); National Research Register (to issue 3, 2006); IBSS: International Bibliography of the Social Sciences (1951 to June 2010); ISI Web of Science: Social Sciences Citation Index (SSCI) (1970 to June 2010); ISI Web of Science: Conference Proceedings Citation Index‐ Science (CPCI‐S) (1990 to June 2010); PsycINFO (1806 to week 3 September 2006); Zetoc (searched 2 September 2006); PubMed (2006‐January (week 2) 2011). The detailed search strategies are reported in Appendix 1 & Appendix 2. Searching other resources Handsearching We handsearched the following journals for relevant articles (from January 2006 to March 2007, and from January 2010 to January 6th 2011): Injury Prevention; Accident Analysis and Prevention; International Journal of Injury Control and Safety Promotion; The Journal of Safety Research. Grey literature and unpublished studies We searched websites relating to traffic and road crash research bodies, government agencies, and injury prevention organisations for any grey literature. In addition, reference lists of the selected papers or topic reviews were scanned for potentially relevant papers. We reviewed a published abstract from the seventh World Conference on Injury Prevention and Control (2004) for potentially relevant studies. We also contacted experts from national and international injury prevention organisations for help in identifying further studies. We sought relevant dissertation abstracts, grey literature, and conference proceedings by a general Internet search using a combination of terms taken from the electronic search strategies.
Characteristics of studies
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Agimi 2013 | (i) Study design ‐ retrospective cohort study. (ii) Interventions were Physician mandatory reporting requirements, length of license renewal, and vision testing. |
| Awardzi 2009 | (i) Study design ‐ retrospective cohort study. (ii) Interventions were in‐person renewal of driving license, reduced renewal cycles of driver license, and vision and medical test. |
| Grabowski 2004 | (i) Study design ‐ retrospective cohort study. (ii) Interventions were in‐person renewal of driving license, road test, and vision test. |
| Levy 1995 | (i) Study design ‐ retrospective cohort study. (ii) Interventions were a combination of vision test, knowledge test, and on‐road driving test. |
| McGwin 2008a | (i) Study design ‐ retrospective cohort study. (ii) Interventions was mandatory vision screening re‐license law, which was implemented to target 80 years and older drivers in Florida. |
| Shipp 1998 | (i) Study design ‐ cohort study. (ii) Interventions were state‐level mandatory vision testing policies for re‐licensing. |
Contributions of authors
Dr Sayed Subzwari contributed significantly to the protocol development, concept and design, and data acquisition. Dr. Subzwari screened the citations of the first search for this review. He also wrote the first draft of the manuscript with the help of Dr Ediriweera Desapriya. Dr Ediriweera Deaspriya, Dr Shelina Babul and Dr Ian Pike contributed significantly to the systematic review's concept and design, and protocol development. Ms Fahra Rajabali and Ms Kate Turcotte contributed significantly to the literature search, and quality assessment. Ms Jacqueline Kinney contributed significantly to the systematic review's data acquisition and interpretation of the data. All authors provided critical revisions to the manuscript and gave final approval of the submitted manuscript.
For the 2011 update: Dr. Ediriweera Desapriya updated the review with help of all other co‐authors of this review. Ms. Harshani Wijeratne contributed by updating the literature review and screening the selected literature for eligibility. All authors provided critical revisions to the updated review and gave final approval of the submitted review.
For the 2014 update: Dr. Ediriweera Desapriya updated the review with help of all other co‐authors of this review. Ms. Rahana Harjee and Dr. Sesath Hewapathirane contributed by updating the literature review and screening the selected literature for eligibility. Dr. Brubacher, Dr. Pike, Dr. Hewapathirane, Ms. Harjee and Dr. Chan provided critical revisions to the updated review and gave final approval of the submitted review.
Sources of support
Internal sources
BC Injury Research & Prevention Unit, Canada.
Department of Pediatrics, University of British Columbia, Vancouver, Canada.
Department of Emergency Medicine, University of British Columbia, Canada.
Centre for Clinical Epidemiology and Evaluation, Vancouver General Hospital, Canada.
External sources
BC Ministry of Health Services, Canada.
Declarations of interest
None known.
New search for studies and content updated (no change to conclusions)
References
References to studies excluded from this review
Agimi 2013 {published data only}
- Agimi Y. Role of state driver licensing policies and physician reporting laws on older driver safety. Dissertation Abstracts International: Section B: The Sciences and Engineering 2013; Vol. 74, issue 1:B(E).
Awardzi 2009 {published data only}
- Awardzi KD. Socio‐ecological determinants of injury among younger and older adults involved in fatal motor vehicle crashes in the United States. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009; Vol. 70, issue (2‐B):923.
Grabowski 2004 {published data only}
- Grabowski DC, Christine MC, Michael AM. Elderly licensure laws and motor vehicle fatalities. JAMA 2004;291:2840‐6. [DOI] [PubMed] [Google Scholar]
Levy 1995 {published data only}
- Levy DT, Vernick JS, Howard KA. Relationship between driver's license renewal policies and fatal crashes involving drivers 70 years and older. JAMA 1995;274:1026‐30. [PubMed] [Google Scholar]
McGwin 2008a {published data only}
- McGwin G, Sarrels SA, Griffin R, Owsley C, Rue LW. The impact of a vision screening law on older driver fatality rates. Archives of Ophthalmology 2008;126(11):1544‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Shipp 1998 {published data only}
- Shipp MD. Potential human and economic cost savings attributable to vision testing policies for driver's license renewal, 1989‐1991. Optometry and Vision Science 1998;75:103‐18. [DOI] [PubMed] [Google Scholar]
Additional references
Adler 2003
- Adler G, Kuskowski M. Driving cessation in older men with dementia. Alzheimer Disease and Associated Disorders 2003;17(2):68‐71. [DOI] [PubMed] [Google Scholar]
Azad 2002
- Azad N, Byszewski A, Amos S, Molnar FJ. A survey of the impact of driving cessation on older drivers. Geriatrics Today 2002;5:170‐4. [Google Scholar]
Ball 1988
- Ball K, Beard B, Roenker D, Miller RL, Griggs DS. Age and visual search: Expanding the useful field of view. Journal of the Optical Society of America 1988;5:2210‐9. [DOI] [PubMed] [Google Scholar]
Ball 1991
- Ball K, Owsley C. Identifying correlates of accident involvement for the older driver. Human Factors 1991;33(3):583‐95. [DOI] [PubMed] [Google Scholar]
Ball 1998
- Ball K, Owsley C, Stalvey B, Roenker DL, Sloane ME, Graves M. Driving avoidance and functional impairment in older drivers. Accident Analysis and Prevention 1998;30(3):313‐22. [DOI] [PubMed] [Google Scholar]
Ball 2006
- Ball KK, Roenker DL, Wadley VG, Edwards JD, Roth DL, McGwin G, et al. Can high‐risk older drivers be identified through performance‐based measures in a Department of Motor Vehicles setting?. Journal of American Geriatric Society 2006;54(1):77‐84. [DOI] [PubMed] [Google Scholar]
Boegner 2004
- Bogner HR, Straton JB, Gallo JJ, Rebok GW, Keyl PM. The role of physicians in assessing older drivers: Barriers, opportunities, and strategies. Journal of the American Board of Family Practice 2004;17:38‐43. [DOI] [PMC free article] [PubMed] [Google Scholar]
Christie 2000
- Christie R. Driver licensing requirements and performance standards including driver and rider training. National Road Transport Commission, Melbourne, Australia 2000.
Clay 2005
- Clay OJ, Wadley VG, Edwards JD. Cumulative meta‐analysis of the relationship between useful field of view and driving performance in older adults: current and future implications. Optometry Vision Science 2005;82(8):724‐31. [DOI] [PubMed] [Google Scholar]
Desapriya 2008
- Desapriya E, Subzwari S, Fujiwara T, Pike I. Conventional vision screening tests and older driver motor vehicle crash prevention. International Journal of Injury Control and Safety Promotion 2008;15(2):124‐6. [DOI] [PubMed] [Google Scholar]
Desapriya 2009
- Desapriya E, Subzwari S, Pike I. Globally we need more comprehensive vision‐screening strategies. British Journal of Opthalmology 2009;93(6):843. [DOI] [PubMed] [Google Scholar]
Desapriya 2012
- Desapriya E, Ranatunga Y, Pike I. We need evidence based tools to identify medically at risk drivers. BMJ 2012;24(345):e7087. [DOI] [PubMed] [Google Scholar]
Dobbs 1997
- Dobbs AR. Evaluating the driving competence of dementia patients. Alzheimer Disease and Associated Disorders 1997;11 Suppl 1:8‐12. [DOI] [PubMed] [Google Scholar]
Eby 2007
- Eby DW, Molnar LJ, Louis RM, Neumeyer AL. Promising approaches for promoting lifelong community mobility. Ann Arbor: University of Michigan, Ann Arbor, Transportation Research Institute, 2007. [Google Scholar]
Fishman 1981
- Fishman GA, Anderson RJ, Stinson L, Haque A. Driving Performance of Retinitis Pigmentosa Patients. British Journal of Ophthalmology 1981;65(2):122‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fonda 2001
- Fonda SJ, Wallace RB, Herzog AR. Changes in driving patterns and worsening depressive symptoms among older adults. Journal of Gerontology Social Science 2001;56B Suppl(6):343‐51. [DOI] [PubMed] [Google Scholar]
Fontaine 2003
- Fontaine H. Driver age and road traffic accidents: what is the risk for seniors? [Age des conducteurs de voiture et accidents de la route: Quel risqué pour les seniors]. Recherche‐Transports‐Securite 2003;79‐80:107‐20. [Google Scholar]
Fox 1997
- Fox GK, Bowden SC, Bashford GM. Alzheimer's disease and driving: prediction and assessment of driving performance. Journal of American Geriatric Society 1997;45:949‐53. [DOI] [PubMed] [Google Scholar]
Gutierrez 1997
- Gutierrez MR, Wilson J. Influence of glaucomatous visual field loss on health‐related quality of life. Archives Ophthalmology 1997;115:777‐84. [DOI] [PubMed] [Google Scholar]
Hakamies Blomqvist 2002
- Hakamies Blomqvist L, Raitanen T, O'Neill D. Driver ageing does not cause higher accident rates per km. Transportation Research Part F: Traffic Psychology and Behaviour 2002;5(4):271‐4. [Google Scholar]
Hakamies Blomqvist 2005
- Hakamies Blomqvist L, Wiklund M, Henriksson P. Predicting older drivers accident involvement? Smeed's law revisited. Accident Analysis and Prevention. 2005;37(4):675‐80. [DOI] [PubMed] [Google Scholar]
Hales 1982
- Hales RH. Functional ability profiles for driver licensing. Archives of Ophthalmology 1982;100:1780‐3. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions 5.1.0 [updated March 2011]. The Cochrane Collaboration 2011. Available from www.cochrane‐handbook.org.
Janke 2001
- Janke MK. Assessing older drivers. Journal of Safety Research 2001;32:43‐74. [Google Scholar]
Javitt 2002
- Javitt JC. Risk of motor vehicle crashes in patients with cataract surgery. JAMA 2002;288(18):2262. [DOI] [PubMed] [Google Scholar]
Johnson 2010
- Johnson CA, Wilkinson ME. Vision and driving: the United States. Journal of Neuroophthalmology 2010;30(2):170‐6. [DOI] [PubMed] [Google Scholar]
Kent 2009
- Kent R, Trowbridge M, Lopez‐Valdes FJ, Ordoyo RH, Segui‐Gomez M. How many people are injured and killed as a result of aging? Frailty, fragility, and the elderly risk‐exposure tradeoff assessed via a risk saturation model. Annals of Advances in Automotive Medicine 2009;53:41‐50. [PMC free article] [PubMed] [Google Scholar]
Langford 2006
- Langford M, Methorst R, Hakamies‐Blomqvist L. Older drivers do not have a high crash risk: a replication of low mileage bias. Accident Analysis and Prevention 2006;38(3):574‐8. [DOI] [PubMed] [Google Scholar]
Li 2003
- Li G, Braver ER, Chen LH. Fragility versus excessive crash involvement as determinants of high death rates per vehicle‐mile of travel among older drivers. Accident Analysis and Prevention 2003;35(2):227‐35. [DOI] [PubMed] [Google Scholar]
Mangione 1998
- Mangione M, Lee PP, Pitts J, Gutierrez P, Berry S, Hays RD. Psychometric properties of the National Eye Institute Visual Function Questionnaire (NEI‐VFQ). Archives of Ophthalmology 1998;116:1496‐504. [DOI] [PubMed] [Google Scholar]
Marottoli 1997
- Marottoli RA, Mendes de Leon CF, Glass TA, Williams CS, Cooney LM, Berkman LF, et al. Driving cessation and increased depressive symptoms: prospective evidence from the New Haven EPESE. Established Populations for Epidemiologic Studies of the Elderly. Journal of American Geriatric Society 1997;45(2):202‐6. [DOI] [PubMed] [Google Scholar]
McCloskey 1994
- McCloskey LW, Koepsell TD, Wolf ME, Buchner DM. Motor vehicle collision injuries and sensory impairments of older drivers. Age and Ageing 1994;23(4):267‐73. [DOI] [PubMed] [Google Scholar]
McGwin 2008
- McGwin G, McCartt AT, Braitman KA, Owsley C. Survey of older drivers' experiences with Florida's mandatory vision re‐screening law for licensure. Ophthalmic Epidemiology 2008;15(2):121‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Molnar 2007
- Molnar FJ, Marshall SC, Man‐Son‐Hing M, Wilson KG, Byszewski AM, Stiell I. Acceptability and concurrent validity of measures to predict older driver involvement in motor vehicle crashes: an Emergency Department pilot case‐control study. Accident Analysis and Prevention 2007;39(5):1056‐63. [DOI] [PubMed] [Google Scholar]
Murray 1996
- Murray CJ, Lopez AD. Alternative visions of the future: projecting mortality and disability, 1990‐2020. The Global Burden of Disease. Cambridge (Massachusetts): Harvard University Press, 1996. [Google Scholar]
NCIPC 2002
- National Center for Injury Prevention and Control. CDC injury research agenda. www.cdc.gov/ncipc/pub‐res/researchagenda/agenda.htm 2002.
OECD 2001
- Organization for Economic Cooperation and Development. Ageing and transport: mobility needs and safety issues. Paris, France. www.oecd.org/dataoecd/40/63/2675189.pdf 2001.
Owsley 1991
- Owsley C, Ball K, Sloane ME, Roenker DL, Bruni JR. Visual/cognitive correlates of vehicle accidents in older drivers. Psychology and Aging 1991;6(3):403‐15. [DOI] [PubMed] [Google Scholar]
Owsley 1998
- Owsley C, McGwin G, Ball K. Vision impairment, eye disease, and injurious motor vehicle crashes in the elderly. Ophthalmic Epidemiology 1998;5(2):101‐13. [DOI] [PubMed] [Google Scholar]
Owsley 1999
- Owsley C, Stalvey B, Wells J, Sloane ME. Older drivers and cataract: Driving habits and crash risk. Journal of Gerontology 1999;54A:M203‐11. [DOI] [PubMed] [Google Scholar]
Owsley 2010
- Owsley C. The vision and driving challenge. Journal of Neuroophthalmology 2010;30(2):115‐6. [DOI] [PubMed] [Google Scholar]
Ragland 2005
- Ragland DR, Satariano WA, MacLeod KE. Driving cessation and increased depressive symptoms. Journal of Gerontology 2005;60(3):399‐403. [DOI] [PubMed] [Google Scholar]
Review Manager [Computer program]
- The Nordic Cochrane Centre. Review Manager (RevMan). Version 5.0. Copenhagen: The Cochrane Collaboration, 2008. [http://ims.cochrane.org/revman]
Rinalducci 2002
- Rinalducci EJ, Mouloua M, Smither J. Cognitive and perceptual factors in aging and driving performance. Report No. VPL‐03‐01. Tallahassee, FL: Florida Department of Transportation 2001.
Rizzo 1997
- Rizzo M, Reinach S, McGehee D, Dawson J. Simulated car crashes and crash predictors in drivers with Alzheimer disease. Archives of Neurology 1997;54:545‐51. [DOI] [PubMed] [Google Scholar]
Rizzo 2011
- Rizzo M. Impaired driving from medical conditions: a 70‐year‐old man trying to decide if he should continue driving. Journal Of American Medical Association 2011;305(10):1018‐26. [DOI] [PMC free article] [PubMed] [Google Scholar]
Roenker 2003
- Roenker DL, Cissell GM, Ball KK, Wadley VG, Edwards JD. Speed‐of processing and driving simulator training result in improved driving performance. Human Factors 2003;45(2):218‐33. [DOI] [PubMed] [Google Scholar]
Rosenbloom 2001
- Rosenbloom S. Sustainability and automobility among the elderly: an international assessment. Transportation 2001;28(4):375‐408. [Google Scholar]
Rubin 2007
- Rubin GS, Ng ES, Bandeen‐Roche K, Keyl PM, Freeman EE, West SK. A prospective, population‐based study of the role of visual impairment in motor vehicle crashes among older drivers: the SEE study. Investigative Ophthalmology Visual Sciences 2007;48(4):1483‐91. [DOI] [PubMed] [Google Scholar]
Shope 1998
- Shope JT, Eby DW. Improvement of Older Driver Safety through Self‐Evaluation: Focus Group Results. Report No. UMTRI‐98‐29. Ann Arbor, MI: University of Michigan Transportation Research Institute 1998.
Silcock 1997
- Silcock CG, Jacobs AA. Socio economic aspects of road accidents in developing countries. Transport Research Laboratory (TRL) 1997;R6237(247):1‐33. [Google Scholar]
Siren 2002
- Siren A. I speeded off and showed the boys how driving is done? Car driving in older women's stories [Painoin tallan lautaan ja näytin pojille missä mennään?autoilu iäkkäiden naisten kertomuksissa]. Naistutkimus Kvinnoforskning 2002;16:30‐42. [Google Scholar]
Sivak 1996
- Sivak M. The information that drivers use: is it indeed 90% visual?. Perception 1996;25:1081‐9. [DOI] [PubMed] [Google Scholar]
Smith 2002
- Smith G. Disability glare and its clinical significance. http://www.optometry.co.uk/uploads/articles/f5dc196f4748c05151e9ad4e9d2bf5f8_smith20020418.pdf 2002.
Staplin 1999
- Staplin L, Lococo KH, Stewart J, Decina LE. Safe Mobility for Older People Notebook. Report No. DOT HS 808 853. Washington, DC: US Department of Transportation 1999.
Stav 2008
- Stav WB. Review of the evidence related to older adult community mobility and driver licensure policies. American Journal of Occupational Therapy 2008;62(2):149‐58. [DOI] [PubMed] [Google Scholar]
Tuokko 1995
- Tuokko H, Tallman K, Beattie BL, Cooper P, Weir J. An examination of driving records in a dementia clinic. Journal of Gerontology 1995;3:S173‐81. [DOI] [PubMed] [Google Scholar]
Underwood 1992
- Underwood M. The older driver: Clinical assessment and injury prevention. Archives of Internal Medicine 1992;152:735‐40. [DOI] [PubMed] [Google Scholar]
West 2003
- West CG, Gildengorin G, Haegerstrom‐Portnoy G, Lott LA, Schneck ME, Brabyn JA. Vision and driving self‐restriction in older adults. Journal of American Geriatric Society 2003;51:1348‐55. [DOI] [PubMed] [Google Scholar]
WHO 2005
- World Health Organization. World report on road traffic injury prevention, 2004. www.whglibdoc.who.int/publications/2005/924159280Xpart3.pdf 2005.
Wood 2001
- Wood JM, Mallon K. Comparison of driving performance of young and old drivers (with and without impairment) measured under in‐traffic conditions. Optometry and Vision Science 2001;78:343‐9. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Desapriya 2011
- Desapriya E, Wijeratne H, Subzwari S, Babul‐Wellar S, Turcotte K, Rajabali F, et al. Vision screening of older drivers for preventing road traffic injuries and fatalities. Cochrane Database of Systematic Reviews 2011, Issue 3. [DOI: 10.1002/14651858.CD006252.pub3] [DOI] [PubMed] [Google Scholar]
Subzwari 2009
- Subzwari S, Desapriya E, Babul‐Wellar S, Pike I, Turcotte K, Rajabali F, et al. Vision screening of older drivers for preventing road traffic injuries and fatalities. Cochrane Database of Systematic Reviews 2009, Issue 1. [DOI: 10.1002/14651858.CD006252.pub2] [DOI] [PubMed] [Google Scholar]