

Key Clinical Message
Chondroid lipoma is rare benign lipomatous lesion could mimic other soft tissue tumor.
Keywords: calcifications, chondroid, chondrosarcoma, lipoma, soft tissue lesion
A rare chondroid lipoma mass could mimic malignancy.

1. INTRODUCTION
A chondroid lipoma is an unusual benign lipomatous lesion that can appear anywhere on the body. It is a rare form of benign lipomatous lesion. Although there aren't many case reports, it could be difficult to identify chondroid lipomas before surgery. In this study, we reported a 33‐year‐old lady who had a lump on her right buttock that has been there for 6 years. The objective of this paper is to summarize the features and possible chondro‐lipoma diagnoses and to conduct a quick literature review.
2. CASE PRESENTATION
2.1. Personal and present history
We described a 33‐year‐old lady who underwent surgery 6 years after experiencing a painless growing tumor in her right buttock. She did not utilize any drugs and had no notable medical or family history. She was discovered to be alert, focused, afebrile, and neither pale nor icteric upon physical examination. A 6 cm smooth, fibro‐elastic, non‐adherent mass was seen at the right buttock. The evaluation of the nervous system was finished. The enlargement was not painful and had a distinct outline. Healthy skin was present above.
2.2. Investigations
A right gluteal subcutaneous fat magnetic resonance scan revealed an inflammatory mass as stranding with no drainable fluid larger than 6.7 × 4.5 × 8 cm (Figure 1). The surface lump was removed after the patient underwent an incisional biopsy during surgery. It was thought that a soft tissue cancer would be present because of a hard mass that was firmly attached to the tissues underneath. For the mass, pathology was requested. The surgical outcome was hampered by a localized wound infection. The patient made the decision not to have a complete excision. After 6 months, the patient's fears vanished.
FIGURE 1.
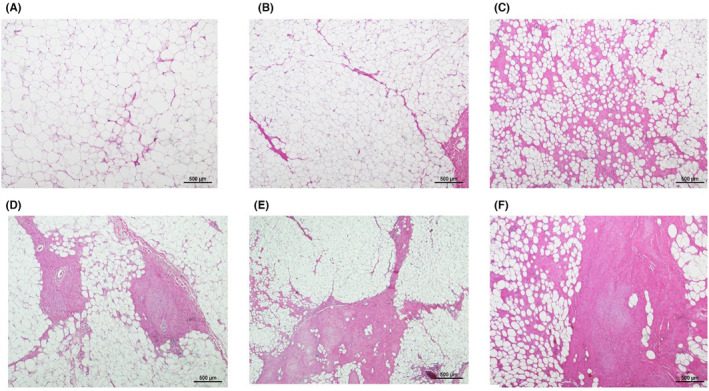
Histopathological images show mature fat cells arranged in lobules separated by connective fibrous tissue septa (A, B) (H&E stain, ×40) with focal cellular morphology (C) and thick walled blood vessels and chondroid matrix (D–F) (H&E stain, ×100).
3. GROSS SPECIMEN AND MICROSCOPIC PICTURE
The tumor was smooth, oily yellow, and 4 × 4 cm in size. Under a microscope, the tumor seemed to be made up of strands of multivacuolated cells and mature fat cells mixed together inside an abundance of chondroid and myxoid stroma. Pleomorphism and mitotic activity are absent from nuclei with a regular shape. (Figure 2).
FIGURE 2.

Histopathological images show that the lesion is composed of mature adipose tissue and myxohyaline chondroid matrix. No significant nuclear atypia or mitotic activity (A–D) (H&E stain, ×200).
3.1. Immunohistochemically
The S‐100 protein had a strong, broad cytoplasmic immunohistochemistry reactivity. Only a few scattered cells stained positively for CD68 in the cytoplasm. Ki67 nuclear staining was only positive in less than 5% of cells.
4. DISCUSSION
Lipomas are frequently movable tumors with defined edges. There is no consensus on its diagnosis or treatment. 1 They frequently include completely formed adipocytes. Numerous lipoma varieties have been documented, including osteolipoma, fibrolipoma, chondroid lipoma, angiolipoma, myolipoma, spindle cell lipoma, and chondroid lipoma. 2 Chondrolipomas are uncommon benign fatty mesenchymal tumors that have proliferating mature adipocytes and varied amounts of mature cartilaginous tissue. 3 , 4
Generally speaking, chondroid lipomas are a rare form of lipomas that were first identified in 1976. 5 In 1993, Meis and Enzinger described it as a separate entity. 6 A comparable tumor was reported as “an extra skeletal chondroma containing lipoblast‐like cells” by Chan et al. in 1986. 7 They are often located in the subcutaneous tissue, superficial muscular fascia, or skeletal muscles of the lip, tongue, and trunk and frequently present as a painless lump. 1 , 3 , 8 Given their potential for growth, they have a higher likelihood of being incorrectly diagnosed as sarcomas. They are normally 4 cm, but can be as little as 1.5–11 cm. 4 , 8 There is no overt racial or geographical bias, although there is a preference for those who are approximately 40 years old (42.85 16.97; median, 41). There are no overt sex differences. 1 Grossly chondroid lipomas are well‐circumscribed, lobulated, and occasionally encapsulated tumors that are generally 4 cm in diameter. The surface is golden and evenly cut. 8
Preadipocytes, mature adipocytes, prelipoblasts, and chondroblasts are among the adipocytes that make up the cells' ultrastructure, which varies from primitive to mature. 9 Chondroid lipomas are actually biphenotypic since they show lipoblastic differentiation and early cartilage features. 4 S‐100 protein, vimentin, and CD‐68 immunohistochemical staining are present on the tumor cells. In certain cases, focal keratin positivity has been discovered. 9
Its histological similarity to liposarcoma and chondrosarcoma, which have a poorer prognosis, overshadows the fact that chondroid lipoma is a clinically benign tumor. Six more Differential diagnosis of chondroid lipoma. Extra‐skeletal myxoid chondrosarcomas are smaller than chondroid lipomas and have a cord‐like arrangement of eosinophilic cells under the microscope. There are no adipose tissue or mature adipocytes. Chondroblasts are homogenous and show few intracytoplasmic vacuoles, whereas the tumor is lobulated and split by fibrous septa. In soft tissue chondroma, multi‐nucleate big cells are discernible as genuine hyaline cartilage. It is located in the hands' and feet's soft tissue and is devoid of fat vacuoles. 10 , 11 In a lipoma, cartilaginous metaplasia is shown to include real cartilage.
Patients with CL usually exhibit a lack of the usual imaging signals because of the unequal distribution of adipose tissues and cartilage‐like tissues in the CL matrix. There were mixed high and low signal intensities on T1WI and short‐time inversion recovery (STIR) sequences, high signal intensities on T2WI, and heterogeneous fat saturation on T2W fat‐saturated images. The low signal intensity on T1WI and the high signal intensity on T2WI are signs of the existence of chondroid tissue. The presence of fat tissue is indicated by the muted high‐intensity signals on T1WI on STIR images, which on fat‐saturated T2W images displays nonuniform fat saturation.
A limited role for ultrasonography in the detection of CL. 10 Pleomorphism, atypia, and the connection of the identified components (proportion, encapsulated, or superficial) to one another will all be important factors in the final diagnosis. Chondroid lipomas and their histological mimics can be distinguished via immunohistochemical investigation. In chondroid lipoma, S100 and vimentin are reactive indicators of tumor cells, whereas keratin, smooth muscle actin, muscle‐specific actin, and CD36 will not. 7 , 10 , 12
A needle biopsy can only sample a small portion of the tumor and examine the tissue architecture in order to evaluate local invasion. Incisional biopsy should be chosen for extensive pathological analysis. Furthermore, we highly urge sending the whole mass for extra examination after excision; nevertheless, the patient in our case report opted observation. 10
5. CONCLUSION
Finally, chondroid lipoma represents exceptional situations. It's critical to distinguish between sarcoma and chondrolipoma because severe surgery and postoperative radiation are choices for treating sarcoma, whereas surgery is an option for treating chondroid lipoma. There may not yet be a consensus on its prognosis or course of therapy.
AUTHOR CONTRIBUTIONS
Nuha Alsaleh: Conceptualization; data curation; formal analysis; methodology; resources; supervision; writing – original draft; writing – review and editing.
FUNDING INFORMATION
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
CONFLICT OF INTEREST STATEMENT
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests.
CONSENT
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
Alsaleh N. Chondroid lipoma that may mimic malignancy: A case report. Clin Case Rep. 2023;11:e8059. doi: 10.1002/ccr3.8059
DATA AVAILABILITY STATEMENT
All data underlying the results are available as part of the article and no additional source data are required.
REFERENCES
- 1. Huang C, Guo W, Qu W, Zhu Z, Li R. Characteristics of chondroid lipoma: a case report and literature review. Medicine. 2019;98(19):e15587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Raj V, Dwivedi N, Sah K, Chandra S. Chondrolipoma: report of a rare intra oral variant with review of histiogenetic concepts. J Oral Maxillofac Pathol. 2014;18(2):276‐280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Ezike KN, Okwudire‐Ejeh IA, Essien LO, et al. Chondrolipoma of the lip: a case report from a secondary health care center in Nigeria. Int J Case Rep Images. 2020;11:101147Z01KE2020. [Google Scholar]
- 4. Shawarby MA, El‐Maraghy MN, Salem RA, et al. Chondroid lipoma, a rare lipomatous tumor: report of two cases. Int J Case Rep Images. 2014;4:527‐531. [Google Scholar]
- 5. Furlong MA, Fanburg‐Smith JC, Childers EL. Lipoma of the oral and maxillofacial region: site and subclassification of 125 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98(4):441‐450. [DOI] [PubMed] [Google Scholar]
- 6. Meis JM, Enzinger FM, Chondroid lipoma . A unique tumor simulating liposarcoma and myxoid chondrosarcoma. Am J Surg Pathol. 1993;17(11):1103‐1112. [PubMed] [Google Scholar]
- 7. Chan J, Lee K, Saw D. Extraskeletal chondroma with lipoblast‐like cells. Hum Pathol. 1986;17(12):1285‐1287. [DOI] [PubMed] [Google Scholar]
- 8. Gokhale U, Pillai GR, Varghese P, et al. Chondroid lipoma: a case report. Oman Med J. 2008;23(2):116. [PMC free article] [PubMed] [Google Scholar]
- 9. Afroze IA, Sultana ZA. Chondroid lipoma–a rare lipomatous tumor: a case report. J Evol Med Dent Sci. 2015;4(62):10879‐10883. [Google Scholar]
- 10. Aloul AA, Savga S, Diaconu C, et al. Giant chondroid lipoma of the breast: a case report and literature review. Exp Ther Med. 2021;22(4):1‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Kapse SS, Surekha U, Javalgi AP. Chondroid lipoma in left thigh ‐a rare case report. J Clin Diagn Res. 2017;11(8):ED17‐ED18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. de Vreeze RS, van Coevorden F, Boerrigter L, et al. Delineation of chondroid lipoma: an immunohistochemical and molecular biological analysis. Sarcoma. 2011;2011:1‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data underlying the results are available as part of the article and no additional source data are required.