

Abstract
Introduction:
The transition to college is a period of elevated risk for a range of mental health conditions. Although colleges and universities strive to provide mental health support to their students, the high demand for these services makes it difficult to provide scalable, cost-effective solutions.
Objective:
To address these issues, the present study aims to compare the efficacy of three different treatments using a large cohort of 600 students transitioning to college. Interventions were selected based on their potential for generalizability and cost-effectiveness on college campuses.
Methods:
The study is a Phase II parallel-group, four-arm, randomized controlled trial with 1:1 allocation that will assign 600 participants to one (n = 150 per condition) of four arms: 1) group-based therapy, 2) physical activity program, 3) nature experiences, or 4) weekly assessment condition as a control group. Physiological data will be collected from all participants using a wearable device to develop algorithmic mental and physical health functioning predictions. Once recruitment is complete, modeling strategies will be used to evaluate the outcomes and effectiveness of each intervention.
Discussion:
The findings of this study will provide evidence as to the benefits of implementing scalable and proactive interventions using technology with the goal of improving the well-being and success of new college students.
Keywords: College Students, Wearables, Ecological Momentary Assessment, Stress, Young Adults
1. Introduction
The transition to college is a high-risk period with more than a third of students entering college with a mental health diagnosis [1]. The COVID-19 pandemic, increased academic demands, novel social pressures, and daily stressors have increased the risk for the development of major depression and generalized anxiety during the first year of college [2,3]. In response to these mental health demands, institutions of higher education need of programs to counteract these stressors and prevent the onset of such conditions at scale [4]. Preventative programs that focus on strategies to promote overall well-being and manage stress have shown promise [5,6]. Well-being is defined a sense of elevated positive affect, adaptive interpersonal relationships, and overall positive functioning in daily activities [7,8]. Meta-analyses have suggested that preventive programs delivered early in a college career can mitigate the likelihood of more severe adverse outcomes during the start of college [5]. However, the optimal models that can be used at scale remains unclear.
Two challenges towards developing prevention models for students transitioning to college are their cost and scale. Traditional mental health treatments often use one-on-one treatment models. Estimates suggest that 34% of college students seek mental health treatment [1]. This is likely an underestimate as many students who would benefit from mental health services do not seek them out or are unable to receive them [9]. To meet demand, a small university with 5,000 students would have approximately 1,500 students seeking services and need 50 or more mental health providers [10]. This demand highlights the need for scalable strategies to address the mental health needs of students transitioning to college.
The current study proposes three preventative interventions aimed at improving wellbeing for college students. First, group-based therapy that helps students acquire cognitive and behavioral skills to use adaptive behaviors such as cognitive restructuring, relaxation techniques, and sleep hygiene have been shown to be effective for depression, generalized anxiety, and chronic stress across a range of populations [11–13]. Recent meta-analyses have suggested that group-based therapy is highly effective at treating such conditions, including depression and generalized anxiety, in college students [14,15]. These interventions are cost-efficient when administered by peers or clinicians in training, when group sizes can accommodate larger (> 5) numbers, and appropriate supervision is available (Votta & Deldin, 2022). Despite these advantages, training is still needed to ensure group leaders can deliver the intervention with fidelity. Appropriate supervision of group leaders is necessary, which requires additional resources and infrastructure.
A second scalable strategy is regular physical activity. Meta-analyses and systematic reviews have demonstrated that regular physical activity is associated with improved physical and mental health outcomes [16,17]. The primary target of such interventions is an increased frequency of rigorous physical activity, as such activity engages multiple biological systems involved in well-being [18]. Many college campuses have fitness facilities and wellness programs available to students at low or no cost [19]. Thus, physical activity programs for students may also promote well-being and give students a means by which to manage stress. The costs associated with such programs include the maintenance of such facilities and the availability of trainers.
A third approach that has received less empirical attention in the literature, but may prove effective and cost-efficient, is exposure to the natural environment. Regular exposure to nature has been associated with increases in positive affect in college-aged samples [20,21]. There is evidence for a dose response relationship in that more time in green spaces is associated with larger increases positive affect [22,23]. Many college campuses have access to green spaces and nature conservation areas. Access to such areas may vary based on the urbanicity of an institution’s location, however. Nature-based programming can be student-run, done in a group setting, and require minimal additional costs to an institution or student. This approach has not yet been evaluated in a rigorous manner such that it remains unclear as to the efficacy of exposure to nature as a potential preventive intervention.
Determining the efficacy of such approaches requires an accurate assessment of the proposed targets for each intervention. Continuous monitoring via active data collection - those that require user input - may prove overly burdensome [24]. Passive data collection - data collected from wearable sensors requiring minimal user interaction – is useful in assessing the extent that each target is engaged. Such wearables can capture numerous indices of well-being including sleep, physical activity, and information about the environment in which an individual spends time [25]. Furthermore, passive data can be gathered for individuals across all intervention groups. Thus, it is possible to test the extent that target mechanism is associated with well-being beyond a given treatment package. For example, if time spent in nature is associated with well-being and all three groups increase their time spent in nature by going on a walk as part of behavioral activation, running in a forested area, or going on a hike, the outcomes of all groups may appear similar. However, these similar outcomes can be tied directly to the mechanism of interest, time in nature, and thus allow for a more precise conclusion to be drawn.
The present study, the Lived Experiences Measured Using Rings Study (LEMURS), aims to compare the efficacy of three treatments delivered to a large cohort of students transitioning to college. Participants will receive either 1) group-based therapy, 2) a physical activity program, 3) a nature experiences group, and 4) a weekly assessment condition (control group). It is hypothesized that all three active interventions will show increased well-being as well as reduced anxiety, depression, and stress relative to the control group. Based on the available prior evidence, it is hypothesized that the therapy and physical activity groups will report reduced anxiety, depression, and stress relative to the nature experiences group. However, there are meaningful differences in the costs needed to mount each group. The cost for each intervention will be tracked and compared at the conclusion Finally, passive data collected via a ring worn wearable and mobile devices will be collected on all participants. These data will be used to evaluate potential mechanisms of change across all intervention groups including engagement in positive activities, physical activity, and exposure to nature.
Methods
2.1. Trial Design
The study is a Phase II parallel-group, four-arm, randomized controlled trial with 1:1 allocation across treatment conditions to evaluate the efficacy and non-inferiority of three potential interventions to improve well-being during the transition to college (Figure 1). The trial was reviewed and approved by the University of Vermont Institutional Review Board and registered with Clinicaltrials.gov: NCT05841979.
Figure 1.
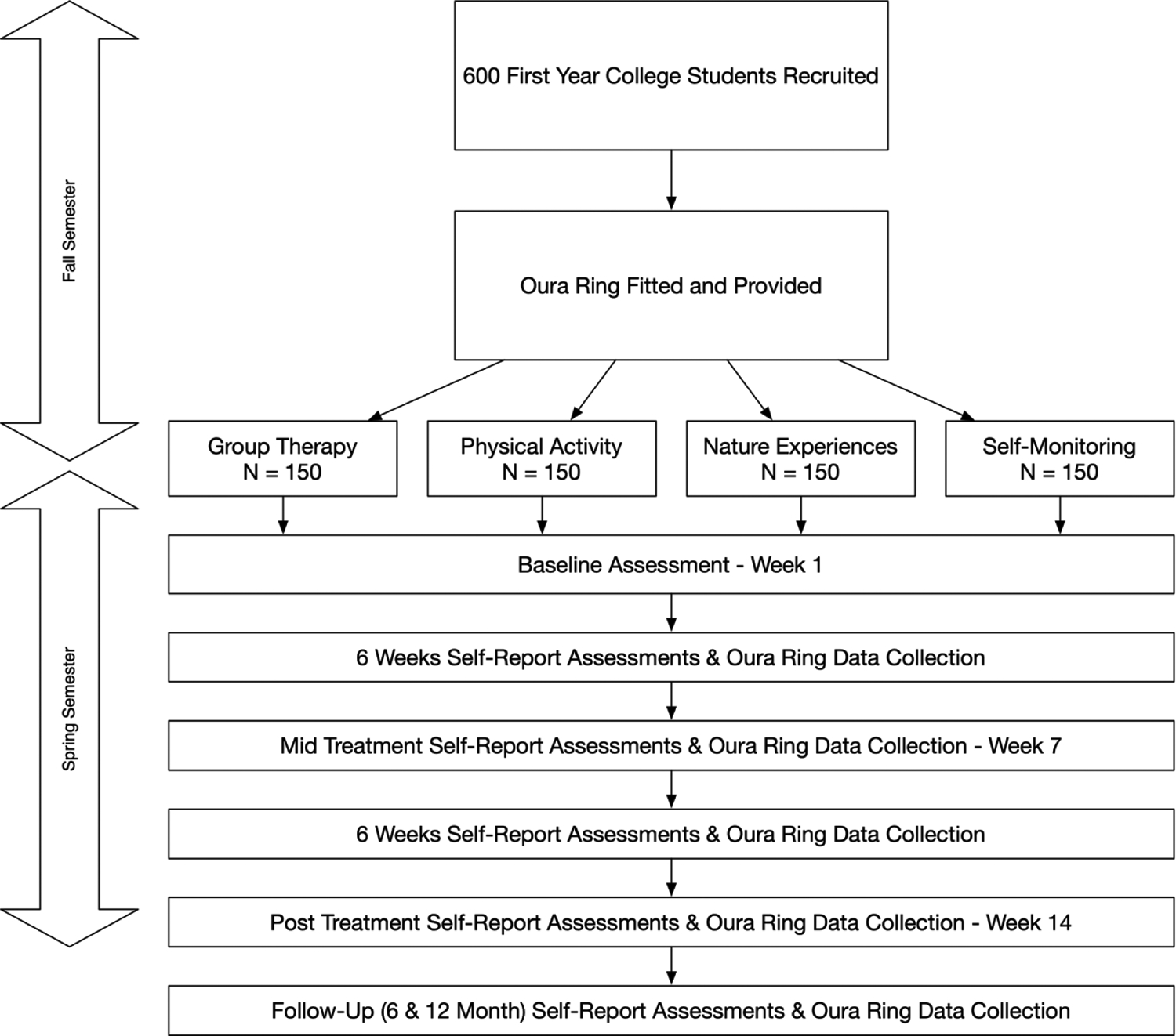
Diagram outlining the study flow.
2.2. Participants
Participants will be N = 600 undergraduate students in their first year at a public university. Inclusion criteria are to have a mobile device, be 18–24 years old, and a full-time student. Recruitment will occur via advertisements for a project assessing well-being throughout campus.
2.3. Recruitment and Randomization
Recruitment will be conducted remotely. Participants will scan a QR code from advertisement materials to access a brief eligibility survey. The survey will determine if they were in their first year and had a mobile device capable of running the mobile applications required for the study. Eligible participants will be sent an online consent form, a brief video summarizing the study along with the risks and benefits of participating, and a comprehension quiz. Enrollment will occur continuously in the Fall semester until the target sample size is obtained. Once participants are enrolled, they will attend a large in-person event with study staff to be oriented to the study. Participants will be randomized in blocks of eight by a study data analyst to allow for equal distribution across the conditions. Group assignment will be delivered the first week of the Spring semester.
2.4. Interventions
Participants (n = 150) will be randomized to the following four conditions (Table S1). All interventions will be delivered in-person.
2.4.1. Group Therapy
Participants randomized to the group therapy condition will receive a 14-week course of the Mood Lifters (ML) treatment protocol designed for undergraduate students. ML, a novel mental wellness program, was developed as a more accessible means to provide psychotherapy (Votta & Deldin, 2022). Meetings cover biopsychosocial areas and skills that were drawn from multiple established therapeutic interventions. Areas included addressing negative thoughts, problem-solving, building relationships, and behavioral activation. Work towards individualized goals and practice is implemented through a homework points system. Points are used as a tracking system for achieving behavioral goals such as improved sleep and mood. This system is designed to increase engagement by reducing the burden of tracking multiple behaviors and making the process of tracking enjoyable. Participants will share their points accrued each week as a means of assessing their use and engagement with the target skills used in the current intervention. In the current study, participants will be randomly assigned to groups of 15 members. Group sessions will occur weekly for one hour and review the predetermined weekly topic. The cost for an academic year of the Group Therapy group is estimated at $195,000 (Table S2).
ML is delivered by peer leaders who are individuals that have completed the program as well as a training program to improve its dissemination. Peer leaders will undergo a dedicated training program that involves completing a course of the Mood Lifters program, a workshop on the delivery of the ML program, and an evaluation with a live confederate to demonstrate competency. Additional information is available from the ML program (https://moodlifters.com/). Throughout the semester, therapists will receive weekly supervision from a licensed clinical psychologist. Adherence will be monitored using a checklist devised for each session to ascertain the number of session components that will be covered in each group.
2.4.2. Physical Activity
Participants randomized to the exercise arm will receive 14 weeks of a structured weekly strength and conditioning training program. The training program consists of three training sessions per week, with one being an in-person group session guided by a certified strength and conditioning specialist with the necessary training expertise to deliver the intervention. Specialists will be provided with a series of exercise routines and trained in their implementation. These routines are designed for general fitness and thus contain basic exercises that a certified conditioning specialists will be able to implement. The trainers will receive regular guidance from the athletic director. The other two training sessions are self-guided via the mobile app Trainheroic.
Each of the training sessions will follow a similar format. The sessions begin with a 10-minute warm-up. The session then shifts focus to general strength training (20 minutes) consisting of “circuit style” strength training movements (designed to develop strength and fitness at the same time). After the strength portion of the session, training shifts to a cardiorespiratory focus (20 minutes). Finally, the session concludes with a 10-minute cooldown period of static stretching exercises. Group-based adherence will be assessed using a checklist in which the interventionist determines the number of activities that were conducted in each session. Participants will also report their engagement in group and individual activities via the pre-made workout routine in TrainHeroic. The cost for an academic year of the Physical Activity group is estimated at $6,300 (Table S2).
2.4.3. Nature Experiences
Participants randomized to the Nature Experiences will participate in 14 weeks of group and self-directed activities to connect with the natural environment. The goal of the intervention is to spend three hours per week engaged with the natural environment. Weekly group activities will be led by Nature Guides, who are undergraduate and graduate students with extensive outdoor education training. The intervention will follow a manual that was created for the study that outlines activities to be conducted as a group each week. Prior to the start of the intervention, Nature Guides met with the developer of the manual to review each activity and general safety information. Locations for each activity were selected based on the number of natural elements with the goal of maximizing quality (e.g., minimal urban elements, large number of natural elements). Group activities will last one hour a week and include hiking in forests, observations in greenhouses, walking in parks, birdwatching, and present-centered mindfulness activities. Each activity will involve at least an hour in natural space. Hikes, walks, and observation activities involve spending time in areas with mostly natural elements with a focus on observing these elements. One session involves a mindfulness reflection while in a natural space that involved bringing awareness to the details of the environment. For their individual activities, participants will be given a list of self-directed activity suggestions each week. Adherence will be evaluated with an intervention specific checklist that will determine the type and number of activities that were conducted within each group session and self-reported activities via the Team LEMURS application. Exposure to nature will be monitored passively using a mobile application, NatureDose, that is described below. The cost of the Nature Experiences group is estimated at $2,940 (Table S2).
2.4.4. Weekly Assessment
The weekly assessment condition will not be asked to engage in any specific activities for a given week. This condition will only complete the weekly self-report assessments, have NatureDose on their mobile device, and sync their Oura Ring.
2.5. Assessments
Assessment data for the current study were conducted via mobile application and Oura rings. A study-specific mobile application named Team LEMURS (Figure 2) was created to manage remote data collection. The application will administer self-report instruments via Qualtrics, facilitate data synchronization via the Oura Ring App, provide overall communication with study participants, and encourage participation in the assigned interventions. The application will also be used to monitor adherences for all interventions. Each week, participants will endorse their attendance at their group-specific intervention meeting and if they engaged in individual intervention activities.
Figure 2.
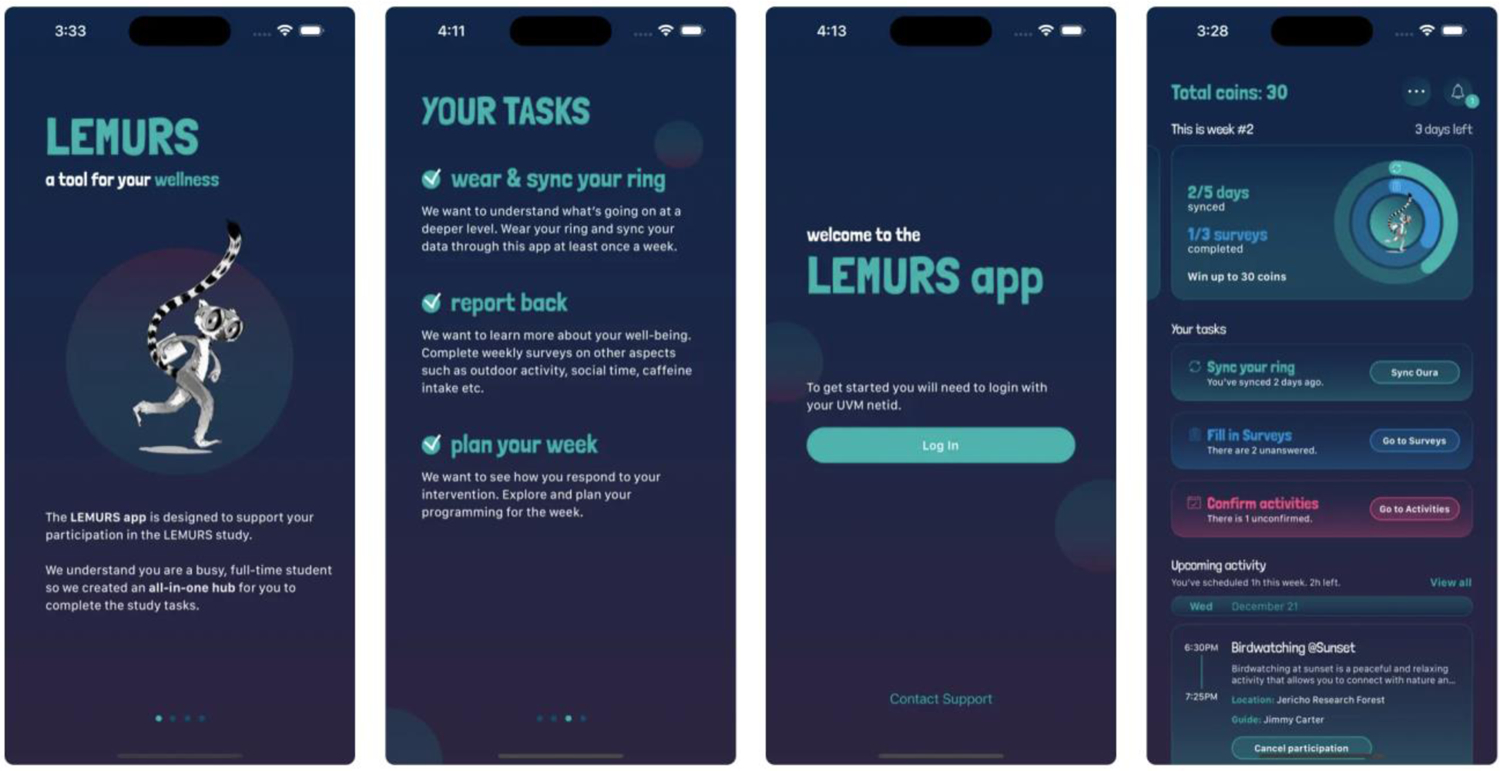
Images of the Team LEMURS Mobile Application to administer surveys and collect Oura Ring data.
2.5.2. Self-Report Assessments
Self-report assessments will be administered weekly via an embedded Qualtrics link within Team LEMURS. The length of the weekly assessment battery is 46 Likert Response questions. For Week 1, Week 7, Week 14, and follow-up assessments at month 6 and 12, additional measures will be added for a more comprehensive baseline, mid-treatment, and post-treatment assessment (Table 1). Unless otherwise specified, all measures referenced the past week.
Table 1.
Schedule of self-report assessments.
| Measures | 1 (Baseline) | 2 | 3 | 4 | 5 | 6 | 7 (Mid point) | 8 | 9 | 10 | 11 | 12 | 13 | 14 (Post Treatment) | Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Primary Outcomes | |||||||||||||||
| Well-Being: WEMWBS | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| Depression, Anxiety, Stress: DASS-21 | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| Stress: PSS | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| Secondary Outcomes | |||||||||||||||
| Sleep Quality | X | X | X | X | X | X | X | X | X | X | X | X | X | X | X |
| Social Support: MOSSS | X | X | X | X | |||||||||||
| Time Outside | X | X | X | X | X | X | X | X | X | X | X | X | X | X | |
| Substance Use: BSTAD | X | X | X | X |
Note: DASS-21 = Depression, Anxiety, Stress Scale −21. PSS = Perceived Stress Scale. WEMWBS = Warwick-Edinburgh Mental Well-being Scale. MOSSS = Medical Outcomes Social Support Scale. BSTAD = Brief Screener for Tobacco, Alcohol, and other Drugs.
Depression, Anxiety, Stress, Scale - 21 [DASS-21 26]:
The DASS-21 is designed to measure depression, anxiety, and stress. Higher scores indicate greater depression, anxiety, or stress. The DASS-21 has been shown to have accurately distinguish between depression, anxiety, and stress in diverse samples of those with a range of psychopathology [27]. Internal consistency and concurrent validity were found to be excellent in validation studies [27,28].
Perceived Stress Scale [PSS; 29]:
The PSS is a 10-item measure of stress associated with life events. Higher scores indicate greater stress. The PSS has excellent psychometric properties among college studies including high internal consistency, construct validity, and a replicable factor structure [30].
Sleep Quality Index (Snyder et al., 2018):
The Sleep Quality Index is a single-item self-report measure designed to assess the overall quality of sleep during the past week. Respondents indicate their quality of sleep on an 11-point scale ranging from “Terrible” to “Excellent.” The Sleep Quality Index has strong criterion validity as shown to have high correlations with mutli-item measures of sleep quality [31]. Furthermore, it accurately distinguished those with and without known sleep difficulties.
Warwick-Edinburgh Mental Well-being Scale (WEMWBS; Tennant et al., 2007):
The WEMWBS is a 14-item scale of mental well-being designed to measure subjective well-being and psychological functioning. Higher scores indicate greater well-being. Studies with the WEMWBS have shown that it has excellent internal consistency, high construct validity, and strong test-retest reliability [32]
Medical Outcomes Social Support Survey (MOSSS; Sherbourne & Stewart, 1991):
The MOSSS is a 19-item questionnaire that measures the level of the perceived social support across four dimensions: emotional/informational, tangible, positive social interaction, and affection. Higher scores indicate greater social support. The timeframe for the MOSSS was the past month. The MOSSS has shown to be one of the most well-established measures of perceived social support having shown construct validity in a range of populations [33,34]
Time Outside Survey:
The Time Outside Survey was developed for this specific study. It was modified and developed based on research studies examining activities conducted outdoors in nature [23,35–39]. Questions asked for self-reported information on the number of days spent outside, the average hours/minutes spent outside during these days, and the time of day these activities occurred.
Brief Screener for Tobacco, Alcohol, and other Drugs (BSTAD; Kelly et al., 2014):
The Brief Screening for Alcohol, Tobacco, and other Drugs questionnaire is a self-report measure designed to assess substance use amongst adolescents and young adults. The questionnaire asks about the use of a specific substance in the past month and the number days in which the substance was used. The BSTAD was developed by the National Institutes of Health to serve as a brief screener for substances among young adults (https://nida.nih.gov/bstad/).
2.5.3. Passive Data
Participants will be given an Oura ring for the study, a wearable device that contains three primary sensors: an infrared photoplethysmography sensor used to measure heart rate and respiration, a negative temperature coefficient sensor used to measure body temperature, and an accelerometer for measuring movement. [41,42]. These sensors are combined with algorithms and information obtained via a mobile device to derive measures of physical activity and sleep quality. Daily physical activity scores range from 0–100 and indicate the amount of physical activity and associated rest/inactivity for a given day [43]. Higher scores indicate an optimal balance between physically active periods and restful and recovery-based periods. Sleep scores also range from 0–100 with higher scores indicating better quality of sleep [41,44].
To gain more information on the types of outdoor environments in which participants spent time, all participants will use NatureDose [45]. NatureDose is a mobile application that assesses time spent in nature. This data is obtained from land and vegetation databases and air pollution indexes to quantify the quality of natural elements to derive a per-minute NatureScore that ranges from 0 (poor) to 100 (high). NatureScores are aggregated per week to indicate the quality and the duration of the nature to which they were exposed [45].
2.6. Data Analysis
The primary analyses for the current study will determine the superiority of intervention conditions to the weekly assessment group using an ITT sample. Differences between the active treatment conditions will be determined within a multilevel model framework to account for the longitudinal nature of the data. The level 2 model will include covariates such as housing location, medication status, and engagement in ongoing therapy. If a covariate is associated with outcomes, it will be evaluated as potential moderator of treatment response by including interaction terms between the covariate, treatment condition, and slope. The level 1 model will contain an intercept corresponding to the baseline assessment and coefficients for a slope using the 14 weeks of assessment. Hypotheses for group differences will be evaluated with a series of planned contrasts at level 2. For the WEMBS, a comparison between the active treatment conditions and the weekly assessment condition will be conducted. For the DASS 21 subscales, and PSS the contrasts will determine if (1) there is a difference between the active treatment conditions and weekly assessment condition and (2) if the group therapy and physical activity conditions had greater reductions than the nature experiences condition. Analyses using follow-up data will incorporate information obtained from the follow-up assessments into the linear model.
Follow-up analyses will examine potential mechanisms as obtained by wearables of treatment outcome for each intervention [46]. The mechanisms of interest are exposure to nature as measured by the NatureScore, physical activity as measured by the Oura ring physical activity score, and Mood Lifters points. The NatureScore and Oura data is obtained for all participants across all conditions. First, comparisons will be made between each treatment condition on each mechanism using a MLM. The intervention that was hypothesized to target a given mechanism will serve as the reference group for each analysis. These results will determine if a given intervention was associated with a change in each mechanism. Second, follow-up analyses will examine the association between each mechanism and treatment outcome within each intervention group. This second step will be performed for the group therapy condition with Mood Lifters points as these are not available for the other interventions.
As a final step, follow-up exploratory analyses will be conducted to identify potential moderators of treatment response for each condition that include /ethnicity, gender identity, and first-generation status. Finally, the costs associated with mounting each intervention will be compared. A sample size of 150 per condition (N = 600 total) provides sufficient power to detect group differences as small as 0.1 standard units with 0.80 power. With an expected attrition rate of 20%, it is still expected that the study will have sufficient power to detect differences among the conditions. There were no planned interim analyses or stopping guidelines.
3. Discussion
The described protocol outlines a four-arm randomized controlled trial to evaluate strategies to promote well-being during the transition to college. The transition to college is a developmental period full of dynamic changes and emotional turbulence [9]. Identifying feasible strategies to help students successfully manage that transition is a high priority for institutions of higher education. The interventions under evaluation in the current study have the potential to address this need in a cost-effective and scalable manner. The results will also ascertain which intervention has the greatest effect on different domains of well-being ranging from self-reported mental health to engagement in wellness behaviors.
The current study has several strengths. First, the study will use weekly self-report assessments of the primary outcome variables. This approach will allow for a greater understanding of the dynamics that students undergo during this transition to college. Second, the use of wearables permits the collection of large quantities of physiological data that require minimal user input. We are thus able to measure treatment targets for most of the interventions in all participants. This will allow us to determine the magnitude of the association between a given target and outcomes. Third, the remote sensors that are used are relatively low profile, provide high-quality measurements, and have a substantial battery life that can be used without regular charging throughout the day. Fourth, the sample will be recruited from the entire body of first-year college students as opposed to those who are specifically seeking treatment. Therefore, the results of the study, including outcome data and completion rates, are likely to be generalizable. Finally, the interventions that are used are all low-cost and utilize resources widely available to many institutions of higher education. Thus, the findings of the current study are likely to be disseminated should they support the hypotheses.
There are several limitations in the current trial as well. The well-being and mental health assessments are self-report, which is prone to bias. Self-report measures were selected due to the challenges of using interview or behavioral coding methods with large samples. The use of the wearable data also offsets these biases by providing objective data. Another limitation is the generalizability of data collected via Oura rings, which may be cost prohibitive at the time of this study. Furthermore, the nature experiences and group therapy arms are multi-component interventions that involve multiple activities. It may be unclear if a specific activity was effective relative to the whole treatment package. The current study was limited to full-time students who are of the typical age for the transition to college. These results may not fully generalize to part-time students or nontraditional students. The intervention will be deployed in the Spring semester of the participants’ first academic year as opposed to their first semester on campus. This was done for feasibility in that it will not be possible to implement the interventions and conduct recruitment prior to students arrival on campus.
The current study will be among the largest clinical trials to determine how to improve the transition to college. Recent events have made this period uniquely challenging, and there is a need for institutions of higher education to support newly enrolled students [3]. Devising strategies that are sustainable is key to providing the necessary support. The results of the present study will provide evidence for different strategies that are generalizable and scalable.
Supplementary Material
Highlights.
The transition to college has become increasingly difficult for a wide range of students.
Institutions of higher education struggle to meet the demands for mental health treatment.
Interventions that are cost-effective and can be delivered at scale are needed.
Objective measures of well-being, such as those obtained by wearables, may inform the delivery of such interventions.
Three interventions will be evaluated including a peer-led group therapy, a physical activity group, and a nature exposure group.
Acknowledgements
This study was supported by a MassMutual Center of Excellence Award to C. Danforth and NIH K23MH123031 (PI: E. McGinnis).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- [1].Lipson SK, Lattie EG, Eisenberg D, Increased Rates of Mental Health Service Utilization by U.S. College Students: 10-Year Population-Level Trends (2007–2017), PS. 70 (2019) 60–63. 10.1176/appi.ps.201800332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Aristovnik A, Keržič D, Ravšelj D, Tomaževič N, Umek L, Impacts of the COVID-19 Pandemic on Life of Higher Education Students: A Global Perspective, Sustainability. 12 (2020) 8438. 10.3390/su12208438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Copeland WE, McGinnis E, Bai Y, Adams Z, Nardone H, Devadanam V, Rettew J, Hudziak JJ, Impact of COVID-19 Pandemic on College Student Mental Health and Wellness, Journal of the American Academy of Child & Adolescent Psychiatry. 60 (2021) 134–141.e2. 10.1016/j.jaac.2020.08.466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Watson JC, Rethinking the Provision of Counseling Services: A Paradigm Shift for College Counselors, Journal of College Counseling. 16 (2013) 3–5. 10.1002/j.2161-1882.2013.00022.x. [DOI] [Google Scholar]
- [5].Conley CS, Durlak JA, Dickson DA, An Evaluative Review of Outcome Research on Universal Mental Health Promotion and Prevention Programs for Higher Education Students, Journal of American College Health. 61 (2013) 286–301. 10.1080/07448481.2013.802237. [DOI] [PubMed] [Google Scholar]
- [6].Smith TB, Dean B, Floyd S, Silva C, Yamashita M, Durtschi J, Heaps RA, Pressing Issues in College Counseling: A Survey of American College Counseling Association Members, Journal of College Counseling. 10 (2007) 64–78. 10.1002/j.21611882.2007.tb00007.x. [DOI] [Google Scholar]
- [7].Stewart-Brown SL, Platt S, Tennant A, Maheswaran H, Parkinson J, Weich S, Tennant R, Taggart F, Clarke A, The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): a valid and reliable tool for measuring mental well-being in diverse populations and projects, J Epidemiol Community Health. 65 (2011) A38–A39. 10.1136/jech.2011.143586.86. [DOI] [Google Scholar]
- [8].Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, Parkinson J, Secker J, Stewart-Brown S, The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): development and UK validation, Health and Quality of Life Outcomes. 5 (2007) 63. 10.1186/1477-7525-5-63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Castillo LG, Schwartz SJ, Introduction to the Special Issue on College Student Mental Health, Journal of Clinical Psychology. 69 (2013) 291–297. 10.1002/jclp.21972. [DOI] [PubMed] [Google Scholar]
- [10].Schueller SM, Washburn JJ, Price M, Exploring mental health providers’ interest in using web and mobile-based tools in their practices, Internet Interventions. 4 (2016) 145–151. 10.1016/j.invent.2016.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Roberts JS, Ferber RA, Funk CN, Harrington AW, Maixner SM, Porte JL, Schissler P, Votta CM, Deldin PJ, Connell CM, Mood Lifters for Seniors: Development and Evaluation of an Online, Peer-Led Mental Health Program for Older Adults, Gerontol Geriatr Med. 8 (2022) 23337214221117430. 10.1177/23337214221117431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Uliaszek AA, Rashid T, Williams GE, Gulamani T, Group therapy for university students: A randomized control trial of dialectical behavior therapy and positive psychotherapy, Behaviour Research and Therapy. 77 (2016) 78–85. 10.1016/j.brat.2015.12.003. [DOI] [PubMed] [Google Scholar]
- [13].Votta CM, Deldin PJ, Mood Lifters: evaluation of a novel peer-led mental wellness program, Mental Health Review Journal. ahead-of-print (2022). 10.1108/MHRJ-11-2021-0084. [DOI] [Google Scholar]
- [14].Cuijpers P, Cristea IA, Ebert DD, Koot HM, Auerbach RP, Bruffaerts R, Kessler RC, Psychological Treatment of Depression in College Students: A Metaanalysis, Depression and Anxiety. 33 (2016) 400–414. 10.1002/da.22461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Janis RA, Burlingame GM, Svien H, Jensen J, Lundgreen R, Group therapy for mood disorders: A meta-analysis, Psychotherapy Research. 31 (2021) 342–358. 10.1080/10503307.2020.1817603. [DOI] [PubMed] [Google Scholar]
- [16].Morres ID, Hatzigeorgiadis A, Stathi A, Comoutos N, Arpin-Cribbie C, Krommidas C, Theodorakis Y, Aerobic exercise for adult patients with major depressive disorder in mental health services: A systematic review and meta-analysis, Depression and Anxiety. 36 (2019) 39–53. 10.1002/da.22842. [DOI] [PubMed] [Google Scholar]
- [17].Stathopoulou G, Powers MB, Berry AC, Smits JAJ, Otto MW, Exercise Interventions for Mental Health: A Quantitative and Qualitative Review, Clinical Psychology: Science and Practice. 13 (2006) 179–193. 10.1111/j.1468-2850.2006.00021.x. [DOI] [Google Scholar]
- [18].Smith PJ, Merwin RM, The Role of Exercise in Management of Mental Health Disorders: An Integrative Review, Annual Review of Medicine. 72 (2021) 45–62. 10.1146/annurev-med-060619-022943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Strand B, Egeberg J, Mozumdar A, The Prevalence and Characteristics of Wellness Programs and Centers at Two-Year and Four-Year Colleges and Universities, Recreational Sports J. 34 (2010) 45–57. 10.1123/rsj.34.1.45. [DOI] [Google Scholar]
- [20].Brymer E, Rogerson M, Barton J, Nature and Health: Physical Activity in Nature, Routledge, 2021. [Google Scholar]
- [21].Patwary MM, Dzhambov A, Disha AS, Bardhan M, Haque MZ, Rahman MA, Tareq MF, Browning MHEM, Larson LR, Alam MA, Labib SM, Shuvo FK, Parkinson C, Exposure to nature during the COVID-19 pandemic and the associated effect on mental health: a systematic review with meta-analysis, The Lancet Planetary Health. 6 (2022) S20. 10.1016/S2542-5196(22)00282-0. [DOI] [Google Scholar]
- [22].Fuegen K, Breitenbecher KH, Walking and Being Outdoors in Nature Increase Positive Affect and Energy, Ecopsychology. 10 (2018) 14–25. 10.1089/eco.2017.0036. [DOI] [Google Scholar]
- [23].White MP, Alcock I, Grellier J, Wheeler BW, Hartig T, Warber SL, Bone A, Depledge MH, Fleming LE, Spending at least 120 minutes a week in nature is associated with good health and wellbeing, Sci Rep. 9 (2019) 7730. 10.1038/s41598-01944097-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Price M, van Stolk-Cooke K, Brier ZMF, Legrand AC, mHealth solutions for early interventions after trauma: improvements and considerations for assessment and intervention throughout the acute post-trauma period, Mhealth. 4 (2018). 10.21037/mhealth.2018.06.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Gurchiek RD, Cheney N, McGinnis RS, Estimating Biomechanical Time-Series with Wearable Sensors: A Systematic Review of Machine Learning Techniques, Sensors. 19 (2019) 5227. 10.3390/s19235227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Henry JD, Crawford JR, The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample, British Journal of Clinical Psychology. 44 (2005) 227–239. 10.1348/014466505X29657. [DOI] [PubMed] [Google Scholar]
- [27].Antony MM, Bieling PJ, Cox BJ, Enns MW, Swinson RP, Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample, Psychological Assessment. 10 (1998) 176–181. 10.1037/1040-3590.10.2.176. [DOI] [Google Scholar]
- [28].Norton PJ, Depression Anxiety and Stress Scales (DASS-21): Psychometric analysis across four racial groups, Anxiety, Stress, & Coping. 20 (2007) 253–265. 10.1080/10615800701309279. [DOI] [PubMed] [Google Scholar]
- [29].Cohen S, Kamarck T, Mermelstein R, A Global Measure of Perceived Stress, Journal of Health and Social Behavior. 24 (1983) 385–396. 10.2307/2136404. [DOI] [PubMed] [Google Scholar]
- [30].Roberti JW, Harrington LN, Storch EA, Further Psychometric Support for the 10-Item Version of the Perceived Stress Scale, Journal of College Counseling. 9 (2006) 135–147. 10.1002/j.2161-1882.2006.tb00100.x. [DOI] [Google Scholar]
- [31].Snyder E, Cai B, DeMuro C, Morrison MF, Ball W, A New Single-Item Sleep Quality Scale: Results of Psychometric Evaluation in Patients With Chronic Primary Insomnia and Depression, Journal of Clinical Sleep Medicine. 14 (2018) 1849–1857. 10.5664/jcsm.7478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Clarke A, Friede T, Putz R, Ashdown J, Martin S, Blake A, Adi Y, Parkinson J, Flynn P, Platt S, Stewart-Brown S, Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Validated for teenage school students in England and Scotland. A mixed methods assessment, BMC Public Health. 11 (2011) 487. 10.1186/1471-2458-11-487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Merino-Soto C, Núñez Benítez MÁ, Domínguez-Guedea MT, Toledano-Toledano F, Moral de la Rubia J, Astudillo-García CI, Rivera-Rivera L, Leyva-López A, Angulo-Ramos M, Flores Laguna OA, Hernández-Salinas G, Rodríguez Castro JH, González Peña OI, Garduño Espinosa J, Medical outcomes study social support survey (MOS-SSS) in patients with chronic disease: A psychometric assessment, Frontiers in Psychiatry. 13 (2023). https://www.frontiersin.org/articles/10.3389/fpsyt.2022.1028342 (accessed August 17, 2023). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Priede A, Andreu Y, Martínez P, Conchado A, Ruiz-Torres M, González-Blanch C, The factor structure of the Medical Outcomes Study–Social Support Survey: A comparison of different models in a sample of recently diagnosed cancer patients, Journal of Psychosomatic Research. 108 (2018) 32–38. 10.1016/j.jpsychores.2018.02.008. [DOI] [PubMed] [Google Scholar]
- [35].Bratman GN, Hamilton JP, Hahn KS, Daily GC, Gross JJ, Nature experience reduces rumination and subgenual prefrontal cortex activation, Proceedings of the National Academy of Sciences. 112 (2015) 8567–8572. 10.1073/pnas.1510459112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Colléony A, Shwartz A, Beyond Assuming Co-Benefits in Nature-Based Solutions: A Human-Centered Approach to Optimize Social and Ecological Outcomes for Advancing Sustainable Urban Planning, Sustainability. 11 (2019) 4924. 10.3390/su11184924. [DOI] [Google Scholar]
- [37].Diffey BL, Is casual exposure to summer sunlight effective at maintaining adequate vitamin D status?, Photodermatol Photoimmunol Photomed. 26 (2010) 172–176. 10.1111/j.1600-0781.2010.00518.x. [DOI] [PubMed] [Google Scholar]
- [38].Pasanen TP, White MP, Wheeler BW, Garrett JK, Elliott LR, Neighbourhood blue space, health and wellbeing: The mediating role of different types of physical activity, Environment International. 131 (2019) 105016. 10.1016/j.envint.2019.105016. [DOI] [PubMed] [Google Scholar]
- [39].Ulrich RS, Simons RF, Losito BD, Fiorito E, Miles MA, Zelson M, Stress recovery during exposure to natural and urban environments, Journal of Environmental Psychology. 11 (1991) 201–230. 10.1016/S0272-4944(05)80184-7. [DOI] [Google Scholar]
- [40].Zatzick DF, Kang S-M, Hinton WL, Kelly RH, Hilty DM, Franz CE, Le L, Kravitz RL, Posttraumatic concerns: A patient-centered approach to outcome assessment after traumatic physical injury., Medical Care. 39 (2001) 327–339. [DOI] [PubMed] [Google Scholar]
- [41].Altini M, Kinnunen H, The Promise of Sleep: A Multi-Sensor Approach for Accurate Sleep Stage Detection Using the Oura Ring, Sensors. 21 (2021) 4302. 10.3390/s21134302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].de Zambotti M, Rosas L, Colrain IM, Baker FC, The Sleep of the Ring: Comparison of the ŌURA Sleep Tracker Against Polysomnography, Behavioral Sleep Medicine. 17 (2019) 124–136. 10.1080/15402002.2017.1300587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Kristiansson E, Fridolfsson J, Arvidsson D, Holmäng A, Börjesson M, Andersson-Hall U, Validation of Oura ring energy expenditure and steps in laboratory and free-living, BMC Medical Research Methodology. 23 (2023) 50. 10.1186/s12874-023-01868-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Willoughby AR, Alikhani I, Karsikas M, Chua XY, Chee MWL, Country differences in nocturnal sleep variability: Observations from a large-scale, long-term sleep wearable study, Sleep Medicine. 110 (2023) 155–165. 10.1016/j.sleep.2023.08.010. [DOI] [PubMed] [Google Scholar]
- [45].Bardhan M, Zhang K, Browning MHEM, Dong J, Liu T, Bailey C, McAnirlin O, Hanley J, Minson CT, Mutel RL, Ranganathan S, Reuben A, Time in nature is associated with higher levels of positive mood: Evidence from the 2023 NatureDose™ student survey, Journal of Environmental Psychology. 90 (2023) 102083. 10.1016/j.jenvp.2023.102083. [DOI] [Google Scholar]
- [46].Insel TR, Gogtay N, National institute of mental health clinical trials: New opportunities, new expectations, JAMA Psychiatry. (2014). 10.1001/jamapsychiatry.2014.426. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.