

Abstract
Background
Patient perceptions of primary care telephone and video telemedicine and whether COVID-19 pandemic-related telemedicine exposure shifted patients’ visit preference is unknown.
Objectives
We examined patient surveys to understand the health care experience of patients seeking primary care via telemedicine and how patients expected their preferences to shift as a result of the COVID-19 pandemic.
Research Design/Subjects
In an integrated delivery system that shifted to a “telemedicine-first” health care model during the COVID-19 pandemic, we sampled monthly and collected 1000 surveys from adults with primary care telemedicine visits scheduled through the online patient portal between 3/16/2020-10/31/2020.
Measures
Participants reported their preferred primary care visit modality (telephone, video or in-person visits) across three time points: before, during and (hypothetically) after the COVID-19 pandemic, and reported their general assessment of primary care visits during the pandemic.
Results
The majority of participants preferred in-person visits before (69%) and after the COVID-19 pandemic (57%). However, most participants reported a preference for telemedicine visits during the pandemic and continue to prefer telemedicine visits at a 12% higher rate post-pandemic. Many participants (63%) expressed interest in using telemedicine at least some of the time. Among participants reporting a recent telemedicine visit, 85% agreed that the visit addressed their health needs.
Conclusion
As primary care visit modality preferences continue to evolve, patients anticipate that they will continue to prefer telemedicine visits, both video and telephone, at an increased rate than before the COVID-19 pandemic.
Keywords: Telemedicine, telephone visits, video visits, primary care
Introduction
Increases in telemedicine use early in the COVID-19 pandemic have been widely documented[1–5]. While expansions in telemedicine use will likely persist post-pandemic [3, 4, 6, 7] there is limited evidence about how patient preferences and perceptions differ between telephone and video telemedicine in primary care[8] and how preferences will continue to shift post-pandemic. Additionally, while temporary provisions provided pandemic coverage during telemedicine expansions, longer term reimbursement is unclear, including across multiple types of virtual care[9, 10].
Video visits can improve communication and provide insights via visual information not available during telephone visits[2], but also pose additional barriers. Successful completion requires that patients and clinicians have the skills and technical requirements (i.e., video-enabled device and internet connection)[11, 12] . Patients lacking these resources may rely on telephone visits when in-person visits are not available or accessible. Regardless of technology access, patients also have personal preferences for the type of telemedicine visit they would choose, which may vary by specific concern[13]. Some patients prefer telephone to limit the need to prepare themselves or their surroundings, while others value the visual information conveyed[14] and increased personal interaction of a video visit.
While in-person visits were historically the dominant modality of health care visits[15], the pandemic created a natural experiment, with novel telemedicine exposure for a substantial proportion of patients. Given the benefits of video and telephone visits, each will likely play a greater role in primary care delivery moving forward than during pre-pandemic times. As future telemedicine use evolves, understanding patients’ experiences can inform primary care best practices and policy decisions. We examined patients’ surveys to understand the health care experience for patients seeking primary care as well as how pandemic-related telemedicine exposure was associated with changes in visit mode preferences.
Methods
Study setting
We compared survey responses between participants with a telephone or video visit during the early COVID-19 pandemic period at Kaiser Permanente Northern California (KPNC), a large integrated delivery system (IDS) with about 4.5 million members. Since 2016, KPNC members can self-select between in-person, telephone or video visits when scheduling primary care visits using the patient portal[16, 17]. During the study period, to limit COVID-19 exposure, KNPC shifted to a “telemedicine-first” health care model[18, 19], where referral for in-person visits required an initial telemedicine visit.
Study population and Data Collection
We collected 1000 completed surveys (among 1680 eligible participants) from a random sample of all patient-initiated telemedicine visits in adult primary care (equal numbers of telephone and video visits) scheduled between 3/16/2020-10/31/2020 through the portal website or mobile applications. Patients were not eligible if they were unable to complete an English-language survey (due to language, hearing, or cognitive barrier), left the health plan, or had no contact information (n=175).
Starting April 2020, an introductory message (email and letter), a mailed paper questionnaire and a personalized link to the electronic survey were sent to potential participants. Participants completed the same survey questions by their choice of mail (18%), online (76%), or telephone interview (6%). Non-responders were contacted by phone to encourage completion. A $10 gift card was sent after survey completion.
Survey
Participants were asked via multiple choice and free response about: visit modality preference (telephone, video or in-person visits) for primary care before, during and (hypothetically) post-pandemic; barriers to, and experience of, primary care visits during the pandemic; and whether telemedicine addressed their needs. Most respondents reported a telemedicine visit within the past 12 months (649 with a video visit and 298 with a telephone visit) and responded to questions about that telemedicine visit experience (see appendix S1 for survey question examples).
Data Analysis
We described patient characteristics and examined patient-reported preference for visit modality by estimating the proportion of participants who reported preferring in-person, telephone and video visits before, during and (hypothetically) post-pandemic. We used a Sankey diagram to illustrate the shift in visit modality preference across the trajectory of the pandemic by plotting the proportion of participants (represented by line thickness) preferring each visit type post-pandemic by preference for visit type pre-pandemic [20, 21]. Among those preferring in-person visits pre-pandemic we examined the shift in post-pandemic visit modality preference by patient characteristics. We also examined the proportion of patients who agreed with statements about their experiences with telemedicine and barriers for in-person, telephone and video visits. All analyses were weighted by sampling weights and non-response weights (based on age and sex), and comparison [22] used Rao-Scott Chi-Squared Test[23]. A threshold of .05 (two-tailed) was used to determine statistical significance.
Two study staff independently assigned free-text responses describing patient visit modality preference to one of 6 primary codes based on the visit preference pattern. A secondary code was given when flexibility in visit mode preference was indicated (see Table 2 for frequencies and a description of each preference pattern). Discrepancies were resolved by consensus.
Table 2.
Representative free-text responses for reason for primary care visit mode preference by key themes.
| PREFERS IN-PERSON AFTER THE PANDEMIC | n |
|---|---|
| Consistently prefers in-person visits (before, during, after COVID) | 173 |
|
“Because I cannot get a comprehensive examination through video or telephone”
“Nothing takes the place of a face to face visit. It’s what I’m used to” |
|
| Usually prefers in-person, but prefers telemedicine during pandemic | 253 |
|
“After the crisis is 100% over and it’s safe to be social outside with others, I would prefer in-person visits as I can physically describe to my doctor things I can’t describe with words … “
“as soon as I feel safe I would prefer an in person visit as I find it more convenient and more effective” |
|
| Initially prefers telemedicine, prefers in-person after (or during and after) the pandemic | 37 |
|
“I would like to see my doctor at least once a year. I like my doctor”
“I have had to wait on eye surgery” |
|
| Preference for in-person visits after the pandemic, but open to telemedicine | 128 |
|
“If I am just renewing an Rx or something simple, a phone visit is fine”
“This is a hard question. For many things in person is better, but sometimes a video visit will work just as well. Once in awhile a phone call or email works. I like having a choice” |
|
| Visit type preference varies, case-by-case | 43 |
| “It all depends on the issue” | |
| “I think depends on the severity. If it was something I think a doctor needed to do a physical exam on in order to have better idea of my symptoms then I would say in person.” | |
| PREFERS TELEMEDICINE AFTER THE PANDEMIC | |
| Initially prefers in-person, prefers Telemedicine after pandemic | 144 |
|
“Prior to COVID-19, I was unaware of the video visit. Now that I’ve used it, I don’t want to go back to in-person visits unless it is necessary””
“I was pleased with my video visit. I would do more now that I have had the experience. I like that I don’t have to drive or worry about parking |
|
| Consistently prefers Telemedicine | 246 |
|
“Not everything needs to be in-person and driving to a medical office is not always convenient”
“If I can get care with a video or telephone visit, then I do not have to get a babysitter or take young kids in the car with me to a medical facility” |
The Institutional Review Board of the Kaiser Foundation Research Institute approved the study protocol and materials and waived the requirement for participant written informed consent.
Results
Among 1,000 adult survey respondents (response rate 60%), 41.6% were aged ≥60 years, 39.8% male, 50.4% of non-Hispanic White race/ethnicity and 60.1% had a household income of <$60,000 (Table 1).
Table 1.
Among patients with video or telephone visits during 03/16/2020-08/31/2020)
| Patient Characteristics | (n=1,000) | Col % | Weighted % | |
|---|---|---|---|---|
| Age | 18-39 | 203 | 20.3% | 21.5% |
| 40-59 | 381 | 38.1% | 37.0% | |
| 60+ | 416 | 41.6% | 41.5% | |
|
| ||||
| Gender | Male | 398 | 39.8% | 43.6% |
|
| ||||
| Race/ethnicity | White | 504 | 50.4% | 51.9% |
| Black | 78 | 7.8% | 5.9% | |
| Hispanic | 107 | 10.7% | 11.0% | |
| Asian | 146 | 14.6% | 17.5% | |
| Multi Race | 70 | 7.0% | 6.4% | |
| Other | 54 | 5.4% | 4.3% | |
|
| ||||
| Overall Health | Excellent/Very good | 393 | 40.6% | 42.7% |
| Good | 375 | 38.7% | 38.4% | |
| Fair | 169 | 17.4% | 17.1% | |
| Poor/Very Poor | 32 | 3.3% | 1.9% | |
|
| ||||
| Education | High school graduate or less | 166 | 17.1% | 14.7% |
| Some college | 304 | 31.4% | 29.6% | |
| College graduate | 239 | 24.7% | 27.8% | |
| Some graduate school or more | 258 | 26.7% | 27.9% | |
|
| ||||
| Income | Less than $40,000 | 196 | 21.4% | 19.8% |
| $40,000-less than $60,000 | 123 | 38.7% | 38.4% | |
| $60,000-$99,999 | 239 | 17.4% | 17.1% | |
| $100,000 or more | 358 | 39.1% | 40.5% | |
The race/ethnicity of 41 participants, overall health of 31 participants; education of 33 participants, and income of 84 participants was unknown
Participants reported their visit modality preference for a health concern that could be helped by an in-person, video or telephone visit before, during and after the COVID-19 pandemic. Figure 1 shows the visit mode preference shifts pre-pandemic versus post-pandemic. Most participants preferred in-person visits before (69%) and expected to prefer in-person visits post-pandemic (57%).
Figure 1.
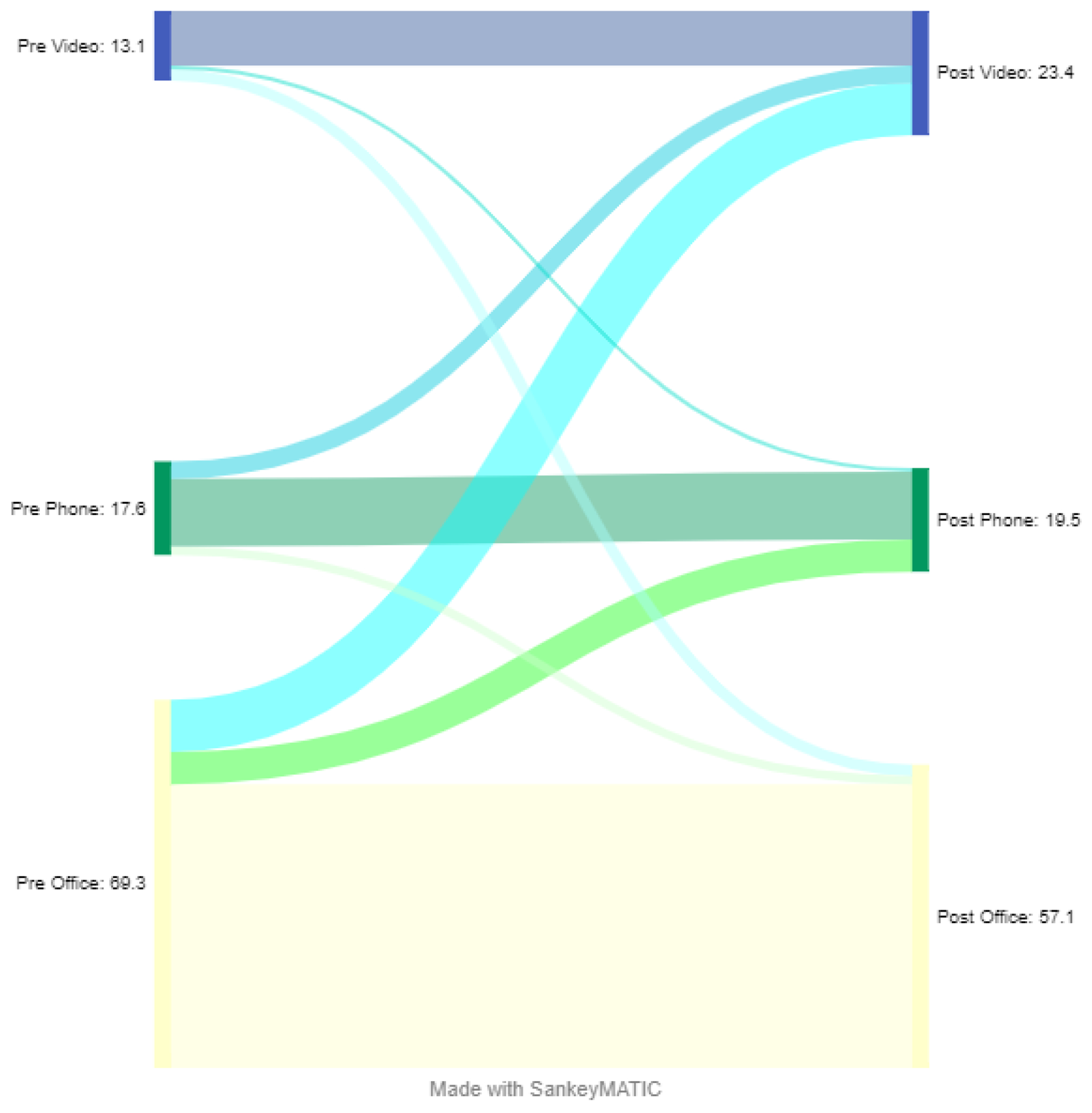
Participant-reported pandemic related visit modality preference shifts
During the pandemic, preference for in-person visits decreased to 23% (p<0.001, appendix S2) and preference for both video and telephone visits increased. Participants expect to sustain a 12% increased preference for telemedicine post-pandemic, mostly for video visits (a 10% increase compared to a 2% increase for telephone).
Key quotes from open-ended responses illustrating visit modality preference shifts towards telemedicine are listed in Table 2. For example:
“Prior to COVID-19, I was unaware of the video visit. Now that I’ve used it, I don’t want to go back to in-person visits unless it is necessary.”
“I was pleased with my video visit. I would do more now that I have had the experience. I like that I don’t have to drive or worry about parking.”
Less commonly (4.1% of open-ended responses), key quotes illustrate a shift away from telemedicine to in-person visits post-pandemic, in some cases to facilitate connection with the doctor or for delayed non-urgent in-person care. For example:
“I would like to see my doctor at least once a year. I like my doctor.”
“I have had to wait on eye surgery.”
Among 896 respondents who provided an open-ended response, the majority (63%) described openness to a mix of different visit types moving forward. For example, a participant who prefers in-person visits post-pandemic, offered:
“If I am just renewing an Rx or something simple, a phone visit is fine.”
Figure 2 shows post-pandemic preference shifts to telephone or video telemedicine by patient characteristic among 642 patients who preferred an in-person visit pre-pandemic. Household income was significantly associated with changes in preference post-pandemic. Differences in preference shifts do not reach statistical significance by patient race/ethnicity, prior video experience, age and internet access. While descriptively more Hispanic participants reported shifting toward telephone rather than video visits post-pandemic, more participants identifying as Asian, White, Black or another race reported shifting to video visits post-pandemic (appendix S3).
Figure 2.
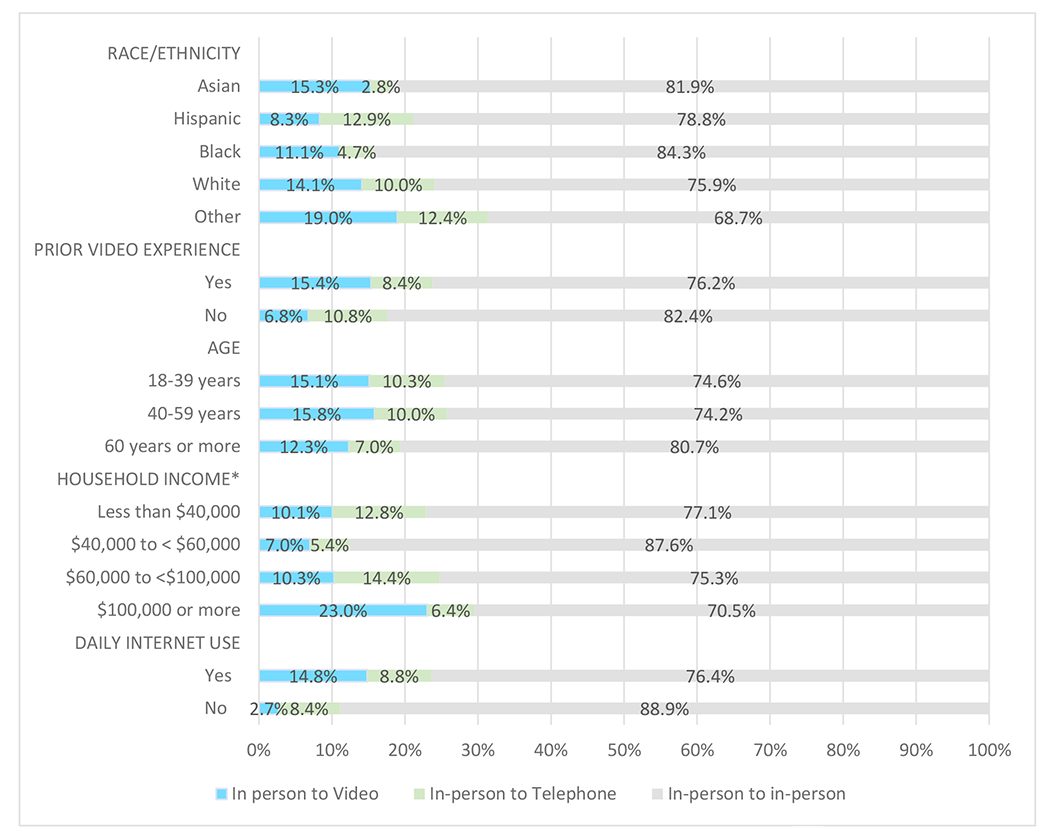
Among participants initially preferring in-person visits: Post-pandemic shifts in visit modality preference by patient characteristics
* Shifts in visit modality preference was significantly associated with household income.
Among all participants, 60% delayed non-urgent care and 31% reported that limited access to in-person visits prevented them from getting care. However, 88% agreed with the statement, “because my doctor shifted toward phone or video visits (to protect patients from COVID-19) I was able to get the care I need without spreading or being exposed to germs” and 80% agreed that telemedicine addressed their health needs as well as an in-person visit when a physical exam is not needed (appendix S4).
Among participants reporting a video visit in the past 12 months, 25% had technical difficulties and 12% said it was complicated to set up their device (data not shown). However, 85% of participants with a recent video (n=649) or telephone visit (n=298) said the visit addressed their health needs and nearly two-thirds of patients said that their health improved because of the visit (Figure 3).
Figure 3.
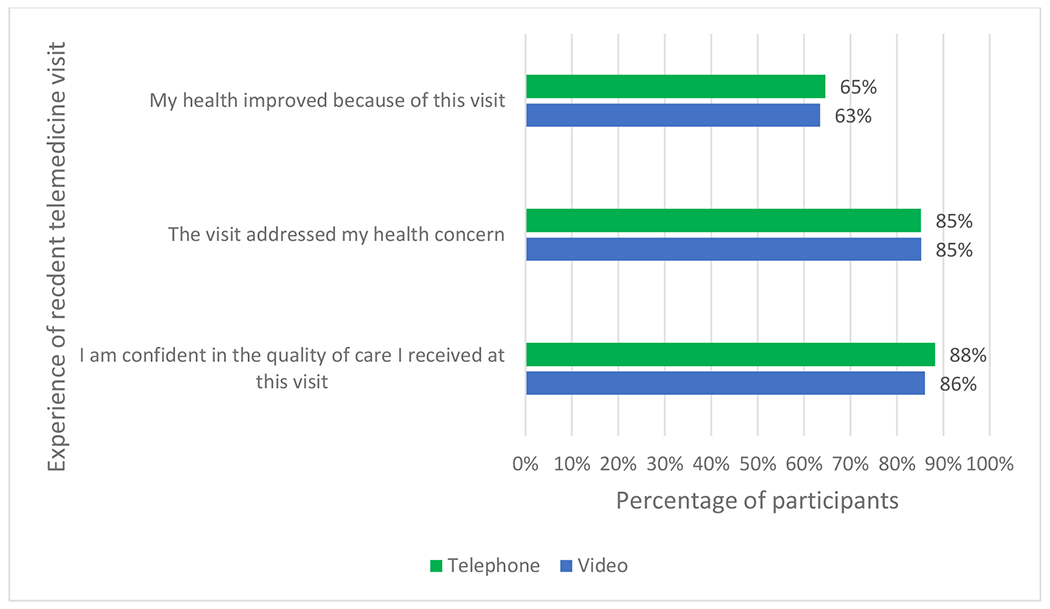
Patient-reported experience of recent telemedicine visit
The majority of patients reported no barriers to telephone (72%) or video visits (57%), however, only 19% of patients had no barriers to in-person visits (appendix S5). Finding a private/quiet space was the most common barrier reported for both video (13%) and telephone visits (10%, appendix S6). Issues related to technology were among the most commonly reported barriers to video visits (i.e., setting up the visit (13%) and having adequate internet connection (11%)).
Discussion
In a survey of patient primary care telemedicine experiences during the COVID-19 pandemic, most participants preferred in-person visits before and after the pandemic. However, patients anticipated a preference shift toward telemedicine post-pandemic. Most patients said the telemedicine visit met their health needs, although many delayed non-urgent or needed care during early pandemic when availability of in-person visits were limited.
While telemedicine visits were widely available for years within the study setting pre-pandemic, uptake had been limited[15, 17, 24]. Prior studies from our setting, before and during the pandemic, generated evidence from automated data about patient characteristics of telemedicine users, the clinical areas addressed, and follow-up care rates after telemedicine versus office visits [15, 19, 25, 26]. Together with the current paper’s distinct and complementary focus describing patient-reported experiences and preferences, these studies offer a more complete picture of telemedicine use and impacts. Although the COVID pandemic created the impetus for novel telemedicine use, positive experience among new users likely facilitated an increased preference for telemedicine beyond the pandemic period.
In our study, even with a larger increased preference for video, telephone visits remain a crucial option for patients who face barriers to, or do not prefer a video-enabled call[6, 29]. Nearly 1 in 5 participants reported a preference for telephone visits post-pandemic and technical issues were reported by 1 in 4 participants during a video visit in this study period. Patients with limited English proficiency were less likely to use video than telephone visits[25], emphasizing the need for continued access to telephone visits to mitigate the impact of the “digital divide” [27, 28] in accessing care.
Among those preferring an office visit pre-pandemic, household income was associated with post-pandemic visit modality preference shifts. Descriptive differences in patient modality shifts across other patient characteristics did not reach the level of significance, possibly due to our limited sample for examining patient subgroups, suggesting an opportunity for future research.
Our study had several limitations. Participation was limited to patients who self-scheduled a visit with their primary care provider using the portal during the early months of the COVID-19 pandemic. Additionally, our setting where telemedicine was already available to patients pre-pandemic, may not be generalizable to settings with unique telemedicine implementation approaches. As an observational study, our data cannot support causal conclusions.
Our study leveraged real world conditions that created opportunity for novel exposure to telemedicine, even among participants previously preferring in-person care. Our results on expected shifts in preferences for accessing primary care will help providers be better prepared to meet patients’ needs. Although long term impacts of the pandemic on telemedicine preference and use patterns remain to be seen, structured and open-ended patient responses suggest that a range of factors are used to determine visit mode preference, including: clinical factors, personal preference, convenience, patient characteristics and technology access. Similar to others, we found that the majority of participants prefer at least some of their post-pandemic health care be delivered via telemedicine [13, 24, 30–33]. Given the likelihood that preference for both telephone and video visits will continue at an increased rate compared to before the pandemic, reimbursement policies that allow for multiple care delivery modalities, will better preserve equitable access for populations without the skills or technology needed to complete a video visit.
Supplementary Material
Acknowledgments.
This work was funded by a grant from the Agency for Healthcare Research and Quality (R01HS25189).
Footnotes
Conflicts of interests. None declared.
Contributor Information
Andrea Millman, Kaiser Permanente Division of Research, 2000 Broadway, 3rd floor, Oakland CA 94612.
Jie Huang, Kaiser Permanente Division of Research, Oakland, CA.
Ilana Graetz, Department of Health Policy and Management, Emory University Rollins School of Public Health, Atlanta GA.
Catherine Lee, Kaiser Permanente Division of Research, Oakland, CA.
Judy Shan, University of California San Francisco, School of Medicine.
Loretta Hsueh, Department of Psychology, University of Illinois Chicago, Chicago, IL.
Emilie Muelly, The Permanente Medical Group, Santa Clara, CA.
Anjali Gopalan, Kaiser Permanente Division of Research, Oakland, CA.
Mary Reed, Kaiser Permanente Division of Research, Oakland, CA.
References
- 1.Bruining N, The post-pandemic legacy: the breakthrough of digital health and telemedicine. Cardiovasc Res, 2021. 117(9): p. e118–e119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chang JE, Lindenfeld Z, Albert SL, et al. , Telephone vs. Video Visits During COVID-19: Safety-Net Provider Perspectives. J Am Board Fam Med, 2021. 34(6): p. 1103–1114. [DOI] [PubMed] [Google Scholar]
- 3.Friedman AB, Gervasi S, Song H, et al. , Telemedicine catches on: changes in the utilization of telemedicine services during the COVID-19 pandemic. Am J Manag Care, 2022. 28(1): p. e1–e6. [DOI] [PubMed] [Google Scholar]
- 4.Mann DM, Chen J, Chunara R, et al. , COVID-19 transforms health care through telemedicine: Evidence from the field. J Am Med Inform Assoc, 2020. 27(7): p. 1132–1135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Patel SY, Mehrotra A, Huskamp HA, et al. , Trends in Outpatient Care Delivery and Telemedicine During the COVID-19 Pandemic in the US. JAMA Intern Med, 2021. 181(3): p. 388–391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Drake C, Lian T, Cameron B, et al. , Understanding Telemedicine’s “New Normal”: Variations in Telemedicine Use by Specialty Line and Patient Demographics. Telemed J E Health, 2022. 28(1): p. 51–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Duffy S and Lee TH, In-Person Health Care as Option B. N Engl J Med, 2018. 378(2): p. 104–106. [DOI] [PubMed] [Google Scholar]
- 8.Rush KL, Howlett L, Munro A, et al. , Videoconference compared to telephone in healthcare delivery: A systematic review. Int J Med Inform, 2018. 118: p. 44–53. [DOI] [PubMed] [Google Scholar]
- 9.Telehealth: What Is It, How to Prepare, Is It Covered? Content reviewed August 26, 2020 May 16, 2023]; Available from: https://www.nia.nih.gov/health/telehealth-what-it-how-prepare-it-covered. [Google Scholar]
- 10.Medicare Telemedicine Health Care Provider Fact Sheet. Mar 17, 2020 May 16, 2023]; Available from: https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet. [Google Scholar]
- 11.Rodriguez JA, Betancourt JR, Sequist TD, et al. , Differences in the use of telephone and video telemedicine visits during the COVID-19 pandemic. Am J Manag Care, 2021. 27(1): p. 21–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Venkatesh KP and Mallipeddi N, Increasing value and facilitating adoption of telehealth in the post-COVID era: An interview with chair of the American Telemedicine Association Joseph Kvedar. Healthc (Amst), 2022. 10(2): p. 100624. [DOI] [PubMed] [Google Scholar]
- 13.Imlach F, McKinlay E, Middleton L, et al. , Telehealth consultations in general practice during a pandemic lockdown: survey and interviews on patient experiences and preferences. BMC Fam Pract, 2020. 21(1): p. 269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Donelan K, Barreto EA, Sossong S, et al. , Patient and clinician experiences with telehealth for patient follow-up care. Am J Manag Care, 2019. 25(1): p. 40–44. [PubMed] [Google Scholar]
- 15.Reed ME, Huang J, Graetz I, et al. , Patient Characteristics Associated With Choosing a Telemedicine Visit vs Office Visit With the Same Primary Care Clinicians. JAMA Netw Open, 2020. 3(6): p. e205873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Reed M, Huang J, Graetz I, et al. , Treatment and Follow-up Care Associated With Patient-Scheduled Primary Care Telemedicine and In-Person Visits in a Large Integrated Health System. JAMA Netw Open, 2021. 4(11): p. e2132793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Reed ME, Parikh R, Huang J, et al. , Real-Time Patient-Provider Video Telemedicine Integrated with Clinical Care. N Engl J Med, 2018. 379(15): p. 1478–1479. [DOI] [PubMed] [Google Scholar]
- 18.Huang J, Gopalan A, Muelly E, et al. , Primary care video and telephone telemedicine during the COVID-19 pandemic: treatment and follow-up health care utilization. Am J Manag Care, 2023. 29(1): p. e13–e17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Huang J, Graetz I, Millman A, et al. , Primary care telemedicine during the COVID-19 pandemic: patient’s choice of video versus telephone visit. JAMIA Open, 2022. 5(1): p. ooac002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lamer A, Laurent G, Pelayo S, et al. , Exploring Patient Path Through Sankey Diagram: A Proof of Concept. Stud Health Technol Inform, 2020. 270: p. 218–222. [DOI] [PubMed] [Google Scholar]
- 21.Kennedy ABW and Sankey HR, THE THERMAL EFFICIENCY OF STEAM ENGINES. REPORT OF THE COMMITTEE APPOINTED TO THE COUNCIL UPON THE SUBJECT OF THE DEFINITION OF A STANDARD OR STANDARDS OF THERMAL EFFICIENCY FOR STEAM ENGINES: WITH AN INTRODUCTORY NOTE. (INCLUDING APPENDIXES AND PLATE AT BACK OF VOLUME). Minutes of the Proceedings of the Institution of Civil Engineers, 1898. 134(1898): p. 278–312. [Google Scholar]
- 22.Lewis T, Weighting Adjustment Methods for Nonresponse in Surveys, in Western Users of SAS Software (WUSS) Conference. 2012, lexjansen.com: Long Beach, CA. [Google Scholar]
- 23.Rao J and Scott A, The analysis of categorical data from complex sample surveys: chi-squared tests for goodness of fit and independence in two way tables. Journal of the American statistical association, 1981. 76(374): p. 221–30. [Google Scholar]
- 24.Reed ME, Huang J, Parikh R, et al. , Patient-Provider Video Telemedicine Integrated With Clinical Care: Patient Experiences. Ann Intern Med, 2019. 171(3): p. 222–224. [DOI] [PubMed] [Google Scholar]
- 25.Hsueh L, Huang J, Millman AK, et al. , Disparities in Use of Video Telemedicine Among Patients With Limited English Proficiency During the COVID-19 Pandemic. JAMA Netw Open, 2021. 4(11): p. e2133129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Juergens N, Huang J, Gopalan A, et al. , The association between video or telephone telemedicine visit type and orders in primary care. BMC Med Inform Decis Mak, 2022. 22(1): p. 302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Graetz I, Gordon N, Fung V, et al. , The Digital Divide and Patient Portals: Internet Access Explained Differences in Patient Portal Use for Secure Messaging by Age, Race, and Income. Med Care, 2016. 54(8): p. 772–9. [DOI] [PubMed] [Google Scholar]
- 28.Walker DM, Hefner JL, Fareed N, et al. , Exploring the Digital Divide: Age and Race Disparities in Use of an Inpatient Portal. Telemed J E Health, 2020. 26(5): p. 603–613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Crotty BH, Hyun N, Polovneff A, et al. , Analysis of Clinician and Patient Factors and Completion of Telemedicine Appointments Using Video. JAMA Netw Open, 2021. 4(11): p. e2132917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ebbert JO, Ramar P, Tulledge-Scheitel SM, et al. , Patient preferences for telehealth services in a large multispecialty practice. J Telemed Telecare, 2021: p. 1357633X20980302. [DOI] [PubMed] [Google Scholar]
- 31.Powell RE, Henstenburg JM, Cooper G, et al. , Patient Perceptions of Telehealth Primary Care Video Visits. Ann Fam Med, 2017. 15(3): p. 225–229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Predmore ZS, Roth E, Breslau J, et al. , Assessment of Patient Preferences for Telehealth in Post-COVID-19 Pandemic Health Care. JAMA Netw Open, 2021. 4(12): p. e2136405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Thomson MD, Mariani AC, Williams AR, et al. , Factors Associated With Use of and Satisfaction With Telehealth by Adults in Rural Virginia During the COVID-19 Pandemic. JAMA Netw Open, 2021. 4(8): p. e2119530. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.