

Abstract
Objective:
To examine the interaction between child temperament and caregiver linguistic input (i.e., syntactic complexity and lexical diversity) on receptive language in children who are deaf or hard-of-hearing (DHH).
Design:
Families of 59 DHH children (M age = 5.66 years) using spoken language for communication participated in this cross-sectional study. Caregivers completed the Child Behavior Questionnaire – Short Form, which measured child temperament across three established factors (i.e., effortful control, negative affectivity, surgency-extraversion) and participated with their child in a semi-structured, dyadic play interaction that occurred during a home visit. Caregivers’ language during the play interaction was quantified based on lexical diversity and syntactic complexity. Children also completed norm-referenced receptive language measures (i.e., Comprehensive Assessment of Spoken Language-2, age-appropriate Clinical Evaluation of Language Fundamentals) during the home visit that were combined into a composite measure of child receptive language.
Results:
When caregivers used lower to moderate levels of lexical diversity, child effortful control was positively related to child receptive language. However, when caregivers used higher levels of lexical diversity, child effortful control and child receptive language were not related to each other.
Conclusions:
Family environments rich in caregiver lexical input to children might provide a protective influence on DHH child language outcomes by helping to ensure DHH children with varying self-regulatory abilities achieve better spoken language comprehension. These findings highlight the importance of encouraging caregivers to provide rich and stimulating language-learning environments for DHH children.
INTRODUCTION
Much of child development occurs within the context of dyadic exchanges between children and their caregivers. Interactions between child temperament and certain caregiver attributes have been shown to influence language outcomes in typically-developing infants and toddlers (Laake & Bridgett, 2018; Spinelli et al., 2018). For example, research in families with typically hearing (TH) infants suggests that rich caregiver input (i.e., diverse vocabulary and grammatical forms) can positively influence language development when infants possess strong attentional skills that support language learning (Spinelli et al., 2018). However, research in children who are deaf or hard of hearing (DHH) has not examined how the interaction between child temperament and caregiver attributes such as linguistic input can together influence spoken language outcomes. Temperament generally refers to the interplay of regulatory (e.g., attentional skills) and reactive (e.g., negative and/or positive emotionality) processes that contribute to individual differences across developmental periods (Rothbart et al., 2004). Child temperament and its interaction with the environment is thought to be more salient during infancy and toddlerhood in children with TH as this is a period of rapid speech and language development (Conture et al., 2013). Once stronger expressive and receptive language skills have been acquired, child temperament is believed to primarily affect social and behavioral development (Chen et al., 2014; Spinelli et al., 2018). However, because DHH children may experience reduced access to linguistic stimuli from their environments even with hearing aids (HAs) and cochlear implants (CIs; Kelly et al., 2019; Moeller & Tomblin; 2015), child temperament may continue to influence dyadic child-caregiver exchanges and child language outcomes for longer periods of development. A better understanding of the transactional (e.g., bidirectional relations between people; Sameroff, 2010) nature of child temperament and caregiver linguistic input could help account for some of the variability observed in spoken language outcomes in DHH children. In addition, knowledge of these transactional relations can inform intervention for children who are DHH, which often includes educating parents to modify their linguistic input to fit the needs of their child (Ambrose et al., 2014; Yoshinaga-Itano et al., 2020).
Child Temperament and Spoken Language Development
One leading definition of child temperament refers to individual differences in reactivity (i.e., tendency for children to respond strongly to stimuli) and self-regulation (i.e., ability to control emotions and behaviors; Rothbart & Posner, 2022). Although there are many theoretical perspectives for studying temperament, most scholars agree that temperament reflects innate traits with a genetic component that are apparent early in life and are, to some degree, subject to environmental influences (Goldsmith et al., 1987; Shiner et al., 2012). A well-accepted theoretical construct used to measure the different temperament traits in school-aged children outlines three broad dimensions that can be observed through children’s behavior: effortful control, negative affectivity, and surgency-extraversion (Rothbart et al., 2001). Effortful control is defined as the ability for children to willfully self-regulate attention, emotion, and behaviors to inhibit a dominant response (Rothbart et al., 2003). Negative affectivity and surgency-extraversion comprise traits associated with emotional reactivity. Negative affectivity constitutes activation of negative emotional responses (e.g., anger, discomfort, fear) when approaching novel stimuli and people, while surgency-extraversion reflects the other end of the emotional spectrum, referring to the activation of extreme positive emotional responses across situations (e.g., activity level, impulsivity; Rothbart et al., 2001). Children can exhibit characteristics across these three dimensions. In typically developing, TH infants, temperaments associated with strong effortful control and positive emotionality have been associated with better language outcomes (Dixon & Smith, 2000; Salley et al., 2013; Slomkowski et al., 1992). Effortful control is thought to positively influence language outcomes by enabling children to direct their attention and focus on linguistically relevant information in their environment (Bloom et al., 1993). Similarly, children with low negative affectivity and surgency-extraversion are thought to possess greater cognitive resources that can be allocated to attending to linguistic information rather than to shifting between emotional states (Bloom, 1993). Although traits underlying negative affectivity and surgency-extraversion may require greater use of attentional resources, they also can prompt caregivers to engage with their children. For example, children with moderate to high levels of surgency-extraversion may appear more outgoing and thus, elicit more opportunities to interact with others compared to those extremely low in surgency-extraversion. Therefore, it is beneficial to consider certain combinations of temperament dimensions when examining their relationship to language development (Gouge, 2011), as children can display varying levels of these different dimensions.
While the relation between temperament and language development in children who are DHH remains largely unexplored, much attention has been given to the relation between various domains of executive functioning and spoken language in DHH children (e.g., Beer et al., 2014; Holt et al., 2012; Kronenberger et al., 2020). Temperament and executive functioning represent two (traditionally distinct) conceptual frameworks for examining self-regulatory abilities. DHH children have been shown to experience deficits in many domains of executive function including attention, inhibition, and emotion regulation (e.g., Beer et al., 2010; Kronenberger et al., 2014; Wiefferink et al., 2012). While these domains of executive functioning may show conceptual overlap with dimensions used to examine temperament (Bridgett et al., 2013, Schmidt et al., 2022), executive functioning is thought to be malleable to intervention (Kronenberger, 2019; Neville et al., 2013). Temperament, on the other hand, reflects innate characteristics present at birth, preceding the development of executive functions. Furthermore, temperament is thought to be static over the course of development but may be influenced to some extent by the environment or life experiences (Rothbart & Bates, 2006). Therefore, investigating how child temperament influences child language can highlight important and relatively stable contributions from DHH children, which can potentially explain some of the variability observed in DHH children’s spoken language development.
The Potential Influence of Caregivers on Child Temperament and Spoken Language
One factor in the home environment that can affect associations between temperament and language in children is the dyadic exchange between a child and their caregiver(s). Indeed, caregiver-child interactions represent an important context for language development (e.g., Hoff, 2006; Loi et al., 2017). Whereas certain temperaments are considered beneficial for child language learning, caregivers can further shape language outcomes based on their responses to their child’s temperament. For example, some studies have examined transactional relations between child temperament and caregiver behaviors, such as supportive parenting behaviors (e.g., structuring the environment, social initiative, positive affect; Laake & Bridgett, 2018) and maternal responsivity (e.g., sensitivity; Karrass & Braungart-Rieker, 2003) during interactions in typically-developing infants. A positive association was observed between maternal support during early infancy and expressive language later in infancy for infants with high positive affect (greater displays of positive emotions such as smiling and laughter), whereas a negative association was observed for infants exhibiting low positive affect (e.g., less smiling and laughter; Laake & Bridgett, 2018). Further, infants displaying traits associated with lower negative affectivity (i.e., low distress to novelty) showed better language when mothers showed high responsivity (Karrass & Braungart-Rieker, 2003). These studies illustrate how child and caregiver characteristics can together influence language development. Specifically, better language outcomes were observed when children exhibited positive affect/low negative affectivity and when caregivers were more responsive. Indeed, other studies have also supported interactions between child temperament and caregiver characteristics such as parenting behaviors and styles (e.g., controlling versus affective parenting, emotional responsiveness, etc.; Kiff et al., 2011; Slagt et al., 2016), suggesting the important contribution of transactional relations between child temperament and caregiver behaviors to developmental outcomes in children.
Another caregiver behavior important to child language development that can interact with child temperament is caregiver linguistic input. The transactional relation between child temperament and caregiver linguistic input can be reflected in caregivers possessing an awareness of their child’s temperament and, in turn, providing more or less language opportunities based on their child’s regulatory skills and emotional tendencies. Spinelli et al. (2018) examined the longitudinal relation between temperament and language in typically developing infants at low, moderate, and high levels of maternal input. Maternal input was quantified using mean length of utterance (MLU) in words and number of different word (NDW) roots as proxies for syntactic complexity and lexical diversity, respectively, as these are two areas of language that rapidly develop during infancy (Spinelli et al., 2018). Transcriptions of the mother-child interactions followed guidelines from Codes for the Human Analysis of Transcripts (CHAT; MacWhinney, 2000), the transcription format used for the CHILDES (Child Language Data Exchange System) Project–a database used for examining child language acquisition. Their study measured infant temperament (duration of orienting – attention; smile and laughter – positive affect; distress to limitations – negative affect) via the Infant Behavior Questionnaire-Revised (IBQ-R; Gartstein & Rothbart, 2003) at 3 months of age. Maternal input was measured during a 3-minute mother-infant interaction at 6, 9, and 12 months of age, and child vocabulary and syntactic competency at 18 and 24 months of age. Findings from Spinelli et al. (2018) revealed that the relation between infant attention and language production at 18 and 24 months of age was moderated by mothers’ use of syntactic complexity and lexical diversity at 6 and 9 months of age. Specifically, infants who demonstrated greater attentional abilities achieved better language outcomes when their caregivers provided greater quality of linguistic input (Spinelli et al., 2018). However, when mothers used low levels of linguistic input, infant temperament was not related to language outcomes – infants with varying attentional abilities performed similar on language outcomes. Together, these findings suggest that only infants with high regulatory skills could capitalize on higher quality maternal input in the form of lexical diversity and syntactic complexity.
The Current Study
The literature examining the interactive effects of temperament and caregiver characteristics on language in typically developing children focuses on the infancy period (Karrass & Braungart-Rieker, 2003; Laake & Bridgett, 2018; Spinelli et al., 2018). After this period of development, language skills appear to be more resilient to the effects of child temperament and the child’s surrounding environment (Conture et al., 2013; Spinelli et al., 2018). Nonetheless, temperament (and its effects on child language) appears to carry importance beyond the infancy period for clinical pediatric populations, such as children who stutter (Singer et al., 2019; Tumanova et al., 2020). The fact that effects of temperament appear to influence language outcomes for a longer developmental period for children who stutter may highlight the extended importance of child-level factors for children who experience challenges in typical language development. Another pediatric clinical population whose temperament may continue to influence language outcomes into childhood is children who are DHH. Children who are DHH with HAs and CIs may have fewer opportunities for language learning due to reduced access to auditory stimuli compared to their peers with TH (e.g., Kelly et al., 2019; Moeller & Tomblin; 2015). As a result, it is likely that the transactional processes underlying interactions between child temperament and caregiver input that influence language outcomes in infancy are salient during childhood for DHH children. Perhaps DHH children with temperaments more conducive for language learning (i.e., high effortful control) can help them overcome potential negative effects of hearing loss. Caregivers may further help compensate for their child’s hearing loss through talking more and providing more language-learning opportunities. Indeed, research supports that DHH children with caregivers who provide high-quality linguistic input and who implement interactive strategies (e.g., high responsiveness, supporting joint engagement, etc.) experience better language outcomes compared to those with caregivers who are less interactive with their children (Ambrose et al., 2014; Moeller & Tomblin, 2015; Roberts, 2019; Desjardin et al., 2014). In environments with rich linguistic input, DHH children with less reactive temperaments that support language processing may be able to achieve better language outcomes, as seen in TH infants. Thus, the purpose of the current study is two-fold: (1) to examine the relation between child temperament, caregiver linguistic input (i.e., lexical diversity and syntactic complexity), and receptive language in children who are DHH; and (2) to examine the possible moderating effect of caregiver linguistic input on associations between child temperament and child receptive language. Based on the previous literature on child temperament and child language (Bloom, 1993, Slomkowski et al., 1992) we expected children with high regulatory capacities (i.e., high effortful control) to be less reactive (i.e., low surgency-extraversion and negative affectivity) and have better receptive language skills. We also expected more regulated children and less reactive children to have caregivers who produced more syntactic complexity and lexical diversity. Further, we predicted that children with temperaments more conducive for language development (i.e., high effortful control, low surgency-extraversion, low negative affectivity) would achieve better receptive language scores regardless of their caregivers’ level of lexical diversity or syntactic complexity.
METHOD
Participants
Caregiver-child dyads were recruited from Ohio and Indiana as part of a larger, longitudinal study investigating the role of the family environment on developmental outcomes in DHH children. The sample consisted of 59 families with children who are DHH and between the ages 3 and 7 years (Mage = 5.66 years; SD = 1.53; 28 female, 31 male, 0 nonbinary) and their caregivers with self-reported typical hearing (54 mothers, 3 fathers, 0 parents/nonbinary, 2 grandmothers, 0 grandfathers, 0 grandparents/nonbinary). Forty-six of the children were White, 8 were Black/African American, 3 were Asian, and 2 were Hispanic or Latino/a. To maintain more experimental control, only families that completed the same measure of child temperament (described in the Materials section) were recruited from the larger study. An additional child with HAs was excluded from the study as she was unable to complete receptive language measures, and thus could not contribute to data analyses.
Twenty-five children were consistent binaural HA users who received diagnosis and intervention by 3 years, and 34 children were consistent CI users (32 binaurally and 2 bimodally, with a CI on one side and a HA on the other) who received diagnosis and intervention by 3.5 years. On average, unaided better-ear pure-tone averages (BEPTAs) were 48 dB HL for children with HAs, and 75 dB HL for children with CIs (note that audiologic data reflect only a subset of DHH children following several attempts to obtain audiologic history from their audiologists; see Table 1). All children participating in this study met the following inclusion criteria: nonverbal cognitive ability (i.e., nonverbal reasoning) score better than 2 standard deviations below the mean on the Differential Ability Scales-II Picture Similarities subtest (Elliot, 2007); family goal of using spoken language and the use of spoken English within the home; no additional developmental difficulties other than those related to hearing loss; and no diagnosis of auditory dyssynchrony.
Table 1.
Child and family demographics with means and standard deviations M(SD).
| Full Sample | HA Subgroup | CI Subgroup | |
|---|---|---|---|
|
| |||
| n | 59 | 25 | 34 |
| Female/Male/Nonbinary | 28/31/0 | 13/12/0 | 15/19/0 |
| Child Age, years | 5.66(1.53) | 5.49(1.31) | 5.79(1.68) |
| Average Caregiver Education Levela | Partial 4-Year College | Bachelor’s Degree | Partial 4-Year College |
| Average Annual Household Income Bracketb | $65,000 – $79,999 | $65,000 – $79,999 | $65,000 – $79,999 |
| Aided Better Ear PTA, dB HLc | 24.86(7.80) | 22.97(15.48) | 25.40(3.91) |
| Unaided Better Ear PTA, dB HLd | 53.15(16.90) | 48.49(14.43)** | 75.31(7.32)** |
| Duration of Device Use, yearse | 4.38(1.63) | 4.59(1.78) | 4.21(1.54) |
| Amount of Early Intervention, hours/monthf | 7.01(7.56) | 5.39(8.67) | 8.20(6.52) |
Note: HA=hearing aid, CI=cochlear implant, PTA=pure-tone average at 500, 1000, 2000, and 4000 Hz
Education scored on a 10-point ordinal scale: 1 = Elementary School, 2 = Junior High/Middle school [9th grade], 3 = Partial High School, 4 = General Education Diploma [High School Equivalence], 5 = High School, 6 = Technical/Vocational School, 7 = Partial 4-Year College, 8 = Bachelor’s Degree, 9 = Master’s Degree, 10 = Doctoral Degree
Reported gross household income from previous year scored on a 10-point interval: 1 = Under $5,000, 2 = $5,500 – $9,999, 3 = $10,000 – $14,999, 4 = $15,000 – $24,999, 5 = $25,000 – $34,999, 6 = $35,000 – $49,999, 7 = $50,000 – $64,999, 8 = $65,000 – $79,999, 9 = $80,000 – $94,999, 10 = $95,000 and over
From a subset of participants for whom these data were available (DHH: n = 36, HA: n = 8, CI: n = 28)
From a subset of participants for whom these data were available (DHH: n = 23, HA: n = 19, CI: n = 4)
Duration of device use calculated from time when children with HAs and CIs were fit with HAs and CIs, respectively (DHH: n = 58, HA: n = 25, CI: n = 33)
Average number of hours per month that the child spent in early intervention services from birth to 3 years of age per caregiver report
p < .001
Child and family demographics are displayed in Table 1. Children with HAs and children with CIs did not differ in age, t(57) = −.745, p = .459, gender, χ2(1) = .359, p = .549, caregiver education, t(57) = .416, p = .679, household income, t(57) = .841, p = .404, aided BEPTA, t(34) = −.774, p = .444, duration of device use, t(56) = .864, p = .391, or amount of early intervention received, t(57) = −1.42, p = .160. However, children with HAs had significantly better unaided BEPTA, t(21) = −3.57, p = .002 than those with CIs, as expected.
Materials
Child Temperament
Child temperament was measured using the Child Behavior Questionnaire–Short Form (CBQ-SF; Rothbart et al., 2001), a 94-item caregiver questionnaire that assesses Effortful Control, Negative Affectivity, and Surgency-Extraversion as three global dimensions of temperament in children 3 – 7 years of age. Primary caregivers rated their child’s behavior during the previous six months across different situational contexts, ranging from 1 (extremely untrue of their child) to 7 (extremely true of their child). The Effortful Control dimension consists of attentional focusing, inhibitory control, low intensity pleasure, and perceptual sensitivity subscales. Example items included in the Effortful Control dimension from the questionnaire include “When building or putting something together, becomes very involved in what s/he is doing, and works for long periods” and “Is good at following directions”. The Surgency-Extraversion dimension is composed of activity level, high intensity pleasure, impulsivity, and reverse-scored shyness subscales. Example items contributing to this dimension include “Often rushes into an activity without thinking about it” and “Is full of energy, even in the evening”. Finally, the anger/frustration, discomfort, fear, sadness, and reverse-scored falling reactivity/soothability subscales make up the Negative Affectivity dimension and include items such as, “Is likely to cry when even a little bit hurt” and “Acts shy around new people”. Two subscales of temperament (approach/positive anticipation and smiling/laughter) are not included in these three global dimensions (Rothbart et al., 2001). Variable internal consistency (α = .62 to .88) has been reported for the subscales on the CBQ-SF, however 12 subscales revealed alpha levels above .70 (Putnam & Rothbart, 2006). Scores from each subscale were averaged together for each respective global dimension and used for analyses. Higher scores reflect children with high levels of that particular temperament dimension.
Child Receptive Language
Children’s receptive language was assessed using two norm-referenced measures administered to the child by a trained clinical researcher during the home visit: The Comprehensive Assessment of Spoken Language-2 (CASL-2; Carrow-Woolfolk & Lynch, 1982) and the age-appropriate version of the Clinical Evaluation of Language Fundamentals (CELF; Semel et al., 2004; Semel et al., 2013). These assessments have commonly been used to assess language skills, including in DHH children (Geers et al., 2019; Holt et al., 2022; Walker et al., 2022). The CASL-2 measures spoken language comprehension abilities (i.e., comprehension, expression, retrieval) in children and young adults (ages 3 – 21 years). The current study utilized the Sentence Comprehension subtest of the CASL-2 as a measure of language comprehension in DHH children. The CASL-2 standard score for this subtest was calculated for each child (normative mean = 100, SD = 15). Children’s complex language comprehension skills were also assessed using the Concepts and Following Directions subscale of the CELF-Preschool-2 for children younger than 6 years of age (CELF-P-2; Semel et al., 2004), or the Following Directions subscale of the CELF-5 for children 6 years and older (Semel et al., 2013). CELF-5/P-2 scaled scores (normative mean = 10, SD = 3) were calculated for each child.
Caregiver Linguistic Input
Systematic Analysis of Language Transcripts (SALT-2; Miller & Iglesias, 2012) software was used to transcribe and analyze caregivers’ spoken language. SALT-2 is a transcription software employing unique conventions for identifying different aspects of utterances from language samples. The software provides analyses of syntax/morphology (e.g., mean length of utterance), semantics (e.g., number of different words), and other aspects of language. For the current study, quality of caregivers’ linguistic input to children was quantified using syntactic complexity and lexical diversity. To capture syntactic complexity (i.e., caregivers’ use of grammatical forms), we obtained mean length of utterance (MLU) in morphemes from caregivers during a semi-structured, naturalistic play session that occurred in the families’ homes using the standard report measure from SALT-2. In addition, we also obtained the number of different root (excluding affixes) words (NDW) used by caregivers during the play session to capture the richness of caregivers’ vocabulary (i.e., lexical diversity).
Procedures
As part of the larger study, caregivers were mailed consent forms, parental permission forms, and questionnaires (including the CBQ-SF) to complete prior to the home visit. All questionnaires completed by the primary caregiver were reviewed and collected during a 1.5- to 2.5-hour home visit. Testing performed during the home visit was completed by two trained clinical researchers. One of the researchers administered child assessments in one area of the home, including the CASL-2 and CELF-5/P-2, while the other administered measures to the caregiver. Note that caregiver and child measures reported here reflect a subset of the measurements administered during home visits with families. All research was approved by The Ohio State University Institutional Review Board.
Language samples were derived from a semi-structured, dyadic caregiver-child play interaction. The caregiver and child were instructed to play together “as they would at home normally” for 15 minutes, followed by a 5-minute clean-up period, using a set of five age-appropriate toys. Parents were told not to physically assist the child during the clean-up session; however, verbal support was allowed. Audio-Technica ATW-T1801 or 1701/L transmitters with an omnidirectional lavalier microphone were worn by both the child and the caregiver and fed into a GoPro Hero4 video camera, which recorded the play interaction. Two trained research assistants were involved in transcribing play interaction videos. To establish consistency, approximately two thirds of the videos were transcribed by both research assistants and any discrepancies were resolved via weekly meetings led by the third author. All subsequent videos were transcribed by one of two transcribers and reviewed by the third author. SALT-2 was used to calculate MLU and NDW for caregivers from the dyadic caregiver-child play interaction (data from the 5-minute clean-up period were not used in analyses).
Data Analyses
All analyses were performed using SPSS-version 27.0 (IBM Statistics, 2020). Descriptive statistics were examined to characterize the sample across study variables. Partial Pearson correlations were performed to examine associations between child temperament, child receptive language, and quality of caregiver linguistic input (syntactic complexity and lexical diversity) while controlling for caregiver education, a known contributor to language development in children who are DHH (Geers et al., 2009; Holt & Svirsky, 2008; Liberatos et al., 1988; Mehra et al., 2009; Neuhauser, 2018; Su & Chan, 2017). Moderation analyses using an SPSS macroinstruction (PROCESS; Hayes, 2017) were performed to examine whether differential associations between child temperament (focal regressor) and child receptive language (outcome variable) depended on caregiver linguistic input (moderator). Caregiver education was also included as a covariate for these analyses. For each model, PROCESS computes a regression analysis that also includes an interaction term (which is the product of the focal regressor and moderator variables). A significant interaction term (p < .05) indicates that the relation between the focal regressor and outcome variable is dependent on the moderator. PROCESS then probes the interaction between the focal regressor and the moderator using the “pick-a-point” approach, examining the relation between the focal regressor and outcome variable at the 16th, 50th, and 84th percentiles of the moderator, corresponding to relatively low, moderate, and high levels of the moderator, respectively (Hayes, 2017). A follow-up Johnson-Neyman analysis is then carried out to identify the exact value of the moderator at which the relation between the focal regressor and outcome variable becomes significant (Hayes, 2017).
RESULTS
Descriptive Analyses
Child Temperament
The top portion of Table 2 displays descriptive statistics for the three temperament dimensions for the entire sample and for the subgroups of HA and CI users. Children with HAs and CIs did not differ in levels of effortful control, t(57) = 1.56, p = .125, d = .410, or negative affectivity, t(57) = −.524, p = .602, d = −.138. However, children with CIs had greater levels of surgency-extraversion compared to children with HAs, t(57) = −3.18, p = .002, d = −.838. The CBQ-SF does not have published norms, but these average scores are generally consistent with those published in the literature from TH children (e.g., Atzaba-Poria et al., 2014; Deater-Deckard et al., 2009; Lane et al., 2015).
Table 2.
Descriptive statistics with mean, standard deviations, and ranges for child temperament, caregiver linguistic input, and child receptive language measures.
| Full Sample M(SD) |
HA Subgroup M(SD) |
CI Subgroup M(SD) |
||
|---|---|---|---|---|
|
| ||||
| CBQ-SF: Effortful Control | Range | 5.13(.65) 3.69 – 6.27 |
5.28(.66) 3.71 – 6.27 |
5.02(.62) 3.69 – 6.04 |
| CBQ-SF: Negative Affectivity | Range | 3.79(.72) 2.28 – 5.17 |
3.74(.79) 2.28 – 5.17 |
3.83(.66) 2.43 – 4.94 |
| CBQ-SF: Surgency-Extraversion | Range | 4.79(.89) 2.53 – 6.34 |
4.40(.86)* 2.53 – 5.76 |
5.08(.78)* 2.92 – 6.34 |
| CASL-2: Sentence Comprehension | Range | 99.39(17.74) 70 – 129 |
101.48(17.10) 73 – 129 |
97.85(18.30) 70 – 129 |
| CELF-5/P-2: Following Directions | Range | 7.42(3.63) 0 – 14 |
7.88(3.38) 2 – 14 |
7.09(3.81) 0 – 14 |
| Caregiver Syntactic Complexity: MLU | Range | 4.38(.72) 3.01 – 6.44 |
4.47(.74) 3.10 – 6.12 |
4.33(.70) 3.01 – 6.44 |
| Caregiver Lexical Diversity: NDW | Range | 206.76(43.78) 105 – 332 |
210.40(46.37) 132 – 332 |
204.09(42.28) 105 – 293 |
Note: HA=hearing aid, CI=cochlear implant, CBQ-SF = Child Behavior Questionnaire Short Form, CASL= Comprehensive Assessment of Spoken Language-2, CELF-5/P-2= Clinical Evaluation of Language Fundamentals 5/Preschool-2, MLU= mean length of utterance, NDW= number of different words
p < .05
Child Receptive Language
The middle portion of Table 2 displays descriptive statistics for the receptive language measures. There was a wide range of scores on both receptive language measures, with 58% of children (34 out of 59 children) scoring within ±1 standard deviation (i.e., within normal limits) of the test mean for the CELF-5/P-2 and 56% (33 out of 59 children) scoring within ±1 standard deviation of the test mean for the CASL-2. Children with HAs and those with CIs did not significantly differ in CASL-2 scores, t(57) = .773, p = .443, d = .204, or CELF-5/P-2 scores, t(57) = .826, p = .413, d = .217, although there was a trend for children with HAs to score higher on both receptive language measures compared to children with CIs. Because of evidence that these two receptive language assessments measure similar underlying constructs (r = .694, p <.001), standard scores from the CASL-2 and scaled scores from the CELF-5/P-2 were standardized into Z-scores and averaged to create a receptive language composite score for each DHH child and used in subsequent analyses. As expected, receptive language composite scores did not differ significantly between children with HAs and children with CIs, t(57) = .870, p = .388, d = .229.
Caregiver Linguistic Input
The bottom of Table 2 displays the descriptive statistics for caregiver linguistic input. Primary caregivers for both children with HAs and CIs used similar levels of syntactic complexity, t(57) = .787, p = .435, d = .207, and lexical diversity, t(57) = .544, p = .589, d = .143, although there was a trend for caregivers of children with HAs to use greater lexical diversity and syntactic complexity than caregivers of children with CIs.
Since children with HAs and CIs did not significantly differ on demographic variables or on most of the study variables, the two groups were combined for all subsequent analyses to increase power, as analyses including only the subgroups would be underpowered for moderation analyses (Hayes, 2017; McClelland & Judd, 1993).
Associations among Child Temperament, Caregiver Linguistic Input, and Child Spoken Language Comprehension
Partial Pearson correlations (controlling for caregiver education) were performed to examine associations between child temperament dimensions, caregiver syntactic complexity and lexical diversity, and child receptive language (see results in Table 3). Higher effortful control was associated with lower levels of negative affectivity and surgency-extraversion. Additionally, children with higher effortful control had better receptive language composite scores and had caregivers who used greater syntactic complexity. Better receptive language composite scores also were observed in children when their caregivers used greater lexical diversity and syntactic complexity. Finally, the two caregiver linguistic input measures were positively correlated with one another. Post-hoc partial Pearson correlations with the sample’s subgroups (i.e., HA and CI group) show similar patterns to the full sample, indicating that neither of the subgroups were driving the results (see Appendix, Supplemental Digital Content 1, for the results of the partial Pearson correlations for each subgroup).
Table 3.
Partial Pearson correlationsa for child temperament, receptive language composite score, and caregiver linguistic input for the entire sample.
| 1 | 2 | 3 | 4 | 5 | 6 | ||
|---|---|---|---|---|---|---|---|
|
| |||||||
| 1 CBQ-SF: Effortful Control | - | - | - | - | - | - | |
| 2 CBQ-SF: Negative Affectivity | −.292* | - | - | - | - | - | |
| 3 CBQ-SF: Surgency-Extraversion | −.329* | −.108 | - | - | - | - | |
| 4 Receptive Language Composite Score | .407* | −.155 | −.154 | - | - | - | |
| 5 Caregiver Syntactic Complexity: MLU | .348* | −.127 | −.231 | .628** | - | - | |
| 6 Caregiver Lexical Diversity: NDW | .036 | .035 | −.134 | .347* | .538** | - | |
Note: CBQ-SF = Child Behavior Questionnaire Short Form, MLU= mean length of utterance, NDW= number of different words
Control variable: caregiver’s highest level of education; df = 56
p < .05,
p < .001
Multiple Regression & Moderation Analyses Estimating Child Receptive Language
Individual multiple linear regressions were performed to estimate child receptive language skills. Model regressors included a dimension of child temperament, a measure of caregiver input, and their interaction (e.g., child temperament × caregiver input interaction term). To simplify each model and because our sample is somewhat small for moderation analyses, we entered one dimension of temperament and one measure of caregiver linguistic input per model. All pairwise combinations were examined (3 temperament dimensions × 2 caregiver input measures = 6 models predicting receptive language composite scores). All models also included caregiver education as a covariate. If the interaction term between child temperament and caregiver linguistic input was significant (indicating significant moderation), we used PROCESS (Hayes, 2017) to probe the interaction and characterize the relationship between the focal regressor (i.e., child temperament) and child receptive language at specific levels of the moderator (i.e., caregiver lexical diversity and syntactic complexity).
Lexical Diversity
Estimating Child Receptive Language from Effortful Control and Caregiver Lexical Diversity
The top portion of Table 4 displays the results of the regression model with effortful control, lexical diversity, and their interaction included as regressors estimating child receptive language (in addition to caregiver education as a covariate). The model was significant: effortful control, lexical diversity, and their interaction contributed significantly to the model above and beyond caregivers’ education level. The relation between effortful control and receptive language was significantly moderated by caregiver lexical diversity, F(1, 54) = 6.36, p = .015, ΔR2 = .07. PROCESS (Hayes, 2017) was then used to probe the conditional effects of the significant interaction using the pick-a-point approach. Significant conditional associations between child effortful control and child receptive language were observed at the 16th (low) and 50th (moderate) percentiles of caregivers’ level of lexical diversity. When caregivers used low (b = .869, p < .001) and moderate (b = .556, p < .001) amounts of lexical diversity, children’s level of effortful control and receptive language abilities were positively related to each other. At high levels of caregiver lexical diversity (84th percentile; b = −.013, p = .961) there was no longer a significant association between effortful control and receptive language in children. A Johnson-Neyman analysis revealed that caregiver lexical diversity moderated the relation between effortful control and receptive language in children whose caregivers used less than 221.68 different words (b = .336, p = .050) during the play session, reflecting 38 of the 59 families. The moderating effects of caregiver lexical diversity on child effortful control and child receptive language are shown in Panel A of Figure 1.
Table 4.
Results of multiple regression analyses including each dimension of child temperament, lexical diversity, and their interaction as regressors (controlling for caregiver education).
| Estimating Child Receptive Language from Effortful Control and Caregiver Lexical Diversity | |||
|
| |||
| Regressors | β | SE | t |
| (Constant) | −16.55* | 4.57 | −3.62 |
| Caregiver Education (Covariate) | .18* | .08 | 2.29 |
| Effortful Control | 2.70* | .87 | 3.10 |
| Lexical Diversity | .06* | .02 | 2.83 |
| Effortful Control x Lexical Diversity | −.01* | .00 | −2.52 |
| Model Summary | R2 = .42, F(4, 54) = 9.60, p < .001** | ||
|
| |||
| Estimating Child Receptive Language from Negative Affectivity and Caregiver Lexical Diversity | |||
|
| |||
| Regressors | β | SE | t |
| (Constant) | −3.03 | 3.38 | −.90 |
| Caregiver Education (Covariate) | .10 | .09 | 1.10 |
| Negative Affectivity | .16 | .81 | .20 |
| Lexical Diversity | .02 | .02 | .93 |
| Negative Affectivity x Lexical Diversity | −.00 | .00 | −.47 |
| Model Summary | R2 = .23, F(4, 54) = 4.12, p = .005* | ||
|
| |||
| Estimating Child Receptive Language from Surgency-Extraversion and Caregiver Lexical Diversity | |||
|
| |||
| Regressors | β | SE | t |
| (Constant) | −.79 | 2.84 | −.28 |
| Caregiver Education (Covariate) | .15 | .09 | 1.67 |
| Surgency-Extraversion | −.37 | .59 | −.63 |
| Lexical Diversity | .00 | .01 | .06 |
| Surgency-Extraversion x Lexical Diversity | .00 | .00 | .45 |
| Model Summary | R2 = .22, F(4, 54) = 3.81, p =.009* | ||
Note:
p <.05,
p<.001
Figure 1.
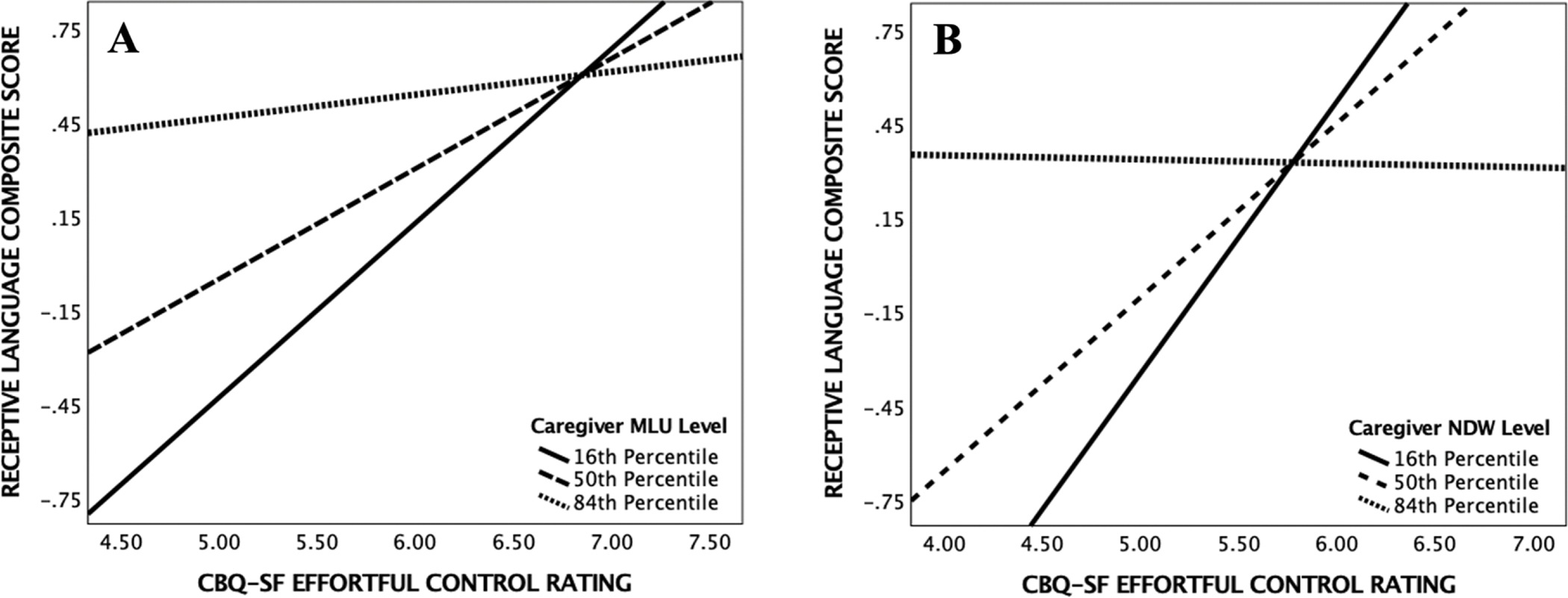
Panel A - The relation between effortful control (CBQ-SF) and receptive language (CASL-2 and CELF-5/P-2 Composite Score) at different levels of syntactic complexity (MLU) during dyadic play. Panel B - The relation between effortful control (CBQ-SF) and receptive language (CASL-2 and CELF-5/P-2 Composite Score) at different levels of lexical diversity (NDW) during dyadic play.
Estimating Child Receptive Language from Negative Affectivity and Caregiver Lexical Diversity
The regression model with negative affectivity, lexical diversity, and their interaction as regressors estimating receptive language are reported in the middle portion of Table 4 with caregivers’ level of education as a covariate. The model was significant; however, none of the regressors contributed significantly to child language. There was no interaction between negative affectivity and caregiver lexical diversity.
Estimating Child Receptive Language from Surgency-Extraversion and Caregiver Lexical Diversity
An additional model (Table 4, bottom portion) regressed surgency-extraversion, lexical diversity, and their interaction (as well as caregivers’ level of education as a covariate) on child receptive language. The model was significant, although no regressors added significance to the model. There was no interaction observed between surgency-extraversion and caregiver lexical diversity.
Syntactic Complexity
Estimating Child Receptive Language from Effortful Control and Caregiver Syntactic Complexity
The regression model with effortful control, syntactic complexity, and their interaction as regressors estimating receptive language (and caregiver education as a covariate) was significant. Specifically, effortful control and syntactic complexity contributed significantly to the model over and above caregiver education level (see the top portion of Table 5). The interaction term was marginally significant, F(1, 54) = 4.01, p = .050, ΔR2 = .04, and revealed a positive relation between child effortful control and receptive language at the 16th (b = .557 p = .007) and 50th (b = .352, p =.019) percentiles of caregiver syntactic complexity (i.e., level of MLU). At high MLU values – the 84th percentile (b = .073, p = .623) – no relation between effortful control and receptive language was observed. The Johnson-Neyman approach revealed that significant moderation effects occurred for caregivers with MLUs below 4.46 (b = .285, p = .050), which included 34 of the 59 families of children. Panel B of Figure 1 displays the moderating effects of caregiver syntactic complexity on child effortful control and receptive language.
Table 5.
Results of multiple regression analyses including each dimension of child temperament, syntactic complexity, and their interaction as regressors (controlling for caregiver education).
| Estimating Child Receptive Language from Effortful Control and Caregiver Syntactic Complexity | |||
|
| |||
| Regressors | β | SE | t |
| (Constant) | −14.31* | 4.43 | −3.23 |
| Caregiver Education (Covariate) | .15* | .07 | 2.34 |
| Effortful Control | 2.01* | .87 | 2.31 |
| Syntactic Complexity | 2.64* | .99 | 2.68 |
| Effortful Control x Syntactic Complexity | −.39 | .19 | −2.00 |
| Model Summary | R2 = .55, F(4, 54) = 14.94, p < .001** | ||
|
| |||
| Estimating Child Receptive Language from Negative Affectivity and Caregiver Syntactic Complexity | |||
|
| |||
| Regressors | β | SE | t |
| (Constant) | −6.08 | 3.19 | −1.91 |
| Caregiver Education (Covariate) | .13 | .07 | 1.81 |
| Negative Affectivity | .45 | .78 | .58 |
| Syntactic Complexity | 1.23 | .66 | 1.86 |
| Negative Affectivity x Syntactic Complexity | −.12 | .17 | −.71 |
| Model Summary | R2 = .46, F(4, 54) = 11.68, p < .001** | ||
|
| |||
| Estimating Child Receptive Language from Surgency-Extraversion and Caregiver Syntactic Complexity | |||
|
| |||
| Regressors | β | SE | t |
| (Constant) | 2.19 | 2.85 | .77 |
| Caregiver Education (Covariate) | .16* | .07 | 2.36 |
| Surgency-Extraversion | −1.49* | .62 | −2.41 |
| Syntactic Complexity | −.71 | .62 | −1.13 |
| Surgency-Extraversion x Syntactic Complexity | .33* | .14 | 2.42 |
| Model Summary | R2 = .51, F(4, 54) = 13.91, p < .001** | ||
Note:
p <.05,
p<.001
Estimating Child Receptive Language from Negative Affectivity and Caregiver Syntactic Complexity
The middle portion of Table 5 displays results from the regression models estimating receptive language from negativity affectivity, syntactic complexity, and their interaction with caregiver education as a covariate. The full model was significant, but no individual regressor was significant and no significant interaction between negative affectivity and syntactic complexity was present.
Estimating Child Receptive Language from Surgency-Extraversion and Caregiver Syntactic Complexity
The model including surgency-extraversion, caregiver syntactic complexity, their interaction, and caregiver education (covariate) as regressors estimating receptive language was significant. Surgency-extraversion and the interaction term were significant regressors above and beyond caregivers’ level of education. While the interaction term was significant for this model, F(1, 54) = 5.88, p = .019, ΔR2 = .05, the pick-a-point approach revealed no significant conditional associations between surgency-extraversion and receptive language at the 16th (b = −.258, p = .082), 50th (b = −.084, p = .440), nor 84th (b = .153, p = .220) percentiles of caregiver syntactic complexity. However, the Johnson-Neyman approach revealed significant moderation effects when caregivers used MLUs below 3.48 (b = −.349, p = .050; 5 out of 59 families) and MLUs above 5.73 (b = .389, p = .050; 3 out of 59 families).
DISCUSSION
The purpose of the current study was two-fold: 1) to examine the relation between child temperament, caregiver linguistic input, and child receptive language in children who are DHH; and 2) to investigate caregiver linguistic input as a potential moderator of the relation between child temperament and DHH children’s receptive language. We predicted that relations between child temperament and child receptive language development might extend beyond the infancy period for children who are DHH based on previous findings in other clinical populations who experience challenges toward what is considered typical language development (Singer et al., 2019; Tumanova et al., 2020). Specifically, we expected positive relations between less reactive temperaments (high effortful control, low negative affectivity, surgency-extraversion) and child receptive language outcomes. Furthermore, we hypothesized that the observed relation between child temperament and child receptive language would be moderated by caregiver linguistic input. Whether caregivers produced low or high levels of linguistic input, we expected children with less reactive temperaments to have better receptive language skills than children with more reactive temperaments. This prediction was based on previous literature theorizing that children with stronger regulatory skills achieve better language outcomes because of their ability to leverage cognitive resources to attend to linguistically relevant information from their caregiver(s) (Bloom, 1993; Dixon & Smith, 2000).
Children with HAs and those with CIs were similar in their levels of effortful control and negative affectivity, caregiver linguistic input, and receptive language scores. However, children with CIs were rated higher in level of surgency-extraversion by their caregivers than children with HAs. This difference between the two subgroups may reflect findings that greater behavioral problems associated with impulsivity tend to be found in children with greater degrees of hearing loss (Bigler et al., 2019: Soleimani et al., 2020).
The negative associations between effortful control and negative affectivity and between effortful control and surgency-extraversion in DHH children could be indicative of the role regulatory processes have in inhibiting reactive tendencies (Rothbart et al., 2004). That is, children with high self-regulatory skills are able to better control emotional and behavioral responses to stimuli. We also found that effortful control was positively associated with receptive language in DHH children. Previous findings in TH children who are typically developing have suggested that children with high effortful control tend to have low reactivity and can achieve better language outcomes through focusing their attention on aspects of their environment that support language development (Bloom, 1993; Dixon & Smith, 2000; Morales et al., 2000). The results of the current study could support that similar processes might be occurring in DHH children.
We also found a positive association between child effortful control and caregiver syntactic complexity, but no significant association between child effortful control and caregiver lexical diversity. It could be that caregivers’ use of lexical diversity is not as sensitive to varying levels of effortful control in school-aged children as caregiver syntactic complexity. Aspects of grammatical development are less salient (e.g., morphological rules, grammatical morphemes) and thus are especially difficult for children who are DHH due to their reduced access to auditory information, whereas lexical development may be supported by lexical cues in the auditory input that are redundant and more salient (McGuckian & Henry 2007; Tomblin et al., 2015). Processing grammatically complex language requires a great amount of cognitive effort, especially for DHH children and even DHH adults who must draw from these available cognitive resources to attend to auditory input (Delage & Tuller, 2010; Penke & Wimmer, 2018; Stewart & Wingfield, 2009; Wingfield et al., 2006). DHH children with low effortful control levels may prompt caregivers to adapt and use less complex language during parent-child interactions, whereas DHH children with higher regulatory skills may prompt caregivers to use greater syntactic complexity. Indeed, previous research in families with typically developing children has suggested that caregivers modify their input (e.g., vocabulary use, sentence complexity, etc.) so that their children can better process and respond to their input (Ambrose et al., 2015), which may help support language development for children with low regulatory abilities. Nonetheless, both greater amounts of caregiver lexical diversity and syntactic complexity were associated with better child receptive language, consistent with the literature reporting positive associations between caregiver language (e.g., MLU, number of word types) and receptive and/or expressive language in DHH children (Cruz et al., 2012; Desjardin & Eisenberg, 2007; Nittrouer et al., 2020).
Lastly, no associations were observed between surgency-extraversion or negative affectivity and any of the child and caregiver language measures. The lack of associations for these temperament dimensions, which are centered around children’s reactivity to different stimuli, may be because surgency-extraversion and negative affectivity relate to other developmental domains, such as social development, as seen in typically developing children and adolescents (Sanson et al., 2004).
Our second purpose was to examine if caregiver linguistic input influences the relation between child temperament and child receptive language. We found that DHH children with better effortful control skills could take more advantage of the lexical cues available from their caregivers to achieve better receptive language outcomes when caregiver lexical diversity was low to moderate in level. We found no relation between effortful control and receptive language in DHH children when caregivers used high levels of lexical diversity. Greater caregiver lexical diversity seems to buffer against negative effects of poorer effortful control on receptive language for children who are DHH. When caregivers used higher quality lexical linguistic input, DHH children with lower levels of effortful control performed similarly to their peers with high effortful control in terms of receptive language. Further, we found that the moderating effect of caregiver’s syntactic complexity on child effortful control and child receptive language was only marginally significant, potentially due to our sample being slightly underpowered. Nonetheless, the model examining the moderating role of syntactic complexity showed similar trends as the previous model that included caregiver lexical diversity. Greater child effortful control resulted in better child receptive language when caregivers used low to moderate syntactic complexity, but not when caregiver syntactic complexity was high. These results may suggest that high-quality caregiver input could have a protective influence on receptive language in DHH children.
We did not find associations between child negative affectivity and child receptive language measures at different levels of caregiver lexical diversity and syntactic complexity. While a significant interaction was observed between child surgency-extraversion and caregiver syntactic complexity on child receptive language, these effects only applied to a small subset of our sample. For five families with caregivers producing low MLUs (less than 3.48 during the play interaction), there was a significant negative association between child surgency-extraversion and child receptive language. For three families with caregivers producing MLUs over 5.73, there was a positive association between surgency-extraversion and receptive language. While these associations are based on a very small number of families, future studies could examine the effects of significantly low and high caregiver MLUs on child temperament and child receptive language in this clinical population. Studies may also examine whether child temperament factors and caregiver language interact to influence other areas of development outside of language, including behavior and psychosocial development.
Hearing loss poses a significant risk to the dyadic interactions between caregivers and DHH children (Holt et al., 2020). Previous longitudinal studies in TH infants have supported the role of caregiver input in associations between child temperament and child language outcomes (Spinelli et al., 2018). Our findings, though based on a cross-sectional design, suggest that when caregivers provide a language environment that is more restrictive in vocabulary and grammatical forms, only DHH children with good regulatory skills achieve better language. It appears that when caregivers provided low to moderate levels of lexical diversity and syntactic complexity, DHH children with higher effortful control can leverage their attentional skills to use the limited language input that was available to them to achieve better receptive language outcomes. Children with even a mild hearing loss experience limitations to audibility that can impact the perception of many important aspects of linguistic development including lexical items and morphosyntactic cues (Tomblin et al., 2015). In turn, this reduced access to auditory information would require increased cognitive and listening effort from DHH children so they can attend to sources of linguistic information, such as caregivers. Our findings may highlight the important role of regulatory processes (those of which precede the development of executive functions) for overcoming the negative effects of limited audibility for DHH children. However, caregivers seem to have the ability to help DHH children with varying levels of regulatory skills overcome limitations imposed by their hearing loss by providing a rich language-learning environment.
Contrary to our findings in a sample of DHH children where high levels of caregiver lexical diversity tended to provide a protective influence on children’s receptive language despite their level of effortful control, Spinelli et al. (2018) reported that greater levels of maternal lexical diversity and syntactic complexity only provided a benefit to typically developing toddlers displaying higher attentional skills during infancy. In typically developing toddlers, high levels of syntactic complexity and lexical diversity appeared to be distracting for toddlers with poorer attentional skills, as they showed poorer language production skills compared to more attentive infants (Spinelli et al., 2018). High levels of lexical diversity may help to provide a protective influence in our sample of DHH children with varying effortful control skills (rather than a benefit to only those with high effortful control skills). What may be considered a distraction to TH toddlers and children who have access to a wide range of auditory information may be considered appropriate linguistic input for DHH children who have reduced auditory access. An increase in lexical and grammatical input to DHH children means more opportunities for language learning. Additionally, the differences between our findings and those of Spinelli et al. (2018) could be a result of the age differences between our samples (i.e., toddlers versus school-aged children) or the outcome measure examined (i.e., receptive vs. expressive language). Similar to our results examining the relations between negative affectivity/surgency-extraversion and child receptive language, Spinelli et al. (2018) found no influence of caregiver linguistic input on infant positive affect (i.e., smile and laughter dimension of the IBQ-R) or negative affect (i.e., distress to limitations of the IBQ-R) and language production.
Clinical Implications
Dyadic interactions reflect an important dynamic within the family environment for facilitating language development. Understanding optimal caregiver-child dynamics that promote social interactions and uptake of linguistically-relevant information is important for understanding language development in children, especially DHH children who experience language delays (Niparko et al., 2010; Yoshinaga-Itano et al., 2018). While child temperament is an attribute of the child that is thought to be static over the course of development, caregivers and their language input serve as important modifiable sources of intervention when it comes to positively improving dyadic interactions (Ambrose et al., 2014; Moeller & Tomblin, 2015; Yoshinaga-Itano et al., 2020). Caregivers should be encouraged to employ a rich language-learning environment characterized by high syntactic complexity and lexical diversity to offer some protection from poor language comprehension outcomes for DHH children, especially when DHH children present with challenging temperaments for caregivers (i.e., traits comprising low regulatory abilities and high reactivity). Therefore, consideration of both the child’s temperament and caregiver language input during intervention can prove useful when coaching caregivers on creating rich language environments for their children.
Limitations
The current study implemented a cross-sectional design as a first step in investigating the influence of caregiver language on temperament and language in DHH children. While previous data and theory might suggest how these transactional processes are related, cross-sectional designs cannot establish directionality on their own. Our study explored the moderating effects of caregiver input on child temperament and child receptive language; however, child temperament could serve as a moderator of caregiver linguistic input and child receptive language. Future studies building on this work may employ a longitudinal design to determine directionality of child temperament, caregiver language, and spoken language outcomes in DHH children. In addition, including multiple language measures can capture the complexities of language in children and provide a greater understanding of the role of caregiver language on child language outcomes. Future work incorporating language production measures and additional measures of complex language comprehension may shed a broader light on the interaction child temperament and caregiver language has on child language outcomes. Lastly, although we measured caregiver language during a semi-structured play session within the home environment, measuring dyadic interactions at one point in time may not reflect daily linguistic input caregivers provide to their children.
CONCLUSIONS
Research examining transactional relations between child temperament and caregiver language in TH infants suggest that rich caregiver language provides a benefit to language for infants with high attentional abilities (Spinelli et al., 2018). The current study found that high-quality caregiver language might serve a protective role for language in DHH children, no matter the child’s level of effortful control. It is when caregivers provide lower quality linguistic input that DHH children must resort to tapping into their effortful control skills to achieve better language comprehension. This work preliminarily supports the importance of rich caregiver linguistic input to DHH children, especially for those with low self-regulatory abilities.
Supplementary Material
Supplemental Digital Content 1. Table displaying partial Pearson correlations between child temperament dimensions, caregiver syntactic complexity and lexical diversity, and child receptive language in children with hearing aids and children with cochlear implants.
Acknowledgments
Financial disclosures/conflicts of interest:
This research was supported by grants from the National Institute on Deafness and Other Communication Disorders (NIDCD) of the National Institutes of Health: R01DC014956. The funding organization had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the decision to submit the article for publication; or in the preparation, review, or approval of the article.
REFERENCES
- Ambrose SE, VanDam M, & Moeller MP (2014). Linguistic input, electronic media, and communication outcomes of toddlers with hearing loss. Ear and hearing, 35(2), 139. 10.1097/AUD.0b013e3182a76768 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ambrose SE, Walker EA, Unflat-Berry LM, Oleson JJ, & Moeller MP (2015). Quantity and Quality of Caregivers’ Linguistic Input to 18-Month and 3-Year-Old Children Who Are Hard of Hearing. Ear and hearing, 36 Suppl 1(0 1), 48S–59S. 10.1097/AUD.0000000000000209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Atzaba-Poria N, Deater-Deckard K, & Bell MA (2014). It takes more than one for parenting: How do maternal temperament and child’s problem behaviors relate to maternal parenting behavior? Personality and Individual Differences, 69, 81–86. 10.1016/j.paid.2014.05.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beer J, Kronenberger WG, Castellanos I, Colson BG, Henning SC, & Pisoni DB (2014). Executive functioning skills in preschool-age children with cochlear implants. Journal of speech, language, and hearing research, 57(4), 1521–1534. 10.1044/2014_JSLHR-H-13-0054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beer J, Pisoni DB, Kronenberger WG, & Geers AE (2010). New research findings: Executive functions of adolescents who use cochlear implants. The ASHA Leader, 15(15), 12–14. 10.1044/leader.FTR2.15152010.12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bigler D, Burke K, Laureano N, Alfonso K, Jacobs J, & Bush ML (2019). Assessment and treatment of behavioral disorders in children with hearing loss: A systematic review. Otolaryngology–Head and Neck Surgery, 160(1), 36–48. 10.1177/0194599818797598 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bloom L (1993). The transition from infancy to language: Acquiring the power of expression. Cambridge University Press. [Google Scholar]
- Bridgett DJ, Oddi KB, Laake LM, Murdock KW, & Bachmann MN (2013). Integrating and differentiating aspects of self-regulation: effortful control, executive functioning, and links to negative affectivity. Emotion, 13(1), 47–63. 10.1037/a0029536 [DOI] [PubMed] [Google Scholar]
- Carrow-Woolfolk E & Lynch J (1982). Comprehensive Assessment of Spoken Language, Second Edition (CASL-2). Torrance, CA: Western Psychological Services. [Google Scholar]
- Chen N, Deater-Deckard K, & Bell MA (2014). The role of temperament by family environment interactions in child maladjustment. Journal of abnormal child psychology, 42(8), 1251–1262. 10.1007/s10802-014-9872-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conture EG, Kelly EM, & Walden TA (2013). Temperament, speech and language: An overview. Journal of Communication Disorders, 46(2), 125–142. 10.1016/j.jcomdis.2012.11.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cruz I, Quittner AL, Marker C, & DesJardin JL (2013). Identification of effective strategies to promote language in deaf children with cochlear implants. Child Development, 84, 543–559. 10.1111/j.1467-8624.2012.01863.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deater-Deckard K, Mullineaux PY, Beekman C, Petrill SA, Schatschneider C, & Thompson LA (2009). Conduct problems, IQ, and household chaos: A longitudinal multi- informant study. Journal of Child Psychology and Psychiatry, 50(10), 1301–1308. 10.1111/j.1469-7610.2009.02108.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Delage H, & Tuller L (2010). Evolution of syntactic complexity and avoidance strategies in children and adolescents with mild-to-moderate hearing loss. In Language Acquisition and Development: Proceedings of GALA 2009 (pp. 107–120). Cambridge Scholars Publishing Newcastle, UK. [Google Scholar]
- DesJardin JL, Doll ER, Stika CJ, Eisenberg LS, Johnson KJ, Ganguly DH, Colson BG, & Henning SC (2014). Parental support for language development during joint book reading for young children with hearing loss. Communication Disorders Quarterly, 35(3), 167–181. 10.1177/1525740113518062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- DesJardin JL, & Eisenberg LS (2007). Maternal contributions: Supporting language development in young children with cochlear implants. Ear and Hearing, 28, 456–69. 10.1097/AUD.0b013e31806dc1ab [DOI] [PubMed] [Google Scholar]
- Dixon WE Jr, & Smith PH (2000). Links between early temperament and language acquisition. Merrill-Palmer Quarterly (1982-), 46(3), 417–440. https://www.jstor.org/stable/23093739 [Google Scholar]
- Elliot C (2007). Differential Abilities Scale—2nd edition (DAS-II) manual. San Antonio, TX: Harcourt Assessment, Inc. [Google Scholar]
- Gartstein MA, & Rothbart MK (2003). Studying infant temperament via the revised infant behavior questionnaire. Infant behavior and development, 26(1), 64–86. 10.1016/S0163-6383(02)00169-8 [DOI] [Google Scholar]
- Geers AE, Moog JS, Biedenstein J, Brenner C, & Hayes H (2009). Spoken language scores of children using cochlear implants compared to hearing age-mates at school entry. Journal of Deaf Studies and Deaf Education, 14, 371–385. 10.1093/deafed/enn046 [DOI] [PubMed] [Google Scholar]
- Geers AE, Moog JS, & Rudge AM (2019). Effects of frequency of early intervention on spoken language and literacy levels of children who are deaf or hard of hearing in preschool and elementary school. Journal of Early Hearing Detection and Intervention, 4(1), 15–27. 10.26077/7pxh-mx41 [DOI] [Google Scholar]
- Goldsmith HH, Buss AH, Plomin R, Rothbart MK, Thomas A, Chess S, Hinde RA, & McCall RB (1987). Roundtable: What is temperament? Four approaches. Child development, 58, 505–529. [PubMed] [Google Scholar]
- Gouge NB, Temperament-Language Relationships during the First Formal Year of School. (2011). Electronic Theses and Dissertations. Paper 1288. https://dc.etsu.edu/etd/1288 [Google Scholar]
- Hayes AF (2017). Introduction to mediation, moderation, and conditional process analysis: A regression based approach (Second Ed.). New York, NY: Guilford Press. [Google Scholar]
- Hoff E (2006). How social contexts support and shape language development. Developmental review, 26(1), 55–88. 10.1016/j.dr.2005.11.002 [DOI] [Google Scholar]
- Holt RF, Beer J, Kronenberger WG, Pisoni DB, & Lalonde K (2012). Contribution of family environment to pediatric cochlear implant users’ speech and language outcomes: some preliminary findings. Journal of speech, language, and hearing research : JSLHR, 55(3), 848–864. 10.1044/1092-4388(2011/11–0143) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holt RF, Beer J, Kronenberger WG, Pisoni DB, Lalonde K, & Mulinaro L (2020). Family environment in children with hearing aids and cochlear implants: Associations with spoken language, psychosocial functioning, and cognitive development. Ear and hearing, 41(4), 762–774. 10.1097/AUD.0000000000000811 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holt RF, Kronenberger WG, & Pisoni DB (2022). Family Environmental Dynamics Differentially Influence Spoken Language Development in Children With and Without Hearing Loss. Journal of Speech, Language, and Hearing Research, 65(1), 361–377. 10.1044/2021_JSLHR-21-00220 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holt RF, & Svirsky MA (2008). An exploratory look at pediatric cochlear implantation: is earliest always best?. Ear and hearing, 29(4), 492–511. 10.1097/AUD.0b013e31816c409f [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karrass J & Braungart-Rieker JM (2003). Parenting and Temperament as Interacting Agents in Early Language Development, Parenting, Science and Practice, 3(3), 235–259. 10.1207/S15327922PAR0303_03 [DOI] [Google Scholar]
- Kelly C, Morgan G, Freeth M, Siegal M, & Matthews D (2019). The Understanding of Communicative Intentions in Children with Severe-to-Profound Hearing Loss. The Journal of Deaf Studies and Deaf Education, 24(3), 245–254. 10.1093/deafed/enz001 [DOI] [PubMed] [Google Scholar]
- Kiff CJ, Lengua LJ, & Zalewski M (2011). Nature and nurturing: Parenting in the context of child temperament. Clinical child and family psychology review, 14(3), 251–301. 10.1007/s10567-011-0093-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kronenberger WG (2019). Executive Functioning and Language Development in Children with Cochlear Implants. Cochlear implants international, 20(Suppl 1), 2–5. [PMC free article] [PubMed] [Google Scholar]
- Kronenberger WG, Beer J, Castellanos I, Pisoni DB, & Miyamoto RT (2014). Neurocognitive risk in children with cochlear implants. JAMA Otolaryngology–Head & Neck Surgery, 140(7), 608–615. 10.1001/jamaoto.2014.757 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kronenberger WG, Xu H, & Pisoni DB (2020). Longitudinal development of executive functioning and spoken language skills in preschool-aged children with cochlear implants. Journal of Speech, Language, and Hearing Research, 63(4), 1128–1147. 10.1044/2019_JSLHR-19-00247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laake LM, & Bridgett DJ (2018). Early language development in context: interactions between infant temperament and parenting characteristics. Early Education and Development, 29(5), 730–746. 10.1080/10409289.2018.1436366 [DOI] [Google Scholar]
- Lane KJ, Nelson TM, Thikkurissy S, & Scott JM (2015). Assessing temperament as a predictor of oral sedation success using the Children’s Behavior Questionnaire Short Form. Pediatric Dentistry, 37(5), 429–435. http://hdl.handle.net/1773/26310 [PubMed] [Google Scholar]
- Liberatos P, Link BG, & Kelsey JL (1988). The measurement of social class in epidemiology. Epidemiologic reviews, 10(1), 87–121. 10.1093/oxfordjournals.epirev.a036030 [DOI] [PubMed] [Google Scholar]
- Loi EC, Vaca K, Ashland MD, Marchman VA, Fernald A, & Feldman HM (2017). Quality of caregiver-child play interactions with toddlers born preterm and full term: Antecedents and language outcome. Early human development, 115, 110–117. 10.1016/j.earlhumdev.2017.10.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacWhinney B (2000). The CHILDES Project: Tools for Analyzing Talk: Volume I: Transcription Format and Programs, Volume II: The Database. Cambridge, MA: MIT Press. 10.1016/S0163-6383(01)00038-8 [DOI] [Google Scholar]
- McClelland GH, & Judd CM (1993). Statistical difficulties of detecting interactions and moderator effects. Psychological Bulletin, 114, 376–390. 10.1037/0033-2909.114.2.376 [DOI] [PubMed] [Google Scholar]
- McGuckian M, & Henry A (2007). The grammatical morpheme deficit in moderate hearing impairment. International Journal of Language & Communication Disorders, 42(S1), 17–36. 10.1080/13682820601171555 [DOI] [PubMed] [Google Scholar]
- Mehra S, Eavey RD, & Keamy DG Jr (2009). The epidemiology of hearing impairment in the United States: newborns, children, and adolescents. Otolaryngology-Head and Neck Surgery, 140(4), 461–472. 10.1016/j.otohns.2008.12.022 [DOI] [PubMed] [Google Scholar]
- Morales M, Mundy P, Delgado CE, Yale M, Neal R, & Schwartz HK (2000). Gaze following, temperament, and language development in 6-month-olds: A replication and extension. Infant Behavior and Development, 23(2), 231–236. [Google Scholar]
- Miller J, & Iglesias A (2012). Systematic analysis of language transcripts (SALT), Research Version 2012 [Computer Software]. Middleton, WI: SALT Software, LLC. [Google Scholar]
- Moeller MP, & Tomblin JB (2015). An Introduction to the Outcomes of Children with Hearing Loss Study. Ear and hearing, 36(Suppl 1), 4S–13S. 10.1097/AUD.0000000000000210 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neuhauser A (2018). Predictors of maternal sensitivity in at-risk families. Early Child Development and Care, 188(2), 126–142. 10.1080/03004430.2016.1207065 [DOI] [Google Scholar]
- Neville HJ, Stevens C, Pakulak E, Bell TA, Fanning J, Klein S, & Isbell E (2013). Family-based training program improves brain function, cognition, and behavior in lower socioeconomic status preschoolers. Proceedings of the national academy of sciences, 110(29), 12138–12143. 10.1073/pnas.1304437110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Niparko JK, Tobey EA, Thal DJ, Eisenberg LS, Wang N-Y, Quittner AL, & Fink NE (2010). Spoken language development in children following cochlear implantation. Journal of the American Medical Association, 303(15), 1498–1506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nittrouer S, Lowenstein JH, & Antonelli J (2020). Parental language input to children with hearing loss: Does it matter in the end? Journal of Speech, Language, and Hearing Research, 63(1), 234–258. 10.1044/2019_JSLHR-19-00123 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Penke M, & Wimmer E (2018). Deficits in comprehending wh-questions in children with hearing loss–the contribution of phonological short-term memory and syntactic complexity. Clinical linguistics & phonetics, 32(3), 267–284. 10.1080/02699206.2017.1350883 [DOI] [PubMed] [Google Scholar]
- Putnam SP, & Rothbart MK (2006). Development of short and very short forms of the Children’s Behavior Questionnaire. Journal of personality assessment, 87(1), 102–112. 10.1207/s15327752jpa8701_09 [DOI] [PubMed] [Google Scholar]
- Roberts MY (2019). Parent-implemented communication treatment for infants and toddlers with hearing loss: A randomized pilot trial. Journal of Speech, Language, and Hearing Research, 62(1), 143–152. 10.1044/2018_JSLHR-L-18-0079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rothbart MK, & Bates JE (2006). Temperament.
- Rothbart MK, & Posner MI (2022). Individual differences in temperament and the efficiency of brain networks. Current Opinion in Behavioral Sciences, 43, 242–248. 10.1016/j.cobeha.2021.11.001 [DOI] [Google Scholar]
- Rothbart MK, Ahadi SA, Hershey KL, & Fisher P (2001). Investigations of temperament at three to seven years: The Children’s Behavior Questionnaire. Child Development, 72(5), 1394–1408. 10.1111/1467-8624.00355 [DOI] [PubMed] [Google Scholar]
- Rothbart MK, Ellis LK, & Posner MI (2004). Temperament and self-regulation. Handbook of self-regulation: Research, theory, and applications, 2, 441–460. [Google Scholar]
- Rothbart MK, Ellis LK, Rosario Rueda M, & Posner MI (2003). Developing mechanisms of temperamental effortful control. Journal of personality, 71(6), 1113–1144. 10.1111/1467-6494.7106009 [DOI] [PubMed] [Google Scholar]
- Salley B, Miller A, & Bell MA (2013). Associations between temperament and social responsiveness in young children. Infant And Child Development, 22(3), 270–288. 10.1002/icd.1785 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sameroff A (2010). A unified theory of development: A dialectic integration of nature and nurture. Child development, 81(1), 6–22. 10.1111/j.1467-8624.2009.01378.x [DOI] [PubMed] [Google Scholar]
- Sanson A, Hemphill SA, & Smart D (2004). Connections between temperament and social development: A review. Social Development, 13(1), 142–170. 10.1046/j.1467-9507.2004.00261.x [DOI] [Google Scholar]
- Schmidt H, Daseking M, Gawrilow C, Karbach J, & Kerner auch Koerner J (2022). Self-regulation in Preschool: Are Executive Function and Effortful Control Overlapping Constructs? Developmental Science, 25, 1–13. 10.1111/desc.13272 [DOI] [PubMed] [Google Scholar]
- Semel E, Wiig EH, & Secord W (2004). Clinical Evaluation of Language Fundamentals Preschool–Second Edition. Pearson. [Google Scholar]
- Semel E, Wiig EH, & Secord W (2013). Clinical Evaluation of Language Fundamentals–Fifth Edition. Pearson. [Google Scholar]
- Shiner RL, Buss KA, McClowry SG, Putnam SP, Saudino KJ, & Zentner M (2012). What is temperament now? Assessing progress in temperament research on the Twenty-Fifth Anniversary of Goldsmith et al. (1987). Child Development Perspectives, 6(4), 436–444. 10.1111/j.1750-8606.2012.00254.x [DOI] [Google Scholar]
- Singer CM, Walden TA, & Jones RM (2019). Differences in the relation between temperament and vocabulary based on children’s stuttering trajectories. Journal of communication disorders, 78, 57–68. 10.1016/j.jcomdis.2019.01.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slagt M, Dubas JS, Deković M, & van Aken MAG (2016). Differences in sensitivity to parenting depending on child temperament: A meta-analysis. Psychological Bulletin, 142(10), 1068–1110. 10.1037/bul0000061 [DOI] [PubMed] [Google Scholar]
- Slomkowski CL, Nelson K, Dunn J, & Plomin R (1992). Temperament and language: Relations from toddlerhood to middle childhood. Developmental Psychology, 28(6), 1090–1095. 10.1037/0012-1649.28.6.1090 [DOI] [Google Scholar]
- Soleimani R, Jalali MM, & Faghih HA (2020). Comparing the prevalence of attention deficit hyperactivity disorder in hearing-impaired children with normal-hearing peers. Archives de Pédiatrie, 27(8), 432–435. 10.1016/j.arcped.2020.08.014 [DOI] [PubMed] [Google Scholar]
- Spinelli M, Fasolo M, Shah PE, Genovese G, & Aureli T (2018). The influence of early temperament on language development: the moderating role of maternal input. Frontiers in Psychology, 9, 1–13. 10.3389/fpsyg.2018.01527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stewart R, & Wingfield A (2009). Hearing loss and cognitive effort in older adults’ report accuracy for verbal materials. Journal of the American Academy of Audiology, 20(2), 147–154. 10.3766/jaaa.20.2.7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Su BM, & Chan DK (2017). Prevalence of hearing loss in US children and adolescents: findings from NHANES 1988–2010. JAMA Otolaryngology–Head & Neck Surgery, 143(9), 920–927. 10.1001/jamaoto.2017.0953 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomblin JB, Harrison M, Ambrose SE, Walker EA, Oleson JJ, & Moeller MP (2015). Language outcomes in young children with mild to severe hearing loss. Ear and Hearing, 36(1), 76S–91S. 10.1097/AUD.0000000000000219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tumanova V, Woods C, & Razza R (2020). The role of behavioral inhibition for conversational speech and language characteristics of preschool-age children who stutter. American journal of speech-language pathology, 29(2), 638–651. 10.1044/2019_AJSLP-19-00026 [DOI] [PubMed] [Google Scholar]
- Walker E. A. Ward, Oleson C, Sapp JJ, McCreery C, Tomblin R, J. B. & Moeller M (2022). Language Growth in Children with Mild to Severe Hearing Loss who Received Early Intervention by 3 Months or 6 Months of Age. Journal of Early Hearing Detection and Intervention, 7(1), 1–10. 10.26077/e97b-7add [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiefferink CH, Rieffe C, Ketelaar L, & Frijns JH (2012). Predicting social functioning in children with a cochlear implant and in normal-hearing children: The role of emotion regulation. International journal of pediatric otorhinolaryngology, 76(6), 883–889. 10.1016/j.ijporl.2012.02.065 [DOI] [PubMed] [Google Scholar]
- Wingfield A, McCoy SL, Peelle JE, Tun PA, & Cox CL (2006). Effects of adult aging and hearing loss on comprehension of rapid speech varying in syntactic complexity. Journal of the American Academy of Audiology, 17(7), 487–497. [DOI] [PubMed] [Google Scholar]
- Yoshinaga-Itano C, Sedey AL, Mason CA, Wiggin M, & Chung W (2020). Early intervention, parent talk, and pragmatic language in children with hearing loss. Pediatrics, 146(Suppl 3), S270–S277. 10.1542/peds.2020-0242F [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yoshinaga-Itano C, Sedey AL, Wiggin M, & Mason CA (2018). Language outcomes improved through early hearing detection and earlier cochlear implantation. Otology & Neurotology, 39(10), 1256–1263. 10.1097/MAO.0000000000001976 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Digital Content 1. Table displaying partial Pearson correlations between child temperament dimensions, caregiver syntactic complexity and lexical diversity, and child receptive language in children with hearing aids and children with cochlear implants.