

Abstract
A 13-year-old male patient presented with right leg pain and walking difficulty. Contrast-enhanced magnetic resonance imaging showed a softtissue lesion between muscle groups in the anterior half of the right thigh. The excisional biopsy result ended in an inflammatory myofibroblastic tumor (IMT). The 18F-fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT) scan showed hypermetabolism in the multifocal soft tissue lesion and also confirmed that no other distant foci were present. A three-phase Tc-99m-methylene diphosphonate study of the region showed heterogeneously increased vascularity within the region. We described an unusual case of IMT in a pediatric patient and the importance of PET/CT scanning to delineate the lesion.
Keywords: Inflammatory myofibroblastic tumor, bone scan, magnetic resonance imaging, 18F-FDG PET/CT
Abstract
On üç yaşında erkek hasta sağ bacakta ağrı ve yürümede zorluk ile başvurdu. Kontrastlı manyetik rezonans görüntülemede sağ uyluk ön grup kasları arasında yumuşak doku lezyonu saptandı. Yapılan eksizyonel biyopsi sonucu enflamatuvar miyofibroblastik tümör (İMT) olarak sonuçlandı. 18F-florodeoksiglukoz (18F-FDG) pozitron emisyon tomografisi/bilgisayarlı tomografi (PET/BT) çalışmasında uzak metastaz olmaksızın yumuşak doku lezyonunda multifokal hipermetabolizma izlendi. Üç fazlı Tc-99m-metilendifosfonat çalışmasında, bölgede heterojen artmış vaskülarite izlendi. Biz pediyatrik bir hastada sıra dışı bir İMT olgusu ve lezyonu tanımlamada 18F-FDG PET/BT’nin önemini anlattık.
Figure 1.
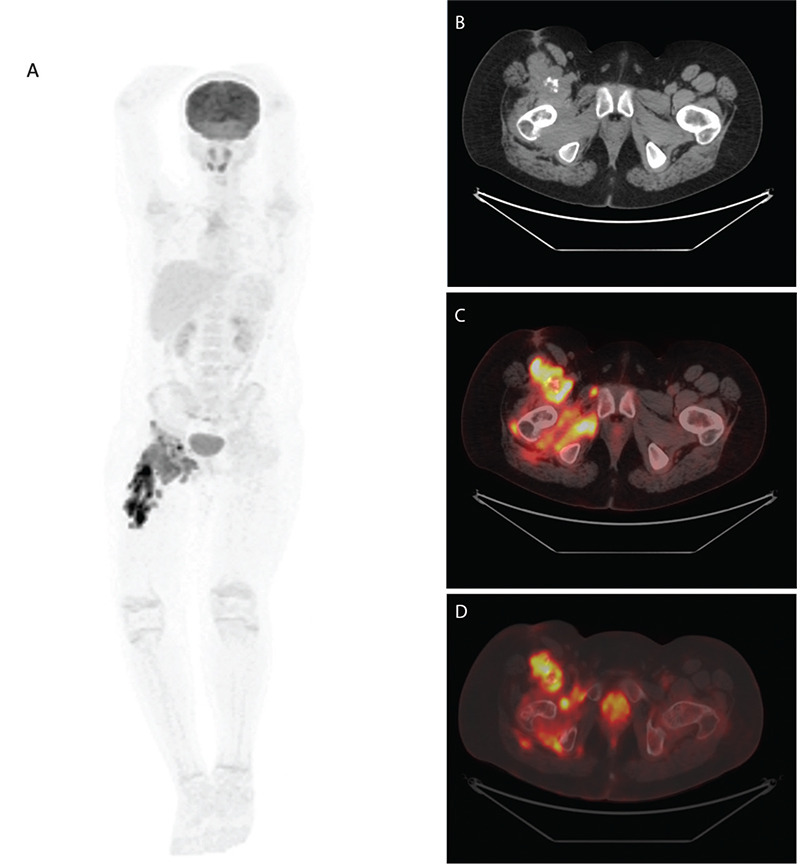
A 13-year-old male patient with an inflammatory myofibroblastic tumor of the right thigh. Maximum intensity projection 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) image (A), axial computed tomography (CT) (B), and axially fused 18F-FDG PET image (C) showed increased 18F-FDG uptake [maximum standardized uptake value (SUVmax): 28.60] in the multifocal mass with heterogeneous calcifications through the anterior part of the femur. Bone structure findings in the axial CT bone window (D) are within normal limits.
Figure 2.
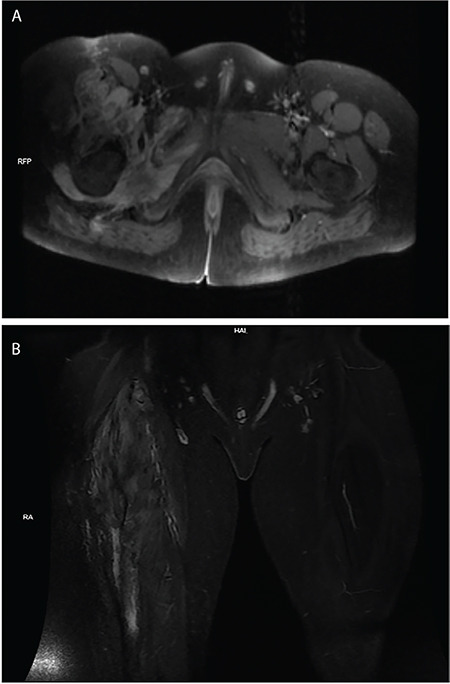
Axial T1-weighted magnetic resonance imaging (MRI) image (A) shows an inhomogeneous hypointense mass in the anterior right thigh. The lesion shows an inhomogeneous hyperintense signal on MRI coronal STIR images (B).
Figure 3.
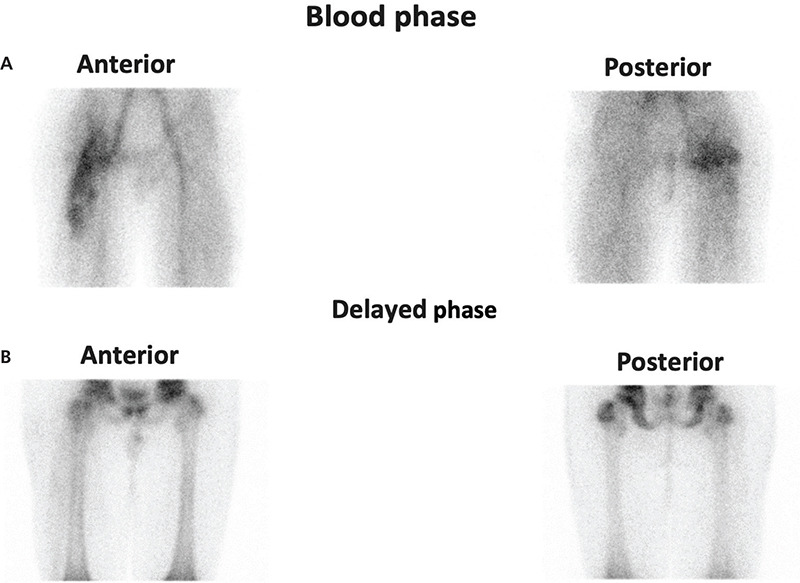
Triphasic Tc-99m-methylene diphosphonate bone scan of the upper part of lower extremities demonstrated heterogeneously increased vascularity and perfusion of the right proximal half of the femur and the right acetabular region (A). A minimal reduction in activity accumulation was observed in the right hip epiphyseal line compared to the contralateral side. However, there was no increased activity accumulation at nearby pelvic bones and the right femur on delayed images (B). An excisional biopsy was performed for the mass measuring 35x25x10 mm with a soft consistency, creamy white and brown in places. The diagnosis of inflammatory myofibroblastic tumors (IMT) was confirmed histopathologically with a large number of lymphoplasmacytic cells, destroying muscle structure. No significant mitotic activity and necrosis were observed. Ki-67 positive tumor cells accounted for approximately 5-6%. IMT is a neoplasm of intermediate biological potential with partial local invasion and recurrence, but they rarely metastasize (1). IMTs can occur in various systems including central nervous system, internal organs, and extremities (2,3). Older children can sometimes be affected by this disease, and it has also been reported as a very rare condition (4). The specific pathogenesis of IMT is unknown, while various infections, inflammatory and autoimmune diseases, and trauma are among the most commonly suspected etiologies of the disease. The clinical presentation of IMT varies depending on the anatomical location and it sometimes mimics lymphoma (5). Patients generally present with general inflammatory symptoms such as fever, weight loss, pain, and malaise which may also raise suspicion of lymphoproliferative malignancies. CT and MR are the most commonly used imaging modalities when evaluating of IMTs. In most cases, a histological examination must be carried out for a reliable diagnosis. 18F-FDG PET/CT scan is useful for detection of primary tumor, local recurrence, treatment response, and distant metastasis (6,7). Histopathologically our case showed low mitotic activity and indicates the uptake of 18F-FDG, mainly related to high glucose utilization of the inflammatory cells contained in the tumor. PET/CT helps in delineating the tumor burden to guide surgery and thus prevents the damage to normal anatomical structures. The best treatment strategy for this type of tumor is complete resection if achieved surgically. Due to the high 18F-FDG avidity of the tumor, the PET/CT scan is also useful to identify local recurrence after resection of the primary tumor.
Footnotes
Ethics
Informed Consent: The patient consent was obtained.
Peer-review: Externally peer-reviewed.
Authorship Contributions
Concept: N.C.M.G., Design: N.C.M.G., Data Collection or Processing: R.Y., A.Y., Analysis or Interpretation: R.Y., N.C.M.G., Literature Search: R.Y., A.Y., Writing: R.Y., N.C.M.G.
Conflict of Interest: No conflicts of interest were declared by the authors.
Financial Disclosure: The authors declare that this study has received no financial support.
References
- 1.Savvidou OD, Sakellariou VI, Papakonstantinou O, Skarpidi E, Papagelopoulos PJ. Inflammatory myofibroblastic tumor of the thigh: presentation of a rare case and review of the literature. Case Rep Orthop. 2015;2015:814241. doi: 10.1155/2015/814241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Raad RA, Haddad L, Jabbour T, El-Rassi Z. Inflammatory Myofibroblastic Tumor of the Liver Mimicking Metastasis on 18F-FDG PET/CT. Clin Nucl Med. 2021;46:47–48. doi: 10.1097/RLU.0000000000003356. [DOI] [PubMed] [Google Scholar]
- 3.Liu H, Yang X, Fan D, Lv T, Chen Y. Mesenteric Inflammatory Myofibroblastic Tumor on 68Ga-FAPI PET/CT. Clin Nucl Med. 2021;46:1026–1027. doi: 10.1097/RLU.0000000000003797. [DOI] [PubMed] [Google Scholar]
- 4.Dalton BG, Thomas PG, Sharp NE, Manalang MA, Fisher JE, Moir CR, St Peter SD, Iqbal CW. Inflammatory myofibroblastic tumors in children. J Pediatr Surg. 2016;51:541–544. doi: 10.1016/j.jpedsurg.2015.11.015. [DOI] [PubMed] [Google Scholar]
- 5.Ma C, Lu J, Chen G, Wang W, Su F, Su X. Inflammatory myofibroblastic tumor mimicking lymphoma on 18F-FDG PET/CT. Report of a case and review of the literature. Hell J Nucl Med. 2018;21:77–80. doi: 10.1967/s002449910710. [DOI] [PubMed] [Google Scholar]
- 6.Dong A, Wang Y, Dong H, Gong J, Cheng C, Zuo C, Lu J. Inflammatory myofibroblastic tumor: FDG PET/CT findings with pathologic correlation. Clin Nucl Med. 2014;39:113–121. doi: 10.1097/RLU.0b013e3182952caa. [DOI] [PubMed] [Google Scholar]
- 7.Jiang JY, Comsa M, Wong VCK, Mansberg R. Steroid responsive inflammatory myofibroblastic tumor of the lung evaluated by FDG PET/CT imaging. Radiol Case Rep. 2022;17:907–910. doi: 10.1016/j.radcr.2021.11.049. [DOI] [PMC free article] [PubMed] [Google Scholar]