

Abstract
Objectives
Oral feeding in preterm infants is a complex and dynamic process involving oral motor development and interaction between the neurological, cardiorespiratory, and gastrointestinal systems. Oral motor stimulation (OMS) is defined as stimulating the oropharyngeal components such as the lips, jaw, tongue, and soft palate with fingers in preterm infants to increase their feeding skills. In this study, we aimed to evaluate the effect of OMS exercises on the sucking and swallowing skills of preterm infants and demonstrate the utility of objective scales to evaluate infants’ readiness for oral feeding.
Methods
This single-center, prospective cohort study was conducted between June 1st and December 31st, 2020, which included preterm infants born at ≤34 weeks of gestation and admitted to the neonatal intensive care unit of our hospital. All procedures of the OMS program were performed once a day, 5 times a week by a language and speech therapist who is an expert in oral feeding skills (OFS) staging and non-nutritive sucking (NNS) scoring. All infants were followed up until discharge with a weekly evaluation of OFS staging and NNS scoring.
Results
A total of 50 infants were included in this prospective cohort study. The mean birth weight was 1376.9±372 g, and the median gestational age was 30 weeks (interquartile range: 25–34). The comparison of OFS stages on day 5 and day 10 of OMS revealed a significant increase (p<0.001). Similarly, there was a significant improvement in the NNS scores on days 5 and 10 compared to the baseline.
Conclusion
In preterm infants, OMS during the transition from gavage feeding to oral feeding improves feeding skills.
Keywords: Feeding skills, oral motor stimulation, preterm
Oral feeding in preterm infants is a complex and dynamic process involving oral motor development and interaction between the neurological, cardiorespiratory, and gastrointestinal systems.[1-3] Inability to reach adequate feeding delays hospital discharge, resulting in the infant having longer exposure to the adverse environmental conditions of the neonatal intensive care unit (NICU) and nosocomial infectious agents.[3-6] Causes of oral feeding difficulties in preterm infants include poor sucking organization, uncoordinated suck-swallow-breath pattern, and oral hypersensitivity to touch.[7-11] Although suck-swallow coordination begins in the intrauterine period, the integration of breathing to achieve successful feeding skills is not expected before 32–34 weeks of gestation.[12,13] The numerous adverse factors to which preterm infants are subjected during intensive care delay this period further. Oral motor stimulation (OMS) is motor stimulation of the lips, jaws, tongue, and soft palate with the finger to activate the oropharyngeal mechanism. Therefore, early OMS exercises are used in preterm infants to promote the attainment of oral feeding skills (OFS). Previous studies have shown that OMS can improve OFS and shorten the transition to oral feeding.[14] In this study, we aimed to evaluate the effect of OMS exercises on the sucking and swallowing skills of preterm infants and demonstrate the utility of objective scales to evaluate infants’ readiness for oral feeding.
Methods
This single-center, prospective cohort study was approved by the Ethics Committee of our hospital (No: 09, dated February 11, 2021). Parental consents were obtained before the patients were included in the study. Our study was conducted in accordance with the Helsinki Declaration.
Participants
The study included preterm infants born at ≤34 weeks of gestation and admitted to the NICU of our hospital between June 1st and December 31st, 2020. Patients with major congenital anomaly, cleft palate-lip, gastrointestinal anomaly, small for gestational age, and severe asphyxia were excluded from the study. All patients were followed up from admission to discharge.
Assessment Tools and OMS Procedure
Two different assessment tools were used to evaluate the patients’ OFS and monitor their development.
The OFS grading developed by Lau and Smith is an objective scale for assessing infants’ OFS.[15] (Fig. 1) If the infant had no oral intake on evaluation on day 0 of the OMS program, they were evaluated as level 1. The patients were reevaluated on day 5 and day 10 of the program. Infants were reevaluated at 5-day intervals until they reached level 4, which is considered successful oral feeding.
Figure 1.
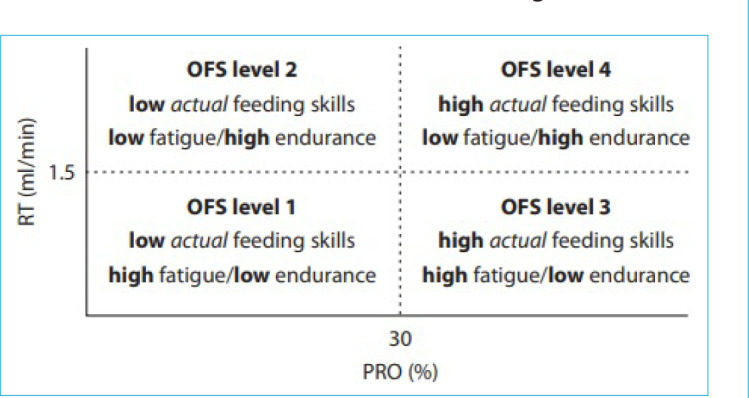
Oral feeding skill.
RT: Rate of milk transfer over an entire feeding; PRO: % volume taken during the first 5 min/total volume.
The non-nutritive sucking (NNS) scoring system developed by Neiva et al.[16] was implemented on days 0, 5, and 10 of the OMS programs (Fig. 2). Based on this assessment, oral feeding was not attempted for infants with scores ≤33. Infants with scores ≥50 were evaluated as ready for oral feeding. Moreover, the group in between (infants with scores of 33–49) was challenged once each day as recommended by the language and speech therapist (LST).
Figure 2.
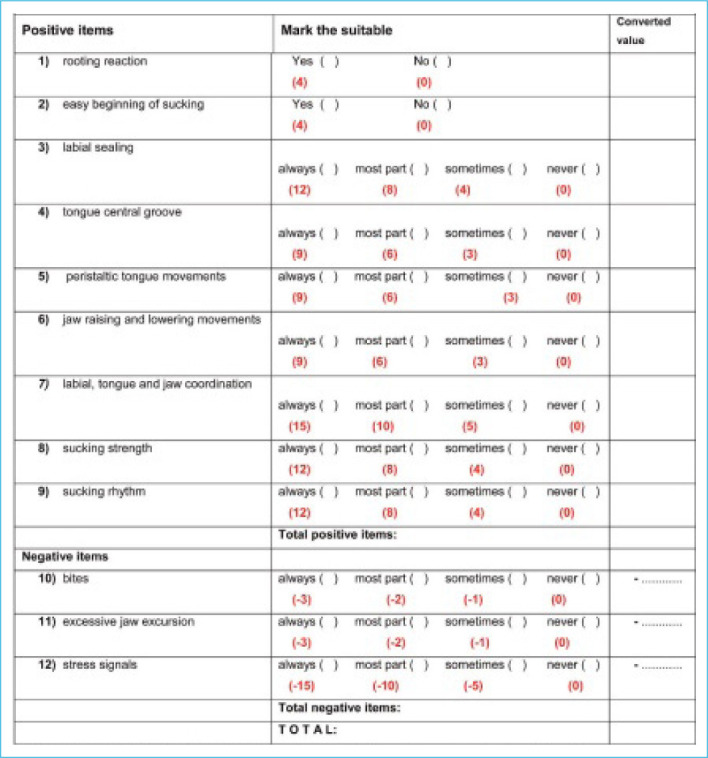
Non-nutritive sucking scoring (NNS score).
The OMS program was initiated at 30 weeks of corrected age for infants <30 weeks of gestational age and right after the 1st day of life for infants >30 weeks of gestational age if the infants are clinically stable and not intubated. Non-invasive ventilation was not a contraindication for the OMS program. The procedure was performed in these physiologically stable infants 15–30 min before tube feeding.[17] Painful and tiring interventions (e.g., ophthalmologic examination and blood collection) were not performed on the infants for at least 30 min before evaluation and the oral stimulation procedure. The procedures were based on the oral stimulation program described by Fucile et al.[17] (Fig. 3). The intervention included movements performed in the perioral and intraoral regions and lasted a total of 12 min. The exercises were performed once a day 5 times a week, after hand-wash and with the use of powder-free gloves. Before the procedure, the infants were awakened and placed in the supine position in the incubator. An LST performed the intervention through the doors of the incubator without removing the infant. Oral stimulation was followed by 3 min of NNS.[17] The procedure was terminated if infants showed any signs of distress, such as desaturation, bradycardia, and apnea. To assess the patients’ oral motor skills, NNS scoring was done before OMS and on days 5 and 10 of OMS, and OFS level was determined on day 5 of OMS.[15,16]
Figure 3.
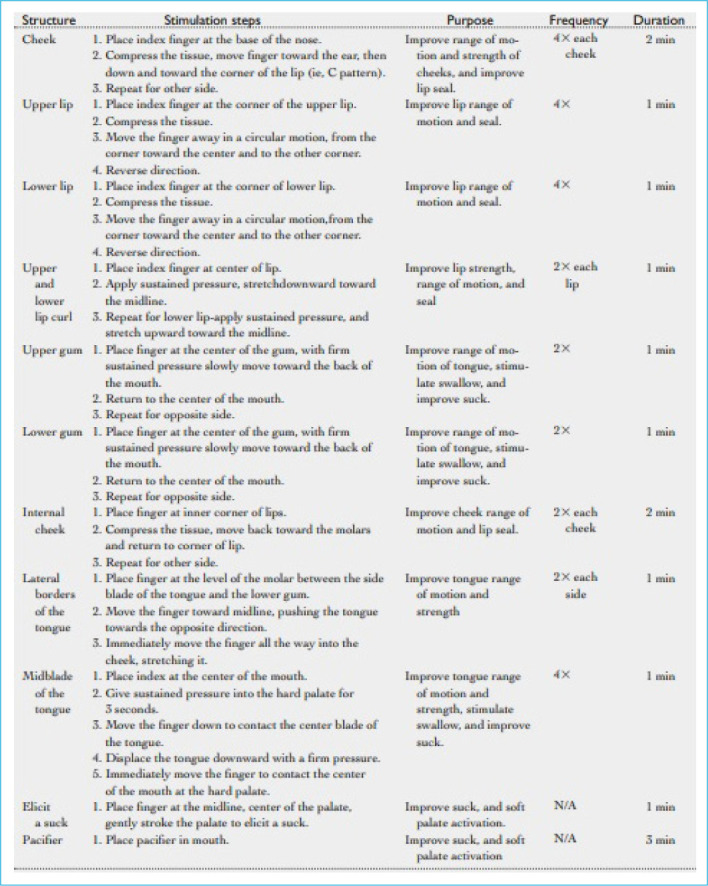
Oral motor stimulation program.
The achievement of full oral feeding was accepted when patients were fed orally with 150 mL/kg for 72 h.
Statistical Analysis
All statistical analyses were performed using the SPSS version 21.0 (IBM Corp, Armonk, NY, USA) statistical software. Data were presented as mean±standard deviation for normally distributed continuous variables, median and interquartile range (IQR) for non-normally distributed continuous variables, and n (%) for categorical variables. Statistical significance was accepted at p<0.05. Non-normally distributed data were analyzed with the Wilcoxon signed-rank test. After the Bonferroni correction, statistical significance was accepted at <0.016.
Sample Size
Based on our previous data from our NICU, we hypothesized that to reveal a 20% decrease in corrected age at full enteral feeding, with a two-sided alpha error of 0.05 and a beta error of 0.2 (80% power), the estimated sample size was 34.
Results
A total of 50 infants were included in this prospective cohort study as shown in the study flowchart (Fig. 4). Of these, 66% were born by cesarean section. The mean birth weight was 1376.9±372 g, and the median gestational age was 30 weeks (range: 25–34). The demographic characteristics of the patients are given in Table 1.
Figure 4.
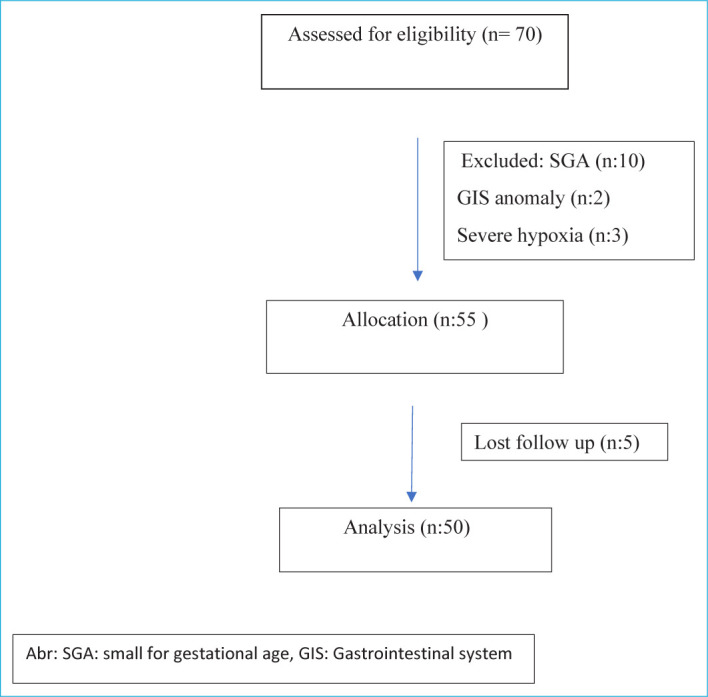
Study flow chart.
Table 1.
Demographic characteristics of the patients
| Patient characteristics | Study group (n=50) |
|---|---|
| Birth weight, g, mean±SD | 1376.9±372 |
| Gestational age, weeks, median (IQR) | 30 (25–34) |
| Gender, male, n (%) | 29 (58%) |
| 5-min Apgar score, median (IQR) | 7 (5–10) |
| Mode of birth, C/S, n (%) | 43 (86%) |
| Intracranial hemorrhage (stage ≥3, %) | 6% |
| NEC (stage ≥2) | 4% |
| Postnatal day of transition to full oral feeding, mean±SD | 34±27 |
SD: Standard deviation; IQR: Interquartile range; C/S: Cesarean section; NEC: Necrotizing enterocolitis.
Initial evaluation and OMS initiation occurred on the mean postnatal day 25.8±23 (range: 2–80). Only 8 patients were evaluated as OFS level 2 at initial evaluation; all other patients were evaluated as level 1. The mean time of transition to level 4 was day 16.7±10.1 (range: 6–39), and the transition to full oral feeding occurred on day 19 (IQR: 7–107) at a median corrected age of 35 weeks (range: 31–37).
The comparison of OFS levels on day 5 and day 10 of OMS revealed a significant increase (p<0.001) (Table 2). Similarly, there was a significant improvement in the NNS scores on days 5 and 10 compared to the baseline (Table 2).
Table 2.
Evaluation of patients’ feeding skills
| Feeding skills | Mean±SD | Median (min-max) |
|---|---|---|
| NNS day 0* | 5.9±4.1 | 6 (–4–13) |
| NNS day 5*,£ | 17.1±11.5 | 15 (10–67) |
| NNS day 10£ | 24.5±12.8 | 20 (10–67) |
| OFS day 0† | 1.09±0.3 | 1 (1–2) |
| OFS day 5†,µ | 1.9±0.62 | 2 (1–3) |
| OFS day 10µ | 2.69±0.83 | 3 (1–4) |
: Comparison NNS day 0 and day 5 p<0.01; £: Comparison NNS day 5 and day 10 p<0.01; †: Comparison OFS day 0 and day 5 p<0.01; µ: comparison OFS day 5 and day 10 p<0.01. SD: Standard derivation; min: Minimum; max: Maximum; NNS: Non-nutritive sucking; OFS: Oral feeding skills.
When grouped according to gestational age, 21 patients were born at 24+0/7-29+6/7 weeks and 29 patients at 30+0/7-34+0/7 weeks.
In 18 infants who transitioned to full oral feeding before a corrected age of 34 weeks (mean 32.5±0.7 weeks), OMS was started on the mean postnatal day 12±7.8, and successful oral feeding was achieved on day 17.2±7.8.
The mean day of and adjusted age at discharge were day 56.4±35.3 and 36.9±3.1 weeks, respectively. In our study, the mean time to discharge was 8 weeks. In the subgroup analysis of born <30 weeks, the mean time to discharge was 10 weeks.
Discussion
The results of this study support the benefit of OMS exercises in improving preterm infants’ feeding skills before the transition from gavage feeding to oral nutrition.
The OMS program has been described in detail in many studies.[17,18] Boiron et al.[18] demonstrated with a pacifier-mounted transducer that sucking performance increased after OMS by finger to the cheek, tongue, and palate for 12 min once a day for 14 days, 30 min before feeding. Say et al.[19] showed that stimulation with a pacifier alone resulted in an earlier transition to oral feeding and discharge. In our study, we implemented the OMS program as described by Fucile et al.[17] Unlike Boiron et al.,[18] we included a 3-min period of NNS after motor stimulation. Combined interventions have been found to be more effective in increasing OFS. Zhang et al.[20] showed that the combination of OMS and NNS was more effective than either intervention alone and accelerated the transition to full oral feeding.
Meta-analyses have also shown that the length of hospital stay and parenteral treatment duration are shorter, and the transition to oral feeding is earlier in preterm infants that receive oral stimulation.[21] In our study, the mean time to discharge in infants born <30 weeks of gestation was 10 weeks. With advances in neonatal intensive care, the mean length of hospital stays for preterm infants born at <30 weeks of gestation is 11–12 weeks.[22] In a retrospective study by Majoli et al.,[23] the mean transition time to full oral feeding was 35.1±1.5 weeks for preterm infants born before 32 weeks of gestation; while in our study, this time was 34.4±1.9 weeks in infants born at gestational ages <30 weeks. According to the literature, the average discharge and transition to full oral feeding times were shortened in our study. However, randomized trials are needed to conclude that OMS exercises shorten the time to discharge and transition to full oral feeding, which is one of the limitations of our prospective cohort study.
Prolonged hospital stays and infections adversely affect physical growth and neurological development in premature infants.[24] Li et al.[24] concluded that premature infant oral motor intervention promoted neuromotor coordination by improving neurodevelopment, which was shown with the Infant Neurological International Battery (INFANIB) scale. We did not use a neurological development scale in our study, but it can be an example for future studies.
All neonatal intensive care procedures involve unpleasant stimuli around and inside the mouth (e.g., orogastric catheter insertion, intubation, and aspiration). Oral stimulation is generally the most overlooked practice during the period of growth after stabilization, and most preterm infants experience feeding difficulties later.[17] Properly implemented OMS within the infant’s mouth can activate central pattern generators, which can affect the physiological function of the mouth and pharynx through stimulation of the lips, chin, tongue, soft palate, and throat, and then effects feeding.[25] The turning point for successful OFS in preterm infants is generally accepted as 33–34 weeks of gestation.[7, 26] In the literature, methods and approaches to promote a safe transition to oral feeding in preterm infants have been collected under headings such as cue-based feeding, oral stimulation interventions to support the development of oral motor functions, NNS, and positioning for oral feeding. One of the frequently asked questions for intensive care physicians and nurses is when preterm infants that have completed gestation are clinically stable, and are not receiving mechanical ventilation will transit from gavage feeding to oral nutrition.[15] In units with a large number of incubators, the process of removing a preterm infant’s orogastric tube and transition to oral feeding is generally evaluated by the attending nurse. This assessment is not objective, as it may vary based on experience. The use of objective and standard scales can provide a safer transition to oral feeding for preterm infants. In infants who do not demonstrate progress, early support can be given to shorten discharge time. In NICUs like ours with high numbers of patients, we believe that objective evaluation is important in the decision to start oral feeding and will guide clinicians in making this decision. The OFS staging by Lau and Smith is an objective, easily applicable assessment.[15] In addition, NNS scoring can be easily implemented by experienced staff and can provide guidance to the clinician and the caregiver team. In our study, feeding skill assessments and the OMI were successfully implemented by an LST.
Although LSTs are widely included in NICU settings and post-discharge follow-up in developed countries, to the best of our knowledge, this is the first report from our country of an LST being present in a NICU and implementing an OMS in preterm infants. In the survey conducted by Çiftci et al.,[27] it was determined that nurses had low awareness of the role of LSTs in the NICU. Evaluating the feeding skills of the infants in our NICU with an expert, increased awareness among the research team and the nurses. Assessing the feeding abilities of the neonates in our NICU with an experienced professional has raised awareness among the clinicians and nurses. While conducting this study, we observed that our breastfeeding success rate also increased and our duration to achieve full oral feeding and discharge was shortened. This study serves as a guide for prospective studies to support OMS and objective evaluation of OFS in the NICU.
Conclusion
In preterm infants, OMS during the transition from gavage feeding to oral feeding improves feeding skills. We believe that LSTs, who have graduated in increasing numbers in the past decade in our country, should take an active role in NICUs.
Footnotes
Please cite this article as ”Yavanoglu Atay F, Berber Ciftci H, Sahin O, Guran O, Colak D, Gok NR, et al. Evaluation of Motor Stimulation on Feeding Skills in Preterm. Med Bull Sisli Etfal Hosp 2023;57(2):189–194”.
Disclosures
Ethics Committee Approval
Umraniye Training and Research Hospital Ethics Committee, Approval No: 09, 11/02/2021.
Peer-review
Externally peer-reviewed.
Conflict of Interest
None declared.
Authorship Contributions
Concept – F.Y.A.; Design – F.Y.A., H.B.C., I.M.A.; Supervision – I.M.A.; Materials – O.G., D.C.; Data collection and/or processing – F.Y.A., H.B.C.; Analysis and/or interpretation – F.Y.A., O.S., B.K.E.; Literature search – O.G., D.C., N.R.G.; Writing – F.Y.A.; Critical review – I.M.A.
References
- 1.Bertoncelli N, Cuomo G, Cattani S, Mazzi C, Pugliese M, Coccolini E, et al. Oral feeding competences of healthy preterm infants: a review. Int J Pediatr. 2012;2012:896257. doi: 10.1155/2012/896257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Han C, Shin J, Jeon GW. Development of swallowing function in infants with oral feeding difficulties. Int J Pediatr. 2020:5437376. doi: 10.1155/2020/5437376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lee JH, Chang YS, Yoo HS, Ahn SY, Seo HJ, Choi SH, et al. Swallowing dysfunction in very low birth weight infants with oral feeding desaturation. World J Pediatr. 2011;7:337–43. doi: 10.1007/s12519-011-0281-9. [DOI] [PubMed] [Google Scholar]
- 4.Comrie JD, Helm JM. Common feeding problems in the intensive care nurseries, maturation, organization, evaluation, and management strategies. Semin Speech Lang. 1997;18:239–61. doi: 10.1055/s-2008-1064075. [DOI] [PubMed] [Google Scholar]
- 5.Chen D, Yang Z, Chen C, Wang P. Effect of oral motor intervention on oral feeding in preterm infants: a systemic review and meta-analysis. Am J Speech Lang Pathol. 2021;30:2318–28. doi: 10.1044/2021_AJSLP-20-00322. [DOI] [PubMed] [Google Scholar]
- 6.Parker LA, Desorcy-Scherer K, Magalhães M. Feeding strategies in preterm very low birth-weight infants: state-of-the-science review. Adv Neonatal Care. 2021;21:493–502. doi: 10.1097/ANC.0000000000000849. [DOI] [PubMed] [Google Scholar]
- 7.Braun MA, Palmer MM. A pilot study of oral-motor dysfunction in “at-risk” infants. Phys Occup Ther Pediatr. 1985;5:13–25. [Google Scholar]
- 8.Nye C. Transitioning premature infants from gavage to breast. Neonatal Netw. 2008;27:7–13. doi: 10.1891/0730-0832.27.1.7. [DOI] [PubMed] [Google Scholar]
- 9.Gewolb IH, Vice FL, Schwietzer-Kenney EL, Taciak VL, Bosma JF. Developmental patterns of rhythmic suck and swallow in preterm infants. Dev Med Child Neurol. 2001;43:22–7. doi: 10.1017/s0012162201000044. [DOI] [PubMed] [Google Scholar]
- 10.Viswanathan S, Jadcherla S. Feeding and swallowing difficulties in neonates: developmental physiology and pathophysiology. Clin Perinatol. 2020;47:223–41. doi: 10.1016/j.clp.2020.02.005. [DOI] [PubMed] [Google Scholar]
- 11.Lau C, Sheena H, Shulman RJ, Schanler RJ. Oral feeding in low birth weight infants. J Pediatr. 1997;130:561–9. doi: 10.1016/s0022-3476(97)70240-3. [DOI] [PubMed] [Google Scholar]
- 12.Amaizu N, Shulman R, Schanler R, Lau C. Maturation of oral feeding skills in preterm infants. Acta Paediatr. 2008;97:61–7. doi: 10.1111/j.1651-2227.2007.00548.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jadcherla SR, Wang M, Vijayapal AS, Leuthner SR. Impact of prematurity and co-morbidities on feeding milestones in neonates: a retrospective study. J Perinatol. 2010;30:201–8. doi: 10.1038/jp.2009.149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ostadi M, Jokar F, Armanian AM, Namnabati M, Kazemi Y, Poorjavad M. The effects of swallowing exercise and non-nutritive sucking exercise on oral feeding readiness in preterm infants: a randomized controlled trial. Int J Pediatr Otorhinolaryngol. 2021;142:110602. doi: 10.1016/j.ijporl.2020.110602. [DOI] [PubMed] [Google Scholar]
- 15.Lau C, Smith EO. A novel approach to assess oral feeding skills of preterm infants. Neonatology. 2011;100:64–70. doi: 10.1159/000321987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Neiva FCB, Leone C, Leone CR. Non-nutritive sucking scoring system for preterm newborns. Acta Paediatr. 2008;97:1370–5. doi: 10.1111/j.1651-2227.2008.00943.x. [DOI] [PubMed] [Google Scholar]
- 17.Fucile S, Gisel E, Lau C. Oral stimulation accelerates the transition from tube to oral feeding in preterm infants. J Pediatr. 2002;141:230–6. doi: 10.1067/mpd.2002.125731. [DOI] [PubMed] [Google Scholar]
- 18.Boiron M, Da Nobrega L, Roux S, Henrot A, Saliba E. Effects of oral stimulation and oral support on non-nutritive sucking and feeding performance in preterm infants. Dev Med Child Neurol. 2007;49:439–44. doi: 10.1111/j.1469-8749.2007.00439.x. [DOI] [PubMed] [Google Scholar]
- 19.Say B, Simsek GK, Canpolat FE, Oguz SS. Effects of pacifier use on transition time from gavage to breastfeeding in preterm infants: a randomized controlled trial. Breastfeed Med. 2018;13:433–7. doi: 10.1089/bfm.2018.0031. [DOI] [PubMed] [Google Scholar]
- 20.Zhang Y, Lyu T, Hu X, Shi P, Cao Y, Latour JM. Effect of nonnutritive sucking and oral stimulation on feeding performance in preterm infants: a randomized controlled trial. Pediatr Crit Care Med. 2014;15:608–14. doi: 10.1097/PCC.0000000000000182. [DOI] [PubMed] [Google Scholar]
- 21.Greene Z, O'Donnell CPF, Walshe M. Oral stimulation for promoting oral feeding in preterm infants. Cochrane Database Syst Rev. 2016;20;9:CD009720. doi: 10.1002/14651858.CD009720.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Murki S, Vardhelli V, Deshabhotla S, Sharma D, Pawale D, Kulkarni D, et al. Predictors of length of hospital stay among preterm infants admitted to neonatal intensive care unit: data from a multicentre collaborative network from India (INNC: Indian National Neonatal Collaborative) J Paediatr Child Health. 2020;56:1584–9. doi: 10.1111/jpc.15031. [DOI] [PubMed] [Google Scholar]
- 23.Majoli M, Artuso I, Serveli S, Panella M, Calevo MG, Ramenghi LA. A key developmental step for preterm babies: achievement of full oral feeding. J Matern Fetal Neonatal Med. 2019;34:519–25. doi: 10.1080/14767058.2019.1610733. [DOI] [PubMed] [Google Scholar]
- 24.Li XL, Liu Y, Liu M, Yang CY, Yang QZ. Early premature infant oral motor intervention improved oral feeding and prognosis by promoting neurodevelopment. Am J Perinatol. 2020;37:626–32. doi: 10.1055/s-0039-1685448. [DOI] [PubMed] [Google Scholar]
- 25.Lau C, Alagugurusamy R, Schanler RJ, Smith EO, Shulman RJ. Characterization of the developmental stages of sucking in preterm infants during bottle feeding. Acta Paediatr. 2000;89:846–52. [PubMed] [Google Scholar]
- 26.Mizuno K, Ueda A. The maturation and coordination of sucking, swallowing, and respiration in preterm infants. J Pediatr. 2003;142:36–40. doi: 10.1067/mpd.2003.mpd0312. [DOI] [PubMed] [Google Scholar]
- 27.Berber Çiftci H, Yılmaz A, Çağlayan A, Topbaş S. Determining the awareness level of neonatal intensive care nurses on the role of speech and language therapists. Dil Konuşma ve Yutma Araştırmaları Derg [Article in Turkish] 2021;4:339–61. [Google Scholar]