

Abstract
Objective:
We assess cannabis advertising exposure among adolescents in rural Oklahoma from medical dispensaries.
Method:
Our mixed-methods study identified medical dispensaries within a 15-minute drive time of rural Oklahoma high schools. Study staff completed observational data collection forms and took photographs of each dispensary. Quantitative data from the forms and qualitative coding of photographs were used to describe dispensary characteristics and likely advertising exposure for adolescents.
Results:
Ninety-two dispensaries were identified across 20 rural communities. The majority presented as retail spaces (n = 71). Product (n = 22) and price promotions (n = 27) were common. Coding of dispensary photographs found that product promotions advertised cannabis use modalities, with cannabis flower being the most common (n = 15), followed by edibles (n = 9) and concentrates (n = 9). Among dispensaries with price promotions, discounts (n = 19) and prices under $10 (n = 14) were common.
Conclusions:
Sampled rural medical dispensaries present as retail spaces and are a likely source of adolescent cannabis advertising exposure.
Cannabis Remains the most widely used illegal substance among adolescents in the United States, with more than one third of 12th graders reporting past-year use in 2020 (National Institute on Drug Abuse, 2020). Results from Monitoring the Future surveys have shown an increase in daily cannabis use from 2018 to 2019 among 10th and 12th graders, with a continued increase in 2020 among 12th graders (Johnston et al., 2021). The harmful effects of cannabis use during adolescence and young adulthood are well documented (Volkow et al., 2014). Cannabis use during adolescence is associated with increased cannabis dependence and lower educational attainment (Hall et al., 2020). A recent systematic review of 69 studies among adolescents and young adults found reduced cognitive functioning among frequent users (Scott et al., 2018). Another recent systematic review reports increases in depression and suicide attempts among adolescent users of cannabis during young adulthood (Gobbi et al., 2019).
As jurisdictions in the United States continue to liberalize cannabis laws, the landscape of adolescent cannabis use is changing rapidly, with uncertain consequences for adolescent use. Findings from studies focused on medical legalization have largely found no association between legalization and adolescent use (Hasin et al., 2015; Lynne-Landsman et al., 2013), whereas findings for recreational legalization have been more mixed, with some studies finding evidence of increased use and consequences among adolescents (Cerdá et al., 2017, 2020) and others finding no difference (Bailey et al., 2023; Coley et al., 2021).
One consequence of the new laws is increased adolescent exposure to cannabis dispensaries and related advertising. Increased exposure to cannabis advertising is strongly associated with increased cannabis use and cannabis-related consequences among adolescents (D’Amico et al., 2018). There is evidence that retailers may target communities, with both medical and recreational cannabis dispensaries more common in economically disadvantaged neighborhoods and in neighborhoods with higher proportions of young adults and racial minorities (Berg et al., 2018).
Research to date on adolescent proximity to dispensaries and related advertising has primarily studied urban settings and has produced mixed findings. Firth et al. (2022) found that 11th graders attending schools within 1 mile of a recreational dispensary were more likely to report past-30-day cannabis use, whereas Kerr et al. found no association between the number of recreational dispensaries within varying distances of adolescent home addresses and cannabis use (Kerr et al., 2022). Comparisons of rural and urban adolescent use have also produced mixed results. Comparing adolescent use across California counties, Paschall et al. (2021) found increased past-30-day cannabis use among more rural adolescents, but comparable studies in Oregon counties found no differences among adolescents by rurality (Paschall & Grube, 2020). The current study adds to this growing literature by describing dispensary characteristics and advertising among medical dispensaries in rural areas of northeast Oklahoma, with particular focus on areas that surround public high schools, largely serving American Indian students. Oklahoma legalized cannabis for medical use in 2018 and has since seen a rapid increase in retail locations and licenses to grow cannabis.
Compared with other states, Oklahoma has comparably little regulation with regard to both the cultivation and the purchasing of cannabis, resulting in the highest number of dispensaries of any U.S. state (Hutchinson, 2020; Romero, 2021), many of which are located in rural areas (Cohn et al., 2023). Medicalization refers to the extent to which cannabis is legally treated similarly to other controlled medications. Although Oklahoma prohibits the sale of cannabis for recreational purposes, among states with legalized medical cannabis, prior research on cannabis medicalization has found that Oklahoma's policies are among the least medicalized (Richard et al., 2021). This is especially true for the requirements pertaining to the patient–clinician relationship, where Oklahoma has the fewest requirements of any state (Richard et al., 2021). As a result of few regulations on medical dispensing, it is unclear whether the Oklahoma cannabis environment functions more like a medical or a recreational cannabis state, and what effect that has on cannabis advertising exposures experienced by adolescents.
Specific features of cannabis dispensaries (e.g., visible age restrictions and medical marijuana card requirements for entry, product promotions, and high visibility waving signs) are subject to distinct restrictions by state (Fiala et al., 2018), and their prevalence may reflect evolving regulations in emerging marijuana retail markets. Increased diversity of cannabis products (including modes of ingestion, flavors, and strains’ intended purposes) and related promotions have coincided with market growth (Berg et al., 2018).
Cannabis advertising exposures may be an important component of adolescents’ risk environment in rural communities, and in-depth study of dispensary characteristics is warranted. The current mixed-methods study is part of an ongoing prevention trial in northeast Oklahoma and describes the extent of cannabis advertising exposure among rural adolescents living in communities associated with the parent trial. Specifically, the study examines the number of dispensaries near rural high schools, the external characteristics of these dispensaries, and the content of both product advertisements and price promotions.
Method
Sample
Communities involved in this study were recruited as part of a community-based substance misuse prevention trial taking place in northeastern Oklahoma within or near a tribal reservation (Komro et al., 2022). To involve and serve underrepresented and underresourced small rural communities, inclusion criteria for the parent study included schools located in a town with a population of less than 3,000 people and class sizes between 30 and 100 students. Schools were considered ineligible for the parent study if they were in metropolitan or micropolitan cores or had an established community drug prevention coalition. Based on the study inclusion and exclusion criteria, 24 schools were invited to be a part of the parent trial, of which 20 agreed to participate.
Dispensaries within the catchment area of the parent trial were identified through the Oklahoma Medical Marijuana Authority's (OMMA) database of licensed dispensaries. The OMMA database does not provide detailed address information for dispensaries, listing only name, phone number, city, zip code, and county. To meet our goal of assessing cannabis dispensaries near study high schools, we ascertained the address of each dispensary through a series of steps. First, we performed a reverse address lookup using the Google Maps API accessed through the “ggmap” package in R v4.1.0. Of the 555 cannabis licenses listed in the OMMA database within the parent trial catchment area, we were able to find addresses for the majority (n = 437). Of the remaining 118 licenses, we were able to find addresses for 90 dispensaries through manual web searches. The remaining 28 licenses appear to be a combination of dispensaries that had permanently closed, had not yet opened, or were cannabis growers. We next restricted the geographic criteria to include only dispensaries that were within a 15-minute drive time of a participating school (n = 100). Prior studies have used a variety of distances and centroids to define likely cannabis advertising exposure ranging from as little as less than a mile from an adolescent's school (Fiala et al., 2020) to within 20 miles of an adolescent's home (Kerr et al., 2022). Kerr et al. (2022) particularly note the need for careful consideration of the selected distance metric when dealing with rural adolescents, as the relevant metric may vary when compared with urban adolescents. The choice of using the school as the defining centroid and a 15-minute drive time as the distance metric was based on discussions with community partners from the parent trial. Specifically, the school was chosen as the centroid as one of the few central locations common to all students in these rural areas, and the 15-minute drive time was chosen based on what residents themselves would define as a reasonable boundary for their community. Drive time from each dispensary to each school was calculated by accessing the Google Maps API using the mapdist() function in R's “ggmap” package.
Measures
To capture cannabis-related messaging and advertising as a potential vector for adolescent exposure, an observation form for dispensaries was developed that included questions on characteristics that would be visible from the exterior of the dispensary (Appendix 1). (A supplemental appendix appears as an online-only addendum to this article on the journal's website.) Items include general dispensary characteristics, signage related to cannabis access, and visible advertisements. General dispensary characteristics include whether the dispensary presented as a medical or retail space (medical, retail, other) and whether the interior of the dispensary was visible from the outside (yes/no). Signage relevant to perceived cannabis access includes minimum age to enter (yes/no), whether a medical marijuana card is required to enter (yes/no), whether a medical marijuana card is required to purchase (yes/no), and whether a medical marijuana card could be obtained on site (yes/no). Whether cannabis advertisements were visible was measured by two items (yes/no) assessing whether there were externally visible product advertisements or price promotions. In addition, photographs of each dispensary's exterior were collected for qualitative assessment of the content of visible product advertisements and price promotions.
Data collection protocol
Research staff collected dispensary data by driving to each of the sampled locations during daylight business hours. At each location, staff completed the observation form based on a visual assessment of the dispensary as seen from the parking lot, using a phone-based Qualtrics app. Eight of the sampled dispensaries could not be located or were not in business at the time of data collection, resulting in a final sample of 92 dispensaries.
Analysis
Frequencies, percentages, and corresponding 95% confidence intervals (CIs) were estimated to describe the distribution of dispensary characteristics within a 15-minute drive of rural schools. To account for potential non-independence across dispensaries, standard errors were clustered at the zip code level. These descriptive analyses were carried out using PROC SURVEYFREQ in SAS v9.4 (SAS Institute Inc., Cary, NC).
Content analysis was carried out for photographs of both product advertisement and price promotions to better understand the content of visible cannabis advertisements at study dispensaries. The research team developed a codebook informed by existing literature (Berg et al., 2018; Fiala et al., 2018) and emergent codes from a preliminary review of eligible photos. Codebook development followed the team-based procedures described by MacQueen et al. (1998). First, four co-authors (ML, AW, CB, SLTB) familiarized themselves with the photographs by reviewing the complete collection and memoing initial impressions. Memos were discussed as a group; emergent descriptors and recurring features (e.g., advertised price promotions, product characteristics) were added to a coding tree, to which subcodes were added after iterative review and full group discussion of code specificity and relevance (e.g., distinction between types of products advertised, such as ingestibles vs. flowers, and which products belonged to each category). After codebook revision and a second discussion between coders to check for consistency in code application, coding was performed independently by the same co-authors on the complete set of photographs. Prevalence of codes in the sample was calculated for each label. Final coding decisions were based on the majority response across the four coders. Codes with tied responses (11 of 184 codes) across the four coders were reconciled by meeting with the research team and coming to consensus. Interrater reliability before consensus coding was estimated using Fliess's kappa statistic using the “irr” package in R v4.1.0.
Results
Survey results
Of the 20 schools included in the parent trial, only 1 did not have a dispensary within a 15-minute drive of the school. Of the remaining 19 schools, the number of dispensaries within a 15-minute drive ranged from 1 to 15. On average, there were more than 5 dispensaries within a 15-minute drive (M = 5.25) of each school.
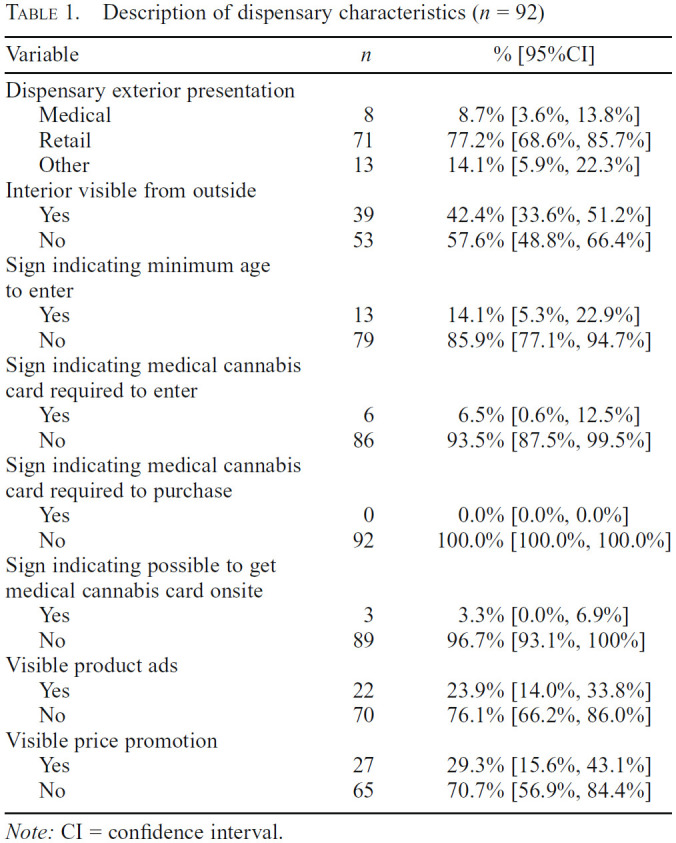
The majority of dispensaries presented as retail spaces (n = 71, 77.2% [68.6%, 85.7%]) (Table 1). Fewer than 10% of dispensaries presented as medical facilities (n = 8, 8.7% [3.6%, 13.8%]). Approximately 14% of dispensaries presented as something other than a retail or medical facility (n = 13, 14.1% [5.9%, 22.3%]), the majority of which appeared to be mechanic garages. Of the dispensaries presenting as retail stores, one was attached to a tobacco outlet and another shared a building with a daiquiri bar. Among dispensaries assessed, 39 had interiors visible from the outside (42.4% [33.6%, 51.2%]).
Table 1.
Description of dispensary characteristics (n = 92)
| Variable | n | % [95%CI] |
|---|---|---|
| Dispensary exterior presentation | ||
| Medical | 8 | 8.7% [3.6%, 13.8%] |
| Retail | 71 | 77.2% [68.6%, 85.7%] |
| Other | 13 | 14.1% [5.9%, 22.3%] |
| Interior visible from outside | ||
| Yes | 39 | 42.4% [33.6%, 51.2%] |
| No | 53 | 57.6% [48.8%, 66.4%] |
| Sign indicating minimum age to enter | ||
| Yes | 13 | 14.1% [5.3%, 22.9%] |
| No | 79 | 85.9% [77.1%, 94.7%] |
| Sign indicating medical cannabis card required to enter | ||
| Yes | 6 | 6.5% [0.6%, 12.5%] |
| No | 86 | 93.5% [87.5%, 99.5%] |
| Sign indicating medical cannabis card required to purchase | ||
| Yes | 0 | 0.0% [0.0%, 0.0%] |
| No | 92 | 100.0% [100.0%, 100.0%] |
| Sign indicating possible to get medical cannabis card onsite | ||
| Yes | 3 | 3.3% [0.0%, 6.9%] |
| No | 89 | 96.7% [93.1%, 100%] |
| Visible product ads | ||
| Yes | 22 | 23.9% [14.0%, 33.8%] |
| No | 70 | 76.1% [66.2%, 86.0%] |
| Visible price promotion | ||
| Yes | 27 | 29.3% [15.6%, 43.1%] |
| No | 65 | 70.7% [56.9%, 84.4%] |
Note: CI = confidence interval.
Only 13 stores presented with signage indicating minimum age requirements to enter (14.1% [5.3%, 22.9%]). Similarly, only 6 (6.5% [0.6%, 12.5%]) had signage indicating that medical cannabis cards were required to enter. Three (3.3% [0.0%, 6.9%]) had signage indicating that a medical cannabis card could be obtained on site. No dispensaries had signage indicating that a medical cannabis card was required to purchase products.
Signage used for advertising was most common, with 22 dispensaries (23.9% [14.0%, 33.8%]) displaying externally visible product advertisements, and 27 displaying externally visible price promotions (29.3% [15.6%, 43.1%]).
Qualitative assessment of price promotions and product ads
Of the 92 stores observed, 29 had either a visible price promotion or product advertisements (Figure 1). Of the 27 dispensaries with a visible price promotion (Table 2), a discounted price was the most common (n = 19, 70.4%); moreover, more than half of dispensaries displayed a product price under $10, indicating the potential for a low-cost purchase. Product characteristics included administration modality, mentions of product quality, and imagery or language indicating therapeutic use/properties. Of the 22 dispensaries mentioning specific products, the majority (n = 15, 68.2%) explicitly displayed advertising for dried flower; although ingestibles (n = 9, 40.9%) and tetrahydrocannabinol (THC) concentrates (n = 9, 40.9%) were also common. Mentions of product quality were less common (n = 4, 18.2%). The majority of product ads also included imagery or language indicating therapeutic benefit in using cannabis (n = 13, 59.1%). The most common therapeutic imagery was a green medical cross. Before consensus coding, inter-rater reliability estimates showed good agreement across coders with estimated κs ranging from .62 to .79.
Figure 1.

Examples of dispensary advertisements
Table 2.
Qualitative assessment of product ads and price promotions

| Code label | Description | Code prevalence, n (%) | Initial interrater reliability, Fleiss's κ |
|---|---|---|---|
| Price promotion (n = 27) | |||
| Price discounts | Mention of discounted price, price reduction, giveaway, BOGO, orother | 19 (70.4%) | .64 |
| Price $10 or below | Mentions of a product at a price of less than $10 | 14(51.9%) | .79 |
| Product characteristics (n = 22) | |||
| Ingestible | Includes gummies, food product, drinks, capsules, tinctures, or othersmokeless product | 9 (40.9%) | .79 |
| Flowers | Includes dried leaves/buds or flowers language orother, “shake,” pre-rolls | 15 (68.2%) | .74 |
| Concentrates | Includes wax, dabs, shatter, or other THC concentrates | 9 (40.9%) | .73 |
| Quality | Mention of top-tier, high-quality product | 4 (18.2%) | .70 |
| Medical or therapeutic | Uses healing, medical, or therapeutic use languageor aesthetics | 13 (59.1%) | .62 |
Notes: BOGO = buy one, get one; THC = tetrahydrocannabinol.
Discussion
After the legalization of medical cannabis in Oklahoma in 2018, more than 500 licenses to sell cannabis were granted within the 20 small rural towns in northeast Oklahoma. Of these licenses, we found nearly 100 active dispensaries within proximity of the 20 rural high schools. The majority of these dispensaries are presented as retail locations and are a likely vector of cannabis advertising, which may influence adolescents’ perceived risk (Firth et al., 2022) and intentions to use cannabis (Hust et al., 2020).
Our finding that relatively few dispensaries presented as medical facilities is consistent with previous research demonstrating the comparatively low levels of medicalization present in Oklahoma's medical cannabis laws. The majority of dispensaries presented as retail spaces, including instances in which dispensaries were paired with retail environments for other recreational substances. Taken together, these findings suggest that medical legalization of cannabis in rural Oklahoma may be functioning more similarly to recreational legalization in other states. The low level of medicalization has concerning implications for adolescent use of cannabis in the region. Prior studies have found little evidence that medical cannabis laws are associated with increased use among adolescents (Lynne-Landsman et al., 2013); however, the consequences of recreational legalization are less clear, as previous evidence shows increases (Cerdá et al., 2017, 2020) or no changes in adolescent cannabis use (Bailey et al., 2023; Coley et al., 2021). Of note, Oklahoma voted down recreational cannabis legalization in March 2023, leaving in place the existing medical cannabis regulatory structure. Despite the relative lack of medical presentation in the current study, many of the surveyed dispensaries involved therapeutic imagery (e.g., green medical cross—commonly associated with medical cannabis, as well as natural remedies/herbal medicine) even when presenting as a retail space.
Visible signage at sampled locations further demonstrates the retail orientation of medical dispensaries in rural Oklahoma. Few dispensaries (7%) indicated that a medical cannabis card was required to enter, no dispensaries had signs indicating that a medical cannabis card was required for purchase, and relatively few had external signs indicating a minimum age to enter (14%). More common were signs advertising specific products (21%) or price promotions (26%). Although prior studies have demonstrated that exposure to cannabis advertising is associated with increased adolescent cannabis use, the presence of price promotions near schools is particularly salient. Research has found that adolescent cannabis use is particularly responsive to changes in price (Pacula & Lundberg, 2014), echoing prior research on tobacco finding that adolescents are more price sensitive than adults (Ding, 2003). The presence of visible price promotions within the vicinity of schools likely heightens the risk environment for adolescents.
Our findings are not without limitations. The measurement of dispensary characteristics is limited to those that are visible from outside the dispensary, and no interior characteristics were assessed. Visible signage on the interior of dispensaries may not correspond to what was observed externally, and these findings may not be representative of advertising and signage exposures for adolescents who enter dispensaries in the area. However, the entire population of locally residing adolescents is regularly exposed to the external presentation of the dispensaries, whereas only a subset of adolescents enter the establishments. Our findings are also limited to those dispensaries that were within a 15-minute drive of high schools involved in the parent trial and likely do not include all dispensaries that adolescents in the study area are likely to be exposed to. Despite these limitations, our results of dispensaries within driving distance of rural high schools capture an important component of cannabis advertising and dispensary exposure that is common to the majority of adolescents within the study communities.
Given the continued trend toward liberalization of cannabis laws in the United States, adolescents are likely to continue to see increased dispensary presence in their physical environments. Our results show that dispensaries are a likely source of advertising exposure for adolescents in a rural environment, despite being in a state where recreational use of cannabis is illegal. Future research in states with medical cannabis should investigate the nuances of state laws to more clearly understand not just whether a state classifies itself as allowing recreational cannabis use, but how those laws operate in practice and the effect such policies have in modifying the adolescent risk environment, especially among underserved populations who face disproportionate risk.
Footnotes
This research was supported by the National Institutes of Health (NIH) through the NIH HEAL Initiative under award number UH3DA050234. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or its NIH HEAL Initiative.
References
- Bailey J. A., Tiberio S. S., Kerr D. C. R., Epstein M., Henry K. L., Capaldi D. M. Effects of cannabis legalization on adolescent cannabis use across 3 studies. American Journal of Preventive Medicine. 2023;64:361–367. doi: 10.1016/j.amepre.2022.09.019. doi:10.1016/j.amepre.2022.09.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berg C. J., Henriksen L., Cavazos-Rehg P. A., Haardoerfer R., Freisthler B. The emerging marijuana retail environment: Key lessons learned from tobacco and alcohol retail research. Addictive Behaviors. 2018;81:26–31. doi: 10.1016/j.addbeh.2018.01.040. doi:10.1016/j.addbeh.2018.01.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cerdá M., Mauro C., Hamilton A., Levy N. S., Santaella-Tenorio J., Hasin D., Martins S. S. Association between recreational marijuana legalization in the United States and changes in marijuana use and cannabis use disorder from 2008 to 2016. JAMA Psychiatry. 2020;77:165–171. doi: 10.1001/jamapsychiatry.2019.3254. doi:10.1001/jamapsychiatry.2019.3254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohn A., Sedani A., Niznik T., Alexander A., Lowery B., McQuoid J., Campbell J. Population and neighborhood correlates of cannabis dispensary locations in Oklahoma. Cannabis. 2023;6:99–113. doi: 10.26828/cannabis/2023.01.008. doi:10.26828/cannabis/2023.01.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coley R. L., Kruzik C., Ghiani M., Carey N., Hawkins S. S., Baum C. F. Recreational marijuana legalization and adolescent use of marijuana, tobacco, and alcohol. Journal of Adolescent Health. 2021;69:41–49. doi: 10.1016/j.jadohealth.2020.10.019. [DOI] [PubMed] [Google Scholar]
- D’Amico E. J., Rodriguez A., Tucker J. S., Pedersen E. R., Shih R. A. Planting the seed for marijuana use: Changes in exposure to medical marijuana advertising and subsequent adolescent marijuana use, cognitions, and consequences over seven years. Drug and Alcohol Dependence. 2018;188:385–391. doi: 10.1016/j.drugalcdep.2018.03.031. doi:10.1016/j.drugalcdep.2018.03.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ding A. Youth are more sensitive to price changes in cigarettes than adults. Yale Journal of Biology and Medicine. 2003;76:115–124. [PMC free article] [PubMed] [Google Scholar]
- Fiala S. C., Dilley J. A., Everson E. M., Firth C. L., Maher J. E. Youth exposure to marijuana advertising in Oregon's legal retail marijuana market. Preventing Chronic Disease. 2020;17:190206. doi: 10.5888/pcd17.190206. doi:10.5888/pcd17.190206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fiala S. C., Dilley J. A., Firth C. L., Maher J. E. Exposure to marijuana marketing after legalization of retail sales: Oregonians’ experiences, 2015-2016. American Journal of Public Health. 2018;108:120–127. doi: 10.2105/AJPH.2017.304136. doi:10.2105/AJPH.2017.304136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Firth C. L., Carlini B., Dilley J., Guttmannova K., Hajat A. Retail cannabis environment and adolescent use: The role of advertising and retailers near home and school. Health & Place. 2022;75:102795. doi: 10.1016/j.healthplace.2022.102795. doi:10.1016/j.healthplace.2022.102795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gobbi G., Atkin T., Zytynski T., Wang S., Askari S., Boruff J., Mayo N. Association of cannabis use in adolescence and risk of depression, anxiety, and suicidality in young adulthood: A systematic review and meta-analysis. JAMA Psychiatry. 2019;76:426–434. doi: 10.1001/jamapsychiatry.2018.4500. doi:10.1001/jamapsychiatry.2018.4500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall W., Leung J., Lynskey M. The effects of cannabis use on the development of adolescents and young adults. Annual Review of Developmental Psychology. 2020;2:461–483. doi:10.1146/annurev-devpsych-040320-084904. [Google Scholar]
- Hasin D. S., Wall M., Keyes K. M., Cerdá M., Schulenberg J., O’Malley P. M., Feng T. Medical marijuana laws and adolescent marijuana use in the USA from 1991 to 2014: Results from annual, repeated cross-sectional surveys. The Lancet Psychiatry. 2015;2:601–608. doi: 10.1016/S2215-0366(15)00217-5. doi:10.1016/S2215-0366(15)00217-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hust S. J. T., Willoughby J. F., Li J., Couto L. Youth's proximity to marijuana retailers and advertisements: Factors associated with Washington State adolescents’ intentions to use marijuana. Journal of Health Communication. 2020;25:594–603. doi: 10.1080/10810730.2020.1825568. doi:10.1080/10810730.2020.1825568. [DOI] [PubMed] [Google Scholar]
- Hutchinson D. KGOU; 2020. Feb 12, Oklahoma leads nation in number of cannabis dispensaries. Retrieved from https://www.kgou.org/business-and-economy/2020-02-12/oklahoma-leads-nation-in-number-of-cannabis-dispensaries. [Google Scholar]
- Johnston L. D., Miech R. A., O’Malley P. M., Bachman J. G., Schulenberg J. E., Patrick M. E. Ann Arbor, MI: Institute for Social Research, University of Michigan; 2021. Monitoring the Future National Survey Results on Drug Use, 1975–2020: Overview, key findings on adolescent drug use. [Google Scholar]
- Kerr D. C. R., Owen L. D., Tiberio S. S., Dilley J. A. Prevention Science. Advance online publication; 2022. Recreational cannabis legalization and proximity to cannabis retailers as risk factors for adolescents’ cannabis use. doi:10.1007/s11121-022-01475-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Komro K. A., Kominsky T. K., Skinner J. R., Livingston M. D., Livingston B. J., Avance K., Wagenaar A. C. Study protocol for a cluster randomized trial of a school, family, and community intervention for preventing drug misuse among older adolescents in the Cherokee Nation. Trials. 2022;23 doi: 10.1186/s13063-022-06096-0. Article no. 175. doi:10.1186/s13063-022-06096-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lynne-Landsman S. D., Livingston M. D., Wagenaar A. C. Effects of state medical marijuana laws on adolescent marijuana use. American Journal of Public Health. 2013;103:1500–1506. doi: 10.2105/AJPH.2012.301117. doi:10.2105/AJPH.2012.301117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacQueen K. M., McLellan E., Kay K., Milstein B. Codebook development for team-based qualitative analysis. CAM Journal. 1998;10:31–36. doi:10.1177/1525822X980100020301. [Google Scholar]
- National Institute on Drug Abuse. Monitoring the Future 2020 Survey Results. 2020. Dec 15, Retrieved from https://www.drugabuse.gov/drug-topics/related-topics/trends-statistics/infographics/monitoring-future-2020-survey-results.
- Pacula R. L., Lundberg R. Why changes in price matter when thinking about marijuana policy: A review of the literature on the elasticity of demand. Public Health Reviews. 2014;35:1–18. doi: 10.1007/BF03391701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paschall M. J., García-Ramírez G., Grube J. W. Recreational marijuana legalization and use among California adolescents: Findings from a statewide survey. Journal of Studies on Alcohol and Drugs. 2021;82:103–111. doi: 10.15288/jsad.2021.82.103. doi:10.15288/jsad.2021.82.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paschall M. J., Grube J. W.2020Recreational marijuana availability in oregon and use among adolescents American Journal of Preventive Medicine 58e63–e69doi:10.1016/j.amepre.2019.09.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richard E. L., Althouse A. D., Arnsten J. H., Bulls H. W., Kansagara D., Kerbag M. N., Starrels J. L. How medical are states’ medical cannabis policies?: Proposing a standardized scale. International Journal on Drug Policy. 2021;94:103202. doi: 10.1016/j.drugpo.2021.103202. doi:10.1016/j.drugpo.2021.103202. [DOI] [PubMed] [Google Scholar]
- Romero S.How Oklahoma became a marijuana boom state. The New York Times. 2021. Dec 29, Retrieved from https://www.nytimes.com/2021/12/29/us/oklahoma-marijuana-boom.html.
- Scott J. C., Slomiak S. T., Jones J. D., Rosen A. F. G., Moore T. M., Gur R. C. Association of cannabis with cognitive functioning in adolescents and young adults: A systematic review and meta-analysis. JAMA Psychiatry. 2018;75:585–595. doi: 10.1001/jamapsychiatry.2018.0335. doi:10.1001/jamapsychiatry.2018.0335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Volkow N. D., Baler R. D., Compton W. M., Weiss S. R. B. Adverse health effects of marijuana use. The New England Journal of Medicine. 2014;370:2219–2227. doi: 10.1056/NEJMra1402309. doi:10.1056/NEJMra1402309. [DOI] [PMC free article] [PubMed] [Google Scholar]