

Abstract
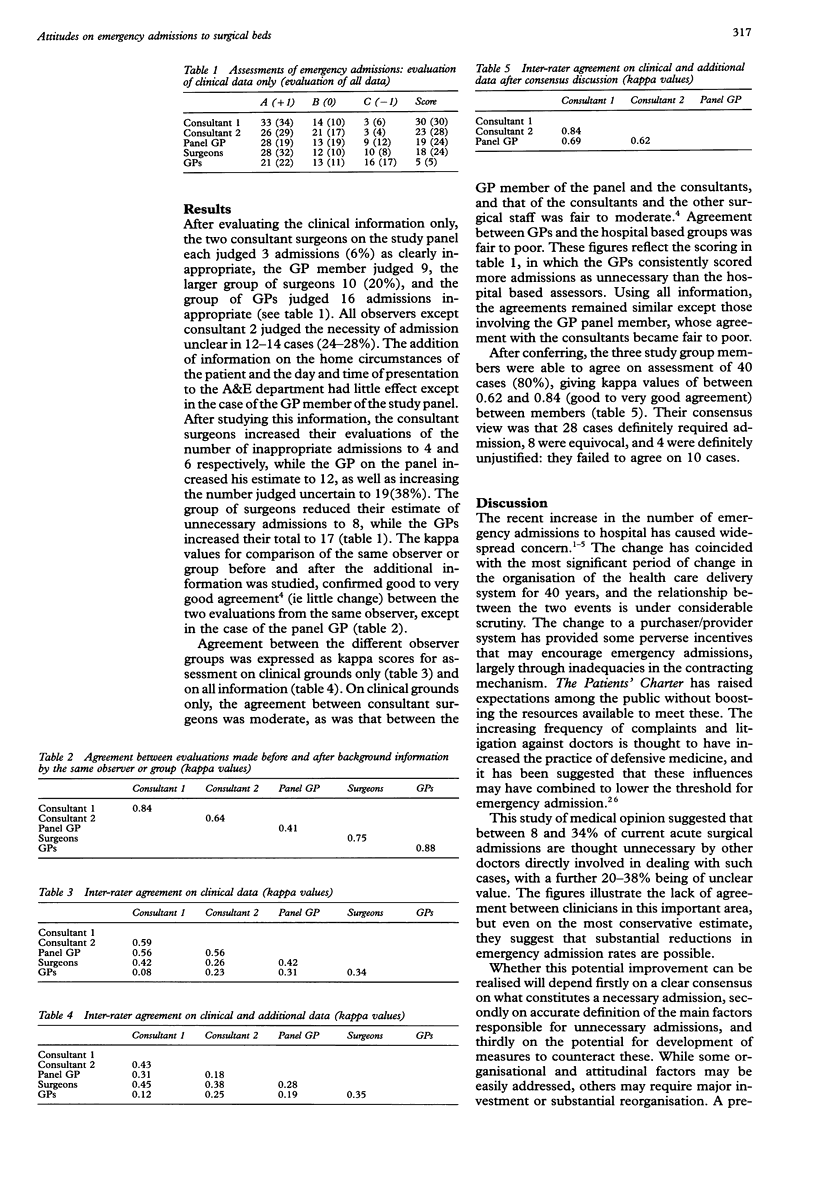
OBJECTIVES: To determine (a) whether doctors involved in the process of emergency surgical admission could agree about which patients should be admitted, (b) whether there were consistent differences between doctors in different specialty groups, and (c) whether these opinions were greatly influenced by non-clinical factors. DESIGN: Independent assessment of summarised case histories by three "expert" clinicians (two consultant surgeons and one general practitioner (GP)), by a group of 10 GPs, and by a group of 10 junior and senior surgeons. Experts, but not other observers, scored admissions both independently and as a consensus group. Observers indicated for each patient whether they would admit, would not admit, or were unsure. SETTING: An urban general hospital with teaching status. SUBJECTS: Fifty consecutive patients admitted to the general surgical unit as emergencies during 1995. MAIN OUTCOME MEASURES: Proportion of admissions considered unnecessary or uncertain: agreement between observers on these proportions: effect of social and procedural factors on the admission decision. RESULTS: Between 8 and 34% of admissions were considered unnecessary and 20-38% of unclear necessity. Agreement between the groups of clinicians was not good. GPs and consultant surgeons showed the poorest agreement (kappa = 0.08 to 0.25, 4 comparisons), and the GPs scored a higher percentage of admissions as unnecessary (34 v 8-12%). After discussion, the consensus group achieved good to very good agreement (kappa 0.61-0.84). CONCLUSIONS: Different groups of doctors vary widely in their views about the need for emergency surgical admission. Good agreement can be reached by consensus discussion. GPs are less likely than surgeons to consider emergency surgical admission necessary.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Brennan P., Silman A. Statistical methods for assessing observer variability in clinical measures. BMJ. 1992 Jun 6;304(6840):1491–1494. doi: 10.1136/bmj.304.6840.1491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chadwick D. R. Rising emergency admissions. GPs must take some responsibility. BMJ. 1995 Apr 1;310(6983):867–867. doi: 10.1136/bmj.310.6983.867b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chappell A. G. Rising emergency admissions. Patients have rising expectations. BMJ. 1995 Apr 1;310(6983):867–868. doi: 10.1136/bmj.310.6983.867c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coast J., Inglis A., Frankel S. Alternatives to hospital care: what are they and who should decide? BMJ. 1996 Jan 20;312(7024):162–166. doi: 10.1136/bmj.312.7024.162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coast J., Inglis A., Morgan K., Gray S., Kammerling M., Frankel S. The hospital admissions study in England: are there alternatives to emergency hospital admission? J Epidemiol Community Health. 1995 Apr;49(2):194–199. doi: 10.1136/jech.49.2.194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gaskell D. J., Lewis P. A., Crosby D. L., Roberts C. J., Fenn N., Roberts S. M. Improving the primary management of emergency surgical admissions: a controlled trial. Ann R Coll Surg Engl. 1995 Sep;77(5 Suppl):239–241. [PubMed] [Google Scholar]
- Hobbs R. Rising emergency admissions. BMJ. 1995 Jan 28;310(6974):207–208. doi: 10.1136/bmj.310.6974.207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tsang P., Severs M. P. A study of appropriateness of acute geriatric admissions and an assessment of the Appropriateness Evaluation Protocol. J R Coll Physicians Lond. 1995 Jul-Aug;29(4):311–314. [PMC free article] [PubMed] [Google Scholar]
- Wardrope J., Kidner N. L., Edhouse J. Rising emergency admissions. Bed crises are occurring almost daily in some hospitals. BMJ. 1995 Apr 1;310(6983):868–868. doi: 10.1136/bmj.310.6983.868. [DOI] [PMC free article] [PubMed] [Google Scholar]