

Abstract
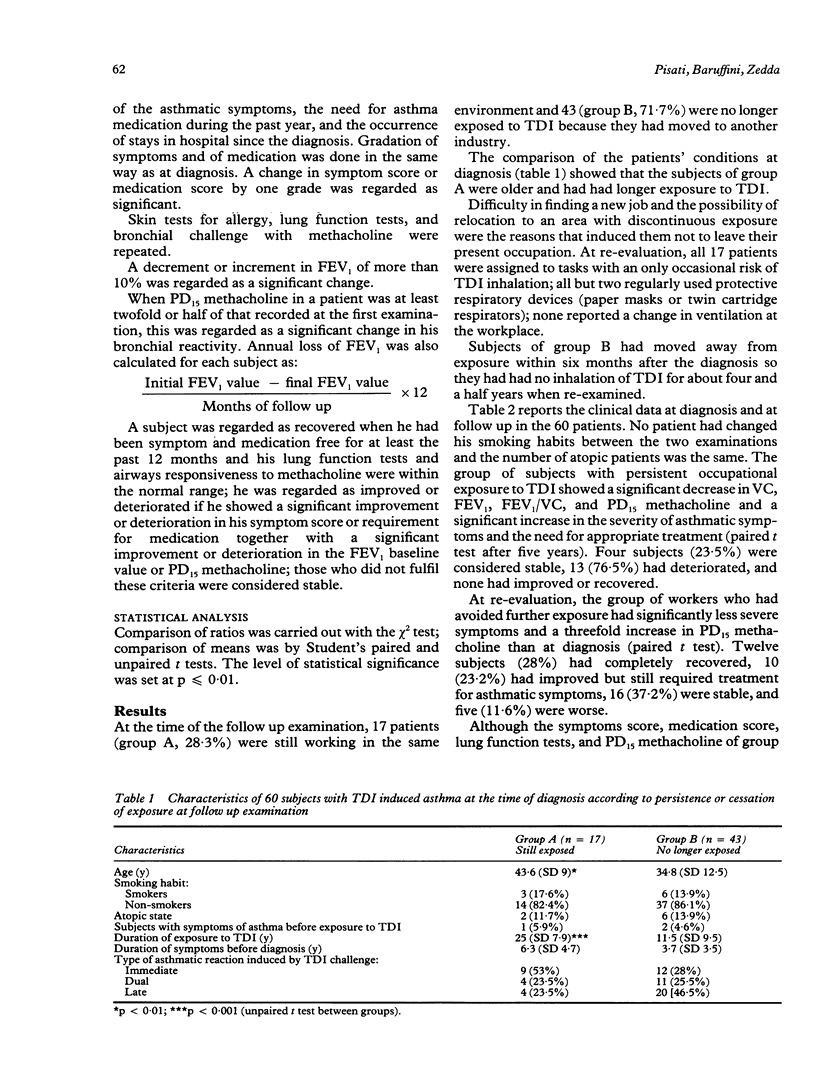
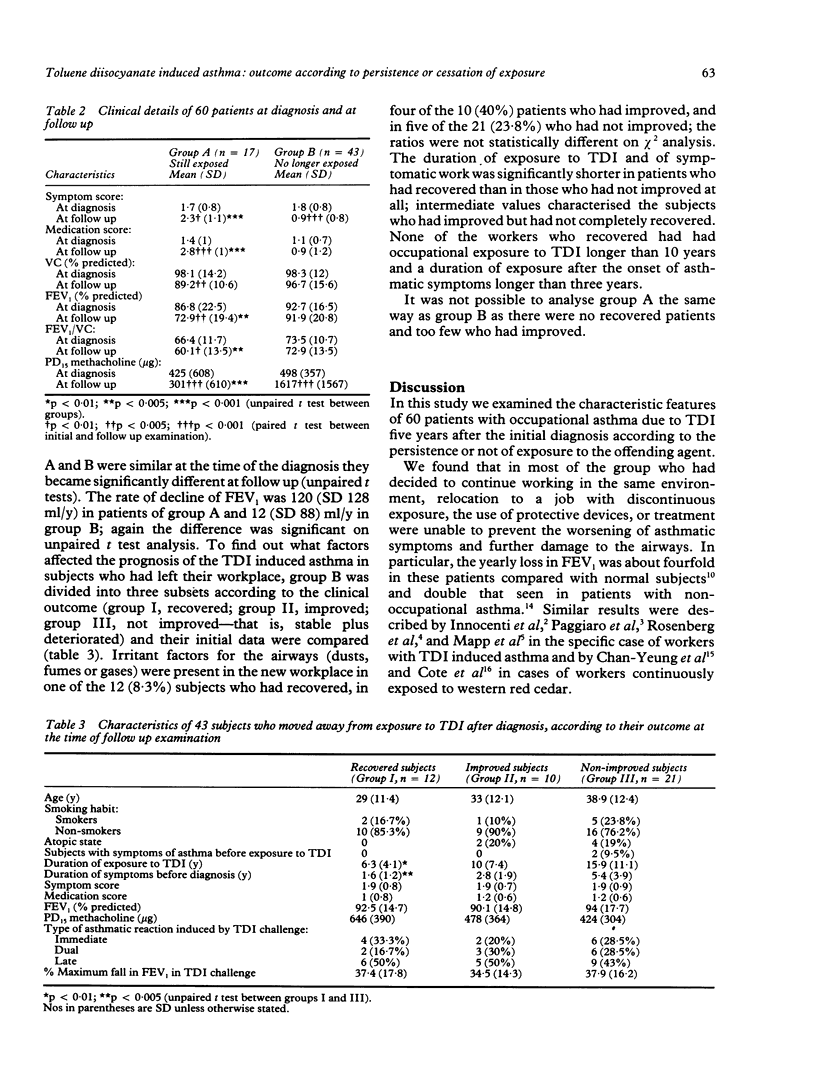
Sixty patients with occupational asthma due to exposure to toluene diisocyanate (TDI) were re-evaluated, five years after the initial diagnosis had been confirmed by a specific bronchial provocation challenge. During both examinations the severity of asthmatic symptoms and the need for antiasthma treatment were graded and lung function tests, measurement of airway responsiveness to methacholine (PD15), and skin tests with common inhalant allergens were carried out. The evolution of the disease was established on the basis of the increase or decrease in asthmatic symptoms, requirements for medication, and FEV1 and PD15 methacholine between the two examinations. At follow up 17 patients (group A, 28.3%) had carried on working in the same environment after relocation to jobs with only occasional exposure to TDI; 15 of them used protective respiratory devices. The remaining 43 (group B, 71.7%) avoided further inhalation of TDI by moving to another sector. Group A showed a significant decrease in FEV1 and PD15 methacholine and significant increases in the severity of symptom score and requirement for medication; 13 subjects (76.5%) were worse, four (23.5%) were stable, and no one had recovered or improved. Group B showed significantly less severe symptoms and a threefold increase in PD15 methacholine; 12 subjects (28.2%) totally recovered, 10 (23.2%) improved, 16 (37.2%) were stable, and five (11.6%) were worse. In group B the duration of exposure to TDI and of symptoms before the initial diagnosis delineated the patients who recovered from those who did not improve; intermediate values in these features characterised the subjects who improved but did not recover. It is inferred that complete removal from exposure is the only effective way of preventing deterioration in patients with occupational asthma due to TDI. Early diagnosis and early removal from exposure after the onset of asthma are important factors for a favourable outcome of the disease.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Adams W. G. Long-term effects on the health of men engaged in the manufacture of tolylene di-isocyanate. Br J Ind Med. 1975 Feb;32(1):72–78. doi: 10.1136/oem.32.1.72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chan-Yeung M., Lam S., Koener S. Clinical features and natural history of occupational asthma due to western red cedar (Thuja plicata). Am J Med. 1982 Mar;72(3):411–415. doi: 10.1016/0002-9343(82)90497-1. [DOI] [PubMed] [Google Scholar]
- Cote J., Kennedy S., Chan-Yeung M. Outcome of patients with cedar asthma with continuous exposure. Am Rev Respir Dis. 1990 Feb;141(2):373–376. doi: 10.1164/ajrccm/141.2.373. [DOI] [PubMed] [Google Scholar]
- Hudson P., Cartier A., Pineau L., Lafrance M., St-Aubin J. J., Dubois J. Y., Malo J. L. Follow-up of occupational asthma caused by crab and various agents. J Allergy Clin Immunol. 1985 Nov;76(5):682–688. doi: 10.1016/0091-6749(85)90671-2. [DOI] [PubMed] [Google Scholar]
- Innocenti A., Franzinelli E., Sartorelli E. Studio longitudinale in lavoratori affetti da asma da resine poliuretaniche. Med Lav. 1981 May-Jun;72(3):231–237. [PubMed] [Google Scholar]
- Malo J. L., Cartier A., Ghezzo H., Lafrance M., McCants M., Lehrer S. B. Patterns of improvement in spirometry, bronchial hyperresponsiveness, and specific IgE antibody levels after cessation of exposure in occupational asthma caused by snow-crab processing. Am Rev Respir Dis. 1988 Oct;138(4):807–812. doi: 10.1164/ajrccm/138.4.807. [DOI] [PubMed] [Google Scholar]
- Mapp C. E., Corona P. C., De Marzo N., Fabbri L. Persistent asthma due to isocyanates. A follow-up study of subjects with occupational asthma due to toluene diisocyanate (TDI). Am Rev Respir Dis. 1988 Jun;137(6):1326–1329. doi: 10.1164/ajrccm/137.6.1326. [DOI] [PubMed] [Google Scholar]
- Moller D. R., Brooks S. M., McKay R. T., Cassedy K., Kopp S., Bernstein I. L. Chronic asthma due to toluene diisocyanate. Chest. 1986 Oct;90(4):494–499. doi: 10.1378/chest.90.4.494. [DOI] [PubMed] [Google Scholar]
- Paggiaro P. L., Loi A. M., Rossi O., Ferrante B., Pardi F., Roselli M. G., Baschieri L. Follow-up study of patients with respiratory disease due to toluene diisocyanate (TDI). Clin Allergy. 1984 Sep;14(5):463–469. doi: 10.1111/j.1365-2222.1984.tb02230.x. [DOI] [PubMed] [Google Scholar]
- Peat J. K., Woolcock A. J., Cullen K. Rate of decline of lung function in subjects with asthma. Eur J Respir Dis. 1987 Mar;70(3):171–179. [PubMed] [Google Scholar]
- Pepys J., Hutchcroft B. J. Bronchial provocation tests in etiologic diagnosis and analysis of asthma. Am Rev Respir Dis. 1975 Dec;112(6):829–859. doi: 10.1164/arrd.1975.112.6.829. [DOI] [PubMed] [Google Scholar]
- Rosenberg N., Garnier R., Rousselin X., Mertz R., Gervais P. Clinical and socio-professional fate of isocyanate-induced asthma. Clin Allergy. 1987 Jan;17(1):55–61. doi: 10.1111/j.1365-2222.1987.tb02319.x. [DOI] [PubMed] [Google Scholar]