

Abstract
Nutrition plays an important role for health, in particular of children and adolescents. In addition to the baseline German Health Interview and Examination Survey for Children and Adolescents (KiGGS, 2003-2006), the nutrition survey EsKiMo (Eating study as a KiGGS Module) assessed the dietary habits of children and adolescents aged 6 to 17 in detail. In KiGGS Wave 2 (2014-2017) the corresponding module is EsKiMo II. Between June 2015 and September 2017, specially trained nutritionists will visit EsKiMo II participants at their homes. The parents of 6-to 11-year-olds are instructed on how to complete food records on four randomly chosen days - three consecutive days, followed later by an additional day. Participants aged 12 to 17 are interviewed personally on their food intake during the past four weeks with the dietary interview programme DISHES. Further information, for example, regarding dietary supplements is also recorded. EsKiMo II will provide an up-to-date and representative overview of the current nutrition status of 6-to 17-year-olds living in Germany, and it allows analysing changes in dietary behaviour over time. EsKiMo II can identify shortcomings in the nutrition of children and adolescents and thus may contribute with important information to nutrition and health policy.
Keywords: NUTRITION, FOOD CONSUMPTION, NUTRIENT SUPPLY, HEALTH MONITORING, KIGGS
1. Background and objective
Eating and drinking are essential for our life, and individual dietary habits have great influence on our physical and mental health. An adequate diet is particularly important for the growth and health development of children and adolescents. Compared to adults, children require a higher amount of nutrients per kilogramme of body weight. Due to their lower body weight and an immune system which is still developing over the first years of their life, children constitute a particularly vulnerable group for the health implications of food contaminated with pathogens or other harmful substances. Additionally, dietary habits generally develop during childhood and have implications for people’s dietary behaviour at adult age [1]. Monitoring potential health risks related to food intake and improving dietary habits are important tasks of nutrition and health policy. Keeping track of population dietary behaviour on a regular basis is therefore necessary.
In the context of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS) of the Robert Koch Institute (RKI), a food frequency questionnaire is used for participants aged 3 and older to obtain both the frequency and the respective portion size of certain food groups that were consumed during the past four weeks [2, 3]. While this information does provide an impression of respondents’ regular dietary behaviour, it cannot, however, answer more complex questions, for example to identify deficits in respondents’ nutrient supply.
EsKiMo II.
Second Wave of the Eating study as a KiGGS Module, 2015-2017
Acronym: EsKiMo - Eating study as a KiGGS Module
Implementation: Robert Koch Institute
Aim: Providing an up-to-date representative overview of the dietary habits of children and adolescents aged 6 to 17 in Germany.
Study design: Cross-sectional study based on a modified diet history interview and food records
Population: Children and adolescents with permanent residence in Germany
Sampling: EsKiMo II participants are randomly selected from the cross-sectional sample of KiGGS Wave 2 (registry office sample). Being invited to EsKiMo II requires participation in KiGGS Wave 2.
Age range: 6 to 17 years
Sample size: at least 2,400 participants
Survey period: June 2015 - September 2017
More information in German is available at www.rki.de/eskimo
This led, in the context of the RKI’s KiGGS baseline study (2003-2006), to the implementation of EsKiMo (Eating study as a KiGGS Module, referred to as EsKiMo I in the following), the first representative survey of the dietary behaviour of children and adolescents aged 6 to 17 in Germany [4, 5]. Funding was provided by the Federal Ministry for Consumer Protection, Food and Agriculture, which today is the Federal Ministry of Food and Agriculture (BMEL). Given that data collection for EsKiMo I took place ten years ago, KiGGS Wave 2 (2014-2017) will include the EsKiMo II module, funded by the BMEL. The Federal Institute for Risk Assessment (BfR) will conduct in addition to EsKiMo II a further module on nutrition (KiESEL – the children’s nutrition survey module in KiGGS Wave 2), assessing the dietary habits of children below six years [6].
As a module of the KiGGS study, EsKiMo II will provide the basis for differentiated analyses for example of the relation between dietary habits, socio-demographic criteria (such as size of town, social status, and education), behavioural factors (such as levels of physical activity, use of media or smoking), as well as a diverse set of health parameters (biochemical and physiological measurements) and diseases. Some of the planned analyses will require data collection on food intake to take place as soon as possible after data collection for KiGGS Wave 2, since certain parameters (such as blood values) may be subject to change over time. Data for EsKiMo II will be collected between June 2015 and September 2017. EsKiMo II aims to provide an up-to-date overview of the dietary habits of children and adolescents aged 6 to 17 living in Germany.
2. Methodology
2.1 Study design and sampling
Participants of EsKiMo II are sampled from the cross-sectional study population of KiGGS Wave 2 (aged 6 to 17), mostly those who took also part in the physical examination of KiGGS Wave 2, and partly those who only answered the KiGGS questionnaire. The target population and sampling for KiGGS Wave 2 is described in detail in the article New data for action. Data collection for KiGGS Wave 2 has been completed in this issue of the Journal of Health Monitoring. Participants receive a written invitation to EsKiMo II three to six months after taking part in KiGGS Wave 2 and about six weeks prior to the scheduled date of the nutrition survey in their locality (routes). Participation and appointments for EsKiMo II are arranged by telephone (Figure 1). During a route, participants are visited at their homes in parallel at several KiGGS Wave 2 sample points (Figure 2) by specially trained nutritionists. Like in KiGGS Wave 2, the order of routes ensures a broad distribution of the regions visited across Germany within seasons, to account for seasonal differences. The survey aims for a net sample of at least 2,400 children and adolescents.
Figure 1.
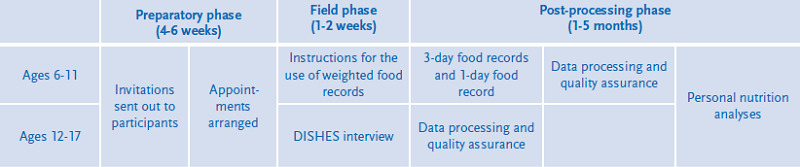
Organisational process of EsKiMo II field phases
Own figure
Figure 2.
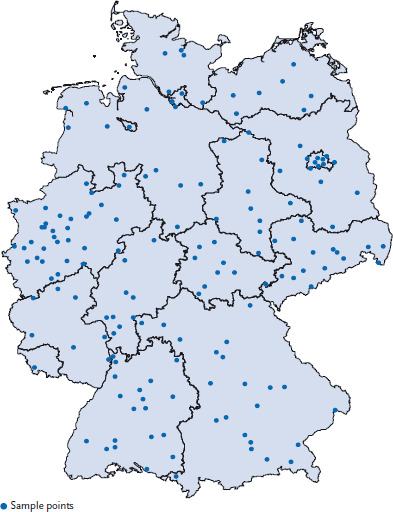
Sample points of EsKiMo II
Source: RKI
EsKiMo II received an approval from the ethics committee of the Hannover School of Medicine (number 2275-2015). Germany’s Federal Commissioner for Data Protection and Freedom of Information has been informed about and has also approved the survey. Parents and guardians of all participants as well as adolescents aged 14 and older have provided their informed consent to participate in the survey.
2.2 Assessment methods and testing instruments
As in EsKiMo I, different assessment instruments are used for the specific age groups. For children aged 6 to 11, the parents (or guardians) are asked to use weighted food records to record children’s food intake on three consecutive days, followed by an additional 1-day weighted food record at a later point in time. A randomisation process is used to determine the recording days. The minimum timespan between the 3-day-weighted food record and the 1-day-weighted food record should be two weeks, the maximum timespan three months. The parents (or guardians) are instructed on how to record their children’s food intake. Entries are to include an exact description of the foods consumed as well as information on the brand, product name, fat content (for example of cheese), the actual amount of food on the plate, and leftovers (Figure 3). Details on the time of consumption, place of food preparation/consumption, the state when purchased (for example raw), on how the meal was prepared, and what type of packaging it came in (for example plastic) are to be recorded as well. In addition, participants are asked to provide the recipes of self-prepared meals. Participants are given kitchen scales and instructions on how to use them, as well as a picture book showing portion sizes. A simplified version of the food record that children can fill out themselves is provided for situations where participants cannot weigh meals (for example in school canteens and/or restaurants). The simplified version of the food record requires participants to describe meals as precisely as possible. Parents are asked to discuss the entries with their children at home. The amounts consumed are estimated based on the picture book or household measures. The picture book aims to improve the accuracy of participants’ estimates. It was adapted for EsKiMo II and contains pictures provided by the International Agency for Research on Cancer (IARC) and the Pilot study for the Assessment of Nutrient intake and food Consumption Among Kids in Europe (PANCAKE) [7, 8]. Parents (or guardians) are also asked to weigh and record in advance the food and beverages that children take with them to school, as well as any leftovers. For children who have school meals, parents (or guardians) are asked to provide the menu where possible.
Figure 3.
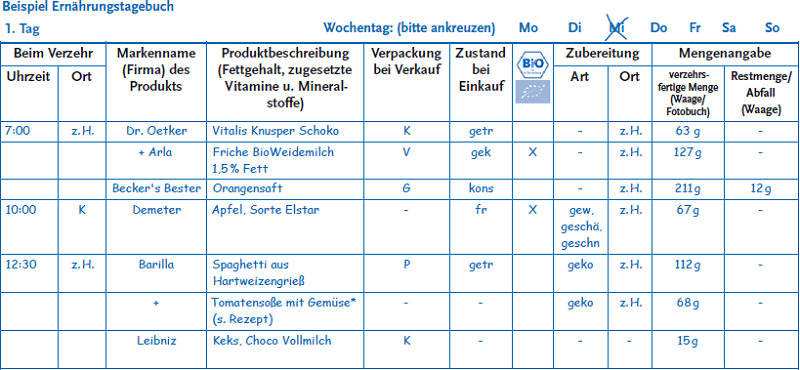
Sample food record page (in German)
Source: RKI
Telephone support is available to respond to any possible question of participants. Participants return the completed food record to the RKI via a post-paid envelope. On the scheduled date they receive the 1-day-weighted food record, which is also to be sent back after completion. After completion, survey participants receive a personal nutrition analysis and a voucher. The information provided in the food records is processed with version 5.3 of the EAT software (Paderborn University) using the codes of the German Nutrient Database version 3.02 [9]. If necessary, discrepancies or missing information is clarified by telephone.
KiGGS Wave 2.
Second follow-up to the German Health Interview and Examination Survey for Children and Adolescents
Data owner: Robert Koch Institute
Aim: Providing reliable information on health status, health-related behaviour, living conditions, protective and risk factors, and health care among children, adolescents and young adults living in Germany, with the possibility of trend and longitudinal analyses.
Study design: Combined cross-sectional and cohort study conducted as an examination and interview survey
KiGGS cross-sectional study
Population: Children and adolescents with permanent residence in Germany
Sampling: Samples from official residency registries - randomly selected children and adolescents from the 167 cities and municipalities covered by the KiGGS baseline study
Age range: 0-17 years
Sample size: Approximately 15,000 participants
KiGGS cohort study
Sampling: Re-invitation of everyone who took part in the KiGGS baseline study (2003-2006; aged between 0 and 17 at that time) and who was willing to participate in a follow-up
Age range: 10-29 years
Sample size: Approximately 10,000 follow-up participants
Survey period: September 2014-August 2017
Modules: BELLA, EsKiMo, GerES, KiESEL, MoMo
More information is available at www.kiggs-studie.de/english
With participants aged 12 to 17 a personal dietary interview is conducted during the home visit using the DISHES software (Dietary Interview Software for Health Examination Studies). Developed at the RKI, DISHES is a tool to record regular dietary habits based on a modified diet history method. This method documents the frequency and portion size of meals during the past four weeks (Figure 4), the collected data are internally coded according to the German Nutrient Database version 3.02 [9]. Portion sizes are estimated using tableware and the picture book mentioned above. The instrument has been validated for adults [10]. Provided respondents give their consent, DISHES interviews are recorded digitally to allow staff to clarify cases where the data provided by participants does not seem plausible. In exchange, adolescents are remunerated and receive a personal nutrition analysis.
Figure 4.
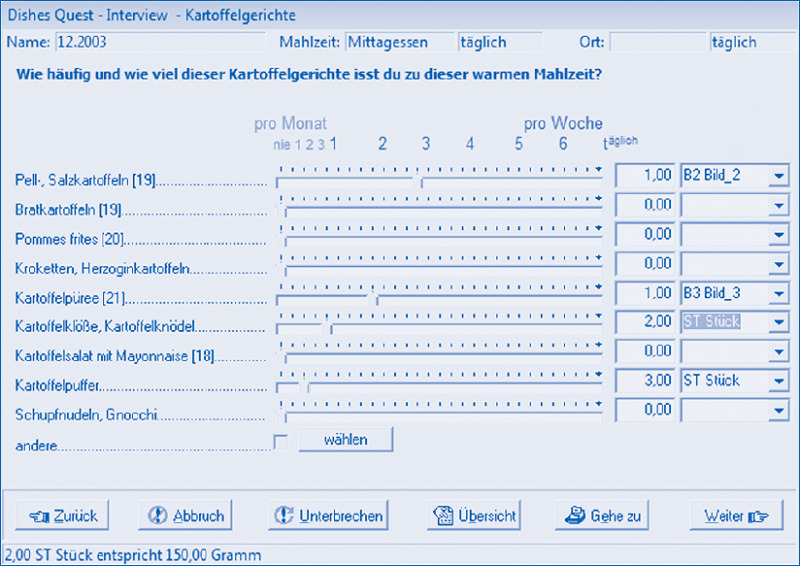
Example of a DISHES interview mask (in German)
Source: RKI
For both age groups, the survey also records details on school meals, diets, consumption of dietary supplements, as well as information including height and weight. This final item is important, because height and weight may be subject to change in the interval between data collection of KiGGS Wave 2 and EsKiMo II. EsKiMo II also includes participants who were not previously examined in the context of KiGGS Wave 2. The participants’ current weight is required to evaluate their diet.
3. Discussion and outlook
EsKiMo II will provide again up-to-date representative data for Germany on the dietary behaviour and nutrient intake of children and adolescents aged 6 to 17. This overview is complemented by data on even younger children collected in the KiESEL survey. This means that a comprehensive data set on the dietary behaviour of children and adolescents of all ages will be available. For nutrition research, food and health policy, as well as for the implementation and evaluation of prevention measures, this data constitutes an important source of information. Besides the Federal Ministry of Food and Agriculture (BMEL) and the Robert Koch Institute, further ministries including the Federal Ministry of Health (BMG), the Federal Ministry for the Environment, Nature Conservation, Building and Nuclear Safety (BMUB), and subordinated institutes such as the Federal Institute for Risk Assessment (BfR), the German Environment Agency (UBA), as well as the European Food Safety Authority (EFSA) are greatly interested in up-to-date data on the dietary behaviour of children and adolescents in Germany. This is because this data helps to identify deficits in the nutrition situation and to develop corresponding consumer protection measures.
Because food supply and therefore also dietary behaviour are changing constantly, surveys on dietary behaviour should be conducted at regular intervals. During the past years, for example, the number of gluten-free, vegetarian, and vegan products on offer has increased significantly. The contents of products such as breakfast cereals are also regularly modified. Consumption of exotic products in Germany has increased as a result of the globalisation of trade. This steadily expanding and changing supply of foods increases the difficulties of recording data on food consumption. Therefore, within EsKiMo II, food composition information on foods not yet included in the German Nutrient Database as well as dietary supplements is continually gathered.
The combination of EsKiMo I (2006) and EsKiMo II (2015-2017) for the first time enables a comprehensive analysis of changes in the dietary habits of children and adolescents in Germany over the past ten years. This is facilitated by the largely identical design and methods used in both surveys. The most important differences between both surveys are that in EsKiMo II data collection was one year longer and that food amounts are weighed instead of estimated. Both of these aspects ought to be considered when interpreting the results. To improve diet-related risk assessment, EsKiMo II uses a 3-day-weighted food record and an independent 1-day food record. EsKiMo is therefore now in line with the standards of other institutions such as EFSA [11]. All of the instruments used in EsKiMo II were developed in close collaboration with the KiESEL study team, a step that will ensure a high degree of comparability between both nutrition surveys.
The food record method produces a detailed and complete appraisal of consumed foods. Frequently, however, food consumption changes while conducting a record. This method is used for young children, in particular, because they cannot be interviewed on their dietary behaviour yet [12]. With adolescents, the willingness to keep such a diary for three consecutive days is probably significantly lower than among parents of younger children. Moreover, adolescents in particular spend a lot of time outside of their homes, which could make filling out a food record difficult. This is why for this group the DISHES interview was used.
Home visits will be concluded in September 2017. A more detailled description of the study design and methods is available elsewhere [13]. First results for EsKiMo II will be available in 2018. EsKiMo II results will be made available to policy-makers, science, and the interested public. Corresponding publication formats are being considered, such as project reports, press releases, and German and English language publications in academic journals.
Key statements
Adequate nutrition is essential in ensuring the healthy development of children and adolescents.
EsKiMo II provides an up-to-date overview of the dietary behaviour of 6-to 17-year-olds in Germany.
The data provide the basis for comprehensive analyses of trends in dietary habits over time of 6-to 17-year-olds.
EsKiMo II is an important source of information for nutrition and health policy.
Acknowledgement
We would like to thank all participants of EsKiMo II, their parents, and the entire KiGGS study staff.
Funding Statement
According to a German Bundestag decision, EsKiMo II was financially supported by the German Federal Ministry of Food and Agriculture (BMEL) through the Federal Office for Agriculture and Food (BLE), grant number 2814HS004.
Footnotes
Disclaimer
Note: External contributions do not necessarily reflect the opinions of the Robert Koch Institute
References
- 1.Birch LL. (1999) Development of food preferences. Annu Rev Nutr 19:41-62 [DOI] [PubMed] [Google Scholar]
- 2.Mensink GBM, Burger M. (2004) Was isst du? Ein Verzehrshäufigkeitsfragebogen für Kinder und Jugendliche. Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz 47(3):219-226 edoc.rki.de/oa/articles/rexKPi8f0KZ3E/PDF/25okAR8peLJI.pdf (As at 31.07.2017) [DOI] [PubMed] [Google Scholar]
- 3.Truthmann J, Mensink GBM, Richter A. (2011) Relative validation of the KiGGS Food Frequency Questionnaire among adolescents in Germany. Nutr J 10:133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mensink GBM, Bauch A, Vohmann C, et al. (2007) EsKiMo – Das Ernährungsmodul im Kinder- und Jugendgesundheitssurvey (KiGGS). Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz 50(5-6):902-908 edoc.rki.de/oa/articles/reEzagAaWOvY/PDF/26r8LhAfE99Dc.pdf (As at 31.07.2017) [DOI] [PubMed] [Google Scholar]
- 5.Stahl A, Vohmann C, Richter A, et al. (2009) Changes in food and nutrient intake of 6- to 17-year-old Germans between the 1980s and 2006. Public Health Nutr 12(10):1912-1923 [DOI] [PubMed] [Google Scholar]
- 6.Schweter A, Parreidt N, Lähnwitz C, et al. (2015) KinderErnährungsstudie zur Erfassung des Lebensmittelverzehrs (KiESEL). UMID 2(2):57-63 [Google Scholar]
- 7.Ocké M, de Boer E, Brants H, et al. (2012) PANCAKE - Pilot study for the Assessment of Nutrient intake and food Consumption Among Kids in Europe. European Food Safety Authority. Supporting Publications 2012:EN-339 [Google Scholar]
- 8.Van Kappel A, Amoyel J, Slimani N, et al. (1995) EPIC-SOFT picture book for the estimation of food portion sizes. International Agency for Research on Cancer, Lyon [Google Scholar]
- 9.Hartmann BM, Vásquez-Caicedo AL, Bell S, et al. (2008) The German nutrient database: Basis for analysis of the nutritional status of the German population. J Food Compost Anal 21, Supplement:P115-P118 [Google Scholar]
- 10.Mensink GBM, Haftenberger M, Thamm M. (2001) Validity of DISHES 98, a computerised dietary history interview: energy and macronutrient intake. Eur J Clin Nutr 55(6):409-417 [DOI] [PubMed] [Google Scholar]
- 11.European Food Safety Authority (2009) General principles for the collection of national food consumption data in the view of a pan-European dietary survey. EFSA Journal 7(12):1435 [Google Scholar]
- 12.Livingstone MB, Robson PJ. (2000) Measurement of dietary intake in children. Proc Nutr Soc 59(2):279-293 [DOI] [PubMed] [Google Scholar]
- 13.Lage Barbosa C, Brettschneider AK, Haftenberger M, et al. (2017) Comprehensive assessment of food and nutrient intake of children and adolescents in Germany: EsKiMo II - the Eating Study as a KiGGS Module. BMC Nutrition 3:75. [DOI] [PMC free article] [PubMed] [Google Scholar]